Aug 30, 2017 - Impact & Effectiveness. Consistent Decreases In Prevalence of: ⢠HPV 6/11/16/18. ⢠Genital warts.
HPV Vaccine WHY? Prof. Karina Butler, Chair NIAC UCD Clinical Professor of Paediatrics Consultant Paediatrician & Infectious Diseases Specialist Our Lady’s Children’s Hospital &Temple Street Children’s University Hospital 30th August 2017
Why immunise? • HPV – about 100 different serotypes – assigned numbers (6, 11, 16, 18 etc) – Invade epithelial cell : skin cells, mucous membrane cells – Different serotypes favour different cell types (40 different types that infect the genital area).
• Almost everybody will experience an infection with HPV at some time in their lives – Generally transmitted by close, skin to skin contact – Infection can be transient – with no sypmtoms – For others - infection can persists
• Some – ‘High Risk’ serotypes if they persist , cause changes in the cells, which can progress to a pre cancers stage and ultimately result in cancer • Some of the low risk types cause genital warts
PREVENTING INFECTION WITH HPV PREVENTS CERVICAL CANCER
PREVENTING INFECTION WITH HPV 16 AND 18 WILL PREVENT 7 OUT OF 10 (70%) CERVICAL CANCERS In Ireland - Every Year
About 300 women develop cervical cancer 90 women die from cervical cancer
HPV and Cancer • And that’s not all…….. • HPV cause other cancers:90% anal 70% vaginal 50% penile 40% vulvar And 13- 72% oropharyngeal cancers
• Introduced in 2006 – now in use in > 60 countries • 270+ million doses globally • 660,000 doses in Ireland • >200,000 fully vaccinated
A Systematic Review of Global Data
Impact & Effectiveness of Quadrivalent Vaccine Review 10 yrs Real World experience Vaccinated vs Contemporaneous unvaccinated
Vaccinated & Unvaccinated vs Pre Vaccine Era
Impact & Effectiveness Consistent Decreases In Prevalence of: • HPV 6/11/16/18 • Genital warts • Low, & high grade cellular changes. • Pre cancer lesions
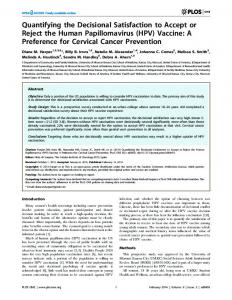
Surveillance study Hypothesis: If the vaccine is effective HPV would decline in vaccinated and unvaccinated over time • 4 sites using Quadrivalent vaccine • Women 13 – 26 yrs • 3 waves of surveillance – 2007–8 (N371), – 2009-2010 (N409) – 2013-2014 (N400)
Proportion of women infected with high risk HPV serotypes Proportion vaccinated
HPV+ unvaccinated 75% HPV+ All participants 90.8% HPV+ in vaccinated
• Significant reduction in proportion infected with vaccine serotypes 34.8 -14.1 -8.7% • Reduction also in unvaccinated 32.5-17.4-22.0% • No change in prevalence of non-vaccine serotypes
THIS VACCINE WORKS
Parental concerns • POTS (Postural Orthostatic Tachcardia Syndrome) • CRS (Chronic Regional Pain Syndrome) • CFS/ME (Chronic Fatigue Syndrome/Myalgic encephalitis) • GBS (Guilian Barre Syndrome) • An Altered Life • Loss of health and vitality
EMA review 2015 • EMA confirms evidence does not support that HPV vaccines cause CRPS or POTS • In the general population about 150/million girls and young women aged 10 – 19 yrs may develop CRPS and at least 150/million develop POTS. • The occurrence of POTS/CRPS is no higher in the vaccinated population than in the unvaccinated
Meeting of the Global Advisory Committee on Vaccine Safety, 7–8 June 2017 • The Global Advisory Committee on Vaccine Safety (GACVS), an independent expert clinical and scientific advisory body, provides WHO with rigorous advice on vaccine safety issues of potential global importance.
http://www.who.int/wer
HPV vaccine is safe • Since 2006 – 270 million doses distributed • Safety reviews 2008, ‘9, ‘13, ‘14, ‘15 and 2017 • Risk of anaphylaxis 1.7/million doses (Risk of anaphylaxis with Penicillin 1 - 5/10,000) • Fainting a common anxiety or stress related reaction • No other adverse reactions identified
Safety concerns raised and addressed • Guillian Barre Syndrome:
– UK: 10.4 million doses of vaccine – no increased risk after any dose – US: 60+ million doses – no increased risk – Can exclude risk greater than 1/million doses (General population risk 1-2/100,000)
• POTS/CRS/Ovarian Failure
– No evidence of causal association
• Coeliac disease
– Not causally related, prexisting condition identified during clinic visit
• Administration in Pregnancy
– Inadvertent administration to 600,000 pregnant women – No adverse outcome
“There are now accumulated safety studies that include several million persons and which compare the risks for a wide range of health outcomes in vaccinated and unvaccinated subjects. However, despite the extensive safety data available for this vaccine, attention has continued to focus on spurious case reports and unsubstantiated allegations. The Committee continues to express concern that the ongoing unsubstantiated allegations have a demonstrable negative impact on vaccine coverage in a growing number of countries, and that this will result in real harm”. GACVS June 2017
Misinformation dissemination and HARM “Several countries that have introduced HPV vaccines to
their immunization programme have reported a 50% decrease in the incidence rate of uterine cervix precancerous lesions among younger women. In contrast, the mortality rate from cervical cancer in Japan, where HPV vaccination is not proactively recommended, increased by 3.4% from 1995 to 2005 and is expected to increase by 5.9% from 2005 to 2015. This acceleration in disease burden is particularly evident among women aged 15–44 years.”
Why immunise? We have a vaccine that is • SAFE and • EFFECTIVE • It can prevent Cancer • It will save Lives
THANK YOU