FAST IMMUNOHISTOCHEMICAL BIOMARKER DETECTION DEVICE FOR CANCER TISSUE SLICES Ata Tuna Ciftlik1*, Bo Song2, Caroline Vandevyver3, Jean-Claude Bünzli2, Hans-Anton Lehr4, And Martin A.M. Gijs1 1
Laboratory of Microsystems, 2Laboratory for Lanthanide Supramolecular Chemistry, 3Research Commission EPFL-SNF, École Polytechnic Fédérale de Lausanne (EPFL), CH-1015 Lausanne, Switzerland, 4Institut Universitaire de Pathologie, Université de Lausanne, Rue du Bugnon 25, 1011 Lausanne, Switzerland
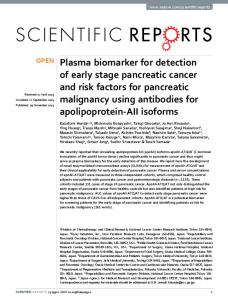
ABSTRACT We report an integrated lab-on-a-chip (LOC) to detect cancer tissue biomarkers, allowing fast (4 min) and large area (256 mm2) immunohistochemical analysis. Tissue Samples (TS) are mechanically clamped to a microfluidic structure and can be replaced within minutes. Assay time optimization is achieved by decreasing dead volumes, increasing the system pressure and realizing uniform reagent and buffer flows over the TS. KEYWORDS: Cancer Detection, Tissue Slice Analysis, Immunohistochemical Analysis, Biomarker Detection, Fast Tissue Analysis INTRODUCTION LOC devices are intrinsically compatible with cell-based applications. In contrast, incorporating a TS inside a microfluidic circuit remains challenging [1-3]. However, if fast detection of cancer tissue biomarkers could be achieved, this would enable immediate fine-tuning of interventions and treatments, even during surgery. Therefore, we realized an integrated LOC system with fast and semi-automated tissue-in/answer-out capability. We have demonstrated a first-generation LOC in PDMS, which permits relatively fast analysis of tissues (20 min versus the conventional 2 h) [4]. Unfortunately, this device showed a limited analysis speed and detection area. The system was unable to hold high pressures, resulting in a maximum operational flow speed of 50 nL/s. The cumbersome assembly and disassembly of the system (manual integration) significantly increased analysis time and dead volume. Also, only part of the TS slice could be exposed (less than a few 10% of the surface), thereby limiting the TS detection area. OPERATION PRINCIPLE We propose here the integrated system of Fig.1. The channels are formed by molding PDMS (Fig.1e) starting from a deep plasma-etched silicon master. The PDMS is squeezed between a glass slide and a PMMA structure (Fig.1b), the latter being designed to fit with commercial high-pressure diode valve fittings (Fig.1a). These are to be connected to automated syringe pumps filled with staining reagents. TS are put in place with a metal holder that is screwed to the PMMA structure, as shown in Fig.1b. Fig.1d shows an assembled device.
Figure 1: a) Illustration of the external fluidic circuit with functional parts indicated. b) Schematic cross-section of the integrated system indicating different parts and the tissue assembly mechanism. c) Schematic top-view of the fluidic microcircuit, the inlet-outlet structure with diode valves for buffer and reagents, and the tissue area (16 mm x 16 mm). d) Top-view photograph of the corresponding integrated system. e) Photograph of a PDMS part after demoulding. f) Close-up view of tissue area during testing with a colour-solution.
978-0-9798064-3-8/µTAS 2010/$20©2010 CBMS
699
14th International Conference on Miniaturized Systems for Chemistry and Life Sciences 3 - 7 October 2010, Groningen, The Netherlands
EXPERIMENTAL Our new device resolves the above-mentioned problems. Firstly, during TS replacement, check valves completely seal the external fluidic circuit and the whole device is kept stable, allowing fast and reproducible TS assembly (~1 min). Such integration also improves throughput, since we prevent re-filling the large dead-volume of the external microfluidic system in each replacement. Moreover, the new system can hold higher pressures, allowing faster flow speeds (10 µL/s), decreasing fill and wash times considerably (down to 3 s). The effective area is maximized (100%) and reagents diffuse uniformly over the large area due to the distributed channel network (Fig.1e, 1c).
Figure 2: Finite Element Method simulations of the convection in the tissue chamber for a 10 PL/s flow rate for 50 um chamber height (COMSOL® Multiphysics). After 2.5 s of buffer wash, the achieved concentration of the previous reagent is only 10-12 of its initial concentration. The fast operation is also verified by simulation (Fig.2). Table 1 quantitatively compares the conventional immunohistochemical analysis method with the microfluidic approaches. Fig.3 shows a fluorescent image of a breast cancer TS, as well as the detection of the estrogen receptor (ER) and human epidermal growth factor (HER2/neu) on the same tissue slice. Each analysis took only 4 min with the protocol listed in Table 2. Table 1: Figure of merit Q, which is a function of the tissue analysis area, assay time and total reagent volume, for different reported tissue slice analysis methods.
Figure 3: On-chip immunohistochemical detection of a breast cancer tissue slice. a) Bright-field image of the tissue section. b) Human Epidermal Growth Factor Receptor-2 (HER2/neu) detected by green-emitting Tb complex. c) Esterogene Receptor (ER) stained with red-emitting Eu complex by direct fluorescence. For details of the ER detection protocol, see Table 2. Note: For the tissue slice preparation, please see details in [4-5].
700
Table 2: Protocol for the ER analysis, taking in total 204 s and using 90 PL reagent consumption. For detailed information about the protocol see [4-5].
CONCLUSIONS
We expect that our fast and semi-automated device will enable analysis of TS and provide fast feedback, even at the surgical intervention site. Moreover, fast three-dimensional tissue reconstruction may become available, when combining TS results from a single biopsy sample. REFERENCES: [1] A. Queval et.al., Lab Chip, 2010, 10, 326-334 [2] E.M. Lucchetta, M.S. Munson, R.F. Ismagilov, Lab Chip, 2006, 6, 185-90. [3] S.M. Hattersley, C.E. Dyer, J. Greenman, S.J. Haswell, Lab Chip, 2008, 8, 1842-6 [4] B. Song, V. Sivagnanam et.al., Analyst, 2009, 134, 1991 - 1993 [5] S. C. Schäfer, H. A. Lehr, Pathobiology, 2007, 74, 259. CONTACT *A.T.Ciftlik, Tel: +41 21 693 79 89;
[email protected]
701