Changes in Conjunctival Clusterin Expression in Severe Ocular Surface Disease Takahiro Nakamura,1 Kohji Nishida,2 Atsuyoshi Dota,1,3 and Shigeru Kinoshita1 PURPOSE. Clusterin is a unique gene transcript in the human ocular surface epithelia and is synthesized by and localized in mucosal epithelia in general. It is not present, however, in keratinized epithelia, such as epidermis. In severe ocular surface disease, pathologic keratinization (squamous metaplasia) of the ordinarily nonkeratinized corneal and conjunctival mucosal epithelia results in severe visual loss. In the current study, the expression of clusterin was examined in conjunctivalized corneas with severe ocular surface disease. METHODS. We examined conjunctiva covering cornea in eight eyes with ocular surface disease (Stevens-Johnson syndrome and ocular cicatricial pemphigoid) in which pathologic keratinization was present. Normal conjunctiva from four agematched individuals served as the control. Semiquantitative RT-PCR was used to investigate expression of the clusterin gene. Immunohistochemistry was used to study the distribution of clusterin protein. RESULTS. The level of clusterin mRNA was significantly lower than normal in the diseased ocular surfaces. Clusterin protein was also markedly decreased in keratinized conjunctiva compared with that in normal eyes. CONCLUSIONS. Clusterin expression is markedly reduced in the pathologic, keratinized ocular surface epithelium, suggesting its importance in maintaining the ocular surface epithelium as a nonkeratinizing epithelium. (Invest Ophthalmol Vis Sci. 2002;43:1702–1707)
C
lusterin is a widely distributed glycoprotein found in many tissues and body fluids.1–3 It has been studied extensively in recent years because of its involvement in a number of biological processes. For example, it has potential amphipathic helical domains that allow it to bind to hydrophobic molecules and potential heparin binding domains that are essential in interaction with cell membranes and extracellular matrices.4 Several functions have been proposed for clusterin, including lipoprotein transport,1 inhibition of complement-mediated cell lysis,2 cell membrane protection,5 regulation of sperm maturation,6 protection of cells from apoptosis,7 and membrane re-
cycling.5,7 Clusterin has also been linked to disease, and its expression is induced in a diverse group of conditions,8 –10 among them glomerulonephritis, acute renal tubular failure, Alzheimer’s disease, atherosclerosis, and myocardial infarction. Our group has reported that clusterin is the most abundant gene transcript in the human corneal epithelium based on cDNA sequencing.11 We also have reported that it is synthesized by and localized in a number of mucosal epithelia, including those in the ocular surface, vagina, esophagus, stomach, small intestine, and colon. It is not present, however, in keratinized epithelia, such as epidermis.12 We have further located the protein in superficial cells of normal corneal and conjunctival mucosal epithelia and hypothesize that clusterin may have important functions in the nonkeratinized ocular surface mucosal epithelium. Severe ocular surface diseases, such as Stevens-Johnson syndrome (SJS) and ocular cicatricial pemphigoid (OCP), are some of the most challenging entities facing the clinician today.13–15 During the chronic cicatricial phase, most patients with ocular surface disease encounter numerous problems, including symblepharon, entropion, corneal vascularization (conjunctivalization), and pathologic keratinization. The pathologic transition of a nonkeratinized, stratified epithelium into a nonsecretory, keratinized epithelium is termed squamous metaplasia16 –18 and is accompanied by a loss of goblet cells, an increase in cellular stratification, an enlargement of superficial cells, and keratinization. Squamous metaplasia has been described in a variety of ocular surface disorders,19 –23 and we have reported recently that various epidermal keratinizationrelated proteins are probably involved in the pathogenesis of cicatrizing ocular surface diseases.24,25 However, little is known about the pathogenesis of this group of diseases. In this study, to better understand the mechanism of keratinization in severe ocular surface disease, we examined the expression of clusterin in pathologically keratinized, conjunctivalized corneas. On the basis of the results, we suggest that clusterin may be essential for maintaining the ocular surface epithelium as a nonkeratinized epithelium.
MATERIALS From the 1Department of Ophthalmology, Kyoto Prefectural University of Medicine, Kyoto, Japan; the 2Department of Ophthalmology, Osaka University Medical School, Osaka, Japan; and 3Santen Pharmaceutical Co., Ltd., Nara, Japan. Supported in part by Grants-in-Aid for Scientific Research from the Japanese Ministry of Health and Welfare and the Japanese Ministry of Education, a research grant from Kyoto Foundation for the Promotion of Medical Science, and the Intramural Research Fund of Kyoto Prefectural University of Medicine. Submitted for publication August 23, 2001; revised January 22, 2002; accepted January 29, 2002. Commercial relationships policy: N. The publication costs of this article were defrayed in part by page charge payment. This article must therefore be marked “advertisement” in accordance with 18 U.S.C. §1734 solely to indicate this fact. Corresponding author: Takahiro Nakamura, Department of Ophthalmology, Kyoto Prefectural University of Medicine, Kawaramachi Hirokoji, Kamigyo-ku, Kyoto 602-0841, Japan;
[email protected].
1702
AND
METHODS
Human Samples Several lines of evidence indicate that the conjunctival epithelium invades and resurfaces the cornea in ocular surface diseases involving limbal stem cell deficiencies.26,27 Examples include SJS and OCP. With proper informed consent and in accordance with the tenets of the Declaration of Helsinki for research involving human subjects (and with approval by the Institutional Review Board of the Kyoto Prefectural University of Medicine), we obtained pathologically keratinized epithelia that covered cornea from four patients with SJS and four with OCP at the time of lamellar keratoplasty (Table 1). All eyes were in the chronic cicatricial phase, and the corneal surfaces were totally covered by conjunctival tissue. Again with proper informed consent, normal human bulbar conjunctiva was obtained during cataract surgery from four age-matched individuals with no history of ocular surface disease. Additional samples of normal human cornea and epidermis were obtained at autopsy. For RNA isolation, tissues were frozen in liquid nitrogen immediately after removal and stored at ⫺80°C with RNA Investigative Ophthalmology & Visual Science, June 2002, Vol. 43, No. 6 Copyright © Association for Research in Vision and Ophthalmology
Changes in Clusterin Expression
IOVS, June 2002, Vol. 43, No. 6 TABLE 1. Patient Profile Patient SJS1 SJS2 SJS3 SJS4 OCP1 OCP2 OCP3* OCP4*
1703
Indirect Immunofluorescence
Age/Gender
Visual Acuity
Age at Onset (y)
Time Since Surgery (y)
62/M 61/F 31/F 57/F 80/F 81/F 83/F 77/F
HM ND 4/200 ND HM HM HM 6/200
30 31 23 27 50 60 — —
32 30 8 30 30 21 — —
HM, hand motion; ND, numerus digitorum. * Age at onset of disease and time since surgery are unknown. extraction reagent (TRIzol; Gibco Life Technologies, Grand Island, NY) until use. Samples for immunohistochemistry were snap frozen in liquid nitrogen and embedded in optimal cutting temperature (OCT) compound (Tissue-Tek II; Miles Laboratories, Elkhart, IN).
RNA Isolation and Semiquantitative RT-PCR of Clusterin Total RNA was isolated from keratinized conjunctiva by the use of RNA extraction reagent in accordance with the manufacturer’s protocol (TRIzol; Gibco). To investigate relative levels of clusterin mRNA expression in diseased conjunctiva, semiquantitative RT-PCR was performed.28 The human G3PDH gene was used as the internal control. Primer sequences used were ACCACAGTCCATGCCATCAC (sense) and TCCACCACCCTGTTGCTGTA (antisense). cDNA was generated by mixing the extracted RNA after ethanol precipitation (1 g/L per sample) with a random hexamer primer (Takara Biomedicals, Tokyo, Japan) and incubated at 65°C for 5 minutes, chilled on ice. The mixture was then reverse transcribed in 25 mM MgCl2, 100 mM Tris-HCl (pH 8.3), 500 mM KCl, 40 U/L RNase inhibitor (Takara Biomedicals), 10 mM dNTP mixture, and 5 U/L reverse transcriptase (AMV XL; Takara Biomedicals), for a final volume of 20 L. The mixture was incubated at 30°C for 10 minutes and 42°C for 30 minutes, heated to 99°C for 5 minutes, and then stored at ⫺20°C until use. For every sample, a 10-L aliquot (half the total volume) of the same RT product was used for PCR amplification. Oligonucleotide primers to the nontandem repeat regions of clusterin were designed from GenBank sequences CTTGATGCCCTTCTCTCCGTA (sense) and AACGTCCGAGTCAGAAGTGTG (antisense), located at, respectively, nucleotides 684 to 704 and 1194 to 1214 of the clusterin cDNA (GenBank is provided in the public domain by the National Center for Biotechnology Information, Bethesda, MD, and is available at http://www.ncbi.nlm.nih.gov/Genbank). PCR amplifications were performed as previously described,12 with conditions optimized for the clusterin gene using the RT product from total conjunctival RNA. The linear range of the amplification reaction for clusterin and G3PDH was determined by checking amplification after each cycle from cycles 16 to 26 for clusterin and from cycles 21 to 31 for G3PDH. This established that 22 cycles was in the midlinear phase for clusterin, whereas 25 cycles was in the midlinear phase for G3PDH. All PCR amplifications started with denaturation at 95°C for 3 minutes and ended with a final elongation at 72°C for 10 minutes. The parameters for PCR amplification were as follows: clusterin and G3PDH, 22 and 25 cycles of denaturation, respectively, at 95°C for 1 minute, annealing at 55°C for 1 minute, and extension at 72°C for 1 minute. A 5-L aliquot of the reaction mixture was then electrophoresed on a 2% agarose gel (Seakem; FMC Bio Products, Rockland, ME) containing ethidium bromide, to evaluate amplification and fragment size. The amount of amplified product was quantified for each sample using a computing densitometer (The 420OE scanner; PDI, Inc., Huntington Station, NY) and software (Quantity One; PDI, Inc.). To account for any differences in starting amounts of RNA, the final amount of PCR product was expressed as the ratio of the amplified clusterin gene to the G3PDH gene.
For indirect immunohistochemical studies of clusterin, cryostat sections (7 m thick) were placed on gelatin-coated slides, air-dried, and rehydrated in phosphate-buffered saline (PBS) at room temperature for 15 minutes. To block nonspecific binding, sections were incubated with 2% bovine serum albumin (BSA) at room temperature for 30 minutes. Subsequently, sections were incubated at room temperature for 2 hours with a commercially available primary antibody raised against clusterin (Quidel, San Diego, CA) that was diluted 1:500 in PBS; control incubations included incubation with normal mouse IgG (Dako, Kyoto, Japan).25 The sections were then washed three times for 15 minutes each in PBS containing 0.15% TritonX-100 (PBST) and incubated at room temperature for 1 hour with the secondary antibody, FITC-conjugated donkey anti-mouse IgG (Jackson ImmunoResearch, West Grove, PA) diluted 1:1000 in PBST. After several washings with PBS, the sections were coverslipped with antifade mounting medium containing propidium iodide (Vectashield; Vector, Burlingame, CA) and the slides examined by confocal microscopy (FluoView; Olympus, Tokyo, Japan). We also used keratin 10 (Biomeda, Foster City, CA) and keratin 13 (American Research Products, Kensington, MD) as markers for keratinized and stratified nonkeratinized cells, respectively. The immunohistochemical procedure was performed as previously described.25
RESULTS The samples we obtained were pathologically keratinized epithelia that covered the cornea and were from four patients with SJS and four with OCP in the chronic cicatricial phase. It has been reported that pathologic keratinization secondary to alterations in the microenvironment is associated with changes in cytokeratin expression in several mucosae.29 –31 Defined subsets of individual cytokeratins are characteristically expressed depending on epithelial cell and tissue type, level of differentiation, or disease state.32–35 Previously, we reported that elevated levels of keratin 1/10 were observed in pathologically keratinized diseases tissues, but that keratin 4/13 and 3/12 remained unchanged. This suggests that elevated expression of keratin 1/10 is characteristic of the pathologic keratinization process in diseased conjunctival epithelium.25 On this basis, we used keratin 10 in the present study as a representative marker for keratinization and keratin 13 as a representative marker for nonkeratinization. Immunohistochemical examination (data not shown) confirmed that, on the basis of their keratin expression patterns, all tissues reported in this study are keratinized.
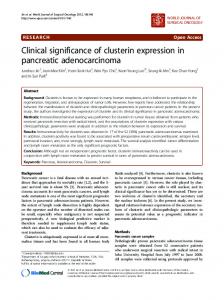
Semiquantitative RT-PCR of Clusterin To compare clusterin mRNA expression semiquantitatively within experimental groups, the linear phase of amplification of each cDNA was demonstrated. For clusterin and for the control housekeeping gene (G3PDH), the linear phases of amplification were established at 22 and 25 cycles, respectively. Clusterin mRNA was detected in normal human conjunctival epithelium, but not at all or at reduced levels in pathologically keratinized conjunctival epithelium (SJS, OCP; Fig. 1A). The results were confirmed by sequence analysis of the bands using a PCR-direct sequencing technique. Densitometric comparisons of clusterin mRNA with G3PDH mRNA were obtained in each of the groups studied (Fig. 1B). We discovered that the ratios of clusterin: G3PDH mRNA in the ocular surface diseases studied were lower than the ratios for normal conjunctival epithelium. These differences were statistically significant (Dunnett test; P ⬍ 0.05).
1704
Nakamura et al.
IOVS, June 2002, Vol. 43, No. 6
FIGURE 1. Semiquantitative analysis of clusterin mRNA expression. (A) Representative RT-PCR experiments. (B) Densitometric analysis. Reduced levels of clusterin mRNA expression were observed in the pathologically keratinized ocular surface epithelium compared with normal. The ratios of Clusterin/G3PDH mRNA in the tissue of ocular surface diseases studied were lower than those in normal conjunctiva. These differences are statistically significant (Dunnett test; P ⬍ 0.05). Lane 1: normal conjunctiva; lane 2: Stevens-Johnson syndrome; lane 3: ocular cicatricial pemphigoid (n ⫽ 4, mean ⫾ SEM).
Indirect Immunofluorescence of Clusterin and Several Cytokeratins Localization of clusterin protein was investigated by immunofluorescence using a monoclonal antibody raised against clusterin (summarized in Table 2). Negative control sections, incubated with normal mouse IgG (Dako), exhibited no discernible specific immunoreactivity over the entire region. Immunostaining patterns in normal stratified squamous epithelia of the human cornea and conjunctiva were similar to previous reports.12 In normal corneal epithelium (Fig. 2A), the superficial cell layers and upper intermediate layers stained intensely, whereas the underlying layers were not immunoreactive. In normal conjunctival epithelium (Fig. 2B), positive staining was seen in the upper half of the cellular multilayer. In contrast, the epithelium of normal epidermis (Fig. 2C) did not stain at all. In the conjunctival epithelia of patients with SJS or OCP, positive immunostaining was restricted to the superficial cell layer (Fig. 2D) or was not seen at all. This reduced expression of clusterin was more evident in sections of highly stratified epithelia (Fig. 3A). These regions were also immunoreactive for keratin 10, a specific marker for keratinized epithelium (Fig. 3B). Keratin 13, in contrast, was observed in all epithelial regions (Fig. 3C).
DISCUSSION Clusterin is an intriguing, ubiquitous, and highly conserved glycoprotein thought to be involved in a variety of biological processes. cDNA sequencing has shown it to be the most abundant gene transcript in human corneal epithelium, a finding that is suggestive of some functional importance in the
ocular surface.11 Also, clusterin expression has been noted in all nonkeratinized mucosal tissues tested, such as corneal, conjunctival, vaginal, and esophageal epithelia.12 Thus, it is possible that clusterin is always expressed in nonkeratinized mucosal epithelia, and we postulate that it may be a representative marker of nonkeratinization. Our previous study, using immunohistochemistry, suggested a possible link between clusterin expression and abnormal conjunctival epithelial cell differentiation in SJS.36 To further investigate this, we undertook the semiquantitative RTPCR study described herein, which disclosed that clusterin mRNA expression was reduced in the keratinized conjunctival epithelia in SJS and OCP,compared with the normal conjunctival epithelium (Fig. 1). Immunohistochemical data on these tissues also clearly demonstrated the reduced expression of clusterin in keratinized conjunctival epithelia, when compared with the strong expression in normal conjunctival epithelium (Figs. 2B, 2D). These findings imply that clusterin may have important functions in ocular surface homeostasis, perhaps at the tear– ocular surface interface. The function of clusterin in the ocular surface, however, remains obscure. In view of the fact that clusterin expression was not seen in the epidermis (Fig. 2C) and was markedly reduced in diseased conjunctival epithelia (Fig. 2D) that had become pathologically keratinized due to severe ocular surface disease, it seems as though the clusterin expression pattern in diseased conjunctival epithelium is changed to resemble that of a keratinized epithelium, such as epidermis. Another finding of this study is the change in clusterin expression depending on cellular stratification and keratinization. In Figure 3, the region of nonstratification showed the presence of clusterin as in normal conjunctiva; however, the clusterin appeared to fade as the tissue stratified (Fig. 3A). Also, the region of nonstratification showed no keratin 10 immunoreactivity (as in normal conjunctiva), whereas in stratified regions of the tissue, keratin 10 was readily immunolocalized (Fig. 3B). Our previous report indicated that keratin 10, which is involved in the physiological keratinization process in the epidermis, is strongly expressed in keratinized conjunctival epithelium, but not in normal conjunctival epithelium.25 We also indicated that keratin 13, a cytokeratin that is observed in nonkeratinized, stratified epithelia, is expressed in both normal and keratinized ocular surface epithelia.25 Our results in this article are consistent with those in our previous report (Fig. 3C). Another of our previous reports indicated that the number of proliferating epithelial cells in SJS conjunctiva that were immunoreactive with a monoclonal antibody (Ki-67) was much greater than normal, suggesting that epithelial overstratification with hyperproliferation may lead to the pathologic keratinization of ocular surface epithelia.24 Reduced clusterin expression also occurred in the regions of epithelial overstratification, leading us to consider a possible link between clusterin expression and keratinization. With this in mind we should point out that in a pterygium, a growth of fibrovascular tissue onto the cornea that appears to be continuous with the conjunctiva and in which no keratinization is
TABLE 2. Distribution and Intensity of Expression of Clusterin Layer
SJS1
SJS2
SJS3
SJS4
OCP1
OCP2
OCP3
OCP4
Normal Conjunctiva
Superficial layer Upper intermediate layer Lower intermediate layer Basal layer
⫹ ⫺ ⫺ ⫺
⫹ ⫺ ⫺ ⫺
⫹ ⫹ ⫺ ⫺
⫺ ⫺ ⫺ ⫺
⫺ ⫺ ⫺ ⫺
⫹ ⫺ ⫺ ⫺
⫹ ⫺ ⫺ ⫺
⫺ ⫺ ⫺ ⫺
⫹⫹ ⫹⫹ ⫺ ⫺
⫺, Nondiscernable stain; ⫹, faint stain; ⫹⫹, moderate stain.
IOVS, June 2002, Vol. 43, No. 6
Changes in Clusterin Expression
1705
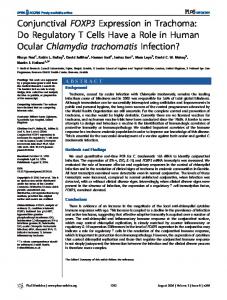
FIGURE 2. Representative immunohistochemical analysis of clusterin in the ocular surface epithelia (green). Tissue samples were obtained from normal adults (A, B, C) and a patient with ocular surface disease (D, patient SJS2). Nuclei were stained with propidium iodide (red). In normal corneal epithelium (A), the superficial cell layers and upper intermediate layers stained intensely, whereas the underlying layers were not immunoreactive. In normal conjunctival epithelium (B), as in normal corneal epithelium, positive staining was seen in the upper half of the cellular multilayer. In contrast, normal epidermis (C) was not stained in any region of the epithelium. In the diseased conjunctival epithelia (D), positive immunostaining was restricted to the superficial cells or was not present. Arrows: basement membrane zone; arrowheads: apical cell membrane. Scale bar, 100 m.
FIGURE 3. Immunolocalization of clusterin (A), keratin 10 (B), and keratin 13 (C) in a patient with ocular surface disease (SJS3; green). Nuclei were stained with propidium iodide (red; A). This particular section was partially nonstratified. (A) The region of nonstratification showed clusterin as in normal conjunctiva (left of ✽), with the clusterin immunoreactivity fading as the tissue stratified (right of ✽). This downregulation was more noticeable in the epithelium where increased cellular stratification was evident. The region of nonstratification showed no keratin 10 (as in normal conjunctiva), but it was present in the stratified region (B). Keratin 13 was present in all epithelial regions (C). Arrows: basement membrane zone; arrowheads: apical cell membrane. Dashed lines: position of the basal surface. Scale bar, 200 m.
reported,37,38 clusterin in eight cases investigated by us (data not shown) induced positive staining in the upper half of the cellular multilayer, as in normal nonkeratinized squamous epithelia of the human cornea and conjunctiva. Taken together with our previous findings, this suggests that clusterin expression may depend on the severity of pathologic keratinization. To further investigate our hypothesis, we are now observing the expression of mucin proteins (e.g., MUC1 and MUC4)39,40 that appear to be involved in the maintenance of the ocular surface epithelium in severe ocular surface disease. Moreover, in an attempt to confirm a possible link between clusterin expression and pathologic keratinization, future experiments will be conducted, not only in patients with dry eye, but in those with other keratinizing diseases, such as chemical burns and superior limbic keratoconjunctivitis. On the basis of the present results, we also suggest that clusterin expression may be a useful marker for terminally differentiated superficial cells of normal stratified squamous epithelia and may be associated with the terminal steps of this differentiation. The outcomes of our research in this field lead us to consider the interesting hypothesis that clusterin may be essential in maintaining the ocular surface epithelium as a nonkeratinizing epithelium. The question remains as to what might cause the unusual expression of clusterin protein in the ocular surface diseases we have examined. It has been reported that conjunctival inflammation may influence goblet cell loss in ocular surface diseases such as SJS, and substantial inflammatory cell infiltration (and cytokine expression) is probably a feature of the chronic phase of this disease.24 We have not studied inflammatory cells in the samples discussed herein; however, our group previously reported that inflammatory cells in the substantia propria of conjunctivalized corneas of patients with SJS and chemical injury are composed of CD4/CD8-positive T cells and/or macrophages.41 Also, the cytokine expression pattern suggests that CD4-positive T cells are T helper-1 cells. Based on the information available, we speculate that the reduced levels of clusterin proteins may be due to inflammatory activity, with the reduction resulting in conjunctival keratinization in severe ocular surface disease. We also suspect that severe tear deficiency may be involved in the pathogenesis of these conditions, because the ocular surface, made up of stratified, nonkeratinizing cell layers, is covered by a tear film that protects
1706
Nakamura et al.
the underlying epithelium. Pathologic keratinization has been described in numerous ocular surface disorders,17,18 including dry eye disorders, in which the aqueous layer of the tear film is deficient,20 and disorders such as SJS and OCP (the ones examined herein), in which the mucous layer is deficient. A relationship has also been found between vitamin A deficiency and clusterin in the male reproductive tract in which an initial increase in clusterin mRNA expression is followed by a subsequent decrease with increasing severity of vitamin A deficiency.42,43 Although the importance of this is unclear, it suggests a relationship between clusterin and vitamin A that may prove relevant for the role of clusterin in the eye. In view of this, we further hypothesize that changes in clusterin gene expression in the ocular surface epithelium may be due to severe tear deficiency. To test this, we are now observing the expression of clusterin proteins in several dry eye conditions. This study, aligned with our previous findings, indicates that clusterin expression is markedly reduced in diseased conjunctival epithelia and is absent in epidermis. This leads us to speculate that clusterin may be essential in maintaining the ocular surface epithelium as a nonkeratinizing epithelium. Even though our studies have demonstrated clusterin changes in conjunctiva in severe ocular surface disease, further investigation is needed to clarify the physiological function of clusterin in the ocular surface. Increased understanding of the process of pathologic keratinization of the ocular surface will undoubtedly enhance our ability to manage these debilitating diseases more effectively.
Acknowledgments The authors thank Andrew J. Quantock (Department of Optometry and Vision Science, Cardiff University, Cardiff, Wales, UK) for critical reading of and comments on the manuscript.
References 1. de Silva HV, Stuart WD, Duvic CR, et al. A 70-kDa apolipoprotein designated apoJ is a marker for subclasses of human plasma high density lipoproteins. J Biol Chem. 1990;265:13240 –13247. 2. Jenne DE, Lowin B, Peitsch MC, Bottcher A, Schmitz G, Tschopp J. Clusterin (complement lysis inhibitor) forms a high density lipoprotein complex with apoprotein A-I in human plasma. J Biol Chem. 1991;266:11030 –11036. 3. Jenne DE, Tschopp J. Molecular structure and functional characterization of a human complement cytolysis inhibitor found in blood and seminal plasma: Identity to sulfated glycoprotein 2, a constituent of rat testis fluid. Proc Natl Acad Sci USA. 1989;86: 7123–7127. 4. de Silva HV, Harmony JAK, Stusrt WD, Gil CM, Robbins J. Apolipoprotein J: structure and tissue distribution. Biochemistry. 1990; 29:5380 –5389. 5. Aronow BJ, Lund SD, Brown TL, Harmony JA. Apolipoprotein J expression at fluid-tissue interfaces: potential role in barrier cytoprotection. Proc Natl Acad Sci USA. 1993;90:725–729. 6. Sylvester SR, Morales C, Oko R, Griswold MD. Localization of sulfated glycoprotein-2 (clusterin) on spermatozoa and in the reproductive tract of the male rat. Biol Reprod. 1991;45:195–207. 7. Jordan-Starck TC, Witte DP, Aronow BJ, Harmony JAK. Apolipoprotein J: a membrane policeman? Curr Opin Lipidol. 1992;3: 75– 85. 8. Jenne DE, Tschopp J. Clusterin: the intriguing guises of a widely expressed glycoprotein. Trends Biochem Sci. 1992;17:154 –159. 9. Silkensen JR, Schwochau GB, Rosenburg ME. The role of clusterin in tissue injury. Biochem Cell Biol. 1994;72:483– 488. 10. Rosenburg ME, Silkensen JR. Clusterin: physiologic and pathophysiologic considerations. Int J Biochem Cell Biol. 1995;27:633– 645. 11. Nishida K, Adachi W, Shimizu-Matsumoto A, et al. A gene expression profile of human corneal epithelium and the isolation of human keratin 12 cDNA. Invest Ophthalmol Vis Sci. 1996;37: 1800 –1809.
IOVS, June 2002, Vol. 43, No. 6 12. Nishida K, Kawasaki S, Adachi W, Kinoshita S. Apolipoprotein J expression in human ocular surface epithelium. Invest Ophthalmol Vis Sci. 1996;37:2285–2292. 13. Tseng SC, Prabhasawat P, Barton K, Gray T, Meller D. Amniotic membrane transplantation with or without limbal allografts for corneal surface reconstruction in patients with limbal stem cell deficiency. Arch Ophthalmol. 1998;116:431– 441. 14. Tsubota K, Satake Y, Kaido M, et al. Treatment of severe ocular surface disorders with corneal epithelial stem-cell transplantation. N Engl J Med. 1999;340:1697–1703. 15. Koizumi N, Inatomi T, Suzuki T, Sotozono C, Kinoshita S. Cultivated corneal epithelial transplantation for ocular surface reconstruction in acute phase Stevens-Johnson syndrome. Arch Ophthalmol. 2001;119:298 –300. 16. Beitch I. The induction of keratinization in the corneal epithelium; a comparison of the dry eye and vitamin A-deficient eye. Invest Ophthalmol Vis Sci. 1970;9:827– 843. 17. Nelson JD, Havener VR, Cameron D. Cellulose acetate impression of the ocular surface. Arch Ophthalmol. 1983;101:1869 – 1872. 18. Tseng SCG. Staging of conjunctival squamous metaplasia by impression cytology. Ophthalmology. 1985;92:728 –733. 19. Friend J, Kiorpes TC, Thoft RA. Conjunctival goblet cell frequency after alkali injury is not accurately reflected by aqueous tear mucin content. Invest Ophthalmol Vis Sci. 1983;24:612– 618. 20. Kinoshita S, Kiorpes TC, Friend J, et al. Goblet cell density in ocular surface disease. Arch Ophthalmol. 1984;102:1049 –1051. 21. Tseng SCG, Hirst LW, Maumenee AE, et al. Possible mechanism for the loss of goblet cells in mucin-deficient disorders. Ophthalmology. 1984;91:545–552. 22. Pflugfelder SC, Huang AJW, Feuer W, et al. Conjunctival cytological features of primary Sjo ¨ gren’s syndrome. Ophthalmology. 1990; 97:985–991. 23. Tseng SCG, Hatchell D, Tierney N, Huang AJ, Sun T-T. Expression of keratin markers by rabbit corneal, conjunctival, and esophageal epithelia during vitamin A deficiency. J Cell Biol. 1984;99:2279 – 2286. 24. Nishida K, Yamanishi K, Yamada K, et al. Epithelial hyperproliferation and transglutaminase 1 gene expression in Stevens-Johnson syndrome conjunctiva. Am J Pathol. 1999;154:331–336. 25. Nakamura T, Nishida K, Dota A, Matsuki M, Yamanishi K, Kinoshita S. Elevated expression of transglutaminase 1 and keratinization-related proteins in conjunctiva in severe ocular surface disease. Invest Ophthalmol Vis Sci. 2001;42:549 –556. 26. Kinoshita S, Kiritoshi A, Ohji M, Ohashi Y, Manabe R. Disappearance of palisades of Vogt in ocular surface disease. Jpn J Clin Ophthalmol. 1986;40:363–366. 27. Chen JJ, Tseng SCG. Corneal epithelial wound healing in partial limbal deficiency. Invest Ophthalmol Vis Sci. 1990;31:1301– 1314. 28. Nakayama H, Yokoi H, Fujita J. Quantification of mRNA by nonradioactive RT-PCR and CCD imaging system. Nucleic Acids Res. 1992;20:4939. 29. Banks SS, Harris CC. Aberrant expression of keratin proteins and cross-linked envelopes in human esophageal carcinomas. Cancer Res. 1984;44:1153–1159. 30. Gigi LO, Geiger B, Levy R, et al. Cytokeratin expression in squamous metaplasia of the human uterine cervix. Differentiation. 1986;31:191–205. 31. Smedts F, Ramaekers F, Robben H, et al. Changing patterns of keratin expression during progression of cervical intraepithelial neoplasia. Am J Pathol. 1990;136:657– 668. 32. Franke WW, Schiller DL, Moll R, et al. Diversity of cytokeratins: differentiation specific expression of cytokeratin polypeptides in epithelial cells and tissues. J Mol Biol. 1981;153:933–959. 33. Tseng SCG, Jarvinen MJ, Nelson WG, Huang JW, Woodcock MJ, Sun T-T. Correlation of specific keratins with different types of epithelial differentiation: monoclonal antibody studies. Cell. 1982; 30:361–372. 34. Sun T-T, Eichner R, Nelson W, et al. Keratin classes: monoclonal markers for different types of epithelial differentiation. J Invest Dermatol. 1983;81:109 –115.
Changes in Clusterin Expression
IOVS, June 2002, Vol. 43, No. 6 35. Eichner R, Bonitz P, Sun T-T. Classification of epidermal keratins according to their immunoreactivity, isoelectric point, and mode of expression. J Cell Biol. 1985;98:1388 –1396. 36. Nishida K, Kawasaki S, Kinoshita S. Clusterin may be essential for maintaining ocular surface epithelium as a non-keratinizing epithelium. Adv Exp Med Biol. 1998;438:629 – 635. 37. Dushku N, Reid TW. Immunohistochemical evidence that human pterygia originate from an invasion of vimentin-expressing altered limbal epithelial basal cells. Curr Eye Res. 1994;13:473– 481. 38. Kwok LS, Coroneo MT. A model for pterygium formation. Cornea. 1994;13:219 –224. 39. Inatomi T, Spurr-Michaud S, Tisdale AS, Gipson IK. Human corneal
40.
41.
42. 43.
1707
and conjunctival epithelia express MUC1 mucin. Invest Ophthalmol Vis Sci. 1995;36:1818 –1827. Inatomi T, Spurr-Michaud S, Tisdale AS, Zhan Q, Feldman ST, Gipson IK. Expression of secretory mucin genes by human conjunctival epithelia. Invest Ophthalmol Vis Sci. 1996;37:1684–1692. Kawasaki S, Nishida K, Sotozono C, Quantock AJ, Kinoshita S. Conjunctival inflammation in the chronic phase of Stevens-Johnson syndrome. Br J Ophthalmol. 2000;84:1191–1193. Hugly S, Griswold M. Regulation of levels of specific Sertoli cell mRNAs by vitamin A. Dev Biol. 1987;121:316 –321. Morales CR, Griswold M. Variations in the level of transferrin and SGP-2 mRNAs in Sertoli cells of vitamin A-deficient rats. Cell Tissue Res. 1991;263:125–130.