Clin Rheumatol (2001) 20:290–292 ß 2001 Clinical Rheumatology
Clinical Rheumatology
Case Report Life-Threatening Complications of Hepatitis B Virus-Related Polyarteritis Nodosa Developing Despite Interferon-a2b Therapy: Successful Treatment with a Combination of Interferon, Lamivudine, Plasma Exchanges and Steroids P. Dele´aval1, P. Stadler1, E. Descombes1, E. Hecker1, G. Schrago1, C. Chizzolini2, A. Nicole1, P. Pugin1 and C. Regamey1 1
Hoˆpital Cantonal, Fribourg; 2University Hospital, Geneva, Switzerland
Abstract: Polyarteritis nodosa (PAN) is a rare vasculitis associated with hepatitis B virus (HBV) infection in a significant proportion of cases. When used to treat HBVrelated PAN, immunosuppressive agents may enhance viral replication and relaspes are frequent. In recent years the use of antiviral drugs has been proposed. We report the case of a patient with HBV-related PAN who, despite 6 weeks of interferon-a2b (IFN-a2b) monotherapy, developed life-threatening complications with bowel perforation. He was thereafter successfully treated with a combination of IFN-a2b, lamivudine, plasma exchanges and short-term steroids. In contrast to IFNa2b, lamivudine is effective in rapidly suppressing viral replication. This may be valuable in the treatment of HBV-related PAN by contributing to a faster diminution of circulating immune complex levels. This case report highlights the importance of aggressive combined therapy in patients with HBV-related PAN. Keywords: Hepatitis B virus; Interferon; Lamivudine; Plasma exchange; Polyarteritis nodosa
Introduction Polyarteritis nodosa (PAN) is a rare necrotising vasculitis that was first described by Ku¨ssmaul and Maier in 1866 [1]. In 1970, Gocke showed an association between PAN and hepatitis B virus (HBV) infection [2]. Several studies have confirmed that PAN is related to HBV infection in 7%–56% of cases [3,4]. Conventional therapy has been based on corticosteroids and immunosuppressive agents, sometimes combined with plasma exchanges [5,6]. However, some authors have pointed out that in HBV-related PAN immunosuppression may enhance viral replication, and therefore a more rational approach would rely on the use of antiviral drugs [3,4,7]. Several antiviral agents have been used, including vidarabine, interferon-a2b (IFN-a2b), famciclovir and lamivudine [3,4,8–11]. We report the case of a patient with HBV-related PAN in whom IFN-a2b monotherapy did not control disease progression, and who developed life-threatening complications that only responded to combined therapy with IFN-a2b, lamivudine, plasma exchanges and short-term steroids.
Case Report
Correspondence and offprint requests to: Dr Eric Descombes, Department of Internal Medicine, Hoˆpital Cantonal, CH-1700 Fribourg, Switzerland. Fax: ++41 26 426 72 44; E-mail:
[email protected]
In November 1998, a previously healthy 44-year-old caucasian man suddenly developed a pain in the right calf and weakness of dorsiflexion of the foot. The attending physician suspected acute ischaemia of the leg and an urgent angiography was performed, which was normal. Electromyography (EMG) showed an axonal lesion of
Hepatitis B Virus-Related Polyarteritis Nodosa
291
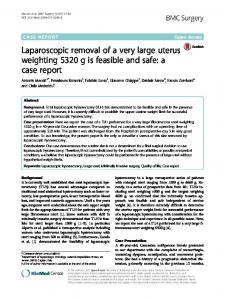
Fig. 1. Changes in C-reactive protein (CRP) and alanine amino transferase (alat) levels during therapy with interferon (IFN), plasma exchanges (PE), lamivudine and corticosteroids (CS).
the right peroneal nerve. In the following weeks the patient’s clinical condition deteriorated, with weight loss (9 kg in 2 months) and increasing weakness. A second EMG revealed involvement of several nerves, compatible with mononeuritis multiplex. He was first admitted to our hospital in January 1999. Clinical examination revealed a poor general condition with diffuse muscular atrophy. There were no cutaneous lesions. Temperature was 36.58C, blood pressure 140/70 mmHg. The neurological examination showed asymmetrical paresis of the lower limbs with bilateral ankle areflexia. ESR was 94 mm/h, C-reactive protein (CRP) 102 mg/l, haemoglobin 128 g/l, leukocytes 10.9 G/l, platelets 513 G/l, serum creatinine 63 mmol/l, alkaline phosphatase 302 U/l, g-GT 106 U/l, ALAT 53 U/l and ASAT 49 U/l. HBs antigen, HBe Ag and anti-HBc IgM were positive; 2.742.429.000 copies/ ml of HBV DNA were detected. Serology for HCV, HIV, syphilis and Lyme disease was negative. Complement was normal but circulating immune complexes were elevated. Rheumatoid factor, antinuclear antibodies, antidsDNA, ANCA and cryoglobulins were negative. Spinal fluid examination was unremarkable. A lumbar MRI study was normal. The liver biopsy showed a moderately active chronic hepatitis. Sural nerve biopsy showed severe subacute neuropathy with lymphocytic inflammatory infiltrates of the small arteries, mainly composed of CD3- and CD8-positive lymphocytes. Echocardiography showed a severe dilated cardiomyopathy with diffuse myocardial hypokinesia (ejection fraction of 35%). The diagnosis of HBV-related PAN was made according to the criteria of the American College of Rheumatology [12] and treatment with IFN-a2b (Intron A1, Essex) 7.5 million units three times a week was instituted.
After 6.5 weeks of IFN-a2b therapy, the patient was readmitted for abdominal pain and shock. He was in a very poor clinical condition. Temperature was 37.28C, blood pressure 90/55 mmHg and heart rate 145 bpm. Abdominal examination showed diffuse peritonitis. WBC were 2.7 G/l, CRP 215 mg/l and serum creatinine 161 mmol/l. A surgical ileal resection was performed because of ischaemic perforation. The histological examination showed acute to chronic ischaemic lesions with chronic inflammatory vasculitis of arterioles. Three days after surgery, the first session of plasma exchange was performed (he underwent 16 sessions in 5 weeks). IFN-a2b was continued and, on the 10th postoperative day, lamivudine (3TC1, Glaxo Wellcome) was added at a dose of 150 mg/day, together with steroids (Solumedrol 500 mg i.v. for 6 days, then oral prednisone 50 mg/day at rapidly tapering doses for 20 days). Clinical and biological improvement was rapid (Fig. 1). After 2 weeks of lamivudine treatment, the HBV DNA was no longer detectable and HBeAg/ anti-HBeAb seroconversion had occurred. HBsAg/antiHBsAb seroconversion occurred 2 weeks later and the antiviral therapy was stopped 6 weeks later. The echocardiogram showed a regression of the cardiac dilatation, with improvement of the ejection fraction to 50%. At the 6-month follow-up visit the patient was in good clinical condition, had gained weight (5 kg) and could walk normally. His renal function was normal and the HBV DNA undetectable. Electromyography showed progressive improvement of nerve conduction. The patient could be considered clinically and serogically cured according to the criteria of Guillevin et al. [4].
292
P. Dele´aval et al.
Discussion
References
Several antiviral agents have been used to treat HBVrelated PAN, including vidarabine, either alone or in combination with IFN-a2b [3,4], IFN-a2b alone [9], IFN-a2b with famciclovir [10], and IFN-a2b with lamivudine [11]. The case of our patient is particularly interesting, as under IFN-a2b monotherapy his clinical condition worsened dramatically and led to a life-threatening complication. The patient quickly improved and was ultimately cured when an aggressive protocol combining two antiviral drugs (IFN-a2b and lamivudine) with plasma exchanges (PE) and corticosteroids (CS) was introduced. As pointed out previously, PE and a short course of CS may be useful to reduce inflammation and circulating immune complexes, whereas antiviral drugs decrease viral load and promote HBV seroconversion [3,4]. According to Guillevin et al. [4], no relapses of PAN occur in patients achieving HbeAg/HBeAb seroconversion. Vidarabine was the first antiviral drug used in the therapy of HBV-related PAN (in combination with PE and CS), with complete recovery in 73%–86% [3,4] of the cases and sustained viral clearance in 25% [4]. In a small cohort of patients treated with IFN and PE, these figures were 100% and 50%, respectively [9]. These results are substantially better than those obtained with conventional therapy [3,4]. Recently, lamivudine, a well tolerated oral nucleoside analogue, has become available for the treatment of chronic hepatitis B [13]. In patients with chronic hepatitis B, the rate of HBsAg/HBsAb seroconversion is similar with IFN-a2b and lamivudine and, according to present data, combination therapy does not provide a greater benefit than monotherapy [13,14]. However, in contrast to IFN-a2b, lamivudine is quite effective in rapidly suppressing viral replication in almost all patients (independently of the HBeAg response) [13]. This effect may be valuable in the therapy of patients with HBV-related PAN by contributing to a more rapid diminution of the circulating immune complex levels. However, further studies are needed to determine the best combined therapeutic approach to HBV-related PAN.
1. Ku¨ssmaul A, Maier K. Ueber eine bisher nicht beschreibene eigenthu¨mliche Arterienerkrankung (Periarteritis Nodosa) die mit Morbus Brightii und rapid fortschreitender allgeimender Mu¨skella¨ hmung einergeht. Dtsch Arch Klin Med 1866;1:483–518. 2. Gocke DJ, Hsu K, Morgan C, Bombardieri S, et al. Association between polyarteritis nodosa and Australia antigen. Lancet 1970;2:1149–53. 3. Tre´po C, Ouzan D, Delmont J, Tremisi J. Supe´riorite´ d’un nouveau traitement e´thiopathoge´nique des pe´riarte´rites noueuses (PAN) induites par le virus de l’he´patite B graˆce a` l’association: corticothe´rapie bre´ve, vidarabine, e´changes plasmatiques. Presse Me´d 1988;17:1527–31. 4. Guillevin L, Lohte F, Cohen P et al. Polyarteritis nodosa related to hepatitis B virus. A prospective study with long-term observation of 41 patients. Medicine (Baltimore) 1995;5:238–53. 5. Guillevin L, Lohte F. Treatment of polyarteritis nodosa and microscopic polyangiitis. Arthritis Rheum 1998;12:2100–5. 6. Gayraud M, Guillevin L, Cohen P, et al. Treatment of good prognosis polyarteritis nodosa and Churg-Strauss syndrome: comparison of steroids and oral or pulse cyclophosphamide in 25 patients. Br J Rheumatol 1997;36:1290–7. 7. Lam KC, Lai CL, Tre´po C, Wu PC. Deleterious effect of prednisone in HbsAg-positive chronic hepatitis. N Engl J Med 1981;304:380–6. 8. Guillevin L, Lhote F, Leon A, et al. Treatment of polyarteritis nodosa related to hepatitis B virus with short term steroid therapy associated with antiviral agents and plasma exchanges. A prospective trial in 33 patients. J Rheumatol 1993;2:289–97. 9. Guillevin L, Lhote F, Sauvaget F, et al. Treatment of polyarteritis nodosa related to hepatitis B virus with interferon-alpha and plasma exchanges. Ann Rheum Dis 1994;53:334–7. 10. Molloy PJ, Friedlander L, Van Thiel DH, Kania RJ. Combined interferon, famciclovir and GM-CSF treatment of HBV infection in an individual with periarteritis nodosa. Hepatogastroenterology 1999;46(28):2529–31. 11. Wicki J, Olivieri J, Pizzolato G et al. Successful treatment of polyarteritis nodosa related to hepatitis B virus with a combination of lamivudine and interferon alpha. Br J Rheumatol 1999;2:183–5. 12. Lightfoot RW, Midchel BA, Bloch DA et al. The American College of Rheumatology 1990 criteria for the classification of polyarteritis nodosa. Arthritis Rheum 1990;33:1088–93. 13. Dienstag J, Schiff E, Wright T, et al. Lamivudine as initial treatment for chronic hepatitis B in the United States. N Engl J Med 1999;341:1256–63. 14. Wong D, Cheung A, O’Rourke K, Naylor D, Detsky A, Heathcote J. Effect of Alpha-interferon treatment in patients with hepatitis B antigen-positive chronic hepatitis B. A meta-analysis. Ann Intern Med 1993;119:312–23.
Received for publication 2 June 2000 Accepted in revised form 19 January 2001