Circulation Journal Official Journal of the Japanese Circulation Society http://www. j-circ.or.jp
IMAGES IN CARDIOVASCULAR MEDICINE
High-Output Cardiomyopathy Regression Following Percutaneous Closure of Left Internal Mammary and Subclavian to Pulmonary Artery Fistulae Elias Adreanides, MD; Gregory Giamouzis, MD*,**; Gregory Pavlides, MD
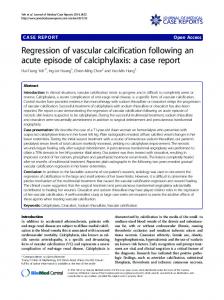
Figure. The large “post-CABG” fistula (A, arrow) between the LIMA and the LPA embolized using a 3.0×15-mm covered stent (B). The final result is excellent (C). Nonselective visualization of 2 large congenital fistulae (D, arrows) draining blood from the left subclavian artery (D, arrowheads) to the LPA. Using a right guiding catheter, the 2 collateral vessels are embolized with a 5-mm (E,F, arrow) and a 4-mm (F, arrowhead) diameter Amplatzer-Plug device, respectively. The final result is excellent (F). Selective visualization of a large congenital fistula (G, arrow) draining blood from the left axillary artery (G, arrowheads) to the LPA, embolized with a 5-mm Amplatzer-Plug (H, arrow) and showing an excellent final result (I). CABG, coronary artery bypass grafting; LIMA, left internal mammary artery; LPA, left pulmonary artery.
Received March 1, 2010; revised manuscript received April 6, 2010; accepted April 12, 2010; released online April 29, 2010 Time for primary review: 7 days First Cardiology Department, Onassis Cardiac Surgery Center, Athens, *Department of Cardiology, Larissa University Hospital, Larissa, Greece and **Division of Cardiology, Emory University Hospital, Atlanta, GA, USA Mailing address: Gregory Giamouzis, MD, Department of Cardiology, University of Thessaly, Larissa University Hospital, PO Box 1425, 411 10 Larissa, Greece. E-mail:
[email protected] ISSN-1346-9843 doi: 10.1253/circj.CJ-10-0177 All rights are reserved to the Japanese Circulation Society. For permissions, please e-mail:
[email protected] Circulation Journal Vol.74, June 2010
Cardiomyopathy Regression After Fistulae Closure
A
62-year-old man presented with progressive dyspnea on exertion. He had a history of coronary artery bypass graft surgery 9 years ago [left internal mammary artery (LIMA) to the left anterior descending artery, a saphenous vein graft (SVG) to the first obtuse marginal branch of the left circumflex artery, and SVG to the right coronary artery (RCA)], at which time transthoracic echocardiography demonstrated a left ventricular ejection fraction (LVEF) of 50% with mild dilatation of the LV (LV end-diastolic dimension (LVEDD), 63 mm). On present examination, echocardiography showed moderate LV dilatation (LVEDD, 75 mm) with impairment of the LV global contractility (LVEF, 35%). He underwent coronary angiography, which revealed: (1) patent grafts, without any significant lesions, (2) a large fistula between the LIMA and the left pulmonary artery (LPA, Figure A) that had not been present in the pre-coronary artery bypass grafting (CABG) evaluation, (3) multiple congenital fistulae, draining blood from the left subclavian (LSA, Figure D) and the left axillary (Figure G) arteries to the LPA, and (4) absence of any significant fistulae of the right IMA. On right-heart catheterization, the maximal QP/QS ratio was estimated at 1.5. We decided to close the LIMA fistula with percutaneous implantation of a 3.0×15-mm covered stent (Figure B), with an excellent final result and a fully patent LIMA post procedure (Figure C). Next, using a right guiding catheter, the 2 larger LSA collateral vessels were embolized with a 5- and a 4-mm diameter Amplatzer-Plug device, respectively (Figures E,F). Finally, the left axillary artery fistula was embolized with a 5-mm Amplatzer-Plug (Figure H). Immediately after the embolization the QP/QS ratio reduced to 1.2. The patient recovered uneventfully, with significant clinical improvement (NYHA I). At the 6- and 12-month post-procedural reassessment the patient remained asymptomatic, demonstrating a remarkable improvement in the LV dimensions (LVEDD, 63 mm) and function (LVEF, 50%). Several cases of “post-CABG”,1–4 as well as of congenital fistulae,5–8 have been previously reported. To the best of our knowledge, the combination of a “post-CABG” LIMA to PA fistula with multiple congenital subclavian and axillary to PA
1261 fistulae, as well as regression of the associated high-output cardiomyopathy following their percutaneous embolization, has never been previously reported. Whether the “postCABG” fistula was the result of surgical manipulations per se, a genetic tendency to develop acquired fistula (seen in patients with congenital fistulae) or a combination of both is not known. Most probably, some branches from the LIMA that could not be divided surgically at the previous operation were draining to the PA (the low pressure system) and gradually developed major fistulae. Further study of the vessel wall properties is needed to elucidate the etiology of such rare cases. Disclosures Conflict of Interest: none.
References 1. Wilsmore B, Gunalingam B. Iatrogenic coronary arteriovenous fistula during percutaneous coronary intervention: Unique insight into intra-procedural management. J Interv Cardiol 2009; 22: 460 – 465. 2. Patterson MS, Vaina S, Serruys PW. Percutaneous treatment of an iatrogenic cardiac fistula. Catheter Cardiovasc Interv 2008; 72: 259 – 262. 3. Kiernan T, Yan BP, Rosenfield K, Gupta V. Coil embolization of an iatrogenic coronary artery to cardiac vein fistula after rotational atherectomy. J Interv Cardiol 2008; 21: 410 – 413. 4. Shindo S, Honda Y, Katsu M, Kaga S, Inoue H, Matsumoto M. Recovery of cardiomegaly after treatment of traumatic popliteal arteriovenous fistula. Circ J 2009; 73: 776 – 778. 5. Chiu CZ, Shyu KG, Cheng JJ, Lin SC, Lee SH, Hung HF, et al. Angiographic and clinical manifestations of coronary fistulas in Chinese people: 15-year experience. Circ J 2008; 72: 1242 – 1248. 6. Hung WP, Wang JN, Chang HK, Chung TJ, Tsai YS, Wu JM. Congenital left ventricle-to-pulmonary artery fistula. J Am Coll Cardiol 2010; 55: 166. 7. Chowdhury UK, Rizhvi A, Sheil A, Jagia P, Mittal CM, Govindappa RM, et al. Successful surgical correction of a patient with congenital coronary arteriovenous fistula between left main coronary artery and right superior cavo-atrial junction. Hellenic J Cardiol 2009; 50: 73 – 78. 8. Soga Y, Hanyu M, Kawatou M, Yokota T, Nomoto T, Nakano J, et al. Congenital left internal thoracic artery-pulmonary artery fistula used as an inflow for a coronary artery bypass graft. J Thorac Cardiovasc Surg 2007; 134: 1581 – 1582.
Circulation Journal Vol.74, June 2010