too use purified PI as vaccinogen. The results of immunisation with PI in animal studies were howeverr disappointing (110), showing the same lymphocyte ...
CHAPTERR 1
Generall Introduction
rr
Introduction Introduction
GENERALL INTRODUCTION 1.. Description of the organism 1.11 History Inn 1944 Eaton and colleagues described an agent that passed through filters with pore sizes thatt retain bacteria and caused pneumonia when inoculated in rodents (1). The agent was believedd to be a virus as it passed through bacteriologie filters and could be grown in chicken embryoss only. The relation of the agent to the primary atypical pneumonia (PAP) syndrome waswas suggested by the fact that human serum from patients recovering from PAP neutralised thee agent. In the early 1960ies it was established that the organism had many characteristics in commonn with the pleuro pneumonia-like organisms (PPLO) isolated in 1898 by Nocard and co-workerss and causing contagious pleuropneumonia in cattle. Its mycoplasmal nature was establishedd by growing the agent on cell free medium (2), and subsequently it was appropriatelyy named Mycoplasma pneumoniae. 1.22 Taxonomy M.M. pneumoniae is one of the currently recognised 102 Mycoplasma species in the order of Mycoplasmatales.. Thirteen of these 102 Mycoplasma species have been isolated from humans.. Mycoplasmas are classified in the Class Mollicutes (mollis=soft, cutis = skin) which namee originates from the lack of a rigid cell wall, separating mycoplasmas from other bacteria.. They are bounded by a cell membrane containing sterols. Because of their deformablee membrane and small size (150-250 nm), mycoplasmas are able to pass through bacteriologiee filters. As mycoplasmas lack a typical bacterial cell wall, they are not visible on Gramm staining and resistant to cell wall-active antimicrobial agents such as penicillins and cephalosporins.. Mycoplasmas are able to grow in cell free media and belong to the smallest self-replicatingg organisms with genome sizes of 580-1350 kb. Recently, sequence data from thee entire genomes of M. pneumoniae (3) and M. genilalium (4) became available. This informationn will enhance the knowledge of the molecular biological basis of these microorganisms.. The small genome is remarkable for such successful pathogens. The question iss whether there is any relation between genome size and the ability of mycoplasmas to grow inn vitro. Recently, Hutchison el al. sorted out the number of essential genes necessary for replicationn of M. genilalium (5). Their conclusion was that 140 of the 340 genes, at least under laboratoryy conditions, are not a prerequisite for the propagation of this smallest-known freelivingg micro-organism. In addition, obligate intracellular bacteria like Chlamydia pneumoniae, CoxiellaCoxiella burnetii, and Rickettsia species have genomes larger than many of the self-replicating mollicutes,, making a direct relation between genome size and the ability to grow in vitro unlikely.. The genome sequence projects provided the genetic explanation for the requirements
99
ChapterChapter 1
off serum, peptone, and yeast extract in nutritious growth media for the in vitro growth of mycoplasmas.. Only a limited number of genes allows biosynthetic pathways in mycoplasmas andd no genes are present for amino acid synthesis (3,4). Therefore, M. pneumoniae and M genitaliumgenitalium are totally dependent on exogenous supply of omino acids. M.M. pneumoniae is a filamentous organism, about 10x200 nm in size, with a genome of 816 kb.. Mycoplasmal DNA has an exceptional low guanine and cytosine (G&C) content, with M. pneumoniaepneumoniae
showing the highest G&C content of 40 mol% of the entire genome.
Characteristicc for mycoplasmas is the use of TGA as a tryptophan codon instead of a stop codon.. The flask shaped cells of M. pneumoniae have a terminal tip structure and exhibit glidingg motility on solid surfaces (6,7). The terminal tip structure is responsible for attachment off the organism to cell membranes. Of the surface proteins required for cytadherence, the 169 kDaa protein PI has been most extensively studied (8-11). 1.33 Habitat Humann mycoplasmas colonise mucous membranes in the ororespiratory or genitourinary tract,, where some species behave as commensals. Under immune suppression, for example afterr organ transplantation, in AIDS patients or in patients with hypogammaglobulinacmia, isolationn of mycoplasmas from joints, pericardial tissue or from respiratory tract tissue differentt from their usual habitat has been described (12,13). Humann mycoplasmas have been shown to be taken up by polymorphonuclear leukocytes (PMNL)) and macrophages (14), but whether mycoplasmas can enter epithelial cells is unclear. M.M. fermentans and M. penetrans have been found in nonphagocytic cells in AIDS patients (15,16).. The mechanism of cell entry is not fully understood. The specialised tip structure of M.M. genitalium and M. penetrans seems to play a role in cell entry but also mycoplasma species lackingg a tip structure like M. fermentans and M. hominis have been found intracellular by electronicc microscopy (17). Whetherr mycoplasmas replicate intracellular^ remains to be resolved. There are indicationss for cell lysis of human lung fibroblasts after infection with M. genitalium (18) and celll disruption after invasion with hi. penetrans (16). The intracellular localisation can protect mycoplasmass against the host immune system and antibiotics and may be responsible for latentt or chronic infection states. M.M. pneumoniae has been shown to parasitize cell surfaces of mammalian cells and to enter thee intracellular environment where it is located throughout the cytoplasm and perinuclear regions.. It can persist intracellularly for at least 7 days (19). Baseman isolated M. pneumoniae mutants,, which are able to cytadhere but not to invade cells, suggesting separate mechanisms forr adherence and invasion (19).
10 0
Introduction Introduction
2.2. Epidemiology 2.11 Epidemiology M.M. pneumoniae causes usually a mild respiratory disease. Most cases will not lead to a doctor'ss visit and confirmed diagnosis is often not accomplished in daily practice. Available dataa on morbidity and mortality due to M. pneumoniae
infection from regular sources
(statisticss of death due to pneumonia, statistics on hospitalisation due to pneumonia or laboratoryy data on M. pneumoniae infection) thus will reveal only a minor part of actually occurringg M. pneumoniae infections. Thee way diagnosis of a M pneumoniae infection is established will influence the outcome off epidemiological studies. Most studies on M. pneumoniae epidemiology performed in the past,, made use of data obtained by serological testing or by culture of the organism. A deficientt knowledge in parameters influencing the antibody response exists. Persistent antibodiess and antibody response after reinfection may differ and probably depend on the age andd immune status of the people under investigation. Although isolation of M. pneumoniae is tediouss and takes several weeks to complete, culture of M. pneumoniae
has provided
additionall information for epidemiology of the organism only in settings in which special attentionn to culture was paid. Prolonged shedding of the micro-organism has been described in certainn populations and is probably related to several factors like the immune status of the host,, the age of the host, intervention with antibiotics, and may be, the virulence of the strain. However,, the asymptomatic carrier state is believed to be rare, although contradictionary resultss have been reported (20,21). Manyy studies have been performed in outbreak investigations of respiratory disease due to M.M. pneumoniae, for example among military and in boarding schools (22-24). Long term studies,, as performed in civilian populations in Seattle (1962-1975)(25) and Tecumseh (26), havee provided data on community infection rates and epidemiological patterns. M.M. pneumoniae infection occurs in temperate climates throughout the year, but the absolute numberr of infections is higher during the winter season. Because most respiratory infections duee to other pathogens such as rhinovirus, respiratory syncytial virus and influenzavirus occur inn wintertime, the proportion of M. pneumoniae infection among respiratory infections is highestt in summer. Althoughh M. pneumoniae is endemic in most civilian populations where the infection has beenn sought for, an epidemic pattern is evident from long-term population studies (27-32). Epidemicss occur with intervals of 4-5 years. However, a change in this epidemic pattern has beenn observed in Denmark, possibly related to a change of protective immunity in children, whichh can be a result from increased use of day-care facilities (27). As can be concluded from longg term population studies among patients with pneumonia (25) and data from laboratories registeringg M. pneumoniae
infection (29)(this thesis), the more severe M. pneumoniae
11 1
ChapterChapter 1
infections,, occur predominantly in school-age children, with another incidence peak in young adults.. Although these data suggest that the overall incidence is lowest in the over 40 age group,, it is likely that there is an underestimation of M. pneumoniae infection occurring in peoplee older than 40 years. Antibody titers due to M. pneumoniae infection in older people are significantlyy lower compared to younger people (29; this thesis, Chapter 3), implying that M.
pneumoniaepneumoniae infection in the older age groups is not diagnosed in case only serological assays aree performed. In studies performed among outpatient populations with respiratory tract infection,, in which diagnosis of M. pneumoniae infection was made by PCR, no difference in incidencee between the different age groups is found (33; this thesis, Chapter 5). 2.22 Results of registration o/M. pneumoniae from Laboratory Reporting Systems in Europe Too gain insight into the epidemiological pattern of M. pneumoniae in Europe, the data from nationall diagnostic laboratory reporting systems in different countries have been analysed. Onlyy countries having data reported per quarter or per month for at least 10 years were included.. These countries were: Finland (1972-1998)(34), England and Wales (19751998X35),, the Netherlands (1981-1998)(36) and Denmark (1972-1999)(37). Data from Icelandd (1987-1996) reported earlier (29), were also included in the analysis. As M. pneumoniaepneumoniae
infection is not a notifiable disease, the information available is based on
volunteerr reporting systems (Finland, England/Wales, the Netherlands) or on data from the nationall laboratory performing M. pneumoniae tests (Denmark, Iceland). The reported data obtainedd from laboratory diagnosed M. pneumoniae
infection, most often by antibody
detectionn in serum (CFT and/or EUSA), are presented as absolute numbers. Inn those countries for which monthly data were available, most infections occurred during thee winter period (November until March)(Fig 1). In epidemic episodes, however, the infectionn is diagnosed during the whole year, without preference for the winter period (Fig 2). Thee data showed that endemic cases occur on a regular basis with epidemic outbreaks every 4 too 5 years. This pattern is most regular in England/Wales and possibly in Iceland, for which countryy only 10 years data are available. Epidemic outbreaks in the different countries do not alwayss coincide (Fig 2), most likely because of the protective immunity built up in a certain population. . Thee laboratory reporting systems from England/Wales and the Netherlands also register sex andd age of the patients diagnosed with M. pneumoniae. M. pneumoniae infection occurred slightlyy more frequent in male patients with an exception for the 16 to 40 years age group in whichh more female patients were diagnosed with M, pneumoniae infection (Fig 3). In both countriess there was a peak incidence of infections in young children (4 to 10 years) and a smaller,, second peak in adults of 30 to 40 years old (Fig 4).
12 2
Introduction Introduction
England/Wales s (1975-1998) ) 3000 0 2500 0 2000 0 1500 0 1000 0 500 0 00 44 week periods
Thee Netherlands (1981-1999) ) 1200 0 1000 0 800 0 600 0 400 0 200 0 55
00 jann
feb mrch apr
may June July
aug sept
oct
nov
dec
aug sept
oct
nov
dec
nov
dec
Finland d (1972-1999) ) 1600 1400 1200 1000 800 600 400 200 0
0 0 0 0 0 0 0 0 0 jann
feb mrch apr
may June July
Denmark k (1990-1999) ) 2000 0 1500 0 1000 0 500 0
l.n.n.n.nn n I:
00 jann
II m I m I HM I n a I i leb mrch apr may June July aug sept
oct
Figuree 1 Seasonall distribution of M. pneumoniae in 4 Northern European Countries (data derived from (34-37))
13 3
ChapterChapter I
MpMp reports &igland/Wales (per month) (n=24,239) ) 400 0
755
77
79
81
83
85
87
89
91
93
95
97
Mpp reports the Netherlands (per month) (n=9672) ) 250 0 200 0
150 0 100 0
vlhMu^li^^ ^
50 0
811 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 MpMp reports Finland (per month) (n=12,105) )
722 74 76
78 80 82 84
86 88 90 92
94 96 98
MpMp reports Denmark (per quarter) (n=29,333) )
1500 0
833
86
89
92
95
98
MpMp reports beland (per quarter) (n=762) ) 60 0 40 0 30 0 20 0 10 0
iMii lAiiili 93 3
Figuree 2 Endemicc and epidemic periods of M. pneumoniae as registered by clinical diagnostic Northernn European countries (data derived from(29;34-37))
14 4
laboratories in 5
Introduction Introduction
Agee and Sex distribution rVfc patients England/Waless 1990-98
(n=12,943) ) 2500 0 2000 0 1500 0
number r 1000 0 500 0
AA AA II I 0-44
II male II female
5-15 16-25 26-40 41-60 > 60 agee category
Agee and Sex distribution N^> patients thee Netherlands 1986-94 (n=4892) ) 1000 0
fa fa
11 11 1
800 0
600 0 number r 400 0
r?fl
jj j
200 0
00
0-44
I—HL
Ell male female
IJIJtlLBi i 5-15 16-25 26-40 41-60 >60 agee category
Figuree 3 Agee and sex distribution of patients diagnosed with M. pneumoniae Netherlandss (data derived from (35;36))
infection in England/Wales and the
15 5
ChapterChapter I
Mpp infections by age (England/Wales 75-98) (n=28,609) )
IlllllllMlMUl l 00
5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 age e
Mpp infections by age (the Netherlands 81-96) (n=7020) )
II
O OO
number r
4000
100 0
III I lilllllllllllllillllllllllllllllllliii
..i,inil,in....,i,l.iM.
33 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 age e
Figuree 4 Agee distribution of patients diagnosed with M. pneumoniae infection in England/Wales and the Netherlands (data derivedd from (35;36))
16 6
Introduction Introduction
2.33 Transmission Transmissionn of respiratory pathogens can occur by aerosols (e.g. influenza virus, BordetellaBordetella spp.), by personal contact (e.g. Epstein-Barr virus) or even via contaminated objectss (respiratory syncytial virus). In the case of M. pneumoniae it is uncertain whether the spreadd is primarily by droplets, or by direct or indirect contact, or by all of these three routes. Infectionn with M. pneumoniae with small-particles (2-3um) in the hamster model resulted in bothh upper and lower respiratory tract infection, whereas infection after exposure to largeparticlee aerosols was limited to the upper respiratory tract (38). Thee incubation period of M. pneumoniae is approximately 3 weeks. Spread of a M. pneumoniaepneumoniae
infection
in
the community
is slow.
However,
within
communities,
microepidemicss can arise, in which spread probably occurs from person to person. Only a few commonn source outbreaks of M. pneumoniae have been reported (39-41).
3.. Clinical disease 3.11 Respiratory infection M.M. pneumoniae infection should be suspected in patients with a respiratory infection with clinicall symptoms as seen with influenza-like illnesses such as fever, cough, headache, malaise,, and myalgia although the onset of an infection with M. pneumoniae is usually less abruptt compared to an influenza virus infection. Also in people with milder respiratory infectionss M. pneumoniae may be the cause of such a disease. Non-productive cough is a characteristicc sign in M. pneumoniae infection. In children cough can be paroxysmal. In an estimatedd 5-10% of patients M. pneumoniae infection progresses to tracheobronchitis or pneumonia.. Sputum may be produced in such cases. Gram staining of sputum specimens revealss only inflammatory cells. Pneumonia is usually mild and self-limited, resolving even withoutt antibiotic treatment (42). However, severe and fulminant cases have been reported (43,44)) and may be underdiagnosed. 3.22 Complications AA variety of complications of M. pneumoniae infection have been described, but their frequenciess are rarely known (45). Skin rashes, one of the commonest complications occurred inn 10-20% of the recognised M. pneumoniae infections (46,47). The Stevens Johnson syndromee (erythema multiforme) although rare, can be a life threatening complication. Other non-pulmonaryy common complications comprise haemolytic anaemia, thrombocytopenia, thrombosiss
and
disseminated
intra-vasculair
coagulation.
Furthermore,
neurological
complicationss like encephalitis, meningitis and the Guillain Barre syndrome, but also myocarditiss and arthritis have been described and are believed to be due to circulating
17 7
ChapterChapter 1
immunee complexes. Recovery of the organism from cerebrospinal fluid (48,49), synovial fluid (50-52)) and the description of mycoplasmal bacteremia as detected by molecular methods (53,54)) suggest systemic spread of the bacterium.
4.. The bacterium and the host 4.11 Virulence and evasion of the host immune response Thee clinical picture of mycoplasma infections is more suggestive of damage due to host immunee and inflammatory responses rather than to direct effects by mycoplasma cell components.. M. pneumoniae
can be considered as a surface parasite of the respiratory
epithelium.. The adhesion is essential for colonisation and infection as the loss of adhesive capacityy results in loss of infectivity. For M. pneumoniae and M. genitalium the mycoplasma adhesins,, their genes (PI, P30, and MgPa) and encoded proteins have been studied most extensively.. The topography of the adhesion molecules with epitope mapping using monoclonall antibodies against adhesion molecules in situ and against synthetic oligopeptides providedd insight into the conformation of the adhesins in the membrane (55). However, in M.
pneumoniaepneumoniae a number of accessory membrane proteins are involved in the process of gliding motilityy and concentration of the adhesin molecules at the attachment tip organelle. Some of thee genes and encoded proteins of the M. pneumoniae cytoskeleton have been identified (30, 400 & 90 kDa, P65 and HMW1 and HMW3) and are shown to be proline rich and possess otherr characteristics of eukaryotic cytoskeletal proteins (56-59). Forr persistence in the host, pathogenic bacteria develop mechanisms to deal with the host immunee response. One of these mechanisms consists of variation in antigenic structure in orderr to avoid host immune recognition. For M. hominis deletions in a repeat-containing gene encodingg a surface localised antigen resulted in antigenic variation (60). Also in the case of M. genitaliumgenitalium regions in the MgPa adhesin gene encoding adherence mediating epitopes have beenn described to be highly variable, thus leading to avoidance of the host immune response (61).. For M. pneumoniae, deletion of repeated sequences in the gene encoding the 30 kDa proteinn of the M, pneumoniae attachment organelle, resulted in a hemadsorption negative mutantt of M. pneumoniae (62). Regions of the PI cytadherence gene which are recognised by cytadherence-inhibitingg anti PI monoclonal antibodies have been shown to vary, at least betweenn PI group I and II M. pneumoniae isolates (63,64). 4.22 Host susceptibility to M. pneumoniae infection Peoplee with congenital or acquired immunodeficiencies are recognised to be more susceptiblee for a variety of mycoplasma infections. The number of recurrences of M.
pneumoniaepneumoniae infection in such patients compared to people with normal immunity is also
18 8
Introduction Introduction
higher.. In hypogammaglobulinaemic patients and in patients undergoing organ transplantation andd immunosuppressive therapy, dissemination of mycoplasmas such as M. pneumoniae, M. hominishominis and Ureaplasma urealyticum to joint and bone tissue has been reported (50,65-69). Primaryy infection with M. pneumoniae does not protect against a subsequent infection with thee bacterium as follows from clinical studies (70) and animal studies (71). Reinfected animalss show more lymphocyte infiltration than primary infected animals, indicating that specificc cell-mediated host response might play a role in the pathology of a reinfection. Experimentall reinfections of mice showed elevated mRNA expressions for proinflammatory cytokiness (72). In humans, the difference in clinical disease between a mild primary infection andd more severe manifestations after a second infection with M. pneumoniae (73), might be duee to enhanced immune response as found in the reinfected animals (74).
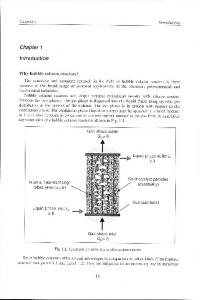
5.. Diagnosis Diagnosiss of M. pneumoniae infection relies mainly on laboratory tests, as discrimination off M pneumoniae from other (mostly viral) respiratory pathogens on clinical parameters only, iss difficult (75). Specific laboratory diagnosis can be made directly, by culture or detection of antigenn or DNA of the organism, or indirectly by detection of antibodies. 5.11 Culture Culturee of M. pneumoniae is labour intensive and requires specific media and experienced personnell to perform. M. pneumoniae is a relatively slow growing bacterium. After adaptation too artificial media the mean generation time is 6 hours (76). In clinical practice this means that incubationn from 1 week to 4 weeks is necessary for propagation of the micro-organism, which makess culture inappropriate for the routine diagnosis in a clinical setting. If culture is attempted,, the transport medium should contain peptide broth, serum albumin and antibiotics too retard overgrowth by other bacteria. Throat swabs, nasopharyngeal aspirates and sputum sampless are all suitable for culturing of M. pneumoniae, provided they have been suspended in appropriatee transport medium. Inoculation should be performed within 24 h or, if not possible, sampless should be stored at -70 °C. Culture media to be used for M pneumoniae have to containn beef heart infusion broth, supplemented with fresh yeast extract and horse serum providingg sterols and nucleic acid precursors. Inoculation is performed using both solid and liquidd medium, the latter containing glucose and phenol red. M. pneumoniae
ferments
glucose,, which is detected by a colour change of the medium from red into yellow. On solid mediaa M. pneumoniae appears in 'mulberry' colonies (Fig 5), which are able to hemadsorb chickk and guinea pig erythrocytes. Specific antisera are required to provide definite identification,, although close serologic relationship between M. pneumoniae
and M.
19 9
ChapterChapter I
genitaliumgenitalium may encounter difficulties in identification (77). Although the usefulness of culturingg M. pneumoniae in daily practice is limited, culture remains important as a standard inn studies in which non-cultural methods are evaluated. Also the development of antimicrobial drugg resistance and antigenic variation can only be studied if clinical isolates of M. pneumoniaepneumoniae are available.
Figuree 5 MM pneumoniae colonies on agar (40x magnification) (courtesy to AF Angulo, RIVM Bilthoven, The Netherlands) )
5.22 Direct detection of M. pneumoniae Ass an alternative for culture, direct antigen tests have been developed. A species specific probee test (Gene-Probe), an EIA and immunoblot assays making use of monoclonal antibodies againstt M. pneumoniae proteins have been applied in direct detection of (antigen of) the micro-organismm in nasopharyngeal specimens (78,79). Inn the last decade studies using amplification of species specific fragments of the M.
pneumoniaepneumoniae genome by PCR have been published. Target sequences used for molecula detectionn of M. pneumoniae are mostly chosen in the PI cytadhesin gene (80-85) or in the 16 SrRNAA gene (86,87). Forr preparation of clinical samples before amplification, various procedures have been described.. Since mycoplasmas lack bacterial cell wall material, DNA can be made available byy relative simple procedures. A boil-freeze method (thermal shock) has been applied to nasopharyngeall aspirates (85) and also lysis with proteinase K on aspirates (88), bronchoalveolarr lavages (84), and throat swab specimens (75,89) has been applied. For preparationn of tissue or blood specimens a more elaborate DNA extraction is required. The
20 0
Introduction Introduction
usee of an internal process control is necessary in order to avoid false negative results (82,85,90).. Up to 20% of the throat swab samples after a proteinase K lysis showed inhibition off the amplification process (90) and up to 25% of nasopharyngeal aspirates after freezeboilingg showed inhibition of the PCR (85), as detected by the lack of the internal control band afterr gelelectrophoresis. Using 6 globine primers, a more roughly way to test for inhibition, up too 10% of the aspirates showed inhibition after proteinase K lysis (88). Identification of the PCRR products has been performed by (microliter well) hybridisation (89,91) as well as by a nestedd PCR (90). Detection limits of M. pneumoniae by PCR in clinical samples have been describedd to vary between 1.0-50 colony forming unit (CFU), 10-100 colour changing units (CCU)) and 5-50 fg of template DNA (53,82,87,90,92). Only a few studies compared reproducibilityy of PCR results obtained with different primersets in different laboratories (75,85). . 5.33 Serology Inn routine laboratories antibody detection in serum is the most commonly used technique in diagnosiss of M. pneumoniae infection. The first serological assay performed was the cold hemagglutininn (CA) test. Cold agglutinins are non-specific IgM class antibodies against the I antigenn of erythrocytes. The specificity of the test can be increased when a cut-off titre of >40 iss used as diagnostic criterion (93). As more specific tests became available, the CA test is not commonlyy used anymore. Thee most widely used serological assay is the complement fixation test (CFT) in which CF antibodiess against M. pneumoniae, in conjunction with antibodies against other, mostly viral, respiratoryy pathogens are determined. The sensitivity of this assay depends on whether the firstt serum sample is collected early or late after onset of illness and on the availability of pairedd sera collected with an interval of 2 to 3 weeks. On interpretation of positive CF titers onee has to bear in mind that the membrane glycolipids-based antigen from M. pneumoniae is notnot highly specific. Cross reactivity with e.g. vegetable lipids (94) and human brain tissue antigenss has been demonstrated (95). ELISAA tests have been developed to detect specific immunoglobulins of different classes, mostt of them using a crude M. pneumoniae
antigen, which includes the cross reacting
glycolipidd fraction. More specific test results can be obtained by using isolated PI protein as antigen,, which is one of the major virulence factors of M. pneumoniae (96). Proteins derived fromm parts of the PI gene have also been applied as antigen in an ELISA test (97). Commerciall availability of these tests sofar is limited. Immunoblotting, to confirm positive resultss from the less specific serological assays, have shown strong reactivity against the 169 kDaa PI protein of M. pneumoniae (98), but reactivity against this protein among clinically healthyy persons interferes with conclusive interpretation. Recently, a commercially available
21 1
ChapterChapter I
immunoblott making use of various recombinant proteins based on M. pneumoniae genome sequencee data (3) has been developed.
6.. Treatment and prevention 6.11 Treatment Upperr respiratory tract infection due to M. pneumoniae is mostly undiagnosed and is not treatedd with antibiotics. Also pneumonia is often a self-limiting disease, but appropriate antimicrobiall treatment shortens the duration of the illness (99; 100). Respiratory infection causedd by M. pneumoniae
is generally treated with tetracycline or erythromycin. As
mycoplasmass lack a cell wall, M. pneumoniae is unaffected by B-lactam antibiotics such as penicillinn
and cephalosporins. Clinical
improvement
upon institution of
appropriate
antimicrobiall therapy is not always accompanied by early eradication of the organism from the respiratoryy tract. The capacity of M. pneumoniae to reside intracellular^ may be responsible forr this. Also the newer macrolides (clarithromycin and azithromycin) and to lesser extent fluoroquinoloness have been found to have in vitro and in vivo activity against M. pneumoniae (101). . 6.22 Prevention Inn terms of transmission, the respiratory route is the least subject to effective control of infectiouss diseases. In non-respiratory transmission such as vehicle-borne, gastro-intestinal infections,, intervention is possible in the food chain or in drinking water systems (102; 103). Inn case of vector borne infections the vector can be eliminated (104) and in case of genital infectionss change in behaviour will reduce transmission of the causative micro-organism (105).. For some respiratory pathogens control is possible by intervention in the environment. Thiss is the case for example with Legionella pneumophila (106) or Chlamydia psittaci (107). However,, for many respiratory pathogens, including M. pneumoniae, environmental control is notnot feasible and the only way of controlling these infections is through immunisation of the hostt or providing chemoprofylaxis. Preventionn of M. pneumoniae infection through vaccination has been studied as early as the 1960ies,, the time that M. pneumoniae was recognised as a respiratory pathogen. These early vaccinee studies made use of an inactivated M. pneumoniae vaccine after administration of whichh volunteers were challenged with agar-grown
mycoplasma. Those
responding
serologicallyy to the vaccination showed protection to respiratory infection. In volunteers who failedd to respond to the vaccine with antibody development, more severe disease developed afterr challenge compared with the controls (108). In larger vaccine trials among military personnell this sensitisation effect could not be confirmed and the protective efficacy of the
22 2
Introduction Introduction
vaccinee against development of M. pneumoniae pneumonia was about 66% in the first year followingg vaccination (109). However, the overall success of formalin inactivated vaccines hass been disappointing and no acceptable live vaccine has been developed for human use. Thee molecular characterisation of the major adhesin PI of M. pneumoniae, prompted trials too use purified PI as vaccinogen. The results of immunisation with PI in animal studies were howeverr disappointing (110), showing the same lymphocyte infiltration in lungtissue after challengee with M. pneumoniae in immunised animals compared to control animals. The conclusionn is that until now, no useful vaccine (inactivated or live) for M. pneumoniae has beenn developed. DNA vaccines, having the advantage of inducing both humoral and cell mediatedd response, have been applied successfully in animals preventing mycoplasmal disease (M.(M. pulmonis, M. hyopneumoniae) (111). This generation of vaccines may become useful in humann mycoplasma disease in the future as well. Onlyy limited data is available on the effect of prophylactic antibiotic use. In a long-term caree facility prophylactic antibiotic usage has shown to significantly reduce the secondary attackk rate of M. pneumoniae infection (112).
23 3
ChapterChapter I
Scopee of the thesis
MycoplasmaMycoplasma pneumoniae is a common respiratory pathogen in humans. The usual mild clinicall presentation of the infected patient does not encourage laboratory diagnosis to be performed.. However, in case antibiotic treatment is instituted this should be different from the firstt choice recommended antibiotics for respiratory infections in general practitioner (GP) settings.. As the organism is notorious for its difficult laboratory diagnosis, molecular techniquess should enable fast diagnosis and subsequently appropriate antibiotic treatment. Currentt knowledge of the epidemiology of M. pneumoniae is based on data predominantly derivedd from studies using serology or culture for diagnosis. Inn this thesis the value of molecular techniques in diagnosis of M. pneumoniae in both childrenn and adult patients with a respiratory infection is investigated (Chapters 2 and 3). For reliablee detection of M. pneumoniae DNA by PCR, control for inhibition of the amplification reactionn is required. Therefore, we developed an amplification control (AC) to detect inhibition,, which is described in chapter 4, This AC was applied to clinical specimens, submittedd for M. pneumoniae PCR. Furthermore, we applied a semiquantitative PCR to enablee discrimination of strong and weak positive PCR results in specimens obtained from hospitalisedd and non-hospitalised patients with a respiratory tract infection (Chapter 4). Too expand knowledge of epidemiological patterns of M. pneumoniae, the PCR was applied too nose/throat specimens obtained from patients with acute respiratory infection, identified by GPss in a routine surveillance for respiratory pathogens. M pneumoniae transmission was studiedd in the households of the M, pneumoniae positive patients (Chapter 5). Molecularr epidemiology of M. pneumoniae is hampered, as variation in its genome allows thee distinction of only two types. In order to refine molecular typing, clinical isolates of M.
pneumoniaepneumoniae collected over time in Denmark and the Netherlands, were subjected to various molecularr typing methods (Chapter 6). For identification of targets, which should enable directt genotyping of M. pneumoniae in clinical specimens, PI genes were sequenced. In addition,, these sequences were analysed to uncover possible mechanisms generating PI gene sequencee variation (Chapter 7).
24 4
Introduction Introduction
REFERENCES S 11 Eaton MD, Meikeljohn G, van Herick W. Studies on the etiology of primary atypical pneumonia:: A filterable agent transmissable to cotton rats, hamsters and chick embryos.. J Exp Med 1944; 79:649. 22 Chanock RM, Hayflick L, Barile MF. Growth on artificial medium of an agent associatedd with atypical pneumonia and its identification as a PPLO. Proc Natl Acad SciUSAA 1962; 48:41. 33 Himmelreich R, Hilbert H, Plagens H, Pirkl E, Li BC, Herrmann R. Complete sequencee analysis of the genome of the bacterium Mycoplasma pneumoniae. Nucleic Acidss Res 1996; 24:4420^449. 44 Fraser CM, Gocayne JD, White O, Adams MD, Clayton RA, Fleischmann RD et al. Thee minimal gene complement of Mycoplasma genitalium [see comments]. Science 1995;; 270:397-403. 55 Hutchison CA, Peterson SN, Gill SR, Cline RT, White O, Fraser CM et al. Global transposonn mutagenesis and a minimal Mycoplasma genome [see comments]. Science 1999;286:2165-2169. . 66 Feldner J, Bredt W, Razin S. Adherence of Mycoplasma pneumoniae to glass surfaces. Infectt Immun 1979; 26:70-75. 77 Miyata M. Mechanisms of mycoplasma chromosomal replication, cell division and glidingg motility. IOM letters: 12 th IOM Congress, Sydney ; 1998. 88 Baseman JB, Cole RM, Krause DC, Leith DK. Molecular basis for cytadsorption of MycoplasmaMycoplasma pneumoniae. J Bacteriol 1982; 151:1514-1522. 99 Su CJ, Tryon VV, Baseman JB. Cloning and sequence analysis of cytadhesin PI gene fromm Mycoplasma pneumoniae. Infect Immun 1987; 55:3023-3029. 100 Dallo SF, Su CJ, Horton JR, Baseman JB. Identification of PI gene domain containing epitope(s)) mediating Mycoplasma pneumoniae cytadherence. J Exp Med 1988; 167:718-723. . 111 Gerstenccker B, Jacobs E. Topological mapping of the Pl-adhcsin of Mycoplasma pneumoniaepneumoniae with adherence-inhibiting monoclonal antibodies. J Gen Microbiol 1990; 136:471-476. . 122 Bonilla HF, Chenoweth CE, Tully JG, Blythe LK, Robertson J A, Ognenovski VM et al.. Mycoplasma felis septic arthritis in a patient with hypogammaglobulinemia. Clin Infectt Dis 1997; 24:222-225. 133 Meyer RD, Clough W. Extragenital Mycoplasma hominis infections in adults: emphasiss on immunosuppression. Clin Infect Dis 1993; 17 Suppl 1:S243-S249. 144 Marshall AJ, Miles RJ, Richards L. The phagocytosis of mycoplasmas. J Med Microbioll 1995; 43:239-250. 155 Lo SC. Mycoplasmas in AIDS. In: Maniloff J, McElhaney RN, Finch LR, Baseman JB,, editors. MycopIasmas:molecular biology and pathogenesis. Washington, D.C.: ASM,, 1992: 525-545. . 166 Lo SC, Hayes MM, Kotani H, Pierce PF, Wear DJ, Newton PB et al. Adhesion onto andd invasion into mammalian cells by mycoplasma penetrans: a newly isolated mycoplasmaa from patients with AIDS. Mod Pathol 1993; 6:276-280. 177 Taylor RD, Davies HA, Sarathchandra P, Furr PM. Intracellular location of mycoplasmass in cultured cells demonstrated by immunocytochemistry and electron microscopy.. Int J Exp Pathol 1991; 72:705-714.
25 5
ChapterChapter I
188 Memaugh GR, Dallo SF, Holt SC, Baseman JB. Properties of adhering and nonadheringg populations of Mycoplasma genitalium. Clin Infect Dis 1993; 17 Suppl 1:S69-S78. . 199 Baseman JB, Lange M, Criscimagna NL, Giron J A, Thomas CA. Interplay between mycoplasmass and host target cells. Microb Pathog 1995; 19:105-116. 200 Gnarpe J, Lundback A, Sundelof B, Gnarpe H. Prevalence of Mycoplasma pneumoniaepneumoniae in subjectively healthy individuals. Scand J Infect Dis 1992; 24:161-164. 211 Foy HM, Kenny GE, McMahan R, Kaiser G, Grayston JT. Mycoplasma pneumoniae inn the community. Am J Epidemiol 1971; 93:55-67. 222 Mogabgab WJ. Mycoplasma pneumoniae and adenovirus respiratory illnesses in militaryy and university personnel, 1959-1966. Am Rev Respir Dis 1968; 97:345-358. 233 van der Veen J, van Nunen MCJ. Role of Mycoplasma pneumoniae in acute respiratoryy disease in a military population. Am J Hyg 1963; 78:293-301. 244 Fernald GW, Clyde-WA J. Epidemic pneumonia in university students. J Adolesc HealthHealth Care 1989; 10:520-526. 255 Foy HM, Kenny GE, Cooney MK, Allan ID. Long-term epidemiology of infections withh Mycoplasma pneumoniae. J Infect Dis 1979; 139:681-687. 266 Monto AS, Higgins MW, Ross HW. The Tecumseh study of respiratory illness. VIII. Acutee infection in chronic respiratory disease and comparison groups. Am Rev Respir Diss 1975; 111:27-36. 277 Lind K, Benzon MW, Jensen JS, Clyde-WA J. A seroepidemiological study of MycoplasmaMycoplasma pneumoniae infections in Denmark over the 50-year period 1946-1995. Eurr J Epidemiol 1997; 13:581-586. 288 Noah ND, Urquhart AM. Epidemiology of Mycoplasma pneumoniae infection in the Britishh Isles, 1974-9. J Infect 1980; 2:191-194. 299 Hauksdottir GS, Jonsson T, Sigurdardottir V, Love A. Seroepidemiology of MycoplasmaMycoplasma pneumoniae infections in Iceland 1987-96. Scand J Infect Dis 1998; 30:177-180. . 300 Rastawicki W, Kaluzewski S, Jagielski M. Occurrence of serologically verified MycoplasmaMycoplasma pneumoniae infections in Poland in 1970-1995. Eur J Epidemiol 1998; 14:37-40. . 311 Foy HM. Infections caused by Mycoplasma pneumoniae and possible carrier state in differentt populations of patients. Clin Infect Dis 1993; 17 Suppl LS37-S46. 322 Sasaki T, Kenri T, Okazaki N, Iseki M, Yamashita R, Shintani M et al. Epidemiologicall study of Mycoplasma pneumoniae infections in Japan based on PCRrestrictionn fragment length polymorphism of the PI cytadhesin gene. J Clin Microbiol 1996;; 34:447-449. 333 Layani-Milon MP, Gras I, Valette M, Luciani J, Stagnara J, Aymard M et al. Incidence off upper respiratory tract Mycoplasma pneumoniae infections among outpatients in Rhone-Alpes,, France, during five successive winter periods. J Clin Microbiol 1999; 37:1721-1726. . 344 Kleemola M, Ruutu P. Laboratory registration data M. pneumoniae in Finland. KTL, Helsinki.. Pers. Communication; 2000. 355 Watson J, Goddard N. Laboratory registration data M. pneumoniae in England and Wales.. PHLS, London. Pers. Communication; 2000. 366 Dutch Clinical Virology Group. Laboratory registration data M. pneumoniae in the Netherlands.. Pers. Communication; 2000. 377 Jensen JS. Laboratory registration data M. pneumoniae in Denmark. SSI, Copenhagen. Pers.. Communication; 2000.
26 6
Introduction Introduction
388 Collier AM, Clyde-WA J, Denny FW. Mycoplasma pneumoniae in hamster tracheal organn culture: immunofluorescent and electron microscopic studies. Proc Soc Exp Bioll Med 1971; 136:569-573. 399 Sande MA, Gadot F, Wenzel RP. Point source epidemic of Mycoplasma pneumoniae infectionn in a prosthodontics laboratory. Am Rev Respir Dis 1975; 112:213-217. 400 Sawyer R, Sommerville RG. An outbreak of Mycoplasma pneumoniae infection in a nuclearr submarine. JAMA 1966; 195:958-959. 411 Broome CV, La Venture M, Kaye HS, Davis AT, White H, Plikaytis BD et al. An explosivee outbreak of Mycoplasma pneumoniae infection in a summer camp. Pediatricss 1980; 66:884-888. 422 Licberman D, Schlaeffer F, Lieberman D, Horowitz S, Horovitz O, Porath A MycoplasmaMycoplasma pneumoniae community-acquired pneumonia: a review of 101 hospitalizedd adult patients. Respiration 1996; 63:261-266. 433 Chan ED, Welsh CH. Fulminant Mycoplasma pneumoniae pneumonia [clinical conference]] [see comments]. West J Med 1995; 162:133-142. 444 Koletsky RJ, Weinstein AJ. Fulminant Mycoplasma pneumoniae infection. Report of a fata!! case, and a review of the literature. Am Rev Respir Dis 1980; 122:491-496. 455 Foy HM, Nolan CM, Allan ID. Epidemiologic aspects of M. pneumoniae disease complications:: a review. Yale J Biol Med 1983; 56:469-473. 466 Cherry JD, Hurwitz ES, Wellivcr RC. Mycoplasma pneumoniae infections and exanthems.. J Pediatr 1975; 87:369-373. 477 Foy HM, Kenny GE, McMahan R, Mansy AM, Grayston JT. Mycoplasma pneumoniae pneumoniaa in an urban area. Five years of surveillance. JAMA 1970; 214:1666-1672. 488 Abramovitz P, Schvartzman P, Harel D, Lis I, Naot Y. Direct invasion of the central nervouss system by Mycoplasma pneumoniae: a report of two cases. J Infect Dis 1987; 155:482-487. . 499 Kasahara I, Otsubo Y, Yanase T, Oshima H, Ichimaru H, Nakamura M. Isolation and characterizationn of Mycoplasma pneumoniae from cerebrospinal fluid of a patient with pneumoniaa and meningoencephalitis. J Infect Dis 1985; 152:823-825. 500 Taylor RD, Gumpel JM, Hill A, Swannell AJ. Isolation of Mycoplasma pneumoniae fromm the synovial fluid of a hypogammaglobulinaermc patient in a survey of patients withh inflammatory polyarthritis. Ann Rheum Dis 1978; 37:180-182. 511 Johnston CL, Webster AD, Taylor RD, Rapaport G, Hughes GR. Primary late-onset hypogammaglobulinaemiaa associated with inflammatory polyarthritis and septic arthritiss due to Mycoplasma pneumoniae. Ann Rheum Dis 1983; 42:108-110. 522 Davis CP, Cochran S, Lisse J, Buck G, DiNuzzo AR, Weber T et al. Isolation of MycoplasmaMycoplasma pneumoniae from synovial fluid samples in a patient with pneumonia and polyarthritis.. Arch Intern Med 1988; 148:969-970. 533 Nanta M, Matsuzono Y, Itakura O, Togashi T, and Kikuta H. Survey of mycoplasmal bacteremiaa detected in children by polymerase chain reaction. Clin Infect Dis 1996; 23:522-5. . 544 Nanta M, Itakura O, Matsuzono Y, Togashi T. Analysis of mycoplasmal central nervouss system involvement by polymerase chain reaction. Pediatr Infect Dis J 1995; 14:236-237. . 555 Razin S, Jacobs E. Mycoplasma adhesion. J Gen Microbiol 1992; 138:407-422. 566 Hahn TW, Willby MJ, Krause DC. HMW1 is required for cytadhesin PI trafficking to thee attachment organelle in Mycoplasma pneumoniae. J Bacteriol 1998; 180:12701276. .
27 7
ChapterChapter 1
577 Romero-Arroyo CE, Jordan J, Peacock SJ, Willby MI, Farmer MA, Krause DC. MycoplasmaMycoplasma pneumoniae protein P30 is required for cytadherence and associated with properr cell development. J Bactenol 1999; 181:1079-1087. 588 Franzoso G, Hu PC, Mcloni GA, Barilc MF. The immunodominant 90-kilodalton proteinn is localized on the terminal tip structure of Mycoplasma pneumoniae. Infect Immunn 1993;61:1523-1530. 599 Krause DC. Mycoplasma pneumoniae cytadherence: unravelling the tie that binds. Mol Microbioll 1996; 20:247-253. 600 Jensen LT, Ladefoged S, Birkelund S, Christiansen G. Selection of Mycoplasma hominiss PG21 deletion mutants by cultivation in the presence of monoclonal antibody 552.. Infect Immun 1995; 63:3336-3347. 611 Peterson SN, Bailey CC, Jensen JS, Borre MB, King ES, Bott KF et al. Characterizationn of repetitive DNA in the Mycoplasma genitalium genome: possible rolee in the generation of antigenic variation. Proc Natl Acad Sci U S A 1995; 92:11829-11833. . 622 Layh SG, Himmelreich R, Leibfried U. The adhesin related 30-kDa protein of MycoplasmaMycoplasma pneumoniae exhibits size and antigen variability. FEMS Microbiol Lett 1997;; 152:101-108. 633 Su CJ, Dallo SF, Baseman JB. Molecular distinctions among clinical isolates of MycoplasmaMycoplasma pneumoniae. J Clin Microbiol 1990; 28:1538-1540. 644 Jacobs E, Vonski M, Oberle K, Opitz O, Pietsch K. Arc outbreaks and sporadic respiratoryy infections by Mycoplasma pneumoniae due to two distinct subtypes? Eur J Clinn Microbiol Infect Dis 1996; 15:38-44. 655 Taylor RD, Webster AD, Furr PM, Asherson GL. Prolonged persistence of MycoplasmaMycoplasma pneumoniae in a patient with hypogammaglobulinaemia. J Infect 1980; 2:171-175. . 666 Roifman CM, Rao CP, Lederman HM, Lavi S, Quinn P, Gelfand EW. Increased susceptibilityy to Mycoplasma infection in patients with hypogammaglobulinaemia. Amm J Med 1986; 80:590-594. 677 Mohiuddin AA, Corren J, Harbeck RJ, Teague JL, Volz M, Gelfand EW. Ureaplasma urealyticumm chronic osteomyelitis in a patient with hypogammaglobulinaemia. J Allergyy Clin Immunol 1991; 87:104-107. 688 Mokhbat JE, Peterson PK, Sabath LD, Robertson JA. Peritonitis due to Mycoplasma hominiss in a renal transplant recipient. J Infect Dis 1982; 146:713. 699 van Westrhenen R, Weening JJ, Krediet RT. Pneumonia and glomerulonephritis causedd by Mycoplasma pneumoniae. Nephrol Dial Transplant 1998; 13:3208-3211. 700 Foy HM, Kenny GE, Sefi R, Ochs HD, Allan ID. Second attacks of pneumonia due to MycoplasmaMycoplasma pneumoniae. J Infect Dis 1977; 135:673-677. 711 Pietsch K, Ehlers S, Jacobs E. Cytokine gene expression in the lungs of BALB/c mice duringg primary and secondary intranasal infection with Mycoplasma pneumoniae. Microbiologyy 1994; 140:2043-2048. 722 Opitz O, Pietsch K, Ehlers S, Jacobs E. Cytokine gene expression in immune mice reinfectedd with Mycoplasma pneumoniae: the role of T cell subsets in aggravating the inflammatoryy response. Immunobiology 1996; 196:575-587. 733 Fernald GW, Collier AM, Clyde WA J. Respiratory infections due to Mycoplasma pneumoniaepneumoniae in infants and children. Pediatrics 1975; 55:327-335. 744 Jacobs E. Mycoplasma pneumoniae provokes adverse events in the host. IOM letters: 122 th IOM Congress, Sydney, 181; 1998.
28 8
Introduction Introduction
755 Dorigo-Zetsmu JW, Zaat SA, Wertheim-van-Dillen PM, Spanjaard L, Rijntjes J, van Waverenn G et al. Comparison of PCR, culture, and serological tests for diagnosis of MycoplasmaMycoplasma pneumoniae respiratory tract infection in children. J Clin Microbiol 1999;37:14-17. . 766 Furness G, Pipes FJ, McMurtrey MJ. Analysis of the life cycle of Mycoplasma pneumoniaepneumoniae by synchronized division and by ultraviolet and x irradiations. J Infect Dis 1968;; 118:7-13. 777 Lind K, Lindhardt BO, Schutten HJ, Blom J, Christiansen C. Serological crossreactionss between Mycoplasma genitalium and Mycoplasma pneumoniae. J Clin Microbioll 1984;20:1036-1043. 788 Kleemola SR, Karjalainen JE, Raty RK. Rapid diagnosis of Mycoplasma pneumoniae infection:: clinical evaluation of a commercial probe test. J Infect Dis 1990; 162:70-75. 799 Kok TW, Varkanis G, Marmion BP, Martin J, Esterman A. Laboratory diagnosis of MycoplasmaMycoplasma pneumoniae infection. 1. Direct detection of antigen in respiratory exudatess by enzyme immunoassay. Epidemiol Infect 1988; 101:669-684. 800 Cadieux N, Lebel P, Brousseau R. Use of a triplex polymerase chain reaction for the detectionn and differentiation of Mycoplasma pneumoniae and Mycoplasma genitalium inn the presence of human DNA. J Gen Microbiol 1993; 139:2431-2437. 811 Williamson J, Marmion BP, Worswick DA, Kok TW, Tannock G, Herd R et al. Laboratoryy diagnosis of Mycoplasma pneumoniae infection. 4. Antigen capture and PCR-genee amplification for detection of the Mycoplasma: problems of clinical correlation.. Epidemiol Infect 1992; 109:519-537. 822 Jensen JS, Sondergard AJ, Uldum SA, Lind K. Detection of Mycoplasma pneumoniae inn simulated clinical samples by polymerase chain reaction. Brief report. APMIS 1989; 97:1046-1048. . 833 Buck GE, OHara LC, Summersgill JT. Rapid, sensitive detection of Mycoplasma pneumoniaepneumoniae in simulated clinical specimens by DNA amplification. J Clin Microbiol 1992;; 30:3280-3283. 844 de Barbeyrac B, Bemet PC, Febrer F, Renaudin H, Dupon M, Bebear C. Detection of MycoplasmaMycoplasma pneumoniae and Mycoplasma genitalium in clinical samples by polymerasee chain reaction. Clin Infect Dis 1993; 17 Suppl LS83-S89. 855 leven M, Ursi D, Van Bever H, Quint W, Niesters HG, Goossens H. Detection of MycoplasmaMycoplasma pneumoniae by two polymerase chain reactions and role of M. pneumoniaee in acute respiratory tract infections in pediatric patients [see comments]. J Infectt Dis 1996; 173:1445-1452. 866 van Kuppeveld FJ, Johansson KE, Galama JM, Kissing J, Bolske G, Hjelm E et al. 16SS rRNA based polymerase chain reaction compared with culture and serological methodss for diagnosis of Mycoplasma pneumoniae infection. Eur J Clin Microbiol Infectt Dis 1994; 13:401-405. 877 Tjhie JH, van Kuppeveld FJ, Roosendaal R, Melchers WJ, Gordijn R, MacLaren DM ett al. Direct PCR enables detection of Mycoplasma pneumoniae in patients with respiratoryy tract infections. J Clin Microbiol 1994; 32:11-16. 888 Abele HM, Busch U, Nitschko H, Jacobs E, Bax R, Pfaff F et al. Molecular approachess to diagnosis of pulmonary diseases due to Mycoplasma pneumoniae. J Clin Microbioll 1998;36:548-551. 899 Luneberg E, Jensen JS, Frosch M. Detection of Mycoplasma pneumoniae by polymerasee chain reaction and nonradioactive hybridization in microtiter plates. J Clin Microbioll 1993;31:1088-1094.
29 9
ChapterChapter 1
900 Dorigo-Zetsma JW, Zaat SA, Vriesema AJ, Dankcrt J. Demonstration by a nested PCRR for Mycoplasma pneumoniae that M. pneumoniae load in the throat is higher in patientss hospitalised for M. pneumoniae infection than in non-hospitalised subjects. J Medd Microbiol 1999;48:1115-1122. 911 Kessler HH, Dodge DE, Pierer K, Young KK, Liao Y, Santner BI et al. Rapid detectionn of Mycoplasma pneumoniae by an assay based on PCR and probe hybridizationn in a nonradioactive microwell plate format. J Clin Microbiol 1997; 35:1592-1594. . 922 Skakni L, Sardet A, Just J, Landman PJ, Costil J, Moniot VN et al. Detection of MycoplasmaMycoplasma pneumoniae in clinical samples from pediatric patients by polymerase chainn reaction. J Clin Microbiol 1992; 30:2638-2643. 933 Barker CE, Sillis M, Wreghitt TG. Evaluation of Serodia Myco II particle agglutinationn test for detecting Mycoplasma pneumoniae antibody: comparison with mu-capturee ELISA and indirect immunofluorescence. J Clin Pathol 1990; 43:163-165, 944 Kenny GE, Newton RM. Close serological relationship between glycolipids of MycoplasmaMycoplasma pneumoniae and glycolipids of spinach. Ann NY Acad Sci 1973; 225:54. 955 Biberfeld G. Mycoplasma pneumoniae infections and antibodies to brain. Lancet 1969; 2:1202. . 966 Jacobs E, Buchholz A, Klemmann B, Bredt W. Use of adherence protein of MycoplasmaMycoplasma pneumoniae as antigen for enzyme-linked immunosorbent assay (ELISA).. Isr J Med Sci 1987; 23:709-712. 977 Duffy MF, Whithear KG, Noormohammadi AH, Markham PF, Catton M, Leydon J et al.. Indirect enzyme-linked immunosorbent assay for detection of immunoglobulin G reactivee with a recombinant protein expressed from the gene encoding the 116kilodaltonn protein of Mycoplasma pneumoniae. J Clin Microbiol 1999; 37:1024-1029. 988 Jacobs E, Fuchte K, Bredt W. A 168-kilodalton protein of Mycoplasma pneumoniae usedd as antigen in a dot enzyme-linked immunosorbent assay. Eur J Clin Microbiol 1986;; 5:435-440. 999 Kingston JR, Chanock RM, Mufson MA, Hellman LP, James WD, Fox HH. Eaton agentt pneumonia. JAMA 1961; 176:118-123. 1000 Shames JM, George RB, Holliday WB, Rash JR, Mogabgab WJ. Comparison of antibioticss in the treatment of Mycoplasmal pneumonia. Arch Intern Med 1970; 125:680-684. . 1011 Taylor RD, Bebear C. Antibiotic susceptibilities of mycoplasmas and treatment of mycoplasmall infections. J Antimicrob Chemother 1997; 40:622-630. 1022 Hutin YJ, Pool V, Cramer EH, Nainan OV, Weth J, Williams IT et a!. A multistats foodbornee outbreak of hepatitis A. National Hepatitis A Investigation Team [see comments].. N Engl J Med 1999; 340:595-602. 1033 Kaplan JE, Feldman R, Campbell DS, Lookabaugh C, Gary GW. The frequency of a Norwalk-likee pattern of illness in outbreaks of acute gastroenteritis. Am J Public Healthh 1982;72:1329-1332. 1044 Anonymous. Outbreak of West Nile-like viral encephalitis-New York, 1999. MMWR Morbb Mortal Wkly Rep 1999; 48:845-849. 1055 Archibald CP, Chan RK, Wong ML, Goh A, Goh CL. Evaluation of a safe-sex interventionn programme among sex workers in Singapore. Int J STD AIDS 1994; 5:268-272. . 1066 Hoepelman IM. Legionella-epidemie in Nederland. Ned Tijdschr Geneeskd 1999; 143(23):: 1192-1196.
30 0
Introduction Introduction
1077 Schlossberg D, Delgado J, Moore MM, Wishner A, Mohn J. An epidemic of avian and humann psittacosis. Arch Intern Med 1993; 153:2594-2596. 1088 Smith CB, Friedewald WT, Chanock RM. Inactivated Mycoplasma pneumoniae vaccine.. Evaluation in volunteers. JAMA 1967; 199:353-358. 1099 Mogabgab WJ. Protective efficacy of killed Mycoplasma pneumoniae vaccine measuredd in large-scale studies in a military population. Am Rev Respir Dis 1973; 108:899-908. . 1100 Jacobs E, Drews M, Stuhlert A, Buttner C, Klein PJ, Kist M et al. Immunological reactionn of guinea-pigs following intranasal Mycoplasma pneumoniae infection and immunizationn with the 168 kDa adherence protein. J Gen Microbiol 1988; 134:473479. . 1111 Barry MA, Lai WC, Johnston SA. Protection against mycoplasma infection using expression-libraryy immunization. Nature 1995; 377:632-635. 1122 Klausner JD, Passaro D, Rosenberg J, Thacker WL, Talkington DF, Werner SB et al. Enhancedd control of an outbreak of Mycoplasma pneumoniae pneumonia with azithromycinn prophylaxis. J Infect Dis 1998; 177:161-166.
31 1