Changes in the four-strand hamstring graft in ... - Semantic Scholar
Recommend Documents
Marc A. Sherry, DPT, CSCS,1 Thomas M. Best, MD, PhD,2,3 Amy Silder, PhD,4,5 Darryl G. Thelen, PhD,6,7,8 and Bryan .... through injury prevention programs.
chronic allograft nephropathy, 50% of losses being due to patient death and the remainder to loss of function. [3]. On the other hand, it has been reported that ...
For reprints and permission queries, please visit SAGE's Web site at http://www.sagepub.com/journalsPermissions.nav. Graft Diameter matters in Hamstring ACL ...
There are several reconstruction graft choices that can be used to ... effect on graft strength and longevity, is graft size. Ac- cording to Conte et al.,11 grafts less than 8 mm in diameter ..... anterior cruciate ligament surgery: Who gets what and
Jan 24, 2018 - Keywords: cardiovascular disease, bypass graft, saphenous vein, vein graft ... cesses during vein graft remodeling and show how inflammation.
invading the thyroid gland and thyroid cartilage, who underwent one stage ... There were none suspicious lymph node ... After the dissection of prelaryngeal.
Graft pulls were performed only on the largest follicular units, i.e. those that had ... transplanted area exposed.3 The introduction of Follicular Unit Extraction,4 ...
returning to competition prematurely can result in further injury ... time for return to play in professional football players with MRI findings after acute hamstring.
transplantations. HLA matches, anti-HLA class I antibodies, positive crossmatch test, or ... plantation, panel-reactive antibodies against HLA class I anti- bodies ...
ABSTRACT. Background The hamstring injury mechanism was assessed by investigating the exercise-related metabolic activity characteristics of the hamstring ...
Feb 25, 2016 - Abstract: In the present study, we evaluated tumor-infiltrating lymphocytes (TILs) and blood regulatory T lymphocyte (Tregs, ...
Figure 1. The concentration of calretinin increases during development. .... (Dizhoor et al., 1993), and visinin-like protein (VILIP) (Lenz et al., 1996)].
the development of chick throughout the entire incubation period. Methods: Chick .... compact layer (Co) is thin and remnants of cardiac jelly (star) are present in ...
Al-Mohanna and Nott (1986) provided evi- dence through electronmicroscopy for the holocrine mode for digestion, rejecting any secretory role for the B-cells,.
Mar 6, 2009 - Marianne Littel Ingmar H.A. Franken Jan W. Van Strien. Institute of Psychology ... balance of alpha activity between the left versus the right frontal hemisphere ..... 1990; 58: 330â341. 19 Fox NA: If it's not left, it's right: electr
search examining a well-developed intervention for generalized anxiety disorder (progressive muscle relaxation or relaxation; Bar- low, Raffa, & Cohen, 2002; ...
The neuropil displayed various degree of necrosis, granular cells showed vacuolation and disintegration of neuroplasm. In hippocampus of rats treated with 300 ...
tretching is commonly used in the med- ical, health, and fitness fields, as well as in school and military settings to increase flexibility and range of motion (ROM) ...
Composite ceramic bone graft substitute in the treatment of locally aggressive benign bone tumours. OS Schindler. Droitwich Knee Clinic and Birmingham ...
Apr 22, 2014 - Abstract. Background: To understand the regulation mechanism of eyestalk ablation on the activities of hepatopancreas, Illumina. RNA-Seq ...
May 19, 2008 - labial junction, a posteriorly inclined upper lip, and a re- ..... grafts,21,28-31 leading to an unnaturally stiff nasal lobule. Accepted for Publication: ...
creatinine and the D/Do of an individual strongly and inversely correlated to their respective initial values. The change in D/P creatinine and D/Do were signifi-.
cock and Agranoff, 1976; Burrell et al., 1979; Giulian et al.,. 1980; Neumann et ..... Goldstein, M. E., H. S. Cooper, J. Bruce, M. J. Carden, V. M.-Y. Lee, and W. W. ...
South Florida Water Management District,. P.O. Box 24680, West Palm Beach, FL, USA. W. F. DeBusk. Escambia County Engineering Department,.
Changes in the four-strand hamstring graft in ... - Semantic Scholar
FRCS(Orth), Orthopaedic. Surgeon. The Royal National. Orthopaedic Hospital, Brockley. Hill, Stanmore, Middlesex. HA5 4LP, UK. Correspondence should be ...
Changes in the four-strand hamstring graft in anterior cruciate ligament reconstruction in the skeletally-immature knee S. Bollen, F. Pease, A. Ehrenraich, S. Church, J. Skinner, A. Williams From Chelsea and Westminster Hospital, London, England
The potential harm to the growth plate following reconstruction of the anterior cruciate ligament in skeletally-immature patients is well documented, but we are not aware of literature on the subject of the fate of the graft itself. We have reviewed five adolescent males who underwent reconstruction of the ligament with four-strand hamstring grafts using MR images taken at a mean of 34.6 months (18 to 58) from the time of operation. The changes in dimension of the graft were measured and compared with those taken at the original operation. No growth arrest was seen on radiological or clinical measurement of leg-length discrepancy, nor was there any soft-tissue contracture. All the patients regained their pre-injury level of activity, including elite-level sport in three. The patients grew by a mean of 17.3 cm (14 to 24). The diameter of the grafts did not change despite large increases in length (mean 42%; 33% to 57%). Most of the gain in length was on the femoral side. Large changes in the length of the grafts were seen. There is a considerable increase in the size of the graft, so some neogenesis must occur; the graft must grow.
Tears of the anterior cruciate ligament (ACL) are significant at any age but in childhood they may lead to particular problems and incremental deterioration of the joint.1-4 The outcome is better in cases treated by surgical reconstruction of the ACL than in those managed conservatively.2,4 Early reconstruction has become increasingly popular,1,5 and most surgeons employ four-strand hamstring grafts using a transphyseal technique.1,6,7 A soft-tissue graft is preferred to bone-patellar tendon-bone constructs, as it is thought to pose less risk to the growth plate, although the latter and similar grafts have been used.8,9 Disturbance of the growth plate has been described, but is often related to technical errors.5 Deformity and growth arrest should now be uncommon when using transphyseal techniques employing softtissue grafts such as hamstrings.6 Although the fate of the growth plate has been considered, very little is known about the progress of the graft itself.
Patients and Methods Reconstruction of the ACL was undertaken in five adolescent males who were followed to skeletal maturity. Their details are summarised in Table I. Their pubertal development, graded according to Tanner,10 was recorded: three
were stage 1 (pre-pubertal) and two were stage 2. The surgery was undertaken by the senior authors (AW and SB). After removing the ACL remnant both used a four-strand semitendinosus/ gracilis tendon transphyseal technique, taking care to avoid the anterior tibial physis and aiming for central penetration of the tibial physis. On the femoral side, standard far-posterior tunnel placement was undertaken with suspensory fixation using an EndobuttonCL (Smith and Nephew Inc., Andover, Massachusetts) or Rigidfix (Mitek Inc., Westwood, Massachusetts). Tibial fixation was more variable because the size of the tibia restricted the choice of implant. Either interference screws or staples were used. In case 1, fixation was aided by tying around a cortical screw on the femur and the tibia. All five patients underwent the same ‘accelerated’ rehabilitation programme, emphasising early full extension and range of movement. Braces were not used. The patients were followed until, or just prior to, skeletal maturity to ensure no premature growth arrest. All had MR scans at their last follow-up. Case 1 had a new injury which required MRI, and this was used in the study. All the other patients were free of symptoms at the time of the final assessment. All had clinical measurement of leg length and radiographs of 455
456
S. BOLLEN, F. PEASE, A. EHRENRAICH, S. CHURCH, J. SKINNER, A. WILLIAMS
Table I. Details of the patients Age at surgery
Tanner10 stage of puberty Delay to surgery
Previous treatment
12 yrs 3 mths
1
20 mths
Two arthroscopies
13 yrs 10 mths
1
19 mths
One arthroscopy
12 yrs 6 mths
1
6 mths
MCL tear grade III, 14 yrs 3 mths braced for six weeks Nil 14 yrs 2 mths
Bracing and physio (different hospital; thought to be isolated MCL tear)
Acute: at 8 weeks after 6 weeks bracing 4 mths
MCL, medial collateral ligament
Fig. 1a
Fig. 1b
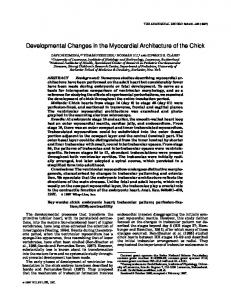
a) Sagittal MRI showing the intra-articular (white dotted line) and tibial (white dashed line) portions of the graft. The real length of each portion is measured by scaling up the length of the lines shown using the scale present on all our scans. b) Coronal MRI showing the ease of measuring the length of the tibial graft (white dotted line). Fig. 2
both knees at approximately six-monthly intervals and at final follow-up, to check for growth disturbance as manifest by alterations in longitudinal growth or deformity of the tibia or femur. The clinical assessment was undertaken by one of the senior authors. The operative measurements of the diameter of the graft, which determined the diameter of the bone tunnels, and the lengths of the tunnels were recorded. The immediate postoperative radiographs were used to estimate the length of the intra-articular portion of the graft. The known sizes of the fixation devices allowed a good estimate of radiological magnification. These measurements were undertaken on lateral radiographs, measuring the length between the apertures of the tibial and femoral tunnels to reflect the length of the intra-articular portion of the graft. The MR scans at follow-up were available in all cases and allowed accurate measurement of the dimensions of the graft and bone tunnel (Figs 1 and 2). Growth was complete in only one patient; the remaining patients had a little growth remaining.
Coronal MRI showing the method of measurement of the length of the graft in the femur. The white dotted line is aligned with the graft on the scan, and this length is converted to real length by means of the scale present on all our scans.
Results The mean follow-up was 34.6 months (18 to 58). No patient developed growth disturbance. The leg lengths were equal on clinical examination, and there was no radiological evidence of bony deformity at final follow-up. There was no soft-tissue contracture. All knees had full extension and flexion. The changes in the dimensions of the tunnel and graft are presented in Table II. The patients grew by a mean of 17.3 cm (14 to 24). The graft diameters did not change despite large changes in the length of the graft, with a mean of 42% (33% to 57%). Most of the gain in length was in the femur. Within each bone, differential growth was evident between the portion of the graft in the epiphysis and that in the metaphysis. A characteristic angulation of the THE JOURNAL OF BONE AND JOINT SURGERY
CHANGES IN THE FOUR-STRAND HAMSTRING GRAFT IN ACL RECONSTRUCTION IN THE SKELETALLY-IMMATURE KNEE
457
Table II. Changes in graft/tunnel dimensions over time/growth Case Period of follow-up (mths) Age (yrs, mths) At surgery At follow-up Height gain (cm) Femoral tunnel diameter (mm) Start to finish Change Tibial tunnel diameter (mm) Start to finish Increase
1
2
3
38
37
58
18
22
12, 3 15, 5 18.5
13, 10 16, 11 15
12, 6 17, 4 15
14, 3 15, 9 14
14, 2 15, 11 24
5
6 to 6 0
7.5 to 7.5 0
7 to 7 0
6.5 to 6.5 0
6.5 to 6.5 0
6 to 6 0
7.5 to 7.5 0
7 to 7.5 0.5 (metaphysis) 2 (epiphysis)
6.5 to 6.5 0
6.5 to 6.5 0
Tibial tunnel length (mm) Start to finish 40 to 52 Increase 12 Percentage increase 30 Femoral tunnel length (mm) Start to finish 40 to 80 Increase 40 Percentage increase 100 Length of intra-articular portion of graft (mm) Start to finish 20 to 25 Increase 5 Percentage increase 25 Length of whole graft (mm) Start to finish 100 to 157 Increase 57 Percentage increase 57
42 to 50 8 19
39 to 50 11 28
56 to 71 15 27
50 to 70 20 40
37 to 60 23 62
34 to 54 20 59
35 to 60 25 71
40 to 75 35 88
23 to 26 3 13
33 to 37 4 12
25 to 27 2 8
25 to 30 5 20
102 to 136 34 33
106 to 141 35 33
116 to 158 42 36
115 to 175 60 52
graft is seen at the growth plate owing to the faster growth in the metaphysis, and slower growth in the epiphysis (Fig. 3). In only one patient (case 3) was there any widening of the tunnel. Widening of 2 mm occurred in the tibial tunnel and was confined to that part of the tunnel proximal to the growth plate ‘scar’. The remaining tunnel was 0.5 mm wider. In all cases the unharvested pes anserinus tendons maintained the normal position of attachment to the tibia. In two, the harvested semitendinosus and gracilis tendons were left attached to the tibia by the external aperture of the tibial tunnel, which then subsequently migrated distally (Fig. 4). At the last follow-up, when the final MR scans were taken, in keeping with skeletally-mature patients who have undergone ACL reconstruction, all patients had a weakly positive Lachman test11 (grade 1) and three of the five had grade 1 laxity of the anterior drawer test.12 The remainder had a normal anterior drawer test. All of these tests were associated with a firm endpoint. No patient had a positive pivot shift. Laximetry testing was not used in this series. All five patients returned to the same level of sporting activity after operation. Case 1 sustained a further tear of the lateral meniscus, while playing football 38 months after it had been repaired, at the time of reconstruction of the ACL. This was repaired again, and to date, 36 months later, he remains asymptomatic. Case 3 had a new injury playing rugby 18 months after ACL reconstruction, resulting in a VOL. 90-B, No. 4, APRIL 2008
4
bucket-handle tear of the medial meniscus, which was repaired. A further 12 months later it tore again in a twisting injury, again playing rugby, and partial meniscectomy was undertaken.
Discussion The dramatic lengthening measured in these grafts poses an intriguing question: either the graft grows or stretches, or a combination of both occurs. As the girth of the graft remains the same, in view of the marked increases in length recorded, it seems logical that growth of the graft occurs. The density of the graft tissue cannot be reliably assessed in our study, and a redistribution of graft structure in a larger volume cannot be excluded. However, the MRI signals of the grafts were typical of hamstring grafts in adults. It is our experience that the abnormal excess anteroposterior laxity, present at post-operative examination, diminishes over time. As our results demonstrate that the graft elongates, tightening of the graft with time may indicate that lengthening of the graft does not keep up with bony growth, implying that some stretching takes place. An alternative explanation may be that in healing of the graft some tightening occurs. Excess tension in the graft may be a causative factor in cases in which growth arrest occurs due to eccentric ‘tethering’ of the physis.13 With pure stretching one would expect thinning of the graft as it elongated. Despite the great changes in length, there was no change in the diameter of the graft in four of
458
S. BOLLEN, F. PEASE, A. EHRENRAICH, S. CHURCH, J. SKINNER, A. WILLIAMS
Fig. 3
Fig. 4
Sagittal MRI showing the angulation of the graft in the tibia at the growth plate (arrow) caused by differential growth in the epiphysis and metaphysis.
five of our cases; in the other there was a small increase in the width of the tunnel. This does not necessarily mean that the graft has grown, as it could be due to an expansion of the bony tunnel. The biological events surrounding graft healing and maturation are poorly understood. This is exemplified when considering the following case report.14 At six weeks following ACL reconstruction with the hamstrings a discharging haematoma required debridement of the wound and no fixation device or graft was left in the tibial tunnel. Despite this, a healthy intra-articular graft was seen at arthroscopy at the time, and an excellent long-term result with no more than average excess laxity was achieved.14 Studies using animal models confirm that hamstring grafts heal and appear similar to native ACL tissue histologically.15 But what of the elongation seen following ACL reconstruction in the growing adolescent? There has been considerable interest in muscle/tendon growth following chronic traction for bone lengthening procedures. Sun et al16,17 looked at the net weight and length gain of muscular and tendinous portions. Histological examination concluded that myofibrillogenesis does exist in traction neogenesis near the myotendinous junction. However, although tissue neogenesis in limb lengthening has been investigated, it has not been assessed in graft elongation in the growing subject. The striking difference is that the tissues in limb lengthening are vascular and innervated vital tissues, whereas a graft is initially avascular, and perhaps always aneural, and at least to begin with, mainly dead. The observation regarding the pes anserinus attachment is hard to explain. Presumably, local mechanical stresses and growth factors determine proper tendon attachment.
Coronal MRI showing the elongated anterior cruciate ligament graft. Note the position of the pes anserinus tendons (oval) in the correct anatomical position, despite the graft (semitendinosus and gracilis) having been left attached to the tibia at surgery, and the external tibial tunnel aperture (circle) which has migrated distally.
There are obvious weaknesses in this study. Our series is small, but the findings are so consistent that we believe that they are noteworthy. There are inevitably problems with measuring the inclination of tunnels in three dimensions from radiographs with variable magnifications, as radiographs are two-dimensional. There are also problems with measuring short distances in this manner. However, this was only done for the intra-articular portion, which is the smallest part of the graft, immediately after reconstruction. Nevertheless, our findings are dramatic and provide new information on the change in dimensions of the graft in the growing patient. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
References 1. Aichroth PM, Patel DV, Zorrilla P. The natural history and treatment of rupture of the anterior cruciate ligament in children and adolescents: a prospective review. J Bone Joint Surg [Br] 2002;84-B:38-41. 2. Janary PM, Nyrström A, Werner S, Hirsch G. Anterior cruciate ligament injuries in skeletally immature patients. J Pediatr Orthop 1996;16:673-7. 3. Mizuta H, Kubota K, Shiraishi M, et al. The conservative treatment of complete tears of the anterior cruciate ligament in skeletally immature patients. J Bone Joint Surg [Br] 1995;77-B:890-4. 4. Arbes S, Resinger C, Vécsei V, Nau T. The functional outcome of total tears of the anterior cruciate ligament (ACL) in the skeletally immature patient. Int Orthop 2007;31:471-5. 5. Kocher MS, Saxon HS, Hovis WD, Hawkins RJ. Management and complications of anterior cruciate ligament injuries in skeletally immature patients: survey of Herodicus Society and the ACL Study Group. J Pediatr Orthop 2002;22:452-7. 6. McIntosh AL, Dahm DL, Stuart MJ. Anterior cruciate ligament reconstruction in the skeletally immature patient. Arthroscopy 2006;22:1325-30.
THE JOURNAL OF BONE AND JOINT SURGERY
CHANGES IN THE FOUR-STRAND HAMSTRING GRAFT IN ACL RECONSTRUCTION IN THE SKELETALLY-IMMATURE KNEE
7. Matava MJ, Siegel MG. Arthroscopic reconstruction of the ACL with semitendinosus-gracilis in skeletally immature adolescent patients. Am J Knee Surg 1997;10:609. 8. Fuchs R, Wheatley W, Uribe JW, et al. Intra-articular anterior cruciate ligament reconstruction using patellar tendon allograft in the skeletally immature patient. Arthroscopy 2002;18:824-8. 9. Shelbourne KD, Patel DV, McCarroll JR. Management of anterior cruciate ligament injuries in skeletally immature adolescents. Knee Surg Sports Traumatol Arthrosc 1996;4:68-74. 10. Tanner JM. The development of the reproductive system. In: Growth at adolescence. Second ed. Oxford: Blackwell Scientific, 1962:28-39. 11. Torg JS, Conrad W, Kalen V. Clinical diagnosis of anterior cruciate ligament instability in the athlete. Am J Sports Med 1976;4:84-93. 12. Marshall JL, Wang JB, Furman W, Girgis FG, Warren R. The anterior drawer sign: what is it? J Sports Med 1975;3:152-8.
VOL. 90-B, No. 4, APRIL 2008
459
13. Edwards TB, Greene CC, Baratta RV, Zieske A, Willis RB. The effect of placing a tensioned graft across open growth plates: a gross and histological analysis. J Bone Joint Surg [Am] 2001;83-A:725-34. 14. Logan M, Williams A, Myers P. Is bone tunnel osseointegration in hamstring tendon autograft anterior cruciate ligament reconstruction important? Arthroscopy 2003;19:1-3. 15. Goradia VK, Rochat MC, Kida M, Grana WA. Natural history of a hamstring tendon autograft used for anterior cruciate ligament reconstruction in a sheep model. Am J Sports Med 2000;28:40-6. 16. Sun JS, Hou SM, Liu TK, Lu KS. Analysis of neogenesis in rabbit skeletal muscles after chronic traction. Histol Histopathol 1994:699-703. 17. Sun JS, Hou SM, Hang YS, Liu TK, Lu KS. Ultrastructural studies on myofibrillogenesis and neogenesis of skeletal muscles after prolonged traction in rabbits. Histol Histopathol 1996;11:285-92.