Faculty of Medicine, Melaka Manipal Medical College, Malaysia .... technical manual of NHMS III (Institute for public health, ..... ta/docs/IDF_Meta_def_final.pdf.
International Journal of Medicine and Medical Sciences, ISSN: 2051-5731, Vol.46, Issue.2
1225
Determinants of Abdominal Obesity and its Predictability of Morbidity: A Cross Sectional Study in Malaysia Nan Nitra Than Faculty of Medicine, Melaka Manipal Medical College, Malaysia
Senthil Kumar.P Faculty of Medicine, Melaka Manipal Medical College, Malaysia
Htoo Htoo Kyaw Soe Faculty of Medicine, Melaka Manipal Medical College, Malaysia
Sawri Rajan Rajagopal AIMST University, Faulty of Medicine, Malaysia
Soe Moe Faculty of Medicine, Melaka Manipal Medical College, Malaysia
Sein Win Faculty of Medicine, Melaka Manipal Medical College, Malaysia
ABSTRACT Globally, it is an accepted fact that abdominal obesity is a better predictor of cardiovascular diseases and diabetes mellitus. Waist circumferences (WC) measurement is the most commonly used method to measure abdominal obesity as it is convenient and inexpensive. The applicability of waist circumference for diagnosis of abdominal obesity as well as predictability of abdominal obesity to other morbidity should be tested in local context. Determinant of abdominal obesity should be identified to provide information for health education to the community. The aim of this study is to identify determinants of abdominal obesity among Malaysians. It also intends to check whether abdominal obesity can be a predictor of general obesity and hypertension in local context. This is a cross sectional study on the available records of medical service users whose age ranged between 18 to 82 years. Data were analysed with using SPSS 12.0 software. The proportion of abdominal obesity among service utilizers is high (81.7%). Higher proportion of abdominal obesity is seen among female compare to male. There were significantly high positive correlation between body mass index (BMI) and waist circumference (WC) in both male and female. Abdominal obesity measured by waist circumference can be a predictor of general obesity however findings fails to show that abdominal obesity can be a predictor of hypertension. Health education to local community especially women for self-assessment of abdominal obesity is recommended.
Keywords-
Abdominal obesity(AO) ,Waist circumference (WC), Body mass Index (BMI) Determinants, Life style, Smoking, Blood pressure
1. INTRODUCTION Abdominal obesity is one of the key indicators of central fat adiposity in adults. Central obesity occur when the main deposits of body fat adipose tissue are localized around the abdomen (intra-abdominal or visceral fat) and
the upper body region. The contribution of intraabdominal fat mass to total body fat is influenced by gender, age, ethnicity, level of energy balance, composition of diet , level of physical activity and a variety of social factors including smoking and alcohol intake [1]. There are several ways to determine abdominal obesity in adults. Anthropometry in terms of waist circumference and waist hip ratio (WHR) measurements, bioelectrical impedance, magnetic resonance imaging and computed tomography are the commonly used methods in assessing abdominal obesity. WHR has many shortcomings including inherent weakness as a ratio index and strong influence by pelvic structure. It is also an unsatisfactory measure of abdominal fat mass especially in non-obese individuals [2]. In terms of BMI, it is now commonly employed as such in epidemiological studies, to predict obesity-related morbidity and mortality in adults. It was not originally intended as an index of obesity but also does not distinguish between weight associated with muscle and weight associated with fat [3], [4].In a large population-based study, waist circumference measurement is the most commonly used method as it is convenient and inexpensive [5]. According to international diabetes federation, it is one of the criteria for diagnosis of metabolic syndrome in adults where individuals with metabolic syndrome are at greater risk for diabetes and cardiovascular disease [6].In addition, it is a better predictor and is independently associated with the risk of cardiovascular disease and diabetes mellitus even in individuals with normal BMI [7], [8]. In terms of measurement technique, a single measurement of WC can be used as a clinical marker to identify individuals who are overweight and abdominally obese [9]. Abdominal obesity has its cut off points being used in identification. According to world health organization criteria, 1998 on abdominal obesity, it is defined as waist circumference >102 cm in men and >88 cm in women. International diabetes federation has drawn up pragmatic ethnic specific
© RECENT SCIENCE PUBLICATIONS ARCHIVES| June 2013|$25.00 | 27702521 | *This article is authorized for use only by Recent Science Journal Authors, Subscribers and Partnering Institutions*
International Journal of Medicine and Medical Sciences, ISSN: 2051-5731, Vol.46, Issue.2
cut-offs for South Asians (Malay, Chinese and Asian Indian population) and its cut offs are >90 cm for men and >80 cm for women [10] & [11]. The determinants of abdominal obesity in adults is depend on sociodemographic factors such as gender , age, ethnicity, marital status, residence area, household income and educational level, level of physical activity , dietary intakes and lifestyle [12],[13],[14]. Cigarette smoking and obesity are leading public health concerns facing modern societies in terms of increase in the risk for cardiovascular disease , cancer and metabolic abnormalities although mechanisms by which they do so appear to differ[15],[16]. Several cross sectional studies have evaluated the association between alcohol and abdominal obesity but the results are still inconclusive [17] where some found a positive association [18] and whereas others found a negative or no association [19], [20].Prevalence of abdominal obesity was substantially higher at 39.5% overall with women at 47.3% and men at 30.1% compared to 17.4% overall, 26% in women and 7.2% in men based on WHO (1998). In United States, NHMS III, NHANES prevalence reported that 59.9% of adult females and 38.3% of adult males had abdominal obesity [21].National surveillance 2006 from disease control division, Ministry of health Malaysia reported an even higher overall prevalence of abdominal obesity at 48.6% with 57.1% of women and 40.7% of men. Free medical check-up was given to public in a medical camp which was available during Deepavali ceremony, 2011 in semi urban area, Kedah State, Malaysia to raise awareness on obesity and related diseases as well as services to check such diseases. Since the data of the person taking the service of that medical camp were available they were further analysed to see the determinants of abdominal obesity and its predictability of general obesity and hypertension.
2. MATERIALS & METHODS All completed records of those people who utilized the medical service at the camp in 2011 were undergone for further analysis. Increased abdominal girth not related to increase adiposity (eg. Pregnancy, abdominal ascites, hypothyroidism and other debilitating illness) were excluded.
2.1 Anthropometric and Blood Pressure Measurement Waist circumference measurements were obtained by trained nurses based on standard procedure listed in technical manual of NHMS III (Institute for public health, 2006). The measurement was made to the nearest 0.1 cm at the natural waist midpoint between the bottom of the rib cage and above the top of the iliac crest based on WHO recommendation. The respondents were classified as abdominal obesity if WC measured more than 90 cm for men and 80 cm for women based on the cut off points recommended by the International Diabetes Federation 2006 .Generalized obesity was measured by body mass index (BMI) as a basic anthropometry measurement to all respondents along with waist circumference measurement.
1226
BMI was computed as the ratio of weight to the square of height (kg/m2). It was classified as under-weight, normal, over-weight and obese according to recommendation for Malaysians by WHO (1998) and WHO Expert Consultation, 2004. Underweight was < 18.5, Normal 18.5 to 24.9, over weight 25 to 29.9 and obese >30. Blood pressure was measured with mercury sphygmomanometer to find out association between health risk and abdominal obesity. Hypertension was defined at base line as systolic blood pressure (SBP) ≥140 mmHg; diastolic blood pressure (DBP) ≥ 90mmHg.Onsite random capillary blood glucose level was taken by glucometer as a screening test for diabetes to all the service utilizers. Normal capillary blood sugar level is 5.6mmol/l. [22]
2.2 Study design & Study population A cross sectional study was done by reviewing available medical records of service users at Medical camp, provided in semi-urban population, Malaysia. Data were collected with the help of records review checklists which included demographic data, blood pressure measurement, measurement of WC.
3. RESULTS A total of 82 respondents were included in this study. Age of the respondents ranged from 18 to 82 years and 31.7% of the respondents were aged 51-60 years while 25.6% were 61-70 years, 20.7% were 41-50 years, 13.4% were older than 70 years and only 8.5% were younger than 40 years. Regarding gender distribution, 65.9% were female population while 40.2% were male. 45.1% of the respondents were Indian, 45.1% were Malay while 18.3% were Chinese. In relation to occupation, 31.7% were manual worker, 37.8% were housewife, 18.3% were retired from work, 9.8% were professional and 2.4% were students. Regarding life style, most of the respondents were non-smokers (86.6%), never consuming alcohol (84.1%) and were never doing regular exercise (72%) (Table1). According to International Diabetes Federation cut off points for Asians, the prevalence of abdominal obesity was 81.7%. (Figure 1)
3.1 Determinants of abdominal obesity Table 2 shows the relationship between sociodemographic characteristics, life style and abdominal obesity.
No Abdominal Obesity
Abdominal Obesity 0
20
40
60
80 100
Figure 1: Abdominal obesity in percentage among respondents (n = 82)
© RECENT SCIENCE PUBLICATIONS ARCHIVES| June 2013|$25.00 | 27702521 | *This article is authorized for use only by Recent Science Journal Authors, Subscribers and Partnering Institutions*
International Journal of Medicine and Medical Sciences, ISSN: 2051-5731, Vol.46, Issue.2
Hypertension was defined at baseline as systolic blood pressure (SBP) ≥140 mmHg and diastolic blood pressure (DBP) ≥ 90mmHg. Most of the respondents had normal SBP and DBP despite presence of abdominal obesity. Among respondents with abdominal obesity, 92.5% had normal SBP and DBP while only 7.5% had hypertension. (Table1). According to International Diabetes Federation cut off points for Asians, the prevalence of abdominal obesity was 81.7%. (Figure 1) Table 1: Socio-demographic characteristics (n = 82) Variables Age ≤ 40 41 – 50 51 – 60 61 – 70 > 70 Sex Male Female Ethnicity Malay Chinese Indian Occupation Manual worker Professional Retired Housewife Student Life style Smoking Yes No Alcohol Yes No Exercise Yes No
Frequency (%) 7 (8.5) 17 (20.7) 26 (31.7) 21 (25.6) 11 (13.4) 33 (40.2) 49 (59.8) 37 (45.1) 15 (18.3) 30 (45.1) 26 (31.7) 8 (9.8) 15 (18.3) 31 (37.8) 2 (2.4)
11 (13.4) 71 (86.6) 13 (15.9) 69 (84.1) 23 (28.0) 59 (72.0)
There were no significant association between age, ethnicity and abdominal obesity. However, there was significant positive association between sex and
1227
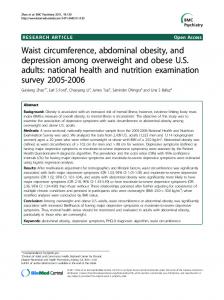
abdominal obesity as female are 5.46 times significantly more likely to have abdominal obesity (95%CI=1.0414.19). Regarding life style, there were no significant relationship between smoking, alcohol drinking, regular exercise and abdominal obesity. (Table 2) Figure 2 and 3 reveals the correlation between BMI and waist circumference in different gender which was significant high positive correlation.
3.2 Blood pressure and abdominal obesity Moreover, there were no significant difference of SBP, DBP and capillary plasma glucose between the respondents who had abdominal obesity and who did not. (Data not shown)
4. DISCUSSION This study intends to figure out the determinants and predictability among abdominal obesity. Reachable medical check-up alarm them to aware of related health risk. In this study, there is a higher prevalence of abdominal obesity among women than in men. Our study follows the same with the other studies where there is consistently higher prevalence among women [23] and similar differences have also been observed in relatively small scale studies carried out in the United States [24], also in Iran [25] Sri Lanka and Turkey [26] respectively. With compared to national wide study figure which is 48%, our prevalence rate of 81.7% may be high because in nationwide study , the sample population is drawn from huge population 70-80,000 and the age group is mostly between 25 to 64 years and cut off point for WC is by using WHO criteria. Our study is only among service utilizers however, it may or may not reflect the actual high prevalence in semi urban population. Differences in body fat distribution between men and women may explain why women are at higher risk of abdominal obesity than men [27].The prevalence was higher among the Indians and Malays compared to Chinese population.This study found the same as NHMS III study [28] & [29].Waist circumference is high in majority of female respondents especially in housewives in this study. The remarkably high prevalence of abdominal obesity among housewives is possibly due to their increased susceptibility to sedentary lifestyles, more accessibility to food and being disadvantaged to get health information.
© RECENT SCIENCE PUBLICATIONS ARCHIVES| June 2013|$25.00 | 27702521 | *This article is authorized for use only by Recent Science Journal Authors, Subscribers and Partnering Institutions*
International Journal of Medicine and Medical Sciences, ISSN: 2051-5731, Vol.46, Issue.2
GENDER:
1228
2 Male
30 28 26 24 22
Body Mass Index
20 18 16 14 70
80
90
100
110
120
Waist circumference
Figure 3: Correlation between BMI and WC in male (n=28) Table 2: Relationship between socio-demographic characteristics, life style and abdominal obesity (n = 82) Variables
Age ≤ 40 41 – 50 51 – 60 > 60 Sex Male Female Ethnicity Chinese Indian Malay Life style Smoking No Yes Alcohol No Yes Regular Exercise No Yes * Significant
AO
OR (95% CI)
P value
1 (14.3) 4 (23.5) 2 (7.7) 8 (25.0)
1 (Reference) 0.54 (0.02-7.78) 2 (0.0-38.04) 0.5 (0.02-5.61)
1.00 0.52 1.00
19 (67.9) 48 (88.9)
9 (32.1) 6 (11.1)
1 (Reference) 3.79 (1.04-14.19)
0.01*
12 (80.0) 24 (80.0) 31 (83.8)
3 (20.0) 6 (20.0) 6 (16.2)
1 (Reference) 1 (0.16-5.79) 1.29 (0.21-7.35)
1.00 0.70
60 (84.5) 7 (63.6)
11 (15.5) 4 (36.4)
1 (Reference) 0.32 (0.07-1.58)
0.11
59 (85.5) 8 (61.5)
10 (14.5) 5 (38.5)
1 (Reference) 0.27 (0.06-1.2)
0.06
48 (81.4) 19 (82.6)
11 (18.6) 4 (17.4)
1 (Reference) 1.09 (0.27-4.67)
1.00
Present N (%)
Absent N (%)
6 (85.7) 13 (76.5) 24 (92.3) 24 (75.0)
Consistent with other studies where abdominal obesity was found to be higher among married or ever married individuals than among those who have never married [30], [31]. Previous study show negatively correlation of obesity with smoking. They concluded that current smokers had less WC & BMI and it also suggested that the aging process increases visceral adiposity [32] [33]. Most of the respondents have no habit of doing regular exercise and it was not significantly associated with abdominal obesity. Regarding life style practices, smoking was not significantly associated as a determinant
factor for abdominal obesity. Our study compatible in relation to smoking habits in women of previous study where women has lower smoking rate which limits the ability to detect modest to moderate associations between smoking and obesity[34].Moreover, alcohol consumption was not significantly associated with abdominal obesity. That finding altered with previous study where alcohol consumption increases abdominal obesity [35]. Our study assert likewise as Okura T et al where Physical activity decreases visceral adiposity [36]. Limitation of our study is we did not divide the group and amount and types of
© RECENT SCIENCE PUBLICATIONS ARCHIVES| June 2013|$25.00 | 27702521 | *This article is authorized for use only by Recent Science Journal Authors, Subscribers and Partnering Institutions*
International Journal of Medicine and Medical Sciences, ISSN: 2051-5731, Vol.46, Issue.2
alcohol and there were no available data on past alcohol history and prior or present patterns of alcohol consumption which are potential cofounders we could not adjust. Also we relied on self-reported measures of smoking habits and we did not measure the potential amount of passive smoke exposure in those who never smoked. In addition, the study subjects were not a representative sample and also didn’t classify the smoking habit and types of smoking. However, our results define a call for the people to be aware of abdominal obesity and how important the WC measurement in a medical setting. GENDER:
1
Female
[4]
James WPT, Chunming C, Inoue S. Appropriate Asian body mass indices, Obesity Reviews 2002;3(3):139.
[5]
Han TS, Sattar N & Lean M .Assessment of obesity and its clinical implication. British Medical Journal 2006; 333: 695-8.
[6]
International Diabetes Federation. The IDF consensuses worldwide definition of the metabolicsyndrome,2006http://www.idf.org/webda ta/docs/IDF_Meta_def_final.pdf.
[7]
Balkau B, Vernay M, Mhamdi L, Novak M, Arondel D, Vol S, Tichet J, Eschwège E; D.E.S.I.R. Study Group .The incidence and persistence of the NCEP (National Cholesterol Education Program) metabolic syndrome. The French D.E.S.I.R. study Diabetes Metab 2003; 29:526–32.
[8]
Wittchen H U,Balkau B,Massien C,Richard A,Haffner S & Despres JP .International Day for the Evaluation of abdominal obesity: rationale and design of a primary care study on the prevalence of abdominal obesity and associated factors in 63 countries. European Heart Journal supplements 2006;8:B26-33
[9]
Lean MEJ, Han TS & CE Morrison Waist circumference as a measure for indicating need for weight Management, BMJ 1995;311:158-61.
[10]
WHO/IOTF/IASO.(2000) The Asia-Pacific perspective: Redefining Obesity and its treatment. Hong Kong: World Health Organization, International Obesity Task Force, International Association for the Study of Obesity.
[11]
The IDF consensus worldwide definition of the metabolic syndrome, International Diabetes Federation, The IDF consensus worldwide definition of the metabolic syndrome 2006 , www.idf.org.
[12]
Arambepola C,Ekanayake R&Fernando D) Gender differentials of abdominal obesity among adults in the district of Colombo,Sri Lanka ,Journal of Preventive Medicine2007; 44:129-134.
[13]
Janghorbani M, Amini M, Willett WC, Gouya MM, Delavari A, Alikhani S & Mahdavi A. First nationwide survey of prevalence of overweight, underweight and abdominal obesity in Iranian Adults Obesity 2007;15: 2797-2808 .
[14]
Erem C, et al. Prevalence of metabolic syndrome and associated risk factors among Turkish adults: Trabzon MetS study. Endocrine 2008; 33: 9-20.
50
40
30
Body Mass Index
20
10
0 60
70
80
90
100
110
120
130
140
Waist circumference
Figure 2: Correlation between BMI and WC in female (n=54)
5. CONCLUSIONS This study showed that there is high prevalence of abdominal obesity among medical service utilizers at a medical camp in semiurban population of Malaysia. Women are more likely to have abdominal obesity. It also gave evidence that waist circumference is a method to measure abdominal obesity which is a good predictor of general obesity but it fails to proof that it can be a predictor of hypertension. Being a small scale study of medical service users, it failed to identify the other determinants of abdominal obesity. Health education to community especially women, for self-assessment of abdominal obesity by measuring their WC is recommended.
REFERENCES [1]
Bouchard C, Bray GA & Hubbard VS Basic and clinical aspects of regional fat distribution, American Journal of Clinical Nutrition, 1990;52: 946-950.
[2]
Goodman- Gruen D, Barrett-Connor E. Sex differences in measures of body fat and body distribution in the elderly, Am J Epidemiol 1996;9: 898-906.
[3]
WHO/IOTF/IASO The Asia-Pacific perspective: Redefining Obesity and its treatment. Hong Kong: World Health Organization, International Obesity Task Force, International Association for the Study of Obesity, 2000.
1229
[15] WHO/IOTF/IASO The Asia-Pacific perspective: Redefining Obesity and its treatment. Hong Kong: World Health Organization, International Obesity Task Force, International Association for the Study of Obesity,2000.
© RECENT SCIENCE PUBLICATIONS ARCHIVES| June 2013|$25.00 | 27702521 | *This article is authorized for use only by Recent Science Journal Authors, Subscribers and Partnering Institutions*
International Journal of Medicine and Medical Sciences, ISSN: 2051-5731, Vol.46, Issue.2
[16]
Oh SW,Yoon YS,Lee ES,Kim WK,Park G,et al, Association between cigarette smoking and metabolic syndrome; the Korea National Health and Nutrition Examination Survey. Diabetes Care PLOS 2005; 28:2064 – 66.
[17]
Vadstrup ES , Petersen L,Sorensen TI,Gronbaek M.Waist circumference in relation to history of amount and type of alcohol; results from Copenhagen City Heart Study. Int J Obes Relat Metab Di-sord 2003;27:238-246.
[18]
[19]
Laws A, Terry RB, Barrett-Connor E. Behavioral covariates of waist-to-hip ratio in Rancho Bernardo. Am J Public Health 1990;80:1358-1362. Haffner SM, Alexander CM, Cook TJ et al. Reduced coronary events in simvastatin-treated patients with coronary heart disease and diabetes mellitus or impaired fasting glucose levels: subgroup analysis on the Scandinavian Simvastatin Survival Study. Arch Intern Med 1999;159 (22):2661-7 39 19.
[20]
Keenan NL, Strogatz DS, James SA, Ammerman AS, Rice BL. Distribution and correlates of waistto-hip ratio in black adults: the Pitt County Study. Am J Epidemiol 1992;135: 678-684.
[21]
Okosun IS, Dinesh Chandra KM, Boev A,Boltri JM, Choi ST, Parish DC & Alan Dever GE Abdominal adiposity in US adults: prevalence and trends, 1960-2000. Preventive Medicine 2004; 39: 197- 206.
[22] [23]
[24]
1230
[28]
Kee CC, Jamaiyah H, Noor Safiza M, Geeta A, Khor GL, Suzana S, Jamalludin AR,Rahmah R, Ahmad AZ, Ruzita AT, Wong NF & Ahmad Faudzi Y, Abdominal Obesity in Malaysian Adults: National Health and Morbidity Survey III (NHMS III, 2006) Mal J Nutr 2008; 14(2): 125 – 135.
[29]
Tan CE, Ma S, Wai D, Chew SK & Tai ES. Can we apply the National Cholesterol Education Program Adult Treatment Panel definition of the metabolic syndrome to Asians? Diabetes Care 2004; 27: 1182-1186.
[30]
Ball K, Mishra G & Crawford D. Which aspects of socioeconomic status are related to obesity among men and women? International Journal of Obesity 2002;26: 559-565.
[31] Arambepola C, Ekanayake R &Fernando D Gender differentials of abdominal obesity among adults in the district of Colombo, Sri Lanka. Journal of Preventive Medicine 2007; 44: 129-134. [32]
Kotani K,Tokunaga K,Fujioka S, Kobatake T,Keno Y,et al. (1994) Sexual dimorphism of agerelated changes in whole body fat distribution in the obese, IntJ Obes Relat Metab Disord 1994;18:207-212.
[33]
Clinical Practice guideline, Malaysia, Management of type II diabetes mellitus, May 2009,Page 6.
Yumi M,Toru N,Shuichiro Y, Yoshihiko T, Mitsuhiko N, et al. Associations of smoking cessation with visceral fat area and prevalence of metabolic syndrome in men : The Hitachi Health Study. Obesity 2011;19:647-651 .
[34]
Bassand JP. Results from a region by-region analysis of the IDEA study highlight the differences in anthropometric characteristics between Asian and European populations. World Congress Press Releases (2006).
Kim JH ,Shim KW,Yoon YS,Lee SY,Kim SS,Oh SW ,Cigarette smoking increases abdominal and visceral obesity but not overall fatness: An observational Study, PLOS 2012;Vol 7,issue 9,e45815 www.plosone.org.
[35]
Okosun IS, Dinesh Chandra KM, Boev A,Boltri JM, Choi ST, Parish DC & Alan Dever GE (2004)Abdominal adiposity in US adults: prevalence and trends, 1960-2000. Preventive Medicine39:197- 206.
Yoon YS, Oh SW, baik HW, Park HS, Kim WY Alcohol consumption and the metabolic syndrome in Korean adults: the 1998 Korean National Health and Nutrition Examination Survey. Am J Clin Nutr; 2004;80:217-224.
[36]
Okura T, Nakata Y, Lee DJ, Ohkawara K, Tanaka K, Effects of aerobic exercise and obesity phenotype on abdominal fat reduction in response to weight loss. Int j Obes (Lond) ;2005;29: 125966.
[25]
Janghorbani M, Amini M, Willett WC, Gouya MM, Delavari A, Alikhani S & Mahdavi A First nationwide survey of prevalence of overweight, underweight and abdominal obesity in Iranian Adults. Obesity 2007,15: 2797-2808.
[26]
Erem C, et al. Prevalence of metabolic syndrome and associated risk factors among Turkish adults: Trabzon MetS study. Endocrine 2008; 33: 9-20.
[27]
Lemieux S, Prudhomme D, Bouchard C, Tremblay A & Despres JP.Sex differences in the relation of visceral adipose tissue accumulation to total body fatness. American Journal of Clinical Nutrition 1993; 58: 463-467.
© RECENT SCIENCE PUBLICATIONS ARCHIVES| June 2013|$25.00 | 27702521 | *This article is authorized for use only by Recent Science Journal Authors, Subscribers and Partnering Institutions*