Comparison of Swab and Sponge Methodologies for Identification of Acinetobacter baumannii from the Hospital Environment Kerri A. Thom,a Tracy Howard,b Sophie Sembajwe,a Anthony D. Harris,a Paula Strassle,a Brian S. Caffo,c Karen C. Carroll,b and J. Kristie Johnsond Department of Epidemiology and Public Health, University of Maryland School of Medicine,a Johns Hopkins University,b Department of Biostatistics, Bloomberg School of Public Health, Johns Hopkins University,c and Department of Pathology, University of Maryland School of Medicine,d Baltimore, Maryland, USA
The ideal sampling method for identification of Acinetobacter baumannii from the health care environment is unknown. In this study, we sampled 145 surfaces in the rooms of patients with known A. baumannii colonization/infection, comparing two methods: swab and sponge. The sensitivity of the swab method was 87%, while the sensitivity of the sponge method was 75%. Given the comparable results, use of the cheaper and less laborious swab technique is acceptable and may be preferable.
A
cinetobacter baumannii is an important pathogen that can cause a variety of health care-associated infections (e.g., pneumonia and urinary tract and bloodstream infections) and is associated with morbidity and mortality (6). A. baumannii is thought to spread from patient to patient primarily through an intermediate such as the hands of health care workers or the health care environment. Identification of A. baumannii on environmental surfaces is sometimes warranted in clinical practice, primarily during investigations of outbreaks, and in research to further define modes of transmission. The ideal method for environmental sampling is unknown. This study aims to compare two different methods, swab and sponge, for the detection of A. baumannii in the health care environment. A prospective cohort of adult intensive care unit (ICU) patients known to have recently been colonized or infected with A. baumannii was identified. Patients with a clinical or surveillance culture positive for growth of A. baumannii in the 72 h preceding data collection were included. Environmental samples were collected during a 2-month period from June to August 2011 at the University of Maryland Medical Center; a 757-bed tertiary care hospital in Baltimore, MD. Patient rooms were cleaned according to hospital policies, which include a 12-step process for daily cleaning and disinfection using a quaternary amine-based product; thoroughness of cleaning was not measured during this study. The study was approved by the University of Maryland’s Institutional Review Board. Environmental samples were obtained from surfaces in patient rooms while occupied. Ten surfaces in each room were sampled: sink, bedrails, bedside table, vital sign monitor touchpad, nurse call button, drawer handles of in-room supply cart, door handle, infusion pump, ventilator adjustment knobs and buttons, and the floor on both sides of the bed. For each room, each surface was sampled first using the swab and then the sponge method. Since each surface was sampled twice, once for each method, the swab sampling (which covers a much smaller surface area) was performed first to reduce interference or dilution of results for the second sampling method. For the swab method, each site was sampled using a sterile cotton swab premoistened with phosphate-buffered saline (PBS) (BactiSwabs; Remel); the swab was rolled back and forth over each surface three times to ensure that all sides of the swab made contact with the surface and that a maximal surface area was covered. After swab sampling, each site was sampled using a sterile sponge (Oxoid Cellulose Sponge;
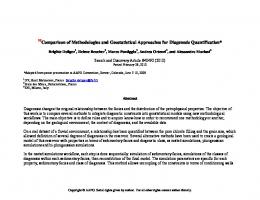
Fisher Scientific) and methods outlined by the Centers for Disease Control (http://www.cdc.gov/niosh/topics/emres/surface-sampling -bacillus-anthracis.html). In brief, the sponge was applied to the area using overlapping “S” strokes to ensure sampling of the entire surface; the sponge was then rotated, and the procedure was repeated four times to coat all sides of the sponge for each surface. After collection, each swab was immersed in 5 ml of brain heart infusion (BHI) broth; mixing was achieved via vortex for 10 s. Sponges were placed in a Stomacher bag with 40 ml of PBS with Tween 20 (PBST) and homogenized for 1 min at 260 rpm using a Stomacher 80 Biomaster (Seward Laboratories). The fluid was then divided equally into two 50-ml conical tubes by the use of a pipette and concentrated by centrifugation at 3,500 ⫻ g for 15 min. Most of the supernatant was removed; pellets were resuspended and then recombined, and a 1-ml aliquot was then inoculated into a 5-ml BHI tube. For each, the broth was incubated overnight at 37°C and then subcultured to a RabaCHROM Acinetobacter plate (Gibson Laboratories) (1). Red colonies (i.e., presumptive for Acinetobacter) were then identified as A. baumannii by the use of API (bioMérieux), Vitek (bioMérieux), or the Phoenix system (Becton, Dickinson). A total of 145 environmental surfaces in the rooms of 15 ICU patients known to have recently been colonized or infected with A. baumannii were sampled using both swab and sponge methodologies (4 patient rooms were missing the ventilator and one the bedside table). A. baumannii was identified using the swab method in 37% of samples (53/145) and using the sponge method in 32% (46/145). If one considers identification of A. baumannii by either methodology the gold standard (i.e., both tests are highly specific, with very few false-positive results), then A. baumannii was identified in 61 samples (by swab only in 15 samples, by sponge only in 8 samples, and by both in 38 samples) (Figure 1). The swab method correctly identified A. baumannii in 53 of the
2140
p. 2140 –2141
jcm.asm.org
Journal of Clinical Microbiology
Received 16 February 2012 Returned for modification 12 March 2012 Accepted 16 March 2012 Published ahead of print 29 March 2012 Address correspondence to Kerri A. Thom,
[email protected]. Copyright © 2012, American Society for Microbiology. All Rights Reserved. doi:10.1128/JCM.00448-12
June 2012 Volume 50 Number 6
Environmental Acinetobacter Sponge versus Swab
methods for environmental sampling for Bacillus anthracis (3, 4, 5, 7). However, no studies comparing the two methods for the identification of A. baumannii (or any hospital-acquired Gram-negative bacteria) in the environment have been performed to date. The findings of the present study suggest that the results of identification of A. baumannii on environmental surfaces are comparable whether using the swab or sponge methodology and support the use of the cheaper and less laborious swab method. ACKNOWLEDGMENTS FIG 1 Comparisons of sensitivities of swab (upper panel) and sponge (lower panel) methods to the gold standard, where “Any Positive” indicates positivity for growth of A. baumannii by either the swab or the sponge method. Sensitivity of swab method, 87% (53/61); sensitivity of sponge method, 75% (46/ 61).
61 samples for a sensitivity of 87%. In contrast, the sponge method correctly identified A. baumannii in 46 of 61 samples for a sensitivity of 75%. Given the assumption that the two tests are equally specific as mentioned above, the result of a smallsample McNemar’s test for equivalency of the sensitivities was the same as if the gold standard were known. There was no statistical difference between the sensitivities of the two methods (P ⫽ 0.21). Identification of A. baumannii on environmental surfaces is relevant in both clinical and research settings: a hospital investigating an A. baumannii outbreak may undertake environmental culturing to identify a potentially modifiable source of transmission, while a researcher may perform assays using environmental cultures to study the role of the environment in the transmission of A. baumannii. Available guidelines provide the option of using the swab or sponge method for environmental sampling in such cases (2, 8). The swab method may be more attractive to many, as it is less costly, does not require the use of expensive and specialized microbiological equipment (e.g., a Stomacher), and is easier to implement with respect to both sampling and microbiological evaluation. Despite these advantages, the sponge method covers a greater surface area and may have theoretical benefits compared to the swab method in recovery of organisms. The latter possibility is supported by existing studies comparing the swab and sponge
June 2012 Volume 50 Number 6
We thank Gwen Robinson for her assistance in the development of protocols for the microbiological evaluation of Acinetobacter baumannii. We also thank Elise Gluck for her help with the microbiological evaluation of the sponge samples. This work was supported by National Institutes of Health (NIH) Career Development grants 1K23AI082450-01A1 (K.A.T.) and 1K24AI07904001A1 (A.D.H.). A.D.H. is also supported by NIH grant 2R01AI06085905A1. B.S.C. is supported by National Institute of Biomedical Imaging and Bioengineering grant R01EB012547. J.K.J. is supported by NIH grant IK12RR023250-04.
REFERENCES 1. Ajao AO, et al. 2011. Comparison of culture media for detection of Acinetobacter baumannii in surveillance cultures of critically-ill patients. Eur. J. Clin. Microbiol. Infect. Dis. 30:1425–1430. 2. Bond WW, Sehulster L. 2010. Microbiological assay of environmental and medical-device surfaces, p 13.10.1 to 13.10.12. In Isenberg HD (ed), Clinical microbiology procedures handbook, vol 3. American Society for Microbiology, Washington, DC. 3. Brown GS, et al. 2007. Evaluation of a wipe surface sample method for collection of Bacillus spores from nonporous surfaces. Appl. Environ. Microbiol. 73:706 –710. 4. Brown GS, et al. 2007. Evaluation of rayon swab surface sample collection method for Bacillus spores from nonporous surfaces. J. Appl. Microbiol. 103:1074 –1080. 5. Estill CF, et al. 2009. Recovery efficiency and limit of detection of aerosolized Bacillus anthracis Sterne from environmental surface samples. Appl. Environ. Microbiol. 75:4297– 4306. 6. Peleg AY, et al. 2008. Acinetobacter baumannii: emergence of a successful pathogen. Clin. Microbiol. Rev. 21:538 –582. 7. Sanderson WT, et al. 2002. Surface sampling methods for Bacillus anthracis spore contamination. Emerg. Infect. Dis. 8:1145–1151. 8. Sehulster L, Chinn RY. 2003. Guidelines for environmental infection control in health-care facilities. Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC). MMWR Recomm. Rep. 52(RR-10):1– 42.
jcm.asm.org 2141