either the diagnosis or the treatment of ASD. .... Social Skills. Research has highlighted a shift from teaching single ...... delivered pivotal response training.
Integration of Evidence-Based Practices
Addressing the Challenges: Developing a Programmatic Framework for the Systematic Integration of Evidence-Based Practices for Young Children with Autism Spectrum Disorder J anine P eck S tichter , U niversity of M issouri –C olumbia T erry B rown , R ikkii C larent , J ill I skow , M onica K rug , and J anet R ichards , H uron I ntermediate S chool D istrict D enise K ay , U niversity of M issouri –C olumbia
Abstract: National concern about the growing number of identified children with autism spectrum disorder (ASD) has increased efforts in the research field (National Research Council, 2001; Odom et al. 2003; Simpson, 2005) and the U.S. federal government (U.S. House of Representatives, 2005) to provide specific recommendations regarding appropriate educational practices. Nevertheless, school districts remain challenged to articulate recommendations in everyday practice, particularly in light of the noted increase in the number of children eligible for ASD-related services under the Individuals with Disabilities Education Improvement Act (IDEA, 2004), the recognized shortages in special education service providers, and the significant increases in per student costs. This article describes how one school district, the Huron Intermediate School District (Huron ISD) responded to this challenge for their pre-K through elementary students with ASD, while still maintaining their commitment to the practical application of established research-based practices for all students. Key features of the program and its implementation as a teambased process are described. Initial data on student outcomes is also presented. The implications and importance of developing a programmatic framework of evidence-based practices to bridge research to practice is discussed.
T
he last decade has demonstrated a six-fold increase in the number of children classified with Autism Spectrum Disorder (ASD) (Center for Disease Control and Prevention, 2005). This increase has spawned growing national interest and subsequent practical concern, specifically in the provision of educational services for students with ASD (Center for Disease Control and Prevention, 2005; Odom et al, 2003). In response to this heightened concern, the United States House of Representative Subcommittee on Human Rights and Wellness commissioned a briefing report to highlight the status of education for children with ASD. The final report summarized three key variables affecting current educational programming for these children: (a) the number of children served under the Individuals with Disabilities Education Act (IDEA) who are diagnosed with ASD; (b) the estimation of the per pupil cost for educating children with ASD; and (c) recent conclusions regarding
18
BB16(1).indd 18
best practices for providing educational services to children with ASD. The briefing report (U.S. House of Representatives, 2005), prepared for the Subcommittee on Human Rights and Wellness, noted a more than 500% increase in the number of children diagnosed with ASD and served under IDEA in the last decade. According to the report, estimations of the average per-pupil expenditure for educating a child with autism is three times that of expenditures for serving students without identified special needs, significantly outpacing any other low-incidence disability category in growth. The increase in the number of children diagnosed with ASD, paired with the second-highest average per-student expenditure ($18,800 as opposed to $20,100), has further oriented the subcommittee and the nation towards formal articulation of recommended educational approaches for these students. To identify recommended educational approaches, the Subcommittee on Human Rights and
Wellness relied heavily on the review published by the National Research Council (NRC). This review, entitled Educating Children with Autism (NRC, 2001), utilized an interdisciplinary approach to synthesize and evaluate current information about autism for the purpose of providing “recommendations regarding educational policies affecting families with young children with autism” (p. 13). The literature review and summaries provided in the NRC report specifically focus on “early intervention, preschool, and school programs designed for children with autism from birth to age 8” (p. 2) with targeted interest in issues such as diagnosis and classification, early intervention, inclusion, assistive technology, and the rights of children with ASD under IDEA. This extensive NRC review is often cited as a research-based guide to effective and emerging best practices for educating children with ASD (Odom et al. 2003; Simpson, 2005). Based on the NRC (2001)
Beyond Behavior
10/23/06 1:10:12 PM
Integration of Evidence-Based Practices
recommendations, the congressional briefing (U.S. House of Representatives, 2005) highlighted several key features for effective educational programming for young children with ASD, including responsive and intensive early intervention to students with a suspected or confirmed diagnosis, active engagement in intensive instructional programs (at least 25 hours per week, over 5 days per week) that include structured environments as well as targeted instructional delivery and curricular domain areas, the incorporation of a family component, and a strong evaluation and monitoring system. In summary, the report presented to the Subcommittee on Human Rights and Wellness echoes the NRC report, highlighting that the educational goals for children with autism and children without identified special needs are the same: personal independence and social responsibility. The distinction for children with ASD, however, is recognized in the intensity and delivery of the supports necessary to achieve these goals (Dawson & Osterling, 1997; Hurth, Shaw, Izeman, Whaley, & Rogers, 1999) Despite the positive implications of the consistent recommendations from the research field (NRC, 2001; Odom et al., 2003; Simpson, 2005) and the federal government (U.S. House of Representatives, 2005), school districts are increasingly challenged to articulate these recommendations in terms of everyday practice, particularly in light of the noted increase in the number of children eligible for services under IDEA, the recognized shortages in special education service providers, and the significant increases in perstudent costs. This article describes how one school district, the Huron Intermediate School District (Huron ISD), responded to this challenge for their pre-K through elementary age students with ASD, while still maintaining their commitment to everyday implementation of established research-based practices for all students.
The Process of Redefining Effective Program Delivery Huron Intermediate School District The Huron Intermediate School District (Huron ISD) is located in a geographically isolated county within the state of Michigan. In recent years this region has experienced downward shifts in economy and demographics, resulting in a decrease in school enrollments across the eight K–12 local school districts, seven K–8 school districts (one-room schoolhouses), and six parochial schools. Together these districts and schools, supported by the ISD, serve approximately 6,500 students. The function of the ISD is to support the educational mission of the local schools, including 100% provision of the special education ancillary services for low-incidence populations. Though the ISD is small, the staff has maintained a reputation for remaining proactive in their program design and implementation efforts, placing high emphasis on the coordination and merging of expertise in order to establish and realign curriculum, plan and implement professional development, and work toward continuous improvement of educational programs and services. In
The educational goals for children with autism and children without identified special needs are the same.
BeyondBehavior
BB
order to meet demands for facilities, staff, administration and/or fiscal support, the ISD actively participates in collaborative relationships with other human service agencies in the county and the state. Despite its size, in recent years the Huron ISD has experienced similar proportional increases in the number of students identified with ASD, as reported at both the national (U.S. House of Representatives, 2005) and state levels (Nutall, 2002). Between 2000 and 2001 alone, the population of students with ASD more than doubled, increasing from 10 to 25 students. Newly diagnosed students in the 2-to5-year-old group reflected the largest increase in numbers of students with ASD. The impact of this increase was most acute in the early childhood classrooms supported by the ISD, with the early childhood staff being especially vulnerable to the challenge of providing appropriate services for the increasing number of students with ASD. Concerns about appropriately meeting the needs of the children’s families were growing as well. Parents of children with ASD were communicating mixed messages, with some parents requesting that the ISD take more of the lead regarding the needs of their children, including the provision of a more clearly defined “best approach” for appropriate service provision. Other parents, accessing the Internet for information and resources about ASD, endorsed specific approaches as the “only hope” for their child. What was once a low-incidence population, typically handled by various staff on a one-by-one basis as issues arose, became a priority for the Huron ISD during the 2000–2001 school year. Concerns developed over a variety of subsequent issues, such as staff-to-student ratios, weekly hours of instruction, training for staff, appropriate curriculum, the use of a variety of appropriate interventions, and ongoing progress-monitoring of students. There was a growing
Fall 2006
BB16(1).indd 19
19
10/23/06 1:10:12 PM
Integration of Evidence-Based Practices
awareness among the ISD staff and administration that the ISD needed to provide comprehensive programming, grounded in research that would provide an efficient but appropriate response to their growing concerns, as well as maintain long-term success for both the students and the district. The Process To identify evidence-based solutions for serving early childhood students with ASD, the Huron ISD recruited a multidisciplinary team of individuals who were familiar with specific problems related to either the diagnosis or the treatment of ASD. The team included teacher and paraprofessional representatives from the spectrum of early childhood programs within the district, as well as representatives from administration and the parent advisory committee. Parents, speech and language pathologists, occupational therapists, and a school psychologist were recruited as additional members of the multidisciplinary team. The initial focus of the multidisciplinary ISD team was to assess program needs. As the team initiated the assessment process, it became apparent that, though the team represented a strong interdisciplinary knowledge-base in educationally relevant practices, additional expertise were needed, specifically expertise regarding ASD characteristics and practices in terms of the research literature. The team solicited the expertise of the first author, who became an adjunct member of the team. The team began by clarifying the priorities of the relevant stakeholders, including the Huron ISD, the educational community, the students and their families, and additional agencies, all to whom the ISD programs were accountable (IDEA, state and local laws, rules, plans). Through a consensus-building model, the ISD determined basic values, beliefs, and guiding principles, eventually establishing a specific educational philosophy for the district. As the clarification process unfolded, the team strengthened their commitment to
20
BB16(1).indd 20
developing individualized programs that were responsive to each student’s level of development and family priorities, that applied a variety of evidence-based strategies and interventions, that utilized ongoing assessment and evaluation, and that engaged students in active learning in order to maximize program effectiveness and student learning in a variety of environments. The second goal of the ISD team was to articulate a framework from which to develop the early childhood program for students with ASD. In this process, repeated emphasis was placed on identifying approaches that either influenced and/or created meaningful outcomes for students. Outcomes of interest to the ISD paralleled many of the recommendations endorsed by the NRC (2001), including success in communicative exchanges, emotional expression and regulation, socialcommunicative motivation, social competence, peer relationships, and functional competence in natural environments. The team recognized that, though projected outcomes might be similar for all children, the delivery of identified approaches would require an additional level of program development, training, and collaboration for children with ASD. In their efforts to identify viable approaches, the ISD team utilized numerous resources, including an extensive review of the research; dialogue and collaboration with others immersed in the field of ASD (e.g., medical field, university faculty, advocacy groups); participation in training and workshops; communication with families; multidisciplinary team discussions; and ongoing clinical practice and experience in the classroom, in therapy, in the community, and in the home environment. After review of all the information collected in this investigative process, the ISD team formalized the educational philosophy for young children with ASD, highlighting 12 fundamental tenets of practice (Brown, Iskow, & Richards, 2001; Dawson & Osterling,
1997; Greenspan & Wieder, 1997; Hurth et al., 1999; NRC, 2001; Olley, 1999) (see Appendix A for a description of each tenet and corresponding references): 1. Focus on individual child 2. Partnership with family 3. Multidisciplinary/collaborative approach 4. Comprehensive developmental assessment/ongoing monitoring of progress 5. Longitudinal and dynamic planning 6. Social, behavior, and communication emphases 7. Appropriate continuum of interventions 8. Instructional strategies/ environmental supports 9. Individualized and contextually relevant curriculum 10. Participation in an inclusive environment 11. Ongoing collaboration/ professional development/ administrative support of team 12. Program evaluation. The underlying goal of the revised early intervention program was to address the unique needs of students with intensive behavior, social, and emotional needs, such as students with ASD, through the continued utilization of evidence-based practices currently recommended in the professional literature. The Buddy Enriched Structured Teaching (B.E.S.T.) program was developed by the ISD as a mechanism for achieving this goal. Model Program Development The programming and curricular components of the B.E.S.T. program are selectively linked to the district’s general education curriculum. The five components of the program are consistent with key features of effective interventions for students with ASD, as highlighted in the briefing to the Subcommittee on Human Rights and Wellness (U.S. House of Representatives, 2005) and the NRC (2001): 1. Curriculum content with specific priority on social/communicative interactions 2. Highly engaging and intensive
Beyond Behavior
10/23/06 1:10:13 PM
Integration of Evidence-Based Practices
learning environments and generalization strategies 3. Family involvement through collaboration and home–school connections 4. Rigorous and consistent assessment and evaluation of student progress and program services 5. Systematic and aligned transitions from the preschool to the elementary education program. These five components provided a strong foundation for integrating solid best-practice activities/interventions into the pilot program. A description of how the various components were implemented and maintained in the Huron ISD follows. Curriculum content with specific priority on social/communicative interactions. The briefing to the Subcommittee on Human Rights and Wellness (U.S. House of Representatives, 2005) suggests that learning objectives for children with ASD focus on the development of: (a) social skills; (b) expressive and receptive language; (c) nonverbal communication skills; (d) functional symbolic communication system; (e) engagement and flexibility in developmentally appropriate tasks and play; (f) fine and gross motor skills; (g) cognitive skills; (h) conventional/ appropriate behavior; (i) independent organizational skills; and (j) skills for success in a regular classroom. When developing the curriculum for the B.E.S.T. program, the Huron ISD was guided by the district’s early childhood curriculum. The early childhood curriculum represents a comprehensive approach that encourages exploration and engagement, utilizes developmentally appropriate practices, and highlights the development of functional competencies through the use of effective research models. In the curriculum development process, the use of evidence-based research served as the backdrop for each programmatic element of the B.E.S.T. program (Ivannone, Dunlop, Huber, & Kincaid, 2003; NRC, 2001;
The delivery of identified approaches would require an additional level of program development, training, and collaboration for children with ASD. Odom et al., 2003; Simpson, 2005). Relevant ISD personnel became versed in key research related to effective instruction and integration of students. Specific intervention strategies for individual students were determined by the student’s profile, which was developed through ongoing assessments across developmental domains, parental input, and consideration of the unique needs of the child. Table 1 represents the initial framework used by the team to develop the B.E.S.T program. For each best practice domain, the table summarizes recommendations from professional literature and offers examples of research-based programs that address the domain. (The individual programming needs and delivery models are determined by the individualized educational plan [IEP] team.) The domains listed support individualized educational programming in a structured and comprehensive manner. The interventions listed have been demonstrated as appropriate for the domain within the literature. However, many of the strategies are applicable
BeyondBehavior
BB
across several domain areas, delivering a comprehensive curriculum that utilizes multiple approaches. Highly engaging and intensive learning environments and generalization strategies. The NRC report (2001) endorses “active engagement in intensive instructional programming” (p. 6) and suggests that instructional programming for students with ASD include use of planned teaching opportunities for relatively brief periods of time and sufficient adult attention during one-on-one and small-group activities. The Huron ISD endorsed similar goals by customizing one classroom, in the building that housed the other early childhood programs run by the ISD, as a venue for providing intensive learning experiences for the early childhood students with ASD. The classroom was set up to look similar to the adjacent School Readiness and Preprimary Inclusion classrooms in which B.E.S.T. students spend a major portion of their time (typically half a day). Although the B.E.S.T. program incorporates developmentally appropriate practices (Bredekamp & Cople, 1997), the B.E.S.T. classroom also includes unique physical and philosophical components to optimize the learning opportunities for students with ASD (Heflin & Alberto, 2001). Additionally, the classroom is easily viewed without disruption through the use of a oneway mirror and adjacent observation room. This feature is particularly beneficial for parents and various support providers. An adjoining room houses the occupation therapy services and can be connected by moving a removable wall. Students receive a minimum of 25 hours of intensive early intervention through the B.E.S.T. site-based program and the home-based component (see the family involvement section that follows) (NRC, 2001; U.S. House of Representatives, 2005). Students typically receive three full days (i.e., Tuesday, Wednesday, and Thursday) of instruction. Half of the day is spent in the B.E.S.T. program, during which highly intensive, individualized instruction takes place. Fall 2006
BB16(1).indd 21
21
10/23/06 1:10:14 PM
Integration of Evidence-Based Practices
Table 1 ��Best Practice Curriculum for Students with Autism (B.E.S.T. Program)
Domain
Description
Social Skills
Research has highlighted a shift from teaching single • LEAP (Strain & Cordisco, 1994; Strain & Hoyson, behaviors (e.g., shaking hands) to essential skills that are 2000) likely to lead to additional skill development and social • Peer-Mediated Social Skills Programs (Odom & opportunities in integrated settings (Koegel & Koegel, Strain, 1986; Lauschey & Heflin, 2000) 1995; Stahmer, 1995; Stichter & Conroy, 2005).
Communication
Current research emphasizes efficient communication skills that lead to naturally reinforcing consequences. These communication acts should require minimal effort, yet effectively achieve their intended purpose. Communication needs to be taught within social contexts across environments. A communication curriculum should be integrated within the student’s life in areas such as social, leisure, academic, and community. (Carr et al, 1994; NRC, 2001; Thorp, Stahmer, & Schreibman, 1995).
Behavior
In the last few decades, research has focused on the use of functional assessment to identify the function of behavior challenges. Additional curriculum components • Applied Behavior Analysis (ABA) (Grindle & Remington, 2002; Koegel, Koegel, & Schreibman, encourage the promotion of prosocial behaviors that 1991; Smith & Lovaas, 1998) support learning. Appropriate prosocial skills are taught as replacements for inappropriate behavior. Preference • Positive Behavior Support (PBS) (Horner, 2000; and strengths are also accessed in order to create Lorimer, Simpson, Myles, & Ganz, 2002) opportunities for success (Dunlap & Fox, 1999; Wolery & Winterling, 1997).
Self Help
To effectively function, children with autism need to learn self-help skills. Learning is optimized when skills are broken down into concrete, manageable tasks and steps. Research has demonstrated many successful ways this can be done (Charlop-Christy, Schreibman, Pierce & Kuntz, 1998; Lovaas & Buch, 1997; Shipley-Benamou, Lutzker, & Taubman, 2002).
Cognition
This domain is essential to address in order to assist children in applying broad concepts and problemsolving skills. Unfortunately, it is often an area underdeveloped in early intervention programs for students with autism. Examples of cognitive skills that can be effectively incorporated are teaching abstract concepts, memory tasks, thinking skills, problemsolving strategies, and self-management (CharlopChristy et al. 1998).
SelfManagement
22
BB16(1).indd 22
Research supports the need for children to work independently, experiencing natural consequences (reinforcers) as opposed to relying on artificial reinforcers. By increasing structure, following natural sequences, and incorporating techniques as visual schedules, students with autism have demonstrated the acquisition of impressive self-management skills (McClanahan & Krantz, 1999; Schreibman & Koegel, 1996).
Selected Interventions
• Picture Exchange Communication System (PECS) (Bondy & Frost, 2001; Charlop-Christy et al., 2002) • TEACCH (Schopler, Mesibov, & Hearsey, 1995; Van Bourgondien, Reichle, & Schopler, 2003)
• Huron ISD Early Childhood State Curriculum Competencies • Developmentally appropriate early childhood practices (Smith et al., 2002) • Huron ISD Early Childhood State Curriculum Competencies • Developmentally appropriate early childhood practices (Smith et al., 2002) • LEAP (Strain & Cordisco, 1994) • Applied Behavior Analysis (ABA) (Grindle & Remington, 2002; Koegel et al, 1991; Smith & Lovaas, 1997)
• TEACCH (Schopler et al., 1995; Van Bourgondien et al., 2003) • PECS (Bondy & Frost, 2001; Charlop-Christy et al, 2002)
Beyond Behavior
10/23/06 1:10:15 PM
BeyondBehavior
BB
Integration of Evidence-Based Practices
Table 1 ��Best Practice Curriculum for Students with Autism (B.E.S.T. Program) (continued)
Domain
Description
Play
Play is an integral part of many best-practice preschool programs. The literature consistently highlights the benefits of play for children in learning to interact effectively with peers, to functionally imitate, and to promote generalization of new skills. Play should be encouraged within natural settings (as opposed to always teacher directed), promoting well-researched elements of play that children can learn and use spontaneously (Baker, 2000; Brown & Conroy, 2002; Stahmer, 1995; Strain & Cordisco, 1994).
Motor Skills
Selected Interventions
Motor skills development has been an ongoing part of early childhood programs. Increased interest in the integration of motor skills for students with autism is emerging. Researchers are looking into the impact of increased attention to physical exercise on reducing behavior problems and promoting increased success in creative areas, such as music and art. Additionally, addressing motor skills early better prepares students for pre-academic and future educational skill areas (Wolery & Winterling, 1997; NRC, 2001).
Structured small-group activities that use a peer-mediated learning model (Stichter & Conroy, 2005) and focus on the developmental areas of social, cognition, sensory, motor, and communication, are also implemented. The staff-to-student ratio is generally 1:2, allowing for high levels of staff support to ensure successful social interactions between the student with ASD and nondisabled peers. The other half of the full-day program (as well as half day on Monday) is spent in an inclusive classroom setting that includes the same buddy that was involved in the peer-mediated learning in the B.E.S.T. room. This integrated format allows students to generalize skills across a variety of environments and situations. Having the same buddy in both settings facilitates generalization as well as reduces anxiety for the student with ASD. The B.E.S.T. program receives support from a variety of services. In addition to providing direct services to the B.E.S.T. program on a
• Floortime—(Developmental, Individual-Difference, Relationship-Based (DIR) (Greenspan & Weider, 1997) • LEAP (Strain & Cordisco, 1994) • Peer-Mediated Social Skills Program (Odom & Strain, 1986; Lauschey & Heflin, 2000) • Huron ISD Early Childhood State Curriculum Competencies • Developmentally appropriate early childhood practices (Smith et al., 2002)
• Huron ISD Early Childhood State Curriculum Competencies • Developmentally appropriate early childhood practices (Smith et al., 2002)
daily basis, a speech pathologist and occupational therapist also serve on planning teams and provide support in skill generalization and transfer (when B.E.S.T. students participate in
The integrated format allows students to generalize skills across a variety of environments and situations.
inclusive classroom activities). A school psychologist facilitates the assessment process and collection of data. A school social worker supports individual students and families (e.g., access services from local agencies, provide information), works with the B.E.S.T. team to implement positive behavior supports, and assists with functional behavior assessments and behavior plans. To accommodate the need to access the expertise of the large number of professionals who work with B.E.S.T. students, Mondays are divided between team planning and consultation with staff in the Early Childhood/School Readiness Program. Monday planning time is devoted to team discussion and evaluation of the effectiveness of current strategies for individual students, with modifications incorporated as necessary. Monday consultation time supports the transfer of skills across environments in the integrated program (Gersten, Chard, & Baker, 2000; Simpson, 2004). Fall 2006
BB16(1).indd 23
23
10/23/06 1:10:16 PM
Integration of Evidence-Based Practices
Comprehensive training is also a key element in securing the success of the learning environments of the B.E.S.T. program. Professional development and access to best practice resources was, and continues to be, an unending priority addressed through ongoing collaboration with the first author and through collaboration with a regional and statewide network. Training efforts for the program include a variety of components: consultation with a content expert to monitor program effectiveness, attendance at professional conferences and workshops that address the latest information in best practice strategies linked to the curricular framework, and training opportunities that focus on team building and/or address the need areas prioritized by the B.E.S.T. program team (Simpson, 2004). Each member of the B.E.S.T. team receives all aspects of the comprehensive training. This has supported the B.E.S.T. model by ensuring that paraprofessionals, as well as teachers and specialists, take equal responsibility for all aspects of the program. For example, this allows any one of the paraprofessionals to facilitate a classroom activity while the speech and language pathologist targets certain communication goals within the activity. Meanwhile, the lead teacher can conduct curriculumbased assessment for one particular student without any concerns regarding the fidelity of program implementation (Iovannone et al., 2003). The lead teacher of course still maintains appropriate level of responsibility for program planning and integrity of implementation. In an effort to enhance the ongoing professional development of the B.E.S.T. team, as well as the professionals in receiving local schools across the county, regional collaborations were initiated and an information packet was designed. The information packet provides information about the causes, characteristics, and current incidence
24
BB16(1).indd 24
rates of ASD as well as strategies to support quality educational programming for students with ASD, including approaches for instructional and classroom management, promoting social interactions, and dealing with challenging behavior. The information packet is disseminated to receiving teachers of students with ASD; shared through regional and statewide conference presentations; and posted on the ISD, regional, and statewide Web sites. Family involvement through collaboration and home–school connections. The NRC report (2001) encourages local school districts to support the families of students with ASD through the consistent provision of: (a) information; (b)
Any one of the paraprofessionals can facilitate a classroom activity while the speech and language pathologist targets communication goals and the teacher conducts curriculum-based assessment. individualized problem solving; and (c) ongoing consultation and guidance targeted to minimize behavioral problems and maximize developmentally appropriate skills. Within the Huron ISD, parents and caregivers of students with ASD are encouraged to be active participants in the comprehensive intervention process (Dunlap, 1999; Odom et al, 2003). Support through home visits
and information dissemination is provided so that families incorporate curriculum goals into their natural environments and routines. The staff complete home visits on Fridays, spending concentrated time with both the parent(s) and the child. In the home, staff can review strategies and model interventions that have been successful in the classroom and that support curriculum goals. The training provided to parents by the Huron ISD is multifaceted, including classroom visits/ observations, local family enrichment opportunities, and participation in formal conferences and workshops as appropriate. Every effort is made to offer local trainings at convenient times and locations for parents. Local family enrichment trainings are typically staggered monthly, between day and evening workshops, and are free of charge (with childcare provided at no cost). When applicable, financial support is available for parents who want to attend costly conferences out of the area. This financial support is available due to the efforts of the ISD to regularly write local and state grants to support many of its professional development and information-dissemination expenses. Rigorous and consistent assessment and evaluation of student progress and program services. NRC (2001) recommends the identification of learning objectives across a wide range of skills for students with ASD. The NRC report also recommends frequent documentation of student progress towards identified objectives in order to inform the effectiveness of, and/or to make appropriate adjustments to, applicable interventions. In order to evaluate student progress and inform teaching strategies, the Huron ISD developed a comprehensive assessment tool. This tool is utilized on a regular basis (two-to-four times per year) so that curriculum can be modified, as necessary, to meet individual needs. This tool incorporates parental
Beyond Behavior
10/23/06 1:10:16 PM
Integration of Evidence-Based Practices
BeyondBehavior
BB
Figure 1 � �Sample page from the B.E.S.T. Family Assessment Tool
Fall 2006
BB16(1).indd 25
25
10/23/06 1:10:21 PM
Integration of Evidence-Based Practices
evaluation of the student’s transfer of skills within both the home and the community. Social, behavior, communication, sensory, health, safety, and self-help domains are evaluated, using a series of simple questions regarding the student’s current level of functioning within and without school settings. Figure 1 depicts part of the social-behavior section of the Family Assessment Tool. Other informal data-collection systems are utilized based on core developmental standards of the program and, in particular, based on those geared toward progress monitoring of IEP goals and objectives. Additional formal and ongoing informal data are continuously collected on individual student progress. Formal assessment tools, such as the Preschool Language Scale (4th ed.) (PLS-4) (Zimmerman, Steiner, & Pond, 1992) for speech and language assessments and the Vineland Adaptive Behavior Scales (Rev. ed.) (Sparrow, Balla, & Cichetti, 1984) for general developmental profiles, are also accessed as appropriate. One measure that is completed each year for students in the B.E.S.T. program (as well as for subsequent programming) is the Assessment of Basic Language and Learning Skills (ABLLS) (Partington & Sundberg, 1998). This assessment provides a baseline and is an ongoing tracking system across 25 skill areas, representing such domains as social/ communication, motor development, and academics (e.g., reading, math, writing, and spelling). Systematic and aligned transitions from the preschool to the elementary education program. One common component in well-known models of early intervention for children with ASD is “specific preparation for children’s transition from intensive intervention into school programs” (NRC, 2001, p. 165). Common elements of transition plans, as highlighted by the NRC (2001) report include: (a) visits to the receiving school in order to determine the potential match between the new school and the child and to identify skills the child will
26
BB16(1).indd 26
need in order to function adequately in the new environment; (b) inviting receiving teachers to visit the early childhood program and to access the child’s intervention history; (c) gradual transitions to the new setting accompanied by familiar staff; and (d) follow-up consultations as needed. The Huron Learning Center early childhood staff developed a transition system that uses the six key points to ensure successful transitions, as suggested by the Early On program model, a transition program for early childhood students (Rosenkoetter & Fowler, 1986). The key elements include: (a) the necessity of preplanning; (b) communication with all involved parties; (c) shared information and trust between all parties; (d) empowering parents to advocate responsibly for their children; (e) seeking least restrictive environments where children can function successfully; and (f) evaluating transitions for further improvement The process by which the Huron ISD integrated many of these points into their early childhood transition program for students with ASD is described in the following section. Preplanning In the spring of 2003, planning for the 2003–2004 school year had already started. While the plan was to continue operation of the B.E.S.T. program, a major priority for the ISD was to ensure a successful and supported transition of the initial B.E.S.T. students who were ready to move on to local kindergarten and first grade classrooms served by the ISD. Students in the B.E.S.T. program had made significant gains, but the generalization of these gains would be jeopardized if action was not taken to ensure that continued progress would occur as the students transitioned upward in their educational careers. The ISD began to discuss the development of a systematic and thorough transition process (Odom et al., 2003). The identified priorities for this transition process were to: (a) increase awareness/acceptance
of students with ASD by the local education agencies (LEA); (b) increase the willingness of LEAs to participate in trainings on ASD and related instructional strategies; (c) ensure successful and appropriate inclusion of students in LEAs (academically and socially); (d) build capacity within LEAs to handle students with these types of issues; and (e) support LEAs in identifying these students as part of their collective student body. Communication and shared information and trust with involved parties. To ensure that the B.E.S.T. students experience a smooth transition to their new school, the B.E.S.T. program teacher leads the transition process. The B.E.S.T. program teacher collaborates with her team, as well as with the child’s parent(s), to explore options and make decisions to benefit the individual student in the transition process. This process culminates in an individualized transition portfolio for each student. Preschool-to-kindergarten transition activities typically begin in the spring of the school year. Emphasis is placed on working closely with each receiving local school to determine appropriate transition activities that are friendly to the student, to the student’s family, and to the local district. These activities may include staffings with current and receiving staff/providers, as well as visits with the student to their new school. The start of the B.E.S.T. program is delayed by two weeks at the beginning of each year so that the B.E.S.T. teachers and other appropriate B.E.S.T. program staff can be available to facilitate the transition of students to their LEA at the start of the year. The parent(s) and receiving teachers have reported benefits to this approach. The parent(s) have the security of knowing that the child will be with a familiar adult in their new school at the beginning of the school year. Receiving school teachers obtain support as they begin the school year with a new and potentially more challenging student. Least restrictive environments. To ensure the continued use of evidence-based programming for the
Beyond Behavior
10/23/06 1:10:22 PM
BeyondBehavior
BB
Integration of Evidence-Based Practices
transferring B.E.S.T. students, the ISD established a model support room, housed at a local elementary school. This particular school was chosen because it was located in the district of residence for many of the B.E.S.T. program students who would be transitioning into kindergarten. For students transferring to other local schools, the B.E.S.T. team members are available to support and evaluate their transition process. For the first year, the model support room was supported by a lead teacher and three paraprofessionals. As in the B.E.S.T program, the ultimate goal of the model support room was to increase student outcomes by: (a) the transfer and implementation of best practice activities in the model support room; (b) the development of a system for integrating peers into the model support room; and (c) the provision of training opportunities to staff so that overall capacity within the school was strengthened. During the course of the year, a change in the name of the program was suggested by parents and staff members. The program was
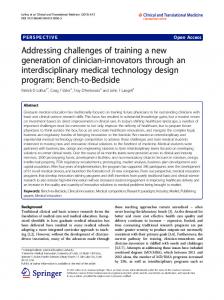
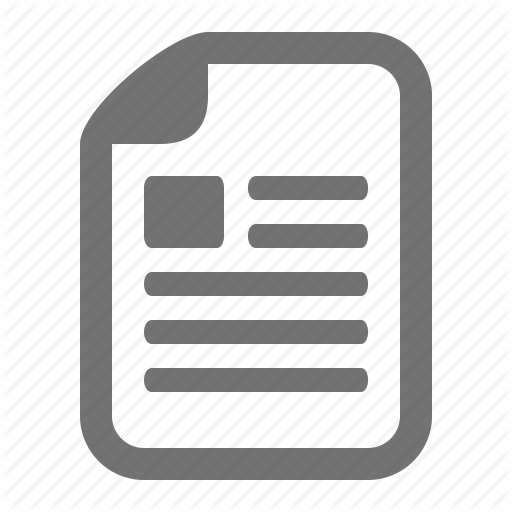
renamed the Giving Everyone More Support (G.E.M.S.) program. Figure 2 depicts the framework that was created for the G.E.M.S. program, including staffing and ancillary team-based support. During the first year of the program, all four staff members were in the building on a full-time basis. Five students identified with ASD utilized the program at varying levels of involvement, as determined by the IEP process. However, each student spent time in the general education classroom for part of their day and was supported by the paraprofessional staff as needed (coteaching or collaborating with general education teacher). The success of the G.E.M.S. program during the first year exceeded all expectations. Individual IEP data indicated that, without exception, all five students transitioned beautifully and demonstrated significant growth in all areas of development. Figures 3 and 4 demonstrate progress by one of the initial students in the program, Jared (pseudonym), as measured during the first year of the B.E.S.T.
program and then again during his first year of transition to the G.E.M.S. program. Note the consistent gains across all domain areas on both the formal ABLLS assessment and the informal family assessment (described previously). Additional data for students in the B.E.S.T program are collected and charted for IEP goals, specific behavior interventions, and communication goals. During the second year of programming, the G.E.M.S. program made a few changes. The lead teacher spent half the day in the program, with the three paraprofessionals continuing full time. Three of the five students who started in the B.E.S.T. program required only minimal time in the G.E.M.S. program. The other two students continued to make strides, but still required some time devoted to direct-instruction activities and needed support during their time in general education. The fluidity of the program design allows the ISD and local LEA to increase staff support when it is anticipated that students with more intense needs will be joining the
Figure 2 � �Framework for the G.E.M.S. program G.E.M.S. (Giving Everyone More Support) PROGRAM GOALS
• Transition B.E.S.T. program students • Provide extra support for other special needs students in building • Offer general-education peer models • Collaboration and integration with general education environment and curriculum Student support across a full continuum of placements G.E.M.S. Room
Kindergarten
First Grade
Specials
Other School Settings
G.E.M.S. School-Based Team
Core Team Members • 1 teacher (with part-time consultant on sliding time scale) • 3 paraprofessionals (at least 1 person is floating at most times) • 1 inclusion teacher • 1 occupational therapist (1 hour/day) • 1 speech and language professional (1 hour/day) • 1 social worker (direct/consult per IEP) • 1 school psychologist (direct/consult per IEP) • Additional members, based on individual student needs
Team Activities • Receiving and addressing requests for problem solving • Regular planning time • Guiding evaluation of program
Support Accommodations Individualized Educational Plans (IEPs) Professional Development
Fall 2006
BB16(1).indd 27
27
10/23/06 1:10:23 PM
Integration of Evidence-Based Practices
Figure 3 � �Family assessment results 2002/2003–2003/2004 Student: Jared
��� ����
1FSDFOU�PG�1PTTJCMF�1PJOUT�
��
����
�� �� �� �� �� �� �� �� �
�
4PDJBM�#FIBWJPS
$PNNVOJDBUJPO
4FOTPSZ
)FBMUI �4BGFUZ �4FMG�)FMQ
�)JHI�TDPSFT�BSF�EFTJSBCMF�
program. The success of the G.E.M.S program required appropriate management of paraprofessional resources. Within the ISD, the historical precedent had been the provision of one-on-one paraprofessional support to assist special and general educators in supporting individual students with ASD. Typically, this decision was not driven by specific IEP needs, but by concerns about behavior and the “unique” needs of students with ASD. In reviewing the paraprofessional literature, the ISD recognized that: (a) this problem was not unique to the Huron ISD (Marks, Schrader & Levine, 1999); (b) one-on-one paraprofessionals were not automatically in the best interest of the child (Giangreco, Edelman, Luiselli, & McFarland, 1997; Giangreco, Yuan, McKenzie, Cameron & Fialka, 2005); (c) paraprofessionals were not being given sufficient training (Fox, 1998; Hammeken, 1996; National Association for the Education of Young Children, 1994; Giangreco, et al, 2005; Twachtman-Cullen, 2000) and yet, were
Figure 4 � �ABLLS assessment results 2002/2003–2003/2004 Student: Jared
��� ��
1FSDFOU�PG�1PTTJCMF�1PJOUT
�� �� �� �� �� �� �� �� � ��������� ���������
28
BB16(1).indd 28
3FDFQUJWF -BOHVBHF �� ��
1MBZ�BOE�-FJTVSF �� ��
4QPOUBOFPVT 7PDBMJ[BUJPOT �� ��
3FBEJOH
.BUI
5PMJFUJOH
8SJUJOH
�� ��
�� ��
� ��
�� OP�EBUB
Beyond Behavior
10/23/06 1:10:24 PM
BeyondBehavior
BB
Integration of Evidence-Based Practices
often the primary educators for these children (Boomer, 1994; Giangreco et al., 2005; Giangreco et al., 1997; Marks et al.,1999; National Association for the Education of Young Children, 1994); and (d) one-on-one paraprofessionals, who often possess the most information about the student, had the least say in programming decisions (Emery, 1991; Giangreco, Broer, & Edelman, 2001) and also often affected the communication cycle between parents and teachers. Review of the professional literature provided the team with the tools necessary to make changes in the use of paraprofessionals. These changes serve to reinforce the notion that the role of the paraprofessional is to aid teachers in delivering educational support to all students in the classroom and that individualized support should be determined solely by the IEP, not based on unresolved fears of bad behavior or due to lack of knowledge. The newly developed paraprofessional policy requires data-based decision making, linked to progress in curricular and IEP goals. Individual student data dictates the amount of paraprofessional support a student receives. All paraprofessional support is automatically faded and generalized across other adults unless studentspecific data dictates otherwise. This gradual shift in how paraprofessional support is utilized assists the ISD in providing adequate staffing and ensuring that adult dependency is not inadvertently fostered. As a result, paraprofessionals are no longer identified as “Jared’s” paraprofessional, but instead are associated with the programs and schools that hire them, in essence a part of the faculty and staff. Whenever possible, paraprofessional training is broadened to include the paraprofessionals at both the ISD and the local level. Conclusion The process of developing a programmatic framework grounded in research has created a foundation by which the visions for home–school partnerships, professional development, and service delivery are realized
with a new level of interconnectivity. The tangible benefits of this process have been plentiful and persistent. The impact on the ISD as a whole has included strengthened skills assessment and instructional strategies for all students. Additionally, the process has supported the use of evidenced-based practices within the ISD and, as a result, contributed to a broadened knowledge base by which to support LEAs serving populations considered more challenging. The practice of utilizing data-based decision making has been enhanced at the program and local levels and in collaboration with families. Employing an evidence-based curricular framework that guides practice, policy, and collaboration has proven effective in increasing opportunities for students with ASD, served by the ISD, to be successful in their home school districts. Additionally, the ISD is more successful at helping LEAs realize their potential in meeting the needs of more challenging students through extended and scaffolded professional development. Clearer processes for determining curricular focus and corresponding assessment measures have assisted LEAs in realizing improved student outcomes. By increasing planned opportunities for inclusion of students with ASD in their local school districts, general education peers have also reaped benefits. These peers are provided with increased opportunities to develop skills in problem solving, conflict resolution, communication, interpersonal relationships, and appreciating diversity within a contextually relevant and consistent environment. Perhaps most salient is the increased confidence expressed by ISD staff that programmatic curricular frameworks will truly align across early childhood, elementary, and secondary education for students with ASD. This has been the ISD’s goal for effective programming, and the impact on student outcomes provides the initial endorsement that programming is effective and meaningful.
Huron ISD has received positive feedback from the state through opportunities to present the programmatic model. The ISD has welcomed visitors from around the state to observe and provide feedback and to secure ongoing grant funding. The ISD still recognizes that this is a fluid model that will need to continually reflect the needs and strengths of the varied students served. The ISD continues to engage in long-term planning in order to adapt the service-delivery model and financial-support needs to the current population. The short- and long-term goals for the ISD include expanding and maintaining data-based decision models, further accessing and integrating community supports, and sustaining participation in regional collaborative networks. Additionally, the ISD continually works to stay abreast of the ever-expanding literature on effective practices. Although the day-to-day challenges persist, the ISD has grown in its efforts to meet the challenges, constructing a framework that serves as a guide as more students with varying needs enter and progress through the district. References
Alberto, P. A. & Troutman, A. C. (2003). Applied behavior analysis for teachers (7th ed.). New York: Merrill Publishing. Baker, M. J. (2000). Incorporating the thematic ritualistic behavior of children with autism into games: Increasing social play interactions with siblings. Journal of Positive Behavior Interventions, 2, 66–84. Bondy, A. & Frost, L. (2001). A picture’s worth: PECS and other visual communication. Bethesda, MA: Woodbine House. Bredekamp, S. & Cople, C. (Eds). (1997). Developmentally appropriate practice in early childhood programs (Rev. ed.). Washington, DC: National Association for the Education of Young Children. Brown, T., Iskow, J., & Richards, J. (2001). Buddy-enriched structured teaching: Best practices for students with autism model demonstration. Sub Grant Awarded by the State of Michigan, Fall, 2001. Brown, W. H. & Conroy, M. A. (2002). Promoting peer-related social-
Fall 2006
BB16(1).indd 29
29
10/23/06 1:10:25 PM
Integration of Evidence-Based Practices
communicative competence in preschool children. In H. Goldstein, L. Kaczmarek, & K. M. English (Eds.), Promoting social communication in children and youth with developmental disabilities (pp. 173–210). Baltimore: Brookes Publishing. Carr, E. G., Levin, L., McConnachie, G., Carlson, J. I., Kemp, D. C., & Smith, C. E. (1994). Communication-based intervention for problem behavior: A user’s guide for producing positive change. Baltimore, MD: Brookes Publishing. Center for Disease Control and Prevention (2005). About autism. Retrieved September 23, 2005, from http://www. cdc.gov/ncbddd/autism/. Charlop-Christy, M. H., Carpenter, M., Le, L., LeBlanc, L. A., & Kellet, K. (2002). Using the Picture Exchange Communication System (PECS) with children with autism: Assessment of PECS acquisition, speech, socialcommunicative behavior and problem behavior. Journal of Applied Behavior Analysis, 35, 213–231. Charlop-Christy, M. H., Schreibman, L., Pierce, K., & Kuntz, P. F. (1998). Childhood autism. In Richard J. Morris & Thomas R. Kratochwill (Eds.), The practice of child therapy (3rd ed., pp. 271–302). Needham Heights, MA: Allyn & Bacon. Dawson, G. & Osterling, J. (1997). Early intervention in autism. In M. Guralnick (Ed.), The effectiveness of early intervention (pp. 307–326). Baltimore: Brookes Publishing. Dunlap, G. (1999). Consensus, engagement, and family involvement for young children with autism. Journal of the Association for Persons with Severe Handicaps, 24, 222–225. Dunlap, G. & Fox, L. (1999). A demonstration of positive behavior support for young children with autism. Journal of Positive Behavior Support, 1, 77–87. Earles, T. L., Carlson, J. K., & Bock, S. J. (1998). Instructional strategies to facilitate successful learning outcomes for students with autism. In R. L. Simpson & B. S. Myles (Eds.), Educating children and youth with autism: Strategies for effective practice (pp. 55–111). Austin, TX: Pro-Ed. Emery, M. J. (1991). Building team pride: Teachers and paraeducators working together. Columbia: University of Missouri. Fox, G. (1998). A handbook for learning support
30
BB16(1).indd 30
assistants: Teachers and assistants working together. London: David Fulton. Gersten, R., Chard, D., & Baker, S. (2000). Factors enhancing sustained use of research-based instructional practices. Journal of Learning Disabilities, 33, 445–457. Giangreco, M. F., Broer, S. M. & Edelman, S. W. (2001). Teacher engagement with students with disabilities: Differences between paraprofessional delivery models. Journal of the Association for Persons with Severe Handicaps, 26, 75–86. Giangreco, M. F., Edelman, S. W., Luiselli, T. E., & McFarland, S. Z. C. (1997). Helping or hovering? Effects of instructional assistant proximity on students with disabilities. Exceptional Children, 64, 7–18. Giangreco, M. F., Yuan, S., McKenzie, B., Cameron, P. & Fialka, J. (2005). Be careful what you wish for: Five reasons to be concerned about the assignment of individual paraprofessionals. Teaching Exceptional Children, 37, 28–34. Greenspan, S. I. (2000). Working with children who have developmental delays. Early Childhood Today, 15, 32–34. Greenspan, S. & Wieder, S. (1997). Developmental patterns and outcomes in infants and children with disorders in relating and communicating: A chart review of 200 cases of children with autism spectrum diagnoses. Journal of Developmental and Learning Disorders, 1, 87–141. Grindle, C. & Remington, B. (2002). Discrete trial training for children when reward is delayed: A comparison of condition cue value and response marking. Journal of Applied Behavior Analysis, 35, 187–190. Hammeken, P. A. (1996). Inclusion: An essential guide for the paraprofessional: A practical reference tool for all paraprofessionals working in inclusionary settings. ERIC document 402720. Peytral Publications, MN: Resources in Education. Heflin, L. J. & Alberto, P. A. (2001). Establishing a behavioral context for learning for students with autism. Focus on Autism and Other Developmental Disabilities, 16, 93–101. Horner, R. H. (2000). Positive behavior supports. Focus on Autism and Other Developmental Disabilities, 15, 97–105. Hurth, J., Shaw, E., Izeman, S. G., Whaley, K., & Rogers, S. J. (1999). Areas of agreement about effective practices among programs serving young
children with autism spectrum disorder. Infants and Young Children, 12, 17–26. Individuals with Disabilities Education Act Amendments of 2004, 20 U.S.C. § 1401. 107th Congress, 2nd Session. Retrieved November 7, 2005, from http://thomas. loc.gov/cgi-bin/cpquery/T?&report=hr 779&dbname=cp108&. Iovannone, R., Dunlap, G., Huber, H., & Kincaid, D. (2003). Effective educational practices for students with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 18, 150–165. Koegel, R. L. & Koegel, L. K. (1995). Teaching children with autism: Strategies for initiating positive interactions and improving learning opportunities. Baltimore: Brookes Publishing. Koegel, R. L., Koegel, L. K., & Schreibman, L. (1991). Assessing and training parents in teaching pivotal behaviors. In R. Prinz (Ed.), Advances in behavioral assessment of children and families: Vol. 5. A research annual (pp. 65–82). Philadelphia: Jessica Kingsley Publishers. Lauschey, K. M. & Heflin, L. J. (2000). Enhancing social skills of kindergarten children with autism through the training of multiple peers as tutors. Journal of Autism and Developmental Disorders, 30, 183–193. Lorimer, P. A., Simpson, R. L., Myles, B. S., & Ganz, J. B. (2002). The use of social stories as a preventative behavioral intervention in a home setting with a child with autism. Journal of Positive Behavior Interventions, 4, 53–60. Lovaas, O. I. & Buch, G. (1997). Intensive behavioral intervention with young children with autism. In N. Singh (Ed.), Prevention and treatment of severe behavior problems: Models and methods in developmental disabilities (pp. 61–86). Belmont, CA: Brooks/Cole. Marcus, L., Schopler, E., & Lord, C. (2000). TEACCH services for preschool children. In J. S. Handleman & S. L. Harris (Eds.), Preschool education programs for children with autism. Austin, TX: Pro-Ed. Marks, S. U., Schrader, C., & Levine, M. (1999). Paraeducator experiences in inclusive settings: Helping, hovering, or holding their own? Exceptional Children, 65, 315–328. McClanahan, L. E. & Krantz, P. J. (1999). Activity schedules for children with autism: Teaching independent behavior. Bethesda,
Beyond Behavior
10/23/06 1:10:26 PM
Integration of Evidence-Based Practices
MD: Woodbine House. National Association for the Education of Young Children (1994). NAEYC position statement: A conceptual framework for early childhood professional development. Young Children, 49, 68–77. National Research Council (2001). Educating children with autism. Washington, DC: National Academy Press. Nutall, J. R. (2002). Twenty-five years of special education in Michigan: Statistical tables of the special education unduplicated child count from 1975 to 2001. 2002 Annual Report to the Michigan Department of Education. Odom. S. L., Brown, W. H., Frey, T., Karasu, N., Smith–Cantor, L. L., & Strain, P. S. (2003). Evidence-based practices for young children with autism: Contributions for single-subject design research. Focus on Autism and Other Developmental Disorders, 18, 166–175. Odom, S. L. & Strain, P. S. (1986). A comparison of peer-initiated and teacher-antecedent interventions for promoting reciprocal social interaction of autism preschoolers. Journal of Applied Behavior Analysis, 19, 59–72. Olley, J. G. (1999). Curriculum for students with autism. School Psychology Review, 28, 595–606. Partington, J. W. & Sundberg, M. L. (1998) The Assessment of Basic Language and Learning Skills (ABLLS). Pleasant Hill, CA: Behavior Analysts, Inc. Prizant, B. & Rubin, E. (1999). Contemporary issues in interventions for autism spectrum disorders: A commentary. Journal of the Association for Persons with Severe Handicaps, 24, 199–208. Rosenkoetter, S. E. & Fowler, S. A. (1986). Teaching mainstreamed children to manage daily transitions. Teaching Exceptional Children, 19, 20–23. Schopler, E., Mesibov, G. B., & Hearsey, K. (1995). Structured teaching in the TEACCH system. In E. Schopler & G.
Mesibov (Eds.), Learning and cognition in autism (pp. 243–267). New York: Plenum Press. Schreibmann, L. & Koegel, R. L. (1996). Fostering self-management: Parentdelivered pivotal response training for children with autistic disorder. In E. D. Hibbs & P. S. Jensen (Eds.), Psychosocial treatments for child and adolescent disorders: Empirically based strategies for clinical practice (pp. 525–552). Washington, DC: American Psychological Association. Shipley-Benamou, R., Lutzker, J. R., & Taubman, M. (2002). Teaching daily living skills to children with autism through instructional video modeling. Journal of Positive Behavior Interventions, 4, 165–175. Simpson, R. L. (2004). Inclusion of students with behavior disorders in general education settings: Researcher and measurement issues. Behavioral Disorders, 30, 19–31. Simpson, R. L. (2005). Evidence-based practices and students with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 20, 140–149. Smith, T. & Lovaas, O. I. (1998). Intensive and early behavioral intervention with autism: The UCLA young autism project. Infants and Young Children, 10, 67–78. Smith, B. J., Strain, P. S., Snyder, P., Sandall, S. R., Mclean, M. E., Broudy-Massey, W. C. et al. (2002). DEC recommended practices: A review of 9 years of EI/ECSE research literature. Journal of Early Intervention, 25, 108–120. Sparrow, S. S., Balla, D., & Cichetti, D. (1984). Vineland adaptive behavior scales (Rev. ed.). Circle Pines, MN: American Guidance Service. Stahmer, A. C. (1995). Teaching symbolic play skills to children with autism using pivotal response training. Journal of Autism and Developmental Disabilities, 25, 123–141.
BeyondBehavior
BB
Stichter, J. & Conroy, M. (2005). How to teach social skills and plan for peer social interactions with learners with autism spectrum disorders. Austin, TX: Pro-Ed. Strain, P. S. & Cordisco, L. K. (1994). LEAP Preschool. In S. Harris & J. Handleman (Eds.), Preschool education programs for children with autism (pp. 225–252). Austin, TX: Pro-Ed. Strain, P. & Hoyson, M. (2000). The need for longitudinal, intensive social-skill intervention: LEAP follow-up outcomes for children with autism. Topics in Early Childhood Special Education, 20, 116–122. Thorp, D. M., Stahmer, A. C., & Schreibman, L. (1995). Effects of sociodramatic play training on children with autism. Journal of Autism and Developmental Disorders, 25, 265–282. U.S. House of Representatives. (2005). Special education children with autism. Report to the Subcommittee on Human Rights and Wellness, Committee on Government Reform. Washington, DC: Author. Available from www.gao.gov. Van Bourgondien, M. E., Reichle, N. C., & Schopler, E. (2003). Effects of modal treatment approach on adults with autism. Journal of Autism and Developmental Disorders, 33, 31–40. Retrieved September 19, 2005, from ERIC database. Volmer, L. (1997). Best practices in working with students with autism. In A. Thomas & J. Grimes (Eds.), Best practices in school psychology (pp. 1031–1038). Washington, DC: National Association of School Psychologists. Wolery, M. & Winterling, V. (1997). Curricular approaches to controlling severe behavior problems. In N. N. Singh (Ed.), Prevention and treatment of severe behavior problems: Models and methods in developmental disabilities (pp. 87–120). Belmont, CA: Brooks/Cole. Zimmerman, I. L., Steiner, V., & Pond, R. E. (1992). Preschool language scale–3. San Antonio, TX: Psychological Corp.
Fall 2006
BB16(1).indd 31
31
10/23/06 1:10:27 PM
Integration of Evidence-Based Practices
Appendix A
12 Tenets of Practice for Young Children with ASD 1. Focus on individual child When working with children and families, the target question is, “What is the best approach for a given child and family?” Each child and family is addressed individually and characterized according to their unique profile. The selected educational approach is to be tailored to the child, rather than attempting to fit the child to an identified program (Dunlap, 1999; Greenspan, 2000; Hurth et al., 1999).
determining curriculum, interventions, and classroom environment/structure. (Charlop–Christy, Carpenter, LeBlanc, & Kellet, 2002; Marcus, Schopler, & Lord, 2000; Strain & Hoyson, 2000).
7. Appropriate continuum of interventions The intervention approaches consider each child’s current developmental level, his or her profile of learning strengths and weaknesses, family priorities, and the “fit” of the intervention approach with the “culture” 2. Partnership with family and lifestyle of the family. Intervention strategies The educational team encourages families to promote are individualized to match a child’s profile across developmental change by embedding developmentally developmental domains (i.e., motor, sensory, social, appropriate change strategies in their natural routines. The cognitive, communicative) (Olley, 1999; Prizant & Rubin, family is involved in assessment, planning, interventions, 1999). Approaches that are limited in practice to one or two and training (Dunlap & Fox, 1999; NRC, 2001; Odom et al; modalities of intervention increase the risk of not meeting 2003; Prizant & Rubin, 1999). significant developmental needs of some children (Odom et al., 2003). 3. Multidisciplinary/collaborative approach Because all developmental domains (e.g., communication, 8. Instructional strategies/environmental supports cognition, social, sensory, motor) are assessed and multiple The classroom instructional strategies and environmental modalities of intervention may be beneficial for a child, supports address the need to provide predictability and related service practitioners (e.g., speech and language routine, generalization opportunities, scaffolding, high pathologist, occupational therapist, school psychologist, structure, reduced stimuli, use of visual cues, functional school social worker) are included as members of approaches to behavioral issues, and transitional services the educational team (NRC, 2001). Team members to future classrooms/programs (Dawson & Osterling, communicate openly, sharing knowledge, skills, and 1997; Earles, Carlson, & Bock, 1998; Heflin & Alberto, 2001; responsibilities across disciplinary and environmental Volmer, 1997). boundaries (Dawson & Osterling, 1997; Prizant & Rubin, 9. Individualized and contextually relevant curriculum 1999; Simpson, 2004). Parents are included as members of The curriculum is individualized and contextually the child’s educational team. relevant for each child. The curriculum includes an 4. �Comprehensive developmental assessment/ongoing emphasis on the development of functional competencies and incorporates modifications to the traditional academic monitoring of progress curriculum (Dawson & Osterling, 1997; Hurth et al, 1999; The educational team conducts comprehensive NRC, 2001; Odom et al. 2003). assessments that involve all relevant functional areas, including a child’s individual processing differences, 10. Participation in an inclusive environment functional developmental level, child–caregiver Integrated situations represent the optimal environment interactions, and family functioning. Ongoing assessment for the effective development and maintenance of and data collection (i.e., describing the child’s functioning functional living skills, communication, and social over time in multiple contexts) is incorporated into each relationships for children with ASD (Alberto & Troutman, child’s program to monitor progress. (Greenspan, 2000; 2003; Dawson & Osterling, 1997; IDEA, 2004). Hurth et al., 1999; Iovannone, Dunlap, Huber, & Kincaid, 2003). 11. �O ngoing collaboration/professional development/ administrative support of team 5. Longitudinal and dynamic planning Time and resources that support both opportunities for The educational team generates a collective vision for the team collaboration and professional development for child’s future and develops an action plan that enables the team members are a priority for program administrators child to gradually progress toward that vision. The vision (Brown, Iskow, & Richards, 2001; Gersten, Chard, & Baker, and plan are adapted on an ongoing basis in response to 2000; Simpson, 2004). variations in the setting and the changing needs of the child. (Dawson & Osterling, 1997; Iovannone et al, 2003; 12. Program evaluation NRC, 2001). Ongoing evaluation of programs and services is critical to assessing the effectiveness of the early childhood program 6. Social, behavior, and communication emphases and planning for excellence in services to children Because social, behavior, and communication domains are with ASD (Brown, Iskow, & Richards, 2001; NRC, 2001; core deficit areas for children with ASD, educators must Simpson, 2005). consciously consider and emphasize these areas when
32
BB16(1).indd 32
Beyond Behavior
10/23/06 1:10:28 PM