Jpn. J. Pharmacol. 90, 223 – 227 (2002)
FORUM MINIREVIEW Development and Application of Chymase Inhibitors Effect of Chymase Inhibitor on Vascular Proliferation Shinji Takai* and Mizuo Miyazaki Department of Pharmacology, Osaka Medical College, 2-7 Daigaku-machi, Takatsuki City, Osaka 569-8686, Japan Received July 25, 2002 Accepted August 30, 2002
ABSTRACT—In vascular tissues, angiotensin II is potentially cleaved from angiotensin I by chymase and angiotensin-converting enzyme (ACE). In the normal state, vascular ACE regulates local angiotensin II formation and plays a crucial role in the regulation of blood pressure, whereas chymase is stored in mast cells and has no enzymatic activity. Chymase is activated immediately upon its release into the extracellular matrix in vascular tissues after mast cells have been activated by stimuli such as vessel injury by grafting or a balloon catheter. In dog grafted veins, chymase activity is increased, and the vascular proliferation is suppressed by either a chymase inhibitor or an angiotensin II receptor blocker. After balloon injury in dog vessels, chymase activity is significantly increased in the injured artery, and a chymase inhibitor is effective in preventing the vascular proliferation, but an ACE inhibitor is ineffective. Chymase plays an important role in the development of vascular proliferation via the induction of local angiotensin II formation in injured vessels. Keywords: Chymase, Inhibitor, Vascular proliferation, Angiotensin II
ACE inhibitors could not suppress chymase-dependent Ang II formation, resulting in vascular proliferation in primate vessels despite the prevention of such proliferation in the rat. A recent clinical trial of an Ang II receptor blocker (ARB) succeeded in preventing restenosis after PTCA (15). These reports strongly suggest that chymase-dependent Ang II formation may play an important role in vascular proliferation. In this review, we address the usefulness of the chymase inhibitor on vascular proliferation.
Angiotensin (Ang) II plays an important role in vascular proliferation (1). In a rat model, neointimal formation in vessels injured by a balloon catheter was prevented by an angiotensin-converting enzyme (ACE) inhibitor (2). However, clinical trials of an ACE inhibitor for preventing restenosis after percutaneous transluminal coronary angioplasty (PTCA) were unsuccessful (3, 4). In graft experimental models, an ACE inhibitor was shown to be effective in preventing vascular proliferation in rat, while it was not in the baboon (5, 6). Such species differences in the effects of ACE inhibitors on neointimal formation may depend on species differences in the Ang II-forming pathways. Rat vascular tissues contain ACE as the only Ang IIforming enzyme, while the vascular tissues of human, monkey, dog and hamster contain chymase in addition to ACE as Ang II-forming enzymes (7 – 10). In general, chymase is known to hydrolyze the C-terminal side of proteins after aromatic amino acids such as Phe, Tyr and Trp. However, using the substrate Ang I, human, monkey, dog and hamster chymases cleave the Phe8-His9 bond of Ang I to yield Ang II, while rat chymase cleaves the Tyr4-Ile5 bond to form inactive fragments (11 – 14). It is thought that
ITA vs SV in grafts Coronary artery bypass grafting is offered to patients with ischemic heart disease (16, 17). The internal thoracic artery (ITA) and saphenous vein (SV) have been frequently used as coronary artery bypass conduits. However, the poor performance of the SV compared with the ITA is well known, and the disorder called “vein graft disease” is a problem that needs to be addressed clinically (18 – 20). Although early occlusions of the SV are thought to be chiefly due to intimal hyperplasia, the mechanism of vascular proliferation is unclear and drugs that prevent vascular proliferation are in great demand. Borland et al. reported that the contractile response of Ang II in isolated human SV was greater than that in the ITA, suggesting that the SV exhibits greater Ang II-mediated action than the
*Corresponding author. FAX: +81-726-84-6518 E-mail:
[email protected] 223
224
S. Takai & M. Miyazaki
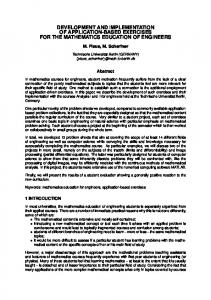
ITA (21). On the other hand, we demonstrated that the chymase activity, but not the ACE activity, was significantly higher in the SV than in the ITA (22). The ratio of chymase activity in the SV to that in the ITA was 162.6% and the total Ang II-forming activity was 163.5% in the SV. This high level of total Ang II-forming activity in the SV is thought to be dependent on the upregulated chymase activity. The number of chymase-positive cells in the SV was also significantly higher than in the ITA. Therefore, both the number of chymase-positive mast cells and the chymase-dependent Ang II-forming ability in the SV are higher than in the ITA and may play an important role in the development of vascular hyperplasia in the SV used as a graft conduit. Role of chymase in vascular proliferation In our models, dogs underwent common carotid artery bypass grafting with the ipsilaterial external jugular vein (23 – 27). The ACE activity in the grafted veins was significantly decreased up to 7 days after the operation; and especially after 1 and 3 days, it was suppressed in the grafted veins to less than 10% of the control value (24). The reason why the ACE activity was decreased at acute periods after the operation is thought to be dependent on the loss of the endothelium, because the endothelium in grafted veins is put under arterial pressure, thus resulting in the loss of the endothelium including ACE (24). On the other hand, 7 days after the operation, the chymase activity was significantly increased in the grafted veins. Considering these findings, up to 7 days after the operation, the Ang II formation in the grafted veins may depend mainly on the chymase-dependent Ang II-forming pathway. In fact, the Ang II concentration and the mRNA levels of fibronectin, collagen I and collagen III, all of which are induced by an increase of Ang II action, were significantly increased in the grafted veins 7 days after the operation (Fig. 1). These findings suggest that chymase-dependent Ang II formation plays an important role in the development of vascular proliferation in grafted veins. Effect of chymase inhibitor in graft-induced vascular proliferation Treatment with a chymase inhibitor, Suc-Val-ProPhep(Oph)2, to the vein only once before grafting was able to prevent the intimal hyperplasia in grafted veins 7 days after the operation in a dog model (24). The chymase inhibitor significantly suppressed increases of the Ang II concentration and the mRNA levels of fibronectin, collagen I and collagen III in the grafted veins 7 days after the operation (Fig. 1). In this model, an ARB, L-158809, also suppressed the vascular proliferation in dog grafted veins (25). These findings clearly suggest the significance of chymaseinduced Ang II formation on the vascular proliferation at an
Fig. 1. Effect of a chymase inhibitor, Suc-Val-Pro-PheP(OPh)2, on ratio of intimal area to medial area, chymase activity, angiotensin II concentration and mRNA levels of fibronectin, collagen I and collagen III in dog grafted veins 7 days after grafting. Modified from Ref. 24 with permission.
acute phase after grafting. However, it has been unclear how long a chymase inhibitor that is used only once during the operation will suppress intimal hyperplasia in dog grafted veins. We also investigated the long-term effect of Suc-Val-Pro-Phep(OPh)2 on intimal hyperplasia in dog grafted veins after bypass surgery. The ACE and chymase activities in the grafted veins were significantly increased to 2 and 15 times, respectively, compared with untreated veins 28 days after the grafting (23). The ACE and chymase activities in the grafted veins were activated after grafting, and the Ang II-forming activity via chymase was especially accelerated, suggesting that the activated Ang II formation via chymase may be important in the development of vascular proliferation. In fact, a single treatment with a chymase inhibitor into grafting veins maintained the suppres-
Role of Chymase on Vascular Diseases
sion of chymase activity and vascular proliferation 3 months after bypass surgery (27). On the other hand, chymase has been reported to activate stem cell factor, a typical cytokine that has the ability to induce accumulation of mast cells (28). The number of mast cells was significantly increased along with the chymase activity in the grafted veins 14 and 28 days after the operation, while it was significantly decreased by treatment with a chymase inhibitor (24). Therefore, inhibition of chymase is thought to prevent not only the Ang II formation but also the accumulation of mast cells. Recently, we demonstrated that oral administration of a chymase inhibitor, NK3201 (2-(5formylamino-6-oxo-2-phenyl-1,6-dihydropyrimidin-1-yl)N-[{3,4-dioxo-1-phenyl-7-(2-pyridyloxy)}-2-heptyl]acetamide) (Nippon Kayaku Co., Ltd., Tokyo), could also prevent both the chymase activity and the vascular proliferation in the grafted veins (26). Therefore, inhibition of chymase activity is thought to be useful for preventing vascular proliferation in grafted veins. Effect of chymase inhibitor in vascular proliferation after balloon injury In a dog balloon-injury model, a balloon catheter was inserted into the common carotid artery, and the artery was injured internally (29 – 32). Both ACE and chymase activities were increased by the injury, with the increase in chymase activity being greater than that of the ACE activity 1 month after the operation (29, 30). Both an ARB and an ACE inhibitor reduced blood pressure almost equally. An ACE inhibitor increased plasma renin activity more strongly than did candesartan, and it significantly decreased vascular and plasma ACE activity. An ARB significantly suppressed the formation of intimal hyperplasia in the injured arteries, while enalapril did not. The difference in the inhibitory action of ARBs and ACE inhibitors is thought to be that ACE inhibitors suppress only the Ang II action produced by ACE but that ARBs can suppress the Ang II action produced by chymase in addition to that by ACE. These results indicated that local Ang II production by chymase is involved in the intimal hyperplasia seen in the injured vessels. Recently, in this model, NK3201 significantly reduced intimal hyperplasia 1 month after the operation (31). However, NK3201, unlike ACE inhibitor and ARB, did not affect blood pressure or plasma renin activity. A chymase inhibitor may not be related to maintain blood pressure. Chymase is stored in mast cells and has no Ang II-forming ability in the normal state. Chymasedependent Ang II formation may function only in local states such as in injured vessels. On the other hand, ACE is expressed in endothelial cells of vascular tissues and has systemic Ang II-forming ability. In the hamster two-kidney, one clip (2K1C) hypertensive model, the blood pressure increased significantly 2 weeks after clipping (acute stage),
225
and it was sustained at a high level until 32 weeks after clipping (chronic stage) (33). Plasma renin activity increased significantly during the acute stage, but returned to the normal level at the chronic stage. In the chronic stage, the vascular ACE activity, but not the chymase activity, increased significantly, and an ACE inhibitor and an ARB showed equipotently hypotensive effects at the acute and chronic stages (33). In the dog 2K1C hypertensive model, a chymase inhibitor could not suppress the high blood pressure (S. Takai et al., unpublished data). These findings suggest that chymase is not involved in the pathogenesis of hypertension. Therefore, chymase-dependent Ang II formation plays a crucial role in the development of vascular proliferation, but not in the regulation of blood pressure. Agents for prevention of vascular proliferation Mast cells may be related to the pathogenesis of vascular proliferation. In injured vessls, mast cells have been activated by strong stimuli such as vein grafting or injury to arteries by a balloon catheter (24, 32). Chymase is activated immediately upon its release into the extracellular matrix in vascular tissues and strongly produces Ang II, which plays an important role in the development of vascular proliferation via the induction of growth factors and extracellular matrix (24). Therefore, agents for the prevention of vascular proliferation aim at three targets: stabilization of mast cells, inhibition of chymase activity, and blockage of Ang II receptor (Fig. 2). A mast cell stabilizer, tranilast, is reported to prevent vascular proliferation after balloon injury in experimental models. Howver, the dose of tranilast needed for prevention of vascular proliferation in experimental models is 10 times greater than that required for anti-allergic therapy (32, 33). On the other hand, tranilast failed to prevent restenosis after PTCA in clinical studies, in spite of using a dose several times higher than that for anti-allergic diseases (34, 35). Originally, mast cell stabilizers including tranilast has been used for the treatment of allergic diseases such as degranulation induced by immunoglobulin E, and a large dose may be needed to prevent mast cells activated by mechanical stimuli such as grafting or PTCA. Chymase inhibitor is able to prevent vascular proliferation in the vessels injured by grafting or a balloon catheter in the dog experimental model. The chymase inhibitor can inhibit the chymase activity released from mast cells when a strong stimulus such as grafting or PTCA is occurred. Therefore, chymase inhibitor may be needed less than mast cell stabilizer. In fact, in the dog grafting model, 1 mg /kg per day of a chymase inhibitor (NK3201) was needed for significant prevention of vascular proliferation, while 100 mg /kg per day of a mast cell stabilizer (tranilast) was needed (31, 32). Although mast cells release a large number of inflammatory mediators
226
S. Takai & M. Miyazaki
Fig. 2. Agents for prevention of vascular proliferation. Mast cell stabilizer supppresses mast cell activation, resulting in reducing the release of chymase (activation). Chymase inhibitor directly suppresses the activity of chymase after vessel injury such as in grafting or PTCA. Ang II receptor blocker inhibits Ang II action induced by chymase released from mast cells.
such as histamine, serotonin, chemotactic factors, cytokines and serine proteases, chymase may be a target for vascular proliferation. Therefore, chymase inhibitor, which can directly inhibit chymase activity, might be able to prevent vascular proliferation, even with a very low dose of it in comparison with mast cell stabilizer. ARB is reported to prevent vascular proliferation in both experimental and clinical studies (15, 25, 30). In our experimental study, the doses that brought about significant effects of prevention of vascular proliferation were several times greater than doses used in anti-hypertensive therapy (25, 30). Conceivably, an increase of chymase activity in the injured vessels strongly induces local Ang II formation, and a large dose of ARB may be needed for blocking the locally increased Ang II. Conclusion Two types of Ang II generating systems are involved in vascular tissues and these two have different functions. In the normal vessels, ACE regulates Ang II formation, whereas chymase is stored in mast cells and has no Ang IIforming activity. On the other hand, chymase functions as an Ang II-forming enzyme after mast cells have been activated by stimuli such as vessel injury by a balloon catheter or grafting, and the chymase-dependent Ang II formation occurs only in vascular incidents. Therefore, chymase inhibitor may be useful for preventing vascular proliferation without affecting blood pressure.
REFERENCES 1 Kim S and Iwao H: Molecular and cellular mechanisms of angiotensin II-mediated cardiovascular and renal diseases. Pharmacol Rev 52, 11 – 34 (2000) 2 Powell JS, Clozel JP, Muller RK, Kuhn H, Hefti F, Hosang M and Baumgartner HR: Inhibitors of angiotensin-converting enzyme prevent myointimal proliferation after vascular injury. Science 245, 186 – 188 (1989) 3 MERCATOR Study Group: Does the new angiotensin converting enzyme inhibitor cilazapril prevent restenosis after percutaneous transluminal coronary angioplasty? Circulation 86, 100 – 110 (1992) 4 Faxon DP: Effect of high dose angiotensin-converting enzyme inhibition on restenosis: final results of the MARCATOR Study, a multicenter, double-blind, placebo-controlled trial of cilazapril. J Am Coll Cardiol 2, 362 – 369 (1995) 5 Roux SP, Clozel JP and Kuhn H: Cilazapril inhibits wall thickening of vein bypass graft in the rat. Hypertension 18, Suppl 4, II43 – II46 (1991) 6 Hanson SR, Powell JS, Dodson T, Lumsden A, Kelly AB, Anderson JS, Clowes AW and Harker LA: Effects of angiotensin converting enzyme inhibition with cilazapril on intimal hyperplasia in injured arteries and vascular grafts in the baboon. Hypertension 18, Suppl 4, II70 – II76 (1991) 7 Okunishi H, Miyazaki M, Okamura T and Toda N: Different distribution of two types of angiotensin II-generating enzymes in the aortic wall. Biochem Biophys Res Commun 149, 1186 – 1192 (1987) 8 Takai S, Shiota N, Jin D and Miyazaki M: Functional role of chymase in angiotensin II formation in human vascular tissue. J Cardiovasc Pharmacol 32, 826 – 833 (1998) 9 Takai S, Jin D, Sakaguchi M and Miyazaki M: Chymase-dependent angiotensin II formation in human vascular tissue. Circulation 100, 654 – 658 (1999) 10 Takai S, Sakaguchi M, Jin D, Yamada M, Kirimura K and
Role of Chymase on Vascular Diseases
11
12
13
14
15
16 17
18 19
20
21
22
23
24
Miyazaki M: Different angiotensin II-forming pathways in human and rat vascular tissues. Clin Chim Acta 305, 191 – 195 (2001) Takai S, Shiota N, Sakaguchi M, Muraguchi H, Matsumura E and Miyazaki M: Characterization of chymase from human vascular tissues. Clin Chim Acta 265, 13 – 20 (1997) Takai S, Shiota N, Kobayashi S, Matsumura E and Miyazaki M: Induction of chymase that forms angiotensin II in the monkey atherosclerotic aorta. FEBS Lett 412, 86 – 90 (1997) Caughey GH, Raymond WW and Wolters PJ: Angiotensin II generation by mast cell alpha- and beta-chymases. Biochim Biophys Acta 1480, 245 – 257 (2000) Takai S, Shiota N, Yamamoto D, Okunishi H and Miyazaki M: Purification and characterization of angiotensin II-generating chymase from hamster cheek pouch. Life Sci 58, 591 – 597 (1996) Peters S, Gotting B, Trummel M, Rust H and Brattstrom A: Valsartan for prevention of restenosis after stenting of type B2 /C lesions: the VAL-PREST trial. J Invasive Cardiol 13, 93 – 97 (2001) Green GE, Stertzer SH and Reppert EH: Coronary arterial bypass grafts. Ann Thorac Surg 5, 443 – 450 (1968) Urschel HC, Miller ER, Razzuk MA, Alvares JF, McNamara JJ and Paulson DL: Aorta-to-coronary-artery vein bypass graft for coronary artery occlusive disease. Ann Thorac Surg 8, 114 – 125 (1969) Fuchs JC, Mitchener JS and Hagen PO: Postoperative changes in autologous vein grafts. Ann Surg 188, 1 – 15 (1978) Lytle BW, Loop FD, Cosgrove DM, Ratliff NB, Easley K and Taylor PC: Long-term (5 to 12 years) serial studies of internal mammary artery and saphenous vein coronary bypass grafts. J Thorac Cardiovasc Surg 89, 248 – 258 (1985) Lytle BW, Loop FD, Taylor PC, Simpfendorfer C, Kramer JR, Ratliff NB, Goormastic M and Cosgrove DM: Vein graft disease: the clinical impact of stenoses in saphenous vein bypass grafts to coronary arteries. J Thorac Cardiovasc Surg 103, 831 – 840 (1992) Borland JA, Chester AH, Crabbe S, Parkerson JB, Catravas JD and Yacoub MH: Differential action of angiotensin II and activity of angiotensin-converting enzyme in human bypass grafts. J Thorac Cardiovasc Surg 116, 206 – 212 (1998) Nishimoto M, Takai S, Sawada Y, Yuda A, Kondo K, Yamada M, Jin D, Sakaguchi M, Asada K, Sasaki S and Miyazaki M: Chymase-dependent angiotensin II formation in the saphenous vein versus the internal thoracic artery. J Thorac Cardiovasc Surg 121, 729 – 734 (2001) Takai S, Yuda A, Jin D, Nishimoto M, Sakagichi M, Sasaki S and Miyazaki M: Inhibition of chymase reduces vascular proliferation in dog grafted veins. FEBS Lett 467, 141 – 144 (2000) Nishimoto M, Takai S, Kim S, Jin D, Yuda A, Sakaguchi M, Yamada M, Sawada Y, Kondo K, Asada K, Iwao H, Sasaki S and Miyazaki M: Significance of chymase-dependent angiotensin II-forming pathway in the development of vascular pro-
227
liferation. Circulation 104, 1274 – 1279 (2001) 25 Yuda A, Takai S, Jin D, Sawada Y, Nishimoto M, Matsuyama N, Asada K, Kondo K, Sasaki S and Miyazaki M: Angiotensin II receptor antagonist, L-158,809, prevents intimal hyperplasia in dog grafted veins. Life Sci 68, 41 – 48 (2000) 26 Takai S, Jin D, Nishimoto M, Yuda A, Sakaguchi M, Kamoshita K, Ishida K, Sukenaga Y, Sasaki S and Miyazaki M: Oral administration of a specific chymase inhibitor, NK3201, inhibits vascular proliferation in grafted vein. Life Sci 69, 1725 – 1732 (2001) 27 Tsunemi K, Takai S, Nishimoto M, Yuda A, Jin D, Sakaguchi M, Sawada Y, Asada K, Kondo K, Sasaki S and Miyazaki M: Lengthy suppression of vascular proliferation by a chymase inhibitor in dog grafted veins. J Thorac Cardiovasc Surg 124, 621 – 625 (2002) 28 Zhang S, Anderson DF, Bradding P, Coward WR, Baddeley SM, MacLeod JD, McGill JI, Church MK, Holgate ST and Roche WR: Human mast cells express stem cell factor. J Pathol 186, 59 – 66 (1998) 29 Miyazaki M, Wada T, Shiota N and Takai S: Effect of an angiotensin II receptor antagonist, candesartan cilexetil, on canine intima hyperplasia after balloon injury. J Hum Hypertens 13, Suppl 1, S21 – S25 (1999) 30 Miyazaki M, Shiota N, Sakonjo H and Takai S: Angiotensin II type 1 receptor antagonist, TCV-116, prevents neointima formation in injured arteries in the dog. Jpn J Pharmacol 79, 455 – 460 (1999) 31 Takai S, Sakonjo H, Fukuda K, Jin D, Sakaguchi M, Kamoshita K, Ishida K, Sukenaga Y and Miyazaki M: A novel chymase inhibitor, 2-(5-formylamino-6-oxo-2-phenyl-1,6-dihydropyrimidine-1-yl)-N-[{3,4-dioxo-1-phenyl-7-(2-pyridyloxy)}-2-heptyl] acetamide (NK3201), suppressed intimal hyperplasia after balloon injury. J Pharmacol Exp Ther (in press) 32 Shiota N, Okunishi H, Takai S, Mikoshiba I, Sakonjo H, Shibata N and Miyazaki M: Tranilast suppresses vascular chymase expression and neointima formation in balloon-injured dog carotid artery. Circulation 99, 1084 – 1090 (1999) 33 Fukuyama J, Ichikawa K, Miyazawa K, Hamano S, Shibata N and Ujiie A: Tranilast suppresses intimal hyperplasia in the balloon injury model and cuff treatment model in rabbits. Jpn J Pharmacol 70, 321 – 327 (1996) 34 Tamai H, Katoh O, Suzuki S, Fujii K, Aizawa T, Takase S, Kurogane H, Nishikawa H, Sone T, Sakai K and Suzuki T: Impact of tranilast on restenosis after coronary angioplasty: tranilast restenosis following angioplasty trial (TREAT). Am Heart J 138, 968 – 975 (1999) 35 Tamai H, Katoh K, Yamaguchi T, Hayakawa H, Kanmatsuse K, Haze K, Aizawa T, Nakanishi S, Suzuki S, Suzuki T, Takase S, Nishikawa H and Katoh O: The impact of tranilast on restenosis after coronary angioplasty: the Second Tranilast Restenosis Following Angioplasty Trial (TREAT-2). Am Heart J 143, 506 – 513 (2002)