Trial Design
A randomized controlled trial of levosimendan to reduce mortality in high-risk cardiac surgery patients (CHEETAH): Rationale and design Alberto Zangrillo, MD, a,b Gabriele Alvaro, MD, c Antonio Pisano, MD, d Fabio Guarracino, MD, e Rosetta Lobreglio, MD, f Nikola Bradic, MD, g Rosalba Lembo, MSc, a Stefano Gianni, MD, a Maria Grazia Calabrò, MD, a Valery Likhvantsev, MD, PhD, h Evgeny Grigoryev, MD, i Giuseppe Buscaglia, MD, j Giovanni Pala, MD, k Elisabetta Auci, MD, l Bruno Amantea, MD, c Fabrizio Monaco, MD, a Giovanni De Vuono, MD, c Antonio Corcione, MD, m Nicola Galdieri, MD, d Claudia Cariello, MD, e Tiziana Bove, MD, a Evgeny Fominskiy, MD, PhD, a Stefano Auriemma, MD, n Massimo Baiocchi, MD, o Alessandro Bianchi, MD, p Mario Frontini, MD, q Gianluca Paternoster, MD, r Fabio Sangalli, MD, s Chew-Yin Wang, MB, ChB, t Maria Chiara Zucchetti, MD, u Giuseppe Biondi-Zoccai, MD, MSc, v,w Marco Gemma, MD, a Michael J. Lipinski, MD, PhD, x Vladimir V. Lomivorotov, MD, PhD, y and Giovanni Landoni, MD a,b Milan, Catanzaro, Naples, Pisa, Torino, Genova, Sassari,Udine, Vicenza, Bologna, Brescia, Potenza, Monza, Messina, Latina, Pozzilli, Italy; Zagreb, Croatia; Moscow, Kemerovo, Novosibirsk, Russia; Kuala Lumpur, Malaysia; Washington DC
Objective Patients undergoing cardiac surgery are at risk of perioperative low cardiac output syndrome due to postoperative myocardial dysfunction. Myocardial dysfunction in patients undergoing cardiac surgery is a potential indication for the use of levosimendan, a calcium sensitizer with 3 beneficial cardiovascular effects (inotropic, vasodilatory, and antiinflammatory), which appears effective in improving clinically relevant outcomes. Design Double-blind, placebo-controlled, multicenter randomized trial. Setting Tertiary care hospitals. Interventions Cardiac surgery patients (n = 1,000) with postoperative
myocardial dysfunction (defined as patients with intraaortic balloon pump and/or high-dose standard inotropic support) will be randomized to receive a continuous infusion of either levosimendan (0.05-0.2 μg/[kg min]) or placebo for 24-48 hours.
Measurements and main results The primary end point will be 30-day mortality. Secondary end points will be mortality at 1 year, time on mechanical ventilation, acute kidney injury, decision to stop the study drug due to adverse events or to start open-label levosimendan, and length of intensive care unit and hospital stay. We will test the hypothesis that levosimendan reduces 30-day mortality in cardiac surgery patients with postoperative myocardial dysfunction.
From the aDepartment of Anesthesia and Intensive Care, IRCCS San Raffaele Scientific Institute, Milan, Italy, bVita-Salute San Raffaele University, Milan, Italy, cAnesthesia and Intensive Care, Policlinico Universitario “Magna Grecia,” Catanzaro, Italy, d Cardiac Anesthesia and Intensive Care Unit, Monaldi Hospital A.O.R.N. “Dei Colli”, Naples, Italy, eDepartment of Anaesthesia and Critical Care Medicine, Azienda Ospedaliero Universitaria Pisana, Pisa, Italy, f Department of Anaesthesia and Critical Care Medicine, Città della Salute e della Scienza, Torino, Italy, g Clinic of Anesthesiology and Intensive Care Medicine, University Hospital Dubrava, Zagreb, Croatia, h Anesthesiology & Intensive Care Department Moscow Regional Clinical & Research Institute, Moscow, Russia, i Department of Intensive Care, Research Institute for Complex Issues of Cardiovascular Diseases, Kemerovo, Russia, j Anesthesia and Intensive Care, A.O.U. IRCSS IST San Martino, Genova, Italy, kCardiac Anesthesia and Intensive Care, Ospedale Civile SS. Annunziata, Sassari, Italy, lAnesthesia and Intensive Care, Azienda Ospedaliera Universitaria Santa Maria della Misericordia, Udine, Italy, m Department of Anesthesia and Critical Care, AORN "Dei Colli", Naples, Italy, nDepartment of Cardiac Surgery, Ospedale S.Bortolo, Vicenza, Italy, o Anesthesia and Intensive Care, S.Orsola-Malpighi University Hospital, Bologna, Italy, p Anesthesia and Intensive Care, Azienda Ospedaliera Ordine Mauriziano,
Torino, Italy, q Anesthesia and Intensive Care, Azienda Ospedaliera Spedali Civili, Brescia, Italy, r Departement of Cardiovascular Anaesthesia and Intensive Care, Azienda Ospedaliera S. Carlo, Potenza, Italy, s Anesthesia and Intensive Care, Ospedale S. Gerardo, Monza, Italy, tDepartment of Anaesthesiology, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia, u Anesthesia and Intensive Care, Azienda Ospedaliera Papardo-Piemonte, Messina, Italy, v Department of Medico-Surgical Sciences and Biotechnologies, Sapienza University of Rome, Latina, Italy, wDepartment of AngioCardioNeurology, IRCCS Neuromed, Pozzilli, Italy, x Division of Cardiology, Medstar Washington Hospital Center, Washington DC, and y Department of Anesthesiology and Intensive Care, State Research Institute of Circulation Pathology, Novosibirsk, Russia. Submitted July 1, 2015; accepted March 30, 2016. Reprint requests: Landoni Giovanni, MD, Department of Cardiothoracic Anesthesia and Intensive Care, San Raffaele Hospital, Via Olgettina 60, Milan, 20132, Italy. E-mail:
[email protected] 0002-8703 © 2016 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.ahj.2016.03.021
American Heart Journal Volume 177
Zangrillo et al 67
Conclusions
This trial is planned to determine whether levosimendan could improve survival in patients with postoperative low cardiac output syndrome. The results of this double-blind, placebo-controlled randomized trial may provide important insights into the management of low cardiac output in cardiac surgery. (Am Heart J 2016;177:66-73.)
Low cardiac output syndrome (LCOS) is a serious complication in patients undergoing cardiac surgery, a setting in which N20% of patients have acute cardiovascular dysfunction in the perioperative period. 1,2 This may result in multiple organ injury with in-hospital and long-term morbidity and mortality, in addition to prolonged intensive care unit (ICU) and hospital stay. Mortality rate in patients who develop LCOS after cardiac surgery is considerably high despite improvements in ICU treatment. However, survivors usually have an acceptable quality of life. Several meta-analyses 3–7 demonstrated that the calcium sensitizer levosimendan has cardioprotective properties (significantly reduces peak postoperative cardiac troponin release) and renal protective properties and may reduce mortality after cardiac surgery. Before the publication of these meta-analyses, no inotropic drug had been associated with improved outcomes in the setting of heart failure or cardiac surgery according to randomized evidence. On the contrary, previous studies and meta-analyses suggested an increased mortality in patients receiving “old” inotropic drugs. 8–10 A recent network meta-analysis confirmed that levosimendan is the most efficacious inodilator to improve survival in cardiac surgery. 11 A further meta-analysis conducted by Harrison et al 12 included 1,155 patients undergoing cardiac surgery with and without preoperative systolic dysfunction. The studies were grouped by mean ejection fraction (EF). Pooled results confirmed a reduction in mortality with levosimendan, and subgroup analyses showed that this benefit was confined to the low-EF (b40%) patients. According to this meta-analysis, levosimendan is associated with a reduction in myocardial injury, postoperative atrial fibrillation, and need for renal replacement therapy. 12 Levosimendan has a triple mechanism of action that may explain the improvement in clinically relevant outcomes. By binding to cardiac troponin C, it enhances myofilament responsiveness to calcium, thereby increasing myocardial contraction without increasing myocardial oxygen consumption. In addition, levosimendan activates sarcolemmal adenosine triphosphate–dependent potassium channels which are important mediators of ischemic and pharmacological cardioprotection. 13,14 Finally, in vitro and in vivo data suggested that the effect of levosimendan on mitochondrial adenosine triphosphate–dependent potassium channels exerts both an antioxidant and anti-inflammatory effect, which could be particularly relevant in the setting of cardiogenic shock. 15–17
In cardiac surgery, there are 2 possible settings in which levosimendan can be used: preoperatively in patients with low EF and postoperatively in patients who develop an acute myocardial dysfunction. The CHEETAH trial will study these latter patients. A panel of European experts recommended the preoperative use of levosimendan in patients with generally compromised myocardial function, including right ventricular dysfunction. 21 In both coronary artery bypass graft and valve surgery, 18,19,20 levosimendan administration was associated with improvement in cardiac function and with lower mortality and number of complications 24,25 in patients with low preoperative EF. An ongoing multicenter trial (LEVO CTS NCT02025621) is already randomizing 760 patients (levosimendan vs placebo) with preoperative EF b35% undergoing on-pump cardiac surgery procedure in North America. Furthermore, a multicenter clinical trial (LICORN NCT02184819) randomized 335 (levosimendan vs placebo) patients with preoperative EF b40% undergoing coronary artery bypass graft surgery with or without associated mitral repair in France. In a different way, we are trying to demonstrate that levosimendan can reduce mortality in patients who had just developed LCOS after cardiac surgery. We decided to randomize patients with ongoing LCOS also for a pharmacoeconomic reason: in our experience, only a small percentage of patients with a preoperative low EF will develop postoperative LCOS, and levosimendan is still a very expensive drug as compared with other inotropic agents. Accordingly, we decided to treat only patients with early postoperative myocardial dysfunction rather than all patients with preoperative low EF to increase the chance to find significant differences in mortality using a reasonably low number of randomized patients. Therefore, we plan to conduct the first large doubleblind, placebo-controlled, multicenter, randomized trial to determine whether levosimendan significantly improves survival in patients with postoperative myocardial dysfunction following cardiac surgery.
Materials and methods Study design, approval, and registration The study was approved by the Ethical Committee of all participating centers and was registered on clinicaltrial.org as NCT00994825.
American Heart Journal July 2016
68 Zangrillo et al
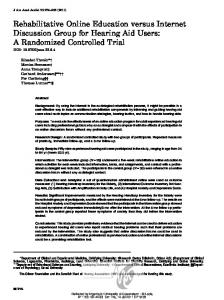
Figure 1
All non emergent cardiac surgery patients are approached preoperatively if they don’t have exclusion criteria (See table 1)
Signed the written consent
Excluded -Decline to participate (5-20% expected) -Participation to other randomized studies (1-5% expected)
Patients with postoperative LCOS defined as need for IABP or high inotropic support within the first 24 hours (10% of patients who signed the written consent and > 95% of randomized population)
Patients with preoperative IABP or a preoperative EF < 25% (< 1% of patients who signed the written consent and