The clinicopathologic characteristics of pediatric thyroid cancer according to the histologic ... The histologic types of thyroid carcinoma were papillary thyroid.
THYROID CANCER AND NODULES
THYROID Volume 19, Number 11, 2009 ª Mary Ann Liebert, Inc. DOI: 10.1089=thy.2009.0073
Diffuse Sclerosing Variant Is a Major Subtype of Papillary Thyroid Carcinoma in the Young Ja Seung Koo,1 Soonwon Hong,1 and Cheong Soo Park2
Background: Pediatric thyroid cancer differs from adult thyroid cancer in presentation and outcome. Pediatric thyroid cancer has a higher recurrence rate and greater percentage of lymph node and pulmonary metastasis. The clinicopathologic characteristics of pediatric thyroid cancer according to the histologic subtype have not been reported, however. In this study, we determined the histological subtypes of pediatric thyroid cancer and analyzed other clinicopathologic characteristics. Methods: All patients with thyroid cancer who were admitted to Severance Hospital, Seoul, South Korea, were retrospectively reviewed; their age was 95% (3–7), pediatric patients with thyroid carcinoma have more frequent recurrences (7,8) and a higher prevalence of lymph node and pulmonary metastasis (7). The prognostic factors in pediatric thyroid carcinoma have been poorly evaluated. Papillary or papillary–follicular histology (6) and age (3) have been significantly associated with time to recurrence after initial surgical treatment in the young. Although the histologic subtype
and age are important prognostic factors in pediatric thyroid carcinoma, the clinicopathologic characteristics according to histologic subtype have not been investigated. We studied a series of pediatric patients who underwent thyroid surgery for thyroid cancer at our institution. We examined the histopathological material to determine the relative frequencies of the subtypes of papillary thyroid carcinoma (PTC) and analyzed the clinical features of the subtypes. Materials and Methods Patients All patients with thyroid carcinoma who were 10 years; p ¼ 0.366), sex ( p ¼ 0.256), lymph node involvement ( p ¼ 0.204), and histologic type ( p ¼ 0.251) were not associated with time to recurrence in this study population. When univariate regression analysis of clinicopathologic factors on time to recurrence was performed in only pediatric papillary carcinoma, there was a statistical significance in
1228
KOO ET AL.
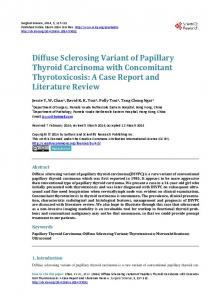
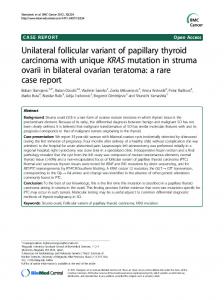
FIG. 1. DSVPC. (A) Prominent fibrosis and sclerosis in intratumoral area make tumor multinodular appearance with somewhat radiating pattern (H&E, original magnification �40). (B) Tumor emboli in lymphatic channel in peritumoral thyroid tissue (H&E, original magnification �200). (C) Squamous metaplasia and morule formation (H&E, original magnification�400). (D) Lymphoplasmacytic infiltration in the stroma of fibrovascular core making warthin-like appearance (H&E, original magnification �200). (E) Numerous psammoma bodies in mainly sclerotic and fibrotic stroma (H&E, original magnification �40). (F) Scattered psammoma bodies in the diffuse sclerotic and fibrotic background involving the entire thyroid lobe with hardly identifiable papillary carcinoma cells (H&E, original magnification �40). DSVPC, diffuse sclerosing variant of papillary carcinoma; H&E, hematoxylin and eosin. Color images available online at www.liebertonline.com=thy. three parameters, histologic subtype (DSVPC vs. non-DSVPC; p ¼ 0.032), extrathyroidal extension ( p ¼ 0.032), and tumor size (4 cm; p ¼ 0.002). However, multivariate Cox regression analysis revealed no independent significant variables. Figure 2 shows Kaplan–Meier estimates of recurrence-free survival between DSVPC and non-DSVPC. Discussion Generally, pediatric thyroid carcinoma shows different tumor characteristics compared with adult thyroid carcinoma. Pediatric thyroid carcinoma has larger tumor size and higher incidence of lymph node metastasis, lung metastasis,
and tumor recurrence than adult thyroid carcinoma does (7,8). However, paradoxically, the prognosis of patients with pediatric thyroid carcinoma is much better than that of adults (3–7). Namely, pediatric thyroid carcinoma demonstrated aggressive tumor presentation and excellent prognosis, but the reason for this discrepancy could not be explained until now. Zimmerman et al. suggested that this was related to the high incidence of nondiploid DNA contents in adult thyroid carcinoma compared with pediatric thyroid carcinoma (7). Another possible reason is that pediatric thyroid carcinoma is more dependent on thyroid-stimulating hormone; therefore, postoperative thyroid-stimulating hormone suppression with thyroid hormone replacement is more effective, and dedif-
DIFFUSE SCLEROSING PAPILLARY THYROID CARCINOMA IN THE YOUNG
1229
FIG. 2. Recurrence-free survival according to histologic subtype in papillary thyroid carcinoma.
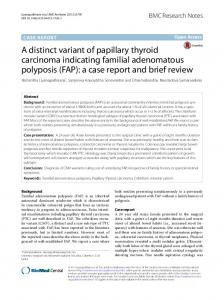
ferentiation from well-differentiated to poorly differentiated carcinoma does not often occur in pediatric thyroid carcinoma (10). Previous studies (1,3–8,11–13) of pediatric thyroid carcinoma are collectively summarized in Table 3. In our study, the male-to-female (M=F) ratio of pediatric thyroid carcinoma was 1:6.5, which showed more female predominance than the previous reports, in which the range was 1:1 to 1:3.3. In addition, the rate of extrathyroidal extension in our study (67.6%) was higher than that of the previous studies (14.6–42.1%). However, the rates of papillary carcinoma (83.8%), lymph node involvement (69.1%), tumor recurrence (23.5%), and metastasis (4.4%) were similar to those of previous studies. One important result of our study is that DSVPC (49.1%) was the most prevalent subtype of pediatric papillary carcinoma. The previous literature on pediatric thyroid cancer did not include a precise classification of tumors. The most prevalent type of pediatric thyroid cancer was papillary carcinoma; however, histologic subtypes of papillary carcinoma were not evaluated in detail in most studies (1,3,4,6–8,11–13). Harach and Williams (5) did report, however, that PTC in children under the age of 15 showed 42% of classical type, 33% of childhood (solid=follicular) type, 10% of DSVPC, and 6% of oxyphil type. When DSVPC was compared with conventional papillary carcinoma, it showed similar predilection for female sex, younger age at tumor presentation, and higher incidence of cervical lymph node involvement and lung metastasis (14–19). In our study, compared with the pediatric nonDSVPC group, DSVPC demonstrated bilateral involvement ( p ¼ 0.003), extrathyroidal extension ( p ¼ 0.009), lymph node involvement ( p ¼ 0.018), and increased number of tumorinvolved lymph nodes ( p ¼ 0.000) with statistical significance. Additionally, all three cases with lung metastasis were DSVPC. One of the reasons that DSVPC was associated with extended disease status is probably the widespread scattered tumor emboli in the intrathyroidal lymphatic channels, which are a characteristic pathologic feature of DSVPC. The DSVPC cases in our study were generally characterized by one thyroid lobe having a dominant tumor mass and the surrounding thyroid parenchyma having multiple tumor nodules and lymphatic tumor emboli. Two cases of DSVPC in our study
had widespread scattered psammoma bodies with hardly identifiable carcinoma cells. Therefore, careful examination is required to ascertain the presence of tumor involvement in these cases. It has been reported that there is no difference in the M=F ratio of DSVPC and conventional papillary carcinoma (14,18). In our study, the M=F ratio of DSVPC was 1:3.7 and that of non-DSVPC was 1:28, showing a relative female predominance in non-DSVPC. The prevalence of DSVPC among all papillary carcinomas in all age groups has been reported to range from 0.7% to 5.3% (15). We noted that 49.1% of pediatric papillary carcinoma patients had DSVPC. This is consistent with studies that the mean age of patients with DSVPC at presentation ranged from 18.0 to 34.7 years (14,16–19), which is about 10–30 years younger compared with that of conventional papillary carcinoma (45–50 years). Notably, patients with DSVPC had larger tumor size and more bilateral neck lymph node involvement likely leading them to seek medical attention at a younger age. This alone is unlikely to explain the higher prevalence of DSVPC in pediatric papillary carcinoma. Radiation exposure, iodine content for diet, familial predisposition, and associated syndromes such as familial polyposis syndrome in the cribriform morular type of papillary carcinoma could be possible contributing factors. DSVPC has been reported to have no BRAF mutation but has RET=PTC rearrangements (20). In other reports, childhood PTC in general was characterized by a relatively high prevalence of RET=PTC rearrangements with predominance of RET=PTC type 1 rearrangements (21,22). There is no consensus on the prognosis of DSVPC. In one report, DSVPC had a relatively poor prognosis as its diseasespecific death rate of 3.6% was higher than the 0.6% of pure PTC (23). In other reports, however, the 5- and 10-year survival rates of DSVPC were 95% (19) and 93% (17), respectively, a survival similar to conventional PTC. In our study, although recurrence-free survival rate of DSVPC was lower than that of non-DSVPC ( p ¼ 0.032), there was no difference in overall survival rate. However, the follow-up (mean, 55 months) in our study was probably too short to assess survival. In conclusion, our study showed that DSVPC is a major subtype of PTC in the young. In the pediatric population with PTC, the prevalence of bilateral thyroid involvement in DSVPC is higher than in non-DSVPC, as is extrathyroidal
1230
Histologic type Papillary Pure Follicular Follicular Recur Extrathyroidal extension Lymph node metastasis Distant metastasis Follow-up (years, mean) Died
Age criteria Number Age (years, mean or range) Male=female (ratio)
Parameter
29 (72.5) 2 (5.0) 22.0 2 (5.0)
55 (83.3)
8 (12.1) 15.4
0 (0)
3 (7.5) 8 (20.0) 13 (32.5)
34 (85)
11=29 (1:2.6)
16=50 (1:3.1)
7 (10.6) 57 (86.4) 2 (3.0)