Clin Oral Invest DOI 10.1007/s00784-017-2174-3
ORIGINAL ARTICLE
Approximal morphology as predictor of approximal caries in primary molar teeth A. Cortes 1,2 & S. Martignon 1,3 & V. Qvist 2 & Kim Rud Ekstrand 2
Received: 14 June 2016 / Accepted: 28 June 2017 # Springer-Verlag GmbH Germany 2017
Abstract Objective To evaluate the predictive power of the morphology of the distal surface on 1st and mesial surface on 2nd primary molar teeth on caries development in young children. Sample and methods Out of 101 3-to 4-year-old children from an on-going study, 62 children, for whom parents’ informed consent was given, participated. Upper and lower molar teeth of one randomly selected side received a 2-day temporarily separation. Bitewing radiographs and silicone impressions of interproximal area (IPA) were obtained. One-year procedures were repeated in 52 children (84%). The morphology of the distal surfaces of the first molar teeth and the mesial surfaces on the second molar teeth (n=208) was scored from the occlusal aspect on images from the baseline resin models resulting in four IPA variants: concave-concave; concave-convex; convex-concave, and convex-convex. Approximal caries on the surface in question was radiographically assessed as absent/ present. Results Of the 52 children examined at follow-up, 31 children (60%) had 1–4 concave surfaces. In total 53 (25%) of the 208 surfaces were concave. A total of 22 children (43%) had 1–4 approximal lesions adding up to 59 lesions. Multiple logistic regression analyses disclosed that gender, surface morphology on one of the approximal surfaces (focus-surface), and * Kim Rud Ekstrand
[email protected] 1
UNICA - Caries Research Unit, Research Vice-rectory, Universidad El Bosque, Bogotá, Colombia
2
Cariology & Endodontics, Department of Odontology, Faculty of Health and Medical Sciences, University of Copenhagen, Nørre Allé 20, Copenhagen, Denmark
3
Dental Innovation and Translation Centre, Dental Institute, King’s College London, London, UK
adjacent-surface morphology were significantly related to caries development (p values ≤ 0.03). The odds ratio for developing caries in the focus-surface/adjacent-surface in the four IPA variants were convex-convex, 1.0; convex-concave, 5.5 (CI 2.0–14.7); concave-convex, 12.9 (CI 4.1–40.3); and concave-concave, 15.7 (CI 5.1–48.3). Conclusion Morphology of approximal surfaces in primary molar teeth, in particular both surfaces being concave, significantly influences the risk of developing caries. Clinical relevance The concave morphology of approximal surfaces can predict future caries lesions supporting specific home-care and in-office preventive strategies. Keywords Morphology . Dental caries . Radiography, bitewing . Tooth, deciduous . Risk assessment
Introduction Although the prevalence of caries in many countries has declined over the last two or three decades, there are still surfaces in both dentitions that are more prone to caries than others. In a study from Denmark using clinical caries recordings from children and adolescents, the occlusal surface on permanent first molar teeth was the surface that most often had DMFS scores >0 (decayed; missed; filled; surfaces) at the age of 18 years. In the primary dentition, both at the age of 3 and 9 years, the occlusal surface on the 1st and 2nd primary molar teeth most often had DMFS scores >0 (decayed; missed; filled; surfaces), closely followed by the adjacent distal surface on 1st primary molar teeth and the mesial surface of 2nd primary molar teeth [1]. However, it should be underlined that children in Denmark are recognized as having low caries experience [2]. Unfortunately, very few epidemiological studies have been performed on children below the age of 5 years.
Clin Oral Invest
Longitudinal data from a study in Scotland on children 1 to 4 years old also showed that the molar teeth are the risk teeth in the primary dentition [3, 4]. Thus, in the 4-year olds, about 25% of the primary molar teeth had DMFS ≥1. Data from a longitudinal epidemiological study on 2- and 4-year-old children from Bogota in Colombia also showed that the primary molar teeth, together with the upper incisor teeth, are caries risk teeth. When data from radiographs were included and the children became 4 and 6 years old, the distal surface on the 1st primary and the mesial surface on the 2nd primary molar teeth were identified as the caries risk surfaces together with the occlusal surfaces on the same teeth [5, 6]. In a Danish study from 2005 on 4–6-year-old children, it was concluded that plaque accumulation, bleeding on probing, and surface-formed contact (broad contact area) between the primary molar teeth were useful predictors for approximal caries in the primary dentition [7]. In his textbook, Carlsen [8] described that the approximal surfaces of permanent and primary molar teeth can be convex or concave in the buccolinqual direction as well as in the occluso-cervical direction. In the current study, we therefore took a step further and hypothesized that the macro-morphology of the approximal surfaces in the interproximal contact area between 1st and 2nd primary molar teeth plays a role for these surfaces being prone to caries and that the morphology can be used as a clinical caries predictor along with e.g., a surface-formed contact between primary molar teeth. The aim of this study was to evaluate the predictive power of the morphology of the distal surface on 1st primary molar teeth and the mesial surface on 2nd primary molar teeth on caries development in young children.
Subjects and methods The project was approved by the Ethical Board in El Bosque University (UEB 129-2011). Sample The participants in this study were already part of a 2-year epidemiological study with an examination of 200 children aged 2–3 years in 2012, continuing with re-examinations in 2013 and 2014 [5, 6]. The children went to kindergartens in Bogota that had been involved in cooperation with El Bosque University on other occasions, but the children did not follow a preventive program. The participants in the present study were selected among the 101 children who were present at the re-examination in 2013 (baseline for the present study). The parents/caregivers were invited to participate in the current study and asked to sign and return an informed consent form. Figure 1 shows the flow diagram of the study, and a total
of 71 children had a baseline examination conducted for the present study. The children’s parents were low and medium socioeconomic status. Colombian population has access to systemic fluoride program that include salt fluoridation (180– 220 mg F/Kg of salt). At baseline, (a) 70% of the children had a Löe & Silness plaque index of 0 or 1 according to the Cariogram [9]; (b) 90% used fluoridated toothpaste (which contained 1100 ppm of fluoride) and brushed two or more times per day with supervision of an adult; and (c) a high frequency of sugared beverages and snacks consumption (≥6 intakes per day according to the Cariogram) [9] was found in more than 90% of the children.
Clinical and radiographic procedures A portable dental unit was brought to the institutions where the examinations took place. To determine caries experience, clinical assessment was performed, including all teeth and surfaces, using the ICDAS-ICCMS™ epi system (depi) [5, 6] by a trained examiner (AC). Surfaces were eventually staged as sound (S); initial (epi): ICDAS 1/2, (there was no access to three-in-one syringes at the institutions); moderate (M): ICDAS 3 and 4; or extensive (E): ICDAS 5 and 6 according to the ICCMS™ classification system [10]. Missed (m) or filled (f) surfaces were also assessed. Children with cavitated caries lesions (ICDAS score 5 and/ or 6) in the distal surface of the 1st molar and/or mesial surface on 2nd primary molar teeth were excluded (Fig. 1). The remaining 67 children had two additional appointments. At the first appointment, the 1st and 2nd upper and lower primary molar teeth in the right or left side of the mouth were temporarily separated with an elastic band (0.8 mm) for 2 days. The side was selected at chair-side using a random number table. At the second appointment, 2 days later, the elastic band was removed and the separation space was measured with a digital caliper (Stainless Steel Electronic LCD Digital Vernier Caliper 0–6). The distal and mesial surfaces were cleaned, and silicone impressions of the approximal contact areas were taken (Honigum® light fast—DMG®). The impressions were cleaned and stored each in a separated plastic bag marked with the patient code, mouth side, and tooth surfaces. At the end of the second appointment, bitewing radiographs were taken, following the EAPD radiograph protection guidelines standards for children [11], using mobile radiographic equipment (X-PORT II Model, EZX-60®), and high speed Kodak conventional films (size 1) with bitewing-radiograph holders (XCP Bitewing aiming ring-red Dentsply™). Five additional children had to be excluded because the elastic band could not be inserted; the child had lost the band or radiographs could not be taken. The baseline sample, thus, comprised 62 children (Fig. 1). Parents/caregivers received written information
Clin Oral Invest Fig. 1 Flow diagram of the study
Enrollment 2013
3-4 years old children participating in another study were invited to participate (n=101) The caries experience was assessed initially by the Clinical ICDAS-ICCMS™ (ICDAS Foundation, 2013)
Inclusion/Exclusion
Baseline 2013
71.2% of the invited children’s parents signed and returned an informed consent to participate (n=71)
Children not meeting inclusion criteria were excluded (n=4): mesial or distal surfaces with cavitated caries lesions
Sample: n=67 One side of the mouth (right or left) was randomly selected Appoinment 1
1st and 2nd upper and lower primary molar teeth, went through a 2-day elective temporarily separation Elastic bands were removed and the separation space was measured with a digital caliper.
Appoinment 2 /Exclusion
The distal and mesial surfaces were cleaned and dried, and silicone impressions of the interproximal area were taken Bitewing radiographs were taken Children not having the elastic band or (n=5) were excluded
Final sample: n=62 Lost to 1-year follow-up (n = 10) No reached after trying phone calls or kindergarten visits
1-year follow-up Follow-up sample: n=52 2014
Appoinments 1 and 2
about the child’s dental health status after the second appointment. About 1 year later, 52 children (84%), now 4–5 years old, turned up for the repeated clinical and radiographic examination (Fig. 1). The same upper and lower primary molar teeth were temporarily separated with an elastic band and impressions and radiographs were taken after 2 days. Study models from the impressions Resinmodels(StruersEpoxicResinKitSpeciFix-20™)weremade from the silicone impressions. Stereomicroscopic (1.6 times magnification) images of the models (Stereo DiscoveryV8 Zeizz® and DeltaPixCameraandSoftware®)weretakenina90° angle,from an occlusal-cervical direction, facing the interproximal area (IPA) between the 1st and 2nd molar teeth in the upper and lower jaw. The images were stored in a computer. Initially, two of the authors (AC and KRE) went through three training sessions where about 50% of the images were examined (baseline models as well as models from the final impressions) in order to calibrate in assessing if the surfaces in question were concave or convex. The sessions were performed in a dark room. Four weeks later, the two examiners individually scored the distal surface on 1st primary molars and the mesial surface on 2nd primary molars as showing a concave or convex morphological appearance. For this purpose, the 104 baseline images belonging to the 52 children who fulfilled the final examination were scored (Fig. 1). The IPA morphology was accordingly classified form distal to mesial as convex-convex, convex-concave, concave-convex, or concave-concave (Fig. 2). After one more week, the two
Caries experience was determined at the 4-5 years old (depiMEmfs)
Were conducted as in baseline radiographs were also taken.
examiners repeated their assessments (individually) of the full sample. Radiographic examination Prior to the radiographic recordings of caries, one external examiner and KRE received a 2-day theoretical and clinical training course in the ICDAS-ICCMS™ radiographic scoring system, conducted by a trained examiner (SM). Radiolucency, in the distal surface of the 1st primary molar teeth and the mesial surface of the 2nd primary molar teeth, was staged according to the radiolucency as [6, 10, 12] RdS=no radiolucency (sound); RdA=radiolucency in outer 1/2 of the enamel or in inner 1/2 of the enamel ± EDJ or radiolucency in the outer 1/3 of the dentine; RdB=radiolucency in the middle 1/3 of dentine; or RdC=radiolucency in the inner 1/3 of dentine or into the pulp. RdA, RdB, and RdC are termed initial, moderate, or extensive staged lesions [5, 6, 10]. Filled (f) and missed (m) surface were also assessed. All radiographs taken at baseline and follow-up examination were analyzed and scored independently by the external examiner and by KRE. The assessments were repeated on the full sample about 1 week after the first assessments. Statistical analysis The reproducibility of the clinical recordings is reported in Cortes et al. [6]. The term CdepiME means that all lesions are included in the index, while CdME means that only moderate (M) and extensive (E) lesions (ICDAS 3 to 6) are included in the index
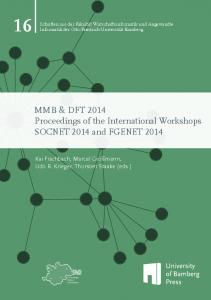
Clin Oral Invest Fig. 2 Classification of interproximal area (IPA) surface morphology of adjacent, primary molar teeth
Convex-Convex
Convex-Concave
1st molar
2nd molar
1st molar
2nd molar
1st molar
2nd molar
1st molar
2nd molar
Distal Surface
Mesial Surface
Distal Surface
Mesial Surface
Distal Surface
Mesial Surface
Distal Surface
Mesial Surface
Convex mesial and distal surfaces with minor plaque retention morphology in both surfaces
(traditional DMFS-index, Table 1). Using the Wilcoxon signed Rank test [13], the mean caries experience of the 10 children who left the study was compared with the mean of the 52 children who remained in the study and both recorded at baseline. Unweighted Kappa with 95% confidence interval was used to express the examiners’ inter- and intra-reproducibility concerning the classification of the morphology using the images from models prepared from baseline impressions. For the inter-examiner reproducibility calculation, the first data set for both examiners were used. Unweighted Kappa was used to express the examiners’ inter- and intra-examiner reproducibility of the radiographic scoring system. For the inter-examiner reproducibility calculation, the first data set from both examiners was used. As analyses disclosed that 75% of the lesions were scored as RdA but only restricted to the enamel, it was decided to report the radiographic assessment as absence or presence of caries lesion. In the statistical analyses, the approximal surfaces were included as a focus-surface as well as an adjacent-surface. Chi-square and Fisher’s exact tests were used to test if the approximal surface morphology, and the occurrence of caries were associated to tooth surfaces and if the occurrence of caries differed among concave and convex surfaces.
Concave-Convex
Concave mesial or distal surfaces with plaque retention morphology in one surface only
Concave- Concave
Concave mesial and distal surfaces with plaque retention morphology in both surfaces
On the surface level, multiple logistic regression analysis based on the generalized estimating equation (GEE) with backward elimination of variables (p > 0.05) was used to estimate the effect of different predictor variables on caries development. The patient was used as cluster variable in the analysis. The independent predictor variables were gender (boy/girl); age at final examination (45–54/55–58/59–65 months); plaque at baseline (no=scores 0 and 1; yes=scores 2 and 3—Cariogram [9]); use of fluoridated toothpaste at baseline (no/yes); sugar consumption at baseline (limited=scores 0 and 1; high=scores 2 and 3— Cariogram [9]); CdMEmfs at baseline (0 />0); CdMEmfs increase from baseline to final examination (0/>0); tooth type (1st molar/ 2nd molar); side (right/left); jaw (upper/lower), side (right/left); morphology of the focus-surface (convex/concave); and morphology of the adjacent-surface (convex/concave). The dependent outcome variable was radiographic presence of caries in the approximal focus-surface at the follow-up examination. The results were expressed by odds ratios with corresponding 95% confidence intervals. Eventually, the associations between radiographic caries and the significant outcome were expressed by odds ratios with corresponding 95% confidence intervals. The significance level was set at 5%. Data analyses were carried out using IBM SPSS Statistics (Version 22.0.01, USA).
Table 1 Prevalence and mean caries experience at baseline and follow-up examination
Prevalence and mean of caries experience
Age Baseline (n = 62) Follow-up (n = 52)
± = standard deviation
Caries experience Prevalence Mean (±) Prevalence Mean (±)
Clinical CdMEmfs 31% 1.8 ± 3.7 39% 2.2 ± 4.2
CdepiMEmfs 47% 4.0 ± 4.9 52% 4.0 ± 5.7
Clinical and radiographic C+RdMEmfs C+RdepiMEmfs 40% 60% 2.2 ± 3.6 4.2 ± 4.7 47% 60% 4.3 ± 3.4 5.1 ± 4.3
Clin Oral Invest
Results
Radiographic assessment
After receiving 71 consent forms by parents, a total of 67, 3 and 4 years old, children were enrolled in this study. The 4 children not included had extensive cavitated lesions in the distal surface of the 1st molar and/or mesial surface on 2nd primary molar teeth and were subsequently excluded and referred for invasive treatment. The mean number of teeth present at the time of the examination was 20 teeth.
At baseline examination, 5 of the 62 children (8%) showed approximal caries lesions, while 22 of the 52 children (42%) showed one or more approximal lesions at the follow-up examination. Additional analyses showed that 50% of the 13 children with one concave surface, 69% of the 12 children with two concave surfaces, and all 6 children with three or four concave surfaces had developed at least one caries lesion. In comparison, only 1 of the 21 children with no concave surfaces on the distal of 1st or mesial of 2nd molar teeth showed approximal lesions. Furthermore, this particular child had developed caries on all four surfaces. Of the 208 approximal surfaces examined at follow-up, 149 surfaces were sound radiograpically (and clinically) (72 distal surfaces and 77 mesial surfaces) and 59 showed caries lesions radiographically. The lesions were distributed with 1, 2, 3, and 4 lesions in 5, 4, 2, and 10 children, respectively. A total of 56 lesions were staged as initial=RdA; 12 in the outer ½ of the enamel; and 44 in the inner ½ of the enamel ±DJ, 2 lesions were staged as moderate=RdB (middle 1/3 of the dentine) and 1 lesion as extensive=Rdc (inner third of the dentine). The caries prevalence varied between 38% (18 out of 52 surfaces) for the distal surfaces of the upper 1st primary molar teeth (tooth 54/64) to 25% (13 out of 52 surfaces) for the mesial surfaces of the upper 2nd molar teeth (tooth 55/65) (p = 0.71). The caries prevalence in first and second molar teeth (p = 0.54), teeth in the upper and lower jaw (p = 0.76) or the right and left side of the mouth (p = 0.76) were not significant either. However, occurrence of caries was strongly associated with surface morphology (p < 0.001) (Table 3).
Reproducibility Using weighted Kappa the intra-examiner reproducibility for the clinical scores was 0.81 [6]. The inter-examiner reproducibility (Kappa) for the morphological assessment was 0.79 (CI = 0.69–0.88), and the intra-examiner reproducibility was 0.84 (CI = 0.76–0.92) and 0.79 (CI = 0.69–0.89). For the radiographic assessments, the values were 0.78 (CI = 0.67– 0.87) (inter-examiner reproducibility), 0.84 (CI = 0.76–0.93) and 0.77 (CI = 0.66–0.86). Caries experience At baseline, 31% of the children had a CdMEmfs ≥ 1, increasing to 39% at the follow-up examination (Table 1). When including the findings from the radiographs C + RdMEmfs ≥ 1, the corresponding figures were 40% (baseline) and 47% at follow-up. At baseline, the mean caries experience in terms of CdMEmfs and CdepiMEmfs was 1.8 ± 3.7 and 4.0 ± 4.9. The CdMEmfs and CdepiMEmfs mean caries experience for the 10 children who were lost during the study period were 2.3 ± 3.2 and 4.4 ± 5.3, respectively, which did not differ from the baseline mean of the 52 children who remained in the study (p = 0.84 and 0.85). The caries experience increased when the observations from the radiographs were included. For example, the mean for CdMEmfs at follow-up was of 2.2 ± 4.2 and when C + RdMEmfs was used as index, it increased to 4.3 ± 3.4 (Table 1). Morphology characteristics The separation space between primary molar teeth after 2 days was 0.7 ± 0.1 mm. Twenty-one children (40%) had no approximal concavities, and 31 (60%) had one to four concave approximal surfaces. As seen in Table 2, a total of 155 (75%) of the 208 examined approximal surfaces were convex (82 from the upper and 73 from the lower jaw) and 53 (25%) surfaces were concave (22 from the upper and 31 from the lower jaw). The analyses disclosed that concave and convex surfaces were equally distributed among the surfaces in question (p = 0.51). Further, no differences in morphology were found between teeth in the upper and lower jaw (p = 0.20), right and left side of the mouth (p = 0.34), or first and second primary molar teeth (p = 0.75).
Regression analyses Twenty-four (15%) of the 155 convex test surfaces developed caries lesions compared to 35 (66%) of the 53 concave test surfaces (Table 2). The multifactorial logistic regression analysis showed that gender (p = 0.03), the morphology of the focus-surface (p < 0.001), and the morphology of the adjacent-surface (p = 0.002) played a significant role for caries development in the present sample (Table 3). The corresponding OR value for caries development in girls was 4.2 compared to boys. The OR value was 6.8 when the focus-surface was concave and not convex, and 2.6 if the adjacent-surface was concave versus convex. None of the other predictive variables included in the multivariate analysis were of significant influence on the development of approximal caries (p = 0.07–0.92; Table 3). The influence of the interproximal morphology with regard to the four IPA variants (concave-concave, concave-convex, convex-concave, and convex-convex) is
Clin Oral Invest Table 2 Distribution of concave and convex approximal surfaces at baseline and presence of caries lesions at follow-up on approximal surfaces in the first and second primary molar teeth
Tooth
Surface n
Concave surfaces
Caries lesions
Convex surfaces
Caries lesions
n
n
n
n
(%)
(%)
(%)
54
Distal
28
9
32
8
89
19
68
2
11
55 64
Mesial Distal
28 24
6 3
21 13
2 3
33 100
22 21
79 88
3 5
14 24
65
Mesial
24
4
17
4
100
20
83
4
20
74 75
Distal Mesial
24 24
7 8
29 33
4 5
57 63
17 16
71 67
4 3
24 19
84
Distal
28
9
32
5
56
19
68
1
5
85
Mesial Total
28 208
7 53
25 25
4 35
57 66
21 155
75 75
2 24
10 15
presented in Table 4, with convex-convex IPA as reference (OR = 1). The OR for the other IPA variants increased from 5.5 for convex-concave to 12.9 for concave-convex, and 15.7 for concave-concave IPA reflecting the significant influence of the morphology of the focussurface as well as the morphology of the adjacent-surface (Table 4).
Table 3 Logistic regression analyses of caries development in the first and second primary molar teeth with distribution between categories of significant variables, odds ratio (OR), 95% confidence interval (CI), and p values
(%)
Variable
Discussion At the time of baseline examination in the current study, the mean caries experience whether expressed by the CdIMEmfs or the CdepiMEmfs among the 52 participants who followed the study to the end did not differ from the caries experience among the 10 children who dropped out between baseline and
Category
n
Multivariate Odds ratio (CI)
Gender Age Plaque
Boy
Final examination Baseline
Use of fluoridated toothpaste
14.2 (1.2–15.2)
0.03
767260
1
0.17
140
1
0.32
No
68 20
1
0.16
Yes
188
Limited
40168
1
0.42
Girl 45–54 months55–58 months59–65 months NoYes
12088
p value
Baseline Sugar consumption Baseline DMFS
0>0
14464
1
0.92
Baseline DMFS increase
0>0
15652
1
0.17
Baseline to final examination Tooth type
First molar
104104
1
0.07
Side
Second molar Right
104104
1
0.16
Jaw
Left Upper
152
1
0.13
Morphology Focus-surface
Lower ConvexConcave
189 15553
Morphology Adjacent-surface
High
ConvexConcave
155 53
16.8 (3.4–13.8) 1 2.6 (1.4–4.8)
Caries in focus-surface at final examination 59 of 208 surfaces. Patient is used as cluster variable