Am. J. Trop. Med. Hyg., 79(6), 2008, pp. 853–855 Copyright © 2008 by The American Society of Tropical Medicine and Hygiene
Case Report: Failure of Subcutaneous Ivermectin in Treating Strongyloides Hyperinfection Victor Leung,* Ghada N. Al-Rawahi, Jennifer Grant, Lawrence Fleckenstein, and William Bowie Department of Internal Medicine, University of British Columbia, Vancouver, BC, Canada; Department of Pathology and Laboratory Medicine, Children’s and Women’s Health Center of British Columbia, Vancouver, British Columbia, Canada; Department of Pathology and Laboratory Medicine, University of British Columbia and Division of Medical Microbiology and Infection Control, Vancouver General Hospital, Vancouver, British Columbia, Canada; Division of Clinical and Administrative Pharmacy, University of Iowa College of Pharmacy, Iowa City, Iowa; Division of Infectious Diseases, University of British Columbia, Vancouver, British Columbia, Canada
Abstract. A man with Escherichia coli meningitis and bacteremia, while on dexamethasone, developed Strongyloides hyperinfection syndrome and died despite salvage therapy with subcutaneous ivermectin. We report the first documented total and free levels of subcutaneous ivermectin used for therapy. floxacin 750 mg q12h for 6 weeks, and he was discharged after 12 days in the hospital. Within a week of discharge, the patient returned to the hospital complaining of nausea, vomitting, abdominal bloating, and constipation. A computed tomography (CT) scan of the abdomen and pelvis showed diffuse hyperemia, dilation, and vascular engorgement within the proximal and mid-small bowel. An esophagogastroduodenoscopy the next day showed edematous and friable mucosa in the third part of the duodenum. A repeat CT abdomen and pelvis 3 days later showed a small bowel obstruction. Abdominal ultrasound and endoscopic retrograde cholangiopancreatography showed a moderately distended gallbladder with sludge and dilatation of the common bile duct. A completion cholangiogram showed no filling defects. The following day, the patient developed septic shock, which precipitated an exploratory laparotomy. Intraoperatively, an isolated band adhesion was found, however the bowel perforated during attempts to milk the small bowel contents so a small bowel resection with primary anastomosis was performed. Postoperatively, the patient was transferred to the intensive care unit and treated intravenously with hydrocortisone 100 mg q8h, fluconazole 400-mg daily, and imipenem/cilastin 500 mg q6h. Blood cultures and a central venous cathether tip from the same day eventually grew Candida utilis. Total parenteral nutrition was started, and he was rapidly tapered from inotropic and vasopressor support. Albumin concentration during hospitalization never exceeded 15 g/L. He was extubated 3 days later. Pathology from the bowel resection showed a heavy burden of helminthic larvae in the resected bowel and lymphatics. Nasogastric and tracheal aspirates showed the presence of S. stercoralis larvae. Special access for ivermectin was obtained from Health Canada and ivermectin 12 mg (Stromectol, Merck Frost, Haarlem, The Netherlands) was administered via the nasogastric tube for 2 days. The patient had high gastric residuals so a parenteral veterinary form of ivermectin (Ivomec, Merial Ltd., Duluth, GA) was obtained from a local veterinary hospital. Informed consent was obtained from the patient and Health Canada was also contacted. The patient was given 200 g/kg of subcutaneous ivermectin daily in the arms. Plasma samples were obtained and stored at −80°C until processing. Ivermectin concentration was analyzed by high-performance liquid chromatography.10 The plasma protein binding of ivermectin was determined by equilibrium dialysis.11 The drug
INTRODUCTION Strongyloides stercoralis is an intestinal nematode, endemic to sub-tropical and tropical areas that can complete its life cycle within a human host.1 Immigrants to Canada from Southeast Asia have high seroprevalence for strongyloidiasis.2 Although usually benign, in immunocompromised hosts an accelerated cycle of autoinfection (hyperinfection) produces increased larval burden and migration through tissues, which can cause gram negative septic shock and multiorgan failure.3 Current treatment options are limited. Regimens are extrapolated from data obtained from treatment of chronic strongyloidiasis; however, many patients with disseminated disease have complications that preclude using oral drugs. There have been six published cases describing use of the parenteral form of ivermectin for treating hyperinfection.4–9 We describe the clinical course of a hypoalbuminemic patient with Strongyloides hyperinfection who was treated with oral followed by subcutaneous ivermectin. This is the first report of total and free ivermectin levels in a patient. This case provides insight into the binding and pharmacokinetics of ivermectin, and underscores the difficulty in treating this serious infection. CASE REPORT A 67-year-old Laotian immigrant with recurrent craniopharyngioma was treated with stereotactic radiation 6 months before consultation. This was complicated by compressive optic neuropathy requiring treatment with dexamethasone 4 mg q8h. Six weeks after starting corticosteroids he presented to the hospital with headache, nausea, and fever. Physical examination revealed meningeal signs. Complete blood count showed normal white blood cell (WBC) count and normal eosinophils. Cerebrospinal fluid (CSF) analysis revealed 760 × 106/L WBC (81% neutrophil), 1757 mg/L protein, and 0.3 mmol/L glucose. The CSF and blood cultures were positive for Escherichia coli. He was treated initially with ceftriaxone 2 grams IV q6h and ampicillin 2 grams IV q4h. Nine days later, his treatment was changed to oral cipro-
* Address correspondence to Victor Leung, 1550 Dr. Penfield, Apt 1406, Montreal, Quebec H3G 1C2. E-mail: victor.leung@mail .mcgill.ca
853
854
LEUNG AND OTHER
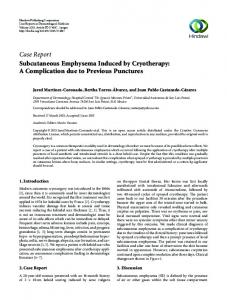
regimen, plasma total, and free ivermectin levels are summarized in Figure 1. Sixteen days after admission, the patient was intubated for a decreased level of consciousness. A CT scan of the abdomen revealed free air and fluid in the vicinity of the anastomosis. Laparotomy revealed multiple areas of perforation. These areas were resected and the bowel was reanastomosed. Two days later a second laparotomy was performed with closure of the abdominal cavity, creation of an end loop jejunostomy, and mucous fistula. Postoperatively septic shock and progressive multiorgan failure developed. Tracheal aspirates and peritoneal wound exudates were positive for Aspergillus fumigatus. Although larval burden from nasogastric and tracheal aspirates had decreased from > 25 organisms/slide to 4 organisms/slide, a nasogastric aspirate taken before he died showed motile larvae by Baermann technique. Comfort care was initiated and he died on the same day. The patient’s family refused a post-mortem examination. DISCUSSION This case illustrates the complications of Strongyloides hyperinfection and the need for prevention. Hyperinfection is often associated with deficits in type-2 immune response, most commonly following corticosteroid use.3 It is estimated that 77.5% of immigrants coming to Canada over the 10-year period between 1991 and 2001 were from Strongyloides endemic countries.12 Individuals with risk factors for acquiring S. stercoralis should be screened and treated with ivermectin if serology or stools is positive before starting corticosteroid therapy. Meningitis is a complication of S. stercoralis hyperinfection and may occur by direct invasion of the central nervous system by migrating larvae with attached fecal flora or by bacteremia secondary to disrupted bowel integrity.13 Gram nega-
FIGURE 1. Plasma ivermectin concentrations and unbound percentage following the administration of oral and subcutaneous ivermectin. Oral ivermectin was given on July 13 and 14, and subcutaneous ivermectin was administered daily from July 15 to July 26. All doses were 200 g/kg. Less than 1% of free ivermectin was found in our patient (the lower limits of detection was 0.2 ng/mL) based on the equilibrium dialysis method.19
tive meningitis is rare in adults without previous neurosurgery and Strongyloides hyperinfection should be considered in the differential diagnosis. Management of hyperinfection is very challenging. Our patient was unable to absorb medication administered enterally because of his persistent ileus. There are six case reports using subcutaneous ivermectin as an adjunct or alternative to oral ivermectin and/or albendazole.4–9 There have also been three case reports on the use of rectal thiabendazole14–16 and one report of rectal ivermectin.17 Although some of these cases reported success, results were confounded by the coadministration of oral medications and an optimal approach remains unknown. After receiving two oral doses of ivermectin, the plasma ivermectin concentration in our patient was 0.7 ng/mL— confirming poor enteric absorption—and rose to 28.3 ng/mL after receiving 6 subcutaneous injections (200 g/kg). From animal studies, ivermectin is slowly absorbed after subcutaneous administration.18 Because of the hypoalbuminemia and edema in our patient, ivermectin absorption may have been retarded and peak ivermectin concentrations may have not been reached during the sampling period from subcutaneous dosing.19 Ivermectin protein binding has not been previously reported in patients with disseminated strongyloidiasis. This is of some interest because hypoalbuminemia is common in hyperinfection, and it might be reasonably expected that free drug concentration would be elevated. Ivermectin is highly bound to human serum albumin, and the percent unbound increases with decreasing albumin concentration.19,20 We found less than 1% of free ivermectin in this patient. This is a surprising result in face of the albumin status of this patient. However, ivermectin is also highly bound to alpha-1 acid glycoprotein.10 It is tempting to speculate that because of the systemic inflammation involved with disseminated Strongyloides, alpha-1 acid glycoprotein levels are elevated, contributing to the low fraction unbound for ivermectin that was observed in this patient. The high protein binding may have reduced the distribution of ivermectin to tissues and contributed to poor therapeutic outcome. It is not known what minimally effective ivermectin concentration is required for treating strongyloidiasis in humans. In vitro studies using Strongyloides ratti and Strongyloides venezuelensis filariform larvae have been done to determine concentration of ivermectin required to immobilize 50% of worms.21,22 However, there is no known correlation with plasma or tissue levels. In humans with disseminated disease, the tissue levels of ivermectin may be very important to the therapeutic outcome. Currently, special access for ivermectin is required from Health Canada and may introduce a delay in administering ivermectin. There are many issues regarding ivermectin administration that are unknown. Because free levels were low in our case, a loading dose of subcutaneous ivermectin could be considered. Furthermore, once the enteral route is available, oral dosing in addition to the subcutaneous route might increase efficacy because of enterohepatic circulation. Strongyloides hyperinfection has a high mortality rate and is difficult to manage. Although more studies are needed to understand the role of parenteral ivermectin in hyperinfection, the most important issue is primary prevention of hyperinfection. A critical requirement for the diagnosis is a high
IVERMECTIN AND HYPERINFECTION
index of suspicion for infection. Because the two most consistent risk factors for hyperinfection are treatment with corticosteroids and infection with HTLV-1, any patient who has lived in an endemic area with these risk factors should be screened by serologic testing and stool examination. If the results are positive, then there is a strong argument to treat empirically with ivermectin given the dire consequences of hyperinfection. The high mortality argues for early and aggressive treatment with combined parenteral and oral ivermectin. Received July 23, 2008. Accepted for publication September 17, 2008. Acknowledgments: The American Committee on Clinical Tropical Medicine and Travelers’ Health (ACCTMTH) assisted with publication expenses. Authors’ addresses: Victor Leung, 1550 Dr. Penfield, Apt 1406, Montreal, Quebec H3G 1C2, Tel: 514-451-8342, Fax: 604-327-2062, Pager: 514-406-3046, E-mail:
[email protected]. Ghada AlRawahi, Department of Pathology and Laboratory Medicine, Children’s and Women’s Health Centre of British Columbia, Rm. 2G27, 4500 Oak Street, Vancouver, BC V6H 3N1, Tel: 604-875-2394, Fax: 604-875-3777, E-mail:
[email protected]. Jennifer Grant, Vancouver General Hospital JPPN, Rm. 1110, 899 W. 12th Avenue, Vancouver, BC V5Z 1M9, Tel: 604-875-4111 ext. 69503, Fax: 604-8754359, Pager: 604-205-1689, E-mail:
[email protected]. Lawrence Fleckenstein, 115 S. Grand Avenue, College of Pharmacy, University of Iowa, Iowa City, IA 52242, Tel: 319-335-8804, Fax: 319-353-5646, E-mail:
[email protected]. William Bowie, 452D HPE 2733 Heather Street, Vancouver, BC V5Z 3J5, Tel: 604-875-4588, Fax: 604-875-4013, E-mail:
[email protected].
REFERENCES 1. Siddiqui AA, Genta RM, Berk SL, 2006. Strongyloidiasis. Guerrant RL, Walker DH, Weller PF, eds. Tropical Infectious Diseases–Principles, Pathogens and Practice. (Second edition). Philadelphia: Churchill Livingstone, 1274. 2. Gyorkos TW, Genta RM, Viens P, MacLean JD, 1990. Seroepidemiology of Strongyloides infection in the southeast Asian refugee population in Canada. Am J Epidemiol 132: 257–264. 3. Keiser PB, Nutman TB, 2004. Strongyloides stercoralis in the immunocompromised population. Clin Microbiol Rev 17: 208– 217. 4. Pacanowski J, Santos MD, Roux A, Maignan C, Guillot J, Lavarde V, Cornet M, 2005. Subcutaneous ivermectin as a safe salvage therapy in Strongyloides stercoralis hyperinfection syndrome: a case report. Am J Trop Med Hyg 73: 122–124. 5. Turner SA, Maclean JD, Fleckenstein L, Greenaway C, 2005. Parenteral administration of ivermectin in a patient with disseminated strongyloidiasis. Am J Trop Med Hyg 73: 911–914. 6. Marty FM, Lowry CM, Rodriguez M, Milner DA, Pieciak WS, Sinha A, Fleckenstein L, Baden LR, 2005. Treatment of hu-
7.
8.
9. 10.
11.
12. 13.
14. 15. 16.
17.
18.
19. 20. 21.
22.
855
man disseminated strongyloidiasis with a parenteral veterinary formulation of ivermectin. Clin Infect Dis 41: e5–e8. Hauber HP, Galle J, Chiodini PL, Rupp J, Birke R, Vollmer E, Zebel P, Lange C, 2005. Fatal outcome of a hyperinfection syndrome despite successful eradication of Strongyloides with subcutaneous ivermectin. Infection 33: 383–386. Salluh JI, Feres GA, Velasco E, Holanda GS, Toscano L, Soares M, 2005. Successful use of parenteral ivermectin in an immunosuppressed patient with disseminated strongyloidiasis and septic shock. Intensive Care Med 31: 1292. Chiodini PL, Reid AJ, Wiselka MJ, Firmin R, Foweraker J, 2000. Parenteral ivermectin in Strongyloides hyperinfection. Lancet 355: 43–44. Kitzman D, Wei SY, Fleckenstein L, 2006. Liquid chromatographic assay of ivermectin in human plasma for application to clinical pharmacokinetic studies. J Pharm Biomed Anal 40: 1013–1020. Barber S, Bowles V, Lespine A, Alvinerie M, 2003. The comparative serum disposition kinetics of subcutaneous administration of doramectin, ivermectin and moxidectin in the Australian Merino sheep. J Vet Pharmacol Ther 26: 343–348. Lim S, Katz K, Krajden S, Fuksa M, Keystone JS, Kain KC, 2004. Complicated and fatal Strongyloides infection in Canadians: risk factors, diagnosis and management. CMAJ 171: 479–484. Takayanagui OM, Lofrano MM, Araujo MB, Chimelli L, 1995. Detection of Strongyloides stercoralis in the cerebrospinal fluid of a patient with acquired immunodeficiency syndrome. Neurology 45: 193–194. Thomas MC, Costello SA, 1998. Disseminated strongyloidiasis arising from a single dose of dexamethasone before stereotactic radiosurgery. Int J Clin Pract 21: 520–521. Boken DJ, Leoni PA, Preheim LC, 1992. Treatment of Strongyloides stercoralis hyperinfection syndrome with thiabendazole administered per rectum. Clin Infect Dis 16: 123–126. Kennedy S, Campbell RM, Lawrence JF, Nichol GM, Rao DM, 1989. A case of severe Strongyloides stercoralis infection with jejunal perforation in an Australian ex-prisoner of war. Med J Aust 150: 92–93. Tarr PE, Miele PS, Peregoy KS, Smith MA, Neva FA, Lucey DR, 2003. Case report: rectal administration of ivermectin to a patient with Strongyloides hyperinfection syndrome. Am J Trop Med Hyg 68: 453–455. Lifschitz A, Virkel G, Pis A, Imperiale F, Sanchez S, Alvarez L, 1999. Ivermectin disposition kinetics after subcutaneous and intramuscular administration of an oil-based formulation to cattle. Vet Parasitol 86: 203–215. Klotz U, Ogbuokiri JE, Okonkwo PO, 1990. Ivermectin binds avidly to plasma proteins. Eur J Clin Pharmacol 39: 607–608. Okonkwo PO, Ogbuokiri JE, Ofoegbu E, Klotz U, 1993. Protein binding and ivermectin estimations in patients with onchocerciasis. Clin Pharmacol Ther 53: 426–430. Satou T, Koga M, Koike K, Tada I, Nikaido T, 2001. Nematocidal activities of thiabendazole and ivermectin against the larvae of Strongyloides ratti and S. venezuelensis. Vet Parasitol 99: 311– 322. Kotze AC, Clifford S, O’Grady J, Behnke JM, McCarthy JS, 2004. An in vitro larval motility assay to determine anthelmintic sensitivity for human hookworm and Strongyloides species. Am J Trop Med Hyg 71: 608–616.