Hay ID, Morris JC. 1996 Toxic adenoma and toxic ... Kosugi S, Shenker A, Mori T. 1994 Constitutive activation of cyclic AMP but not phosphatidylinositol ...
0021-972X/98/$03.00/0 Journal of Clinical Endocrinology and Metabolism Copyright © 1998 by The Endocrine Society
Vol. 83, No. 2 Printed in U.S.A.
Hyperfunctioning Thyroid Nodules in Toxic Multinodular Goiter Share Activating Thyrotropin Receptor Mutations with Solitary Toxic Adenoma* MASSIMO TONACCHERA, LUCA CHIOVATO, ALDO PINCHERA, PATRIZIA AGRETTI, EMILIO FIORE, FILOMENA CETANI, ROBERTO ROCCHI, PAOLO VIACAVA, PAOLO MICCOLI, AND PAOLO VITTI Istituto di Endocrinologia (M.T., L.C., A.P., P.A., E.F., F.C., R.R., P.V.), Dipartimento di Oncologia Sezione di Anatomia Patologica (P.V.), and Dipartimento di Clinica Chirurgica (P.M.), Universita` di Pisa, Pisa, Italy ABSTRACT Toxic multinodular goiter is a cause of nonautoimmune hyperthyroidism and is believed to differ in its nature and pathogenesis from toxic adenoma. Gain-of-function mutations of the TSH receptor gene have been identified as a cause of toxic adenoma. The pathogenesis at the molecular level of hyperfunctioning nodules in toxic multinodular goiter has yet not been reported. Six patients with a single hot nodule within a multinodular goiter and 11 patients with toxic thyroid adenoma were enrolled in our study. At histology five hyperfunctioning nodules in multinodular goiters showed the features of adenomas, and one was identified as a hyperplastic nodule. The entire exon 10 of the TSH receptor gene was directly sequenced after PCR amplification from genomic DNA obtained from surgical specimens. Functional studies of mutated receptors were performed in COS-7 cells. Five out of 6 (83%) hyperfunctioning nodules within toxic multi-
nodular goiters harbored a TSH receptor mutation. A TSH receptor mutation was also evident in the hyperfunctioning nodule that at histology had the features of noncapsulated hyperplastic nodule. Among toxic adenomas, 8 out of 11 (72%) nodules harbored a TSH receptor mutation. All the mutations were heterozygotic and somatic. Nonfunctioning nodules, whether adenomas or hyperplastic nodules present in association with hyperfunctioning nodules in the same multinodular goiters, had no TSH receptor mutation. All the mutations identified had constitutive activity as assessed by cAMP production after expression in COS-7 cells. Hyperfunctioning thyroid nodules in multinodular goiters recognize the same pathogenetic event (TSH receptor mutation) as toxic adenoma. Other mechanisms are implicated in the growth of nonfunctioning thyroid nodules coexistent in the same gland. (J Clin endocrinol Metab 83: 492– 498, 1998)
T
distinguishable from nonfunctioning nodules and extranodular parenchyma (1, 2). Recently, somatic gain-of-function mutations of the TSH receptor (TSHr) gene have been identified as a cause of toxic adenoma (4 –10), although controversy still exists about the frequency of such mutations in this condition. The majority of hot nodules in 11 patients with toxic adenoma were found to harbor an activating TSHr mutation by Parma et al. (4, 6). Subsequent studies by other groups reported a lower frequency of TSHr mutations in toxic adenoma ranging from 3% (8) to 20% (9 –11). The pathogenesis of hyperfunctioning nodules in toxic multinodular goiter has not been investigated at the molecular level and, to our knowledge, no data on TSHr mutations in this condition are available. The aim of the present study was to search for activating TSHr mutations in hyperfunctioning thyroid nodules arising in toxic multinodular goiters of patients living in an area of iodine deficiency. Patients with well-defined single hyperfunctioning nodules within a toxic multinodular goiter were selected. The frequency of TSHr mutations was also studied in patients with solitary toxic adenoma living in the same area. TSHr mutations were identified by direct sequencing of the entire exon 10 of the TSHr gene after PCR amplification of genomic DNA obtained from surgical specimens. Our results indicate that activating TSHr mutations occur in the majority of hyperfunctioning nodules within toxic
OXIC multinodular goiter is a cause of nonautoimmune hyperthyroidism and is believed to differ in its nature and pathogenesis from toxic adenoma (1). Toxic adenoma is a benign neoplasm presenting as a discrete solitary hyperfunctioning and capsulated thyroid nodule surrounded by normal thyroid tissue (1, 2); rarely two or more adenomas coexist in an otherwise normal thyroid gland (multiple adenomatosis) (3). Toxic multinodular goiter is commonly found in areas of iodine deficiency, in which patients with long-standing nontoxic goiter frequently develop thyrotoxicosis (3). The term toxic multinodular goiter encompasses a spectrum of different clinical entities, ranging from a single hyperfunctioning nodule within an enlarged thyroid gland having additional nonfunctioning nodules, to multiple hyperfunctioning areas scattered throughout the gland, barely Received July 22, 1997. Revision received September 16, 1997. Accepted October 22, 1997. Address all correspondence and requests for reprints to: Massimo Tonacchera, Istituto di Endocrinologia, Universita` degli Studi di Pisa, Via Paradisa 2, 56124, Cisanello, Pisa. * This work was supported by grants from the National Research Council (CNR Rome, Italy: Target Project Biotechnology and Bioinstrumentation, Grant 91. 01219, PF 70; Target Project: Prevention and Control of Disease Factors (FATMA), Grant 93. 00689, PF 41; EEC Stimulation Action-Science Plan Contract SC1-CT91– 0707; Target Project Ageing, Subproject Gerontobiology, Grant 93. 00437. PF 40).
492
TSHr MUTATIONS IN TOXIC NODULAR GOITER
multinodular goiters and suggest that, similar to toxic adenoma, gain-of-function TSHr mutations are responsible for the genesis of hyperfunctioning nodules in multinodular goiters. No TSHr mutation was identified in adenomatous or hyperplastic nonfunctioning nodules contained in the same gland. A new, not previously described TSHr mutation, was identified in a hyperfunctioning nodule of a patient with multinodular goiter. Patients and Methods
493
changes. A diffuse oxyphil pattern was observed in one case of toxic adenoma. At histology, five out of six hyperfunctioning nodules contained in multinodular goiters showed the typical features of adenomas. In the remaining patient with toxic multinodular goiter (patient 14), the hyperfunctioning nodule was a noncapsulated hyperplastic nodule with a micro-macrofollicular architecture and no compression of the adjacent tissue. At histology, nonfunctioning thyroid nodules in patients 12 and 16 were not distinguishable from hyperfunctioning adenomas contained in the same gland, showing a typical thin fibrous capsule and a micromacrofollicular architecture. All the remaining nonfunctioning nodules were noncapsulated hyperplastic nodules.
Patients Included in this study were 17 patients who were submitted to surgery. Eleven of them had toxic adenoma and 6 had toxic multinodular goiter. Lobectomy was performed in patients with toxic adenoma and subtotal or near total thyroidectomy in those with toxic multinodular goiter. At the time of diagnosis, all patients were clinically thyrotoxic with high free T4 (FT4) and FT3 concentrations and undetectable serum TSH by a sensitive method. Thyroid autoimmunity was excluded for the absence of circulating antithyroglobulin, antithyroperoxidase, and antiTSHr antibodies. Thyroid glands were studied by clinical examination, thyroid ultrasound, scintiscan imaging using 131I, and histology. All patients were prepared before surgery with methimazole and iodide.
Thyroid ultrasound Ultrasound evaluation was performed by the same examiner using a linear transducer (7.5 MHz) attached to a real-time instrument (AU 590 Asynchronous Apparatus, Esaote Biomedica, Milan, Italy). Patients were examined in the supine position with the neck hyperextended. Thyroid volume was calculated according to the formula of the ellipsoid model (12): width (mm) 3 length (mm) 3 thickness (mm) 3 0,52 3 each lobe 5 volume (mL). The thyroid volume used as the normal reference value, obtained by measurements of 130 adult healthy individuals (65 males and 65 females) residing in urban areas with sufficient iodine intake of the same region, was 11.3 6 3.4 mL in males and 8.6 6 2.2 mL in females.
Classification of disease Laboratory evaluation of thyroid function Thyroid diseases were classified according to the following criteria. Toxic adenoma. Cases of toxic adenoma had 1) a solitary nodule in an otherwise normal thyroid gland as assessed by palpation and thyroid ultrasound; 2) exclusive 131I uptake in the nodule (hot nodule) with suppression of the extranodular parenchyma at thyroid scintiscan; and 3) a well-circumscribed lesion surrounded by a fibrous capsule at histology. Toxic multinodular goiter. Cases of toxic multinodular goiter had 1) an enlarged thyroid gland with two or more nodules as assessed by palpation and thyroid ultrasound; 2) exclusive 131I uptake in one nodule with functional suppression of the extranodular tissue and coexistent nonfunctioning nodules; and 3) multinodular goiter at histology. Age, sex, and the findings at thyroid ultrasound in patients with toxic adenoma or toxic multinodular goiter are shown in Tables 1 and 2, respectively. Functioning and nonfunctioning thyroid nodules were identified by matching the ultrasound and thyroid scintigraphy and were carefully isolated during surgery from the surrounding tissue. Four patients had two or more nonfunctioning nodules each; the remaining two had only one nonfunctioning nodule each. At microscopic examination, all solitary toxic adenomas were well defined tumors surrounded by a complete thin fibrous capsule with compression of the adjacent tissue. All toxic adenomas exhibited a micro-macrofollicular architecture with occasional foci of necrosis, hemorrhage, and cystic
FT4 and FT3 were measured by RIA (Lysophase, Technogenetics SpA, Milan, Italy). Thyrotropin was assessed with a sensitive method (sensitive-TSH IRMA, Delfia, Wallac, Finland). Antithyroperoxidase and antithyroglobulin antibodies were measured by passive agglutination (SERODIA-AMC and SERODIA-ATG, Fujirebio, Tokyo, Japan). TSHr antibodies were measured using a commercial radioreceptor assay (TRAK assay, B.R.A.H.M.S., Berlin, Germany).
Sequence determination Genomic DNA was extracted from hyperfunctioning and nonfunctioning thyroid nodules and from the normal extranodular tissue, as previously described (6, 13). We sequenced the entire portion of the C-terminal region of the TSHr gene coding for all seven transmembrane segments, and extracellular and intracellular loops codified by exon 10. At least two different PCR amplifications from genomic DNA were sequenced on double strands with sense and antisense primers. Two fragments encompassing the entire exon 10 of the TSHr gene were amplified by PCR and subjected to direct sequencing (13). Fragment A, positions 942-1960; forward primer: 59 TGTGAATGCCTTGAATAGCC 39; reverse primer 59 AACAGCTATGACCATGTGAGAGGCTTGTTCAGAATT 39. Fragment B, positions 1746 –2204; forward primer: 59 TGTAAAACGACGGCCAGTTATTGTTTTTGTTCTGACGC 39; reverse primer: 59 ATGTTGTGGAGACCCTGCCT 39. Underlined sequences correspond to the M13 sequencing primer.
TABLE 1. Age, sex, and findings at thyroid ultrasound in patients with toxic adenoma Patient no.
Age
Sex
1 2 3 4 5 6 7 8 9 10 11
46 51 46 49 29 51 61 36 41 40 36
F F F M F M M F F F M
a
Hyperfunctioning nodule
Contralateral lobe
Diameter (mm)
Volumea (mL)
Ultrasound pattern
Diameter (mm)
Volumea (mL)
39 3 60 3 68 30 3 42 3 70 50 3 90 3 60 49 3 51 3 57 36 3 50 3 65 25 3 35 3 50 26 3 48 3 40 21 3 24 3 34 30 3 39 3 43 40 3 45 3 55 47 3 52 3 58
83 46 140 74 61 23 26 9 26 52 74
Solid, hypoechogenic Mixed Mixed Mixed Mixed Solid, hypoechogenic Solid, isoechogenic Solid, isoechogenic Mixed Solid, isoechogenic Mixed
15 3 15 3 30 11 3 12 3 17 13 3 10 3 28 12 3 14 3 35 15 3 10 3 35 11 3 11 3 30 14 3 16 3 35 12 3 12 3 35 11 3 15 3 36 10 3 12 3 30 15 3 12 3 35
3 1 2 3 3 2 4 3 3 2 3
Volume of nodules and of contralateral lobes were calculated according to ellipsoid formula (see Patients and Methods).
494
JCE & M • 1998 Vol 83 • No 2
TONACCHERA ET AL.
TABLE 2. Age, sex, and findings at thyroid ultrasound in patients with toxic multinodular goiter
Patient no.
Age
Hyperfunctioning nodulea
Sex
Extranodular tissue
Cold nodules
Diameters (mm)
Volumeb (mL)
Ultrasound pattern
no.
Diameter (mm)
Volumeb (mL)
28 3 38 3 40 10 3 13 3 16 10 3 12 3 18 12 3 12 3 15 12 3 14 3 20 18 3 25 3 30 15 3 18 3 25 20 3 15 3 25 18 3 20 3 28 18 3 23 3 29 20 3 22 3 25 15 3 18 3 22 16 3 20 3 25
22 1 1 1 2 7 3.5 4 5 6 6 3 4
12 13
48 54
M F
30 3 40 3 50 34 3 40 3 45
31 32
Mixed Solid, isoechogenic
1 3
14
35
F
30 3 30 3 40
19
Mixed
3
15
30
M
32 3 38 3 48
30
Mixed
2
16 17
53 42
F M
27 3 43 3 42 35 3 40 3 60
25 44
Mixed Solid, isoechogenic
1 3
Volumeb,c (mL)
21 10 91 11 27 120
a
All hyperfunctioning nodules but that of patient 14 were defined as adenomas on microscopic examination (see text). Volume of nodules and of extranodular tissue were calculated according to ellipsoid formula (see Patients and Methods). Volume of extranodular tissue was calculated by measuring diameter of whole lobes and by subtracting volumes of functioning and nonfunctioning nodules. b c
Primer containing the M13 sequences were biotinylated. PCR was performed in a final volume of 100 mL containing 1 mg DNA, 50 mm KCl, 10 mm Tris-Cl, pH 8.3, 1.5 mm MgCl2, 0.01% gelatin, 0.2 mm deoxynucleotide triphosphate, 5 U Taq polymerase (Gibco BRL, Life Technologies, Gaithersburg, MD) and 150 nm (for fragment A) or 200 nm (for fragment B) of each primer. Annealing temperature was 50 C and 54 C for fragments A and B, respectively. PCR products were purified on streptavidin-coated magnetic beads (Dynal, Oslo, Norway) and sequenced with Sequenase (version 2, United States Biological, Cleveland, OH) (14) and 35 S-labeled deoxyadenosine ATP-a S (Amersham, Buckingamshire, UK). No other coding region of the gene was sequenced. To confirm the presence of a TSHr mutation, all mutations were subcloned in a plasmid, and sequences were repeated on individual clones. Contamination problems were ruled out by including PCR control samples with no DNA as template. Extraction of DNA and pre-PCR reactions were performed in different rooms with respect to post-PCR reactions.
Construction and expression of mutated genes pSVL-TSHr constructs harboring mutations D619G, A623V, L629F, I630L, T632I, D633E, and P639S were obtained by replacing, within the original wild-type construct (wtTSHr), a CvnI-BstEII segment (positions 1604 –2169) directly amplified from genomic DNA of affected patients. This mutated segment was obtained as previously described (4, 5). To facilitate the insertion in a pSVL-based construct of I486M, a unique SpeI restriction site within the sequence encoding the end of transmembrane segment I of wtTSHr was created as described in Parma et al. (6). Constructs containing the mutant TSHr sequences were obtained by replacing a SpeI-CvnI segment (positions 1322–1603) from this new construct by the corresponding segments of the mutants, obtained by direct PCR amplification of genomic DNA. The sequences of the resulting mutated constructs were verified by double-stranded sequencing. COS-7 cells transfected with wild type, and mutated receptors were used for binding studies and cAMP determination. COS-7 cells were grown in DMEM supplemented with 10% FBS, 100 IU mL21 penicillin, 100 mg mL21 streptomycin, 2.5 mg mL21 fungizone, and 1 mm sodium pyruvate. For the transient expression of mutated TSHrs, COS-7 cells were seeded at the concentration of 150,000 cells/3-cm dish. One day after seeding, cells were transfected using the diethylaminoethyl (DEAE)-Dextran method followed by a 2-min 10% dimethylsulfoxide shock.
Functional assays Forty-eights hours after transfection, cells were used for cAMP production assay and 125I TSH binding studies. All experiments were performed in triplicate, and each experiment was repeated at least three times. Results were expressed as mean 6 se.
TABLE 3. Base substitutions and amino acid modification in hyperfunctioning nodules TSHr gene codon
Base substitution
Amino acid change
Patient no.
486 619 623 629 630 632 633 639
ATC/ATG GAT/GGT GCC/GTC TTG/TTT ATC/CTC ACC/ATC GAC/GAG CCA/TCA
Ile/Met Asp/Gly Ala/Val Leu/Phe Ile/Leu Thr/Ile Asp/Glu Pro/Ser
6 17 9 11,14 5,12 4, 7,10,13 1 16
cAMP assay production. Cells were washed with hypotonic medium (HBSS without NaCl) and preincubated in the same buffer for 30 min at 37 C. This was followed by a 1-h incubation at 37 C in the presence of 0.5 mm isobutylmethylxantine (IBMX), as a cAMP phosphodiesterase inhibitor, in the absence of bovine TSH (bTSH). Extracellular cAMP was measured in the medium collected at the end of the incubation by an in-house RIA method using a commercial polyclonal anti-cAMP antibody, as previously described (15). 125
I TSH binding assay. Forty-eight hours after transfection, cells were washed with Hanks’ solution in which NaCl was replaced by sucrose 280 mm containing 0.2% BSA and 2.5% low-fat milk (6). Binding studies were performed by incubating cells in the same medium at room temperature for 4 h in the presence of 80,000 counts/min 125I TSH, (35 mCi/mg, 40 U/mg) and the appropriate concentrations of cold bTSH (125I TSH was a gift from B.R.A.H.M.S. Diagnostica). At the end of the incubation, cells were rinsed twice with ice-cold Hanks’ medium and then solubilized with 1 N NaOH. Cell-bound radioactivity was determined in a g-counter. Under these conditions, nonspecific binding (defined as the radioactivity bound to dishes in the presence of 100 mU/mL cold bTSH) was identical to that bound to mock transfected cells (1% of total counts added). In the absence of a consensus about the bioactivity of pure bTSH (16), we expressed all TSH or TSHr concentrations in milliunits per milliliters, assuming a 1:1 stoichiometry for TSH binding to its receptor. The competitive binding curves were made to fit by nonlinear regression assuming a single receptor site (17).
Results
Direct sequencing of exon 10 of the TSHr gene revealed the presence of a mutation in 13 out of 17 hyperfunctioning nodules (Table 3 and Fig. 1). Five out of 6 (83%) hyperfunctioning nodules within toxic multinodular goiter harbored a
TSHr MUTATIONS IN TOXIC NODULAR GOITER
495
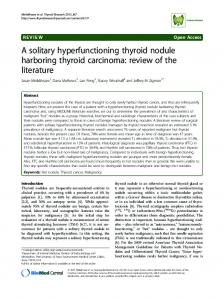
FIG. 1. Nucleotide sequence of gene segments encoding part of TSHr gene of hyperfunctioning nodules. Direct sequencing ( u ) (noncoding strand: sequence is shown as antisense CAT) of PCR-amplified DNA corresponding to part of first (I486M) extracellular loop of receptor is illustrated. Direct sequencing (coding strand) of PCR-amplified DNA corresponding to part of third intracellular loop (D619G, A623V) and VI transmembrane segment (L629F, I630L, T632I, D633E, P639S) is illustrated. Wild-type alleles coexist in each case with mutated alleles. Base substitutions and amino acid change are also shown in Table 3.
TSHr mutation (patients 12, 13, 14, 16, and 17). Included in these five cases harboring a TSHr mutation was also the patient in whom the hyperfunctioning nodule at histology appeared as a noncapsulated hyperplastic nodule rather than a true adenoma. Among toxic adenomas, 8 out of 11 (72%) nodules (patients 1, 4, 5, 6, 7, 9, 10, and 11) harbored a TSHr mutation. Most mutations were located in the VI transmembrane segment. In two nodules, a phenylalanine instead of a leucine in position 629 (L629F) was identified, and in two others, a leucine instead of a isoleucine in position 630 (I630L) was identified. An isoleucine instead of a threonine in position 632 (T632I) was found in four cases, and a glutamic acid instead of an aspartic acid (D633E) and a serine instead of a proline in position 639 (P639S) were detected in two distinct nodules. In two cases an amino acidic substitution was located in the third intracellular loop: a glycine instead of an aspartic acid (D619G) and a valine instead of an alanine (A623V). Interestingly, a methionine replacing an isoleucine in the first extracellular loop (I486M) was also found in one nodule. All the mutations identified were heterozygotic and somatic. Direct sequence analysis of genomic DNA revealed that the proportion of the mutated and wild-type allele were similar, suggesting that the mutation affected only one allele and that it was dominant. Mutation P639S is a new, not previously described mutation. Only wtTSHr sequences were found in the normal extranodular tissue and in nonfunctioning nodules. Functional characteristics of the TSHr mutations
The L629F and I630L mutations have been recently reported (18, 19), but their functional characteristics were not yet published. The P639S mutation has been identified in this study for the first time. The functional characteristics of mutations L629F, I630L, and P639S were analyzed. To demon-
strate that the L629F, I630L, and P639S are activating mutations responsible for the development of hyperfunctioning nodules, the cAMP pathway was studied. Basal cAMP production was measured after transient expression of 250 ng DNA of various constructs in COS-7 cells. As previously shown, cells transfected with wtTSHr exhibited an increased production of cAMP compared to cells transfected with vector alone (Fig. 2). Cells transfected with constructs harboring the mutated receptors L629F, I630L, or P639S exhibited an increased cAMP production with respect to the wtTSHr (Fig. 2). As assessed by 125I TSH binding experiments, all mutated TSHr constructs showed lower levels of expression on the cell surface (Fig. 2, Table 4), demonstrating that the increased cAMP production was not caused by overexpression of the receptor. The functional characteristics of the D619G, A623V, T632I, and D633E mutations were already described (4 – 6, 20 –22). Discussion
In the present study we showed that, similarly to solitary toxic thyroid adenomas, the large majority of single hyperfunctioning thyroid nodules within toxic multinodular goiters harbor an activating TSHr mutation. A TSHr mutation was found in 83% of single hyperfunctioning nodules within toxic multinodular goiters and in 73% of toxic thyroid adenomas. Activating TSHr mutations in toxic thyroid adenomas have been described in several studies (4 –10, 20), but their frequency varies greatly varies in different studies (8 – 11, 20). The occurrence of TSHr mutations was never reported in hyperfunctioning nodules within multinodular goiters. The latter disease is commonly believed to differ in its nature and pathogenesis from toxic thyroid adenoma (1). The term toxic multinodular goiter encompasses a spectrum of different clinical conditions ranging from a single hyperfunctioning nodule in an enlarged thyroid gland bearing one or more nonfunctioning nodules to hyperfunctioning areas
496
TONACCHERA ET AL.
FIG. 2. Basal cAMP production of mutated TSHrs expressed in COS-7 cells. DNA (250 ng/dish) of mutated receptors (L629F, I630L, P639S), wtTSHr, or pSVL alone were transfected in COS-7 cells. The same cultures (150,000/cells dish) were studied for basal cAMP (A) and 125I TSH binding (B). Accumulation of cAMP was expressed as picomoles per dish (mean 6 SE). Total receptor amount [maximum binding capacity (Bmax)] and dissociation constant (Kd) are shown in Table 4.
TABLE 4. Bmax and Kd of wtTSHr and mutated TSH receptors after expression in COS-7 cells Construct
wtTSHr L629F I630L P639S
Bmax
Kd
0.37 6 0.05 0.16 6 0.01 0.23 6 0.03 0.20 6 0.03
2.2 6 0.3 0.8 6 0.09 1.3 6 0.18 1.1 6 0.20
Bmax, expressed in milliunit equivalents of TSH per milliliter; Kd expressed in milliunits/per milliliter.
scattered throughout the gland, barely distinguishable from nonfunctioning nodules and extranodular parenchyma (1, 2). Toxic multinodular goiter is frequently found in iodinedeficient areas (1, 2), where patients with long-standing goiter experience a progressive increase in size and number of nodules. Within this process, thyroid function may progress from a fully TSH-dependent condition to autonomy (i.e. independent from TSH regulation), and then to overt thyrotoxicosis.
JCE & M • 1998 Vol 83 • No 2
According to current pathogenetic concepts, toxic multinodular goiter results from chronic TSH stimulation leading to progressive accumulation of new follicles with heterogeneous ability of iodine turnover and hormone synthesis (23– 26). Follicles with high rates of iodine turnover eventually progress towards autonomous growth and function (i.e. independent from TSH regulation). Large clusters of autonomously functioning thyroid follicles may mimic hyperfunctioning adenomas (24). The observation that similar to toxic thyroid adenoma single hyperfunctioning thyroid nodules within toxic multinodular goiters harbor a TSHr gene mutation, suggests that the basic mechanism leading to the formation of toxic thyroid adenoma and hyperfunctioning nodules in toxic multinodular goiter is the same. TSHr gene mutations were found in four out of five hyperfunctioning nodules within multinodular goiters that at microscopic examination were diagnosed as true adenomas but, interestingly, also in the one hyperfunctioning nodule that lacked the histological features of true adenoma. The notion that toxic thyroid adenoma is more frequent and that toxic multinodular goiter is almost exclusively observed in areas of iodine deficiency (27–30) suggests that iodine deficiency and/or chronic TSH stimulation plays a role in the clinical expression of gain-of-function mutations of the TSHr gene. In all cases of toxic multinodular goiter, the hyperfunctioning nodules were greater in size than nonfunctioning nodules. Although we have no information about the time of appearance of nonfunctioning and hot nodules, respectively, it could be argued that further growth of nonfunctioning nodules was prevented by the suppression of TSH by the hyperfunctioning nodules. All TSHr gene mutations identified in the present study were shown to activate constitutively either the cAMP cascade alone or both the cAMP and the inositolphosphate pathways. Mutations D619G, A623V, T632I, and D633E were already shown to increase intracellular cAMP accumulation in the absence of the specific ligand (20). The I486M mutation displays a constitutive activity also towards the phosholipase-C pathway (6). Two mutations (L629F and I630L) had been already reported (18, 19), but their functional activity had not been studied. The P639S is a newly identified mutation. When transfected in COS cells, mutations L629F, I630L, and P639S increased basal cAMP accumulation to a greater extent as compared with wtTSHr. In binding experiments, these mutated receptors displayed lower expression levels as compared with the wtTSHr, indicating that the increased cAMP accumulation was not caused by an overexpression of mutated receptors. These functional data prove that the above-described amino acid substitutions are indeed active mutations of the TSHr and not simple polymorphysms. Mutations were mainly located in the VI transmembrane segment of TSHr, confirming that this is a hot spot for gain-of-function mutations (4, 7, 10, 20). When genotype was correlated to phenotype, no relationship was found between the type or location of the mutation and the size of the nodule, its ultrasound pattern (solid, cystic, hypo- or hyper-isoechogenic), or the degree of thyrotoxicosis. Seventy-three percent of toxic thyroid adenomas con-
TSHr MUTATIONS IN TOXIC NODULAR GOITER
sidered in this study were found to harbor a TSHr mutation. A much lower frequency of TSHr mutations in toxic thyroid adenoma was found by other authors (8 –11). This discrepancy might be because of racial differences in the population studied (Caucasian vs. Japanese), or to different criteria utilized to define toxic thyroid adenoma. Failure to entirely sequence exon 10 of the TSHr gene (8) or the use of less-sensitive techniques, such as single-stranded conformational polymorphism, might also explain the lower frequency of TSHr gene mutations reported in other studies (8, 31, 32). A further explanation is that several of these studies used material obtained from fine-needle aspiration (7, 9), in which normal tissue surrounding the hyperfunctioning nodule can dilute the DNA expressing the mutated allele. Our data confirm the notion that gainof-function mutations of the TSHr gene account for the majority of toxic thyroid adenomas. The minority of hyperfunctioning thyroid nodules with no TSHr mutation could result from alterations of other proteins involved in the activation of the cAMP pathway. In this respect, it is interesting to note that Gsa mutations (gsp oncogene) were reported in about 30% of toxic thyroid adenomas (33). At variance with the hyperfunctioning nodules of toxic multinodular goiters, nonfunctioning thyroid nodules within the same gland, whether histologically classified as true adenomas or as hyperplastic nodules, lacked TSHr mutations. This observation indicates that the mutated TSHr sequences in hyperfunctioning nodules identified in this study are somatic. Other mechanisms are implicated in the growth of nonfunctioning thyroid nodules coexistent in the same gland (32, 34). In conclusion, our data indicate that single hyperfunctioning thyroid nodules within toxic multinodular goiters recognize the same pathogenetic event (an activating TSHr mutation) as toxic thyroid adenoma. The pathogenetic mechanisms involved in the development of other varieties of toxic multinodular goiter in which distinct hyperfunctioning nodules are not recognized, remain to be elucidated. Addendum
When the present manuscript was under review, a study by Parma et al. was published in the August 1997 issue of Journal of Clinical Endocrinology and Metabolism (35). This paper confirms the high frequency of TSHr mutations in toxic thyroid adenoma. As shown in Table 1 in that article, 6 out of the 33 patients studied had a toxic multinodular goiter. This finding was not further discussed. Acknowledgments We thank Dr. F. Lippi, Dr. C. Marcocci, Prof. Enio Martino, and Dr. Furio Pacini for their clinical help in identifying patients with thyroid diseases. We thank Henning B.R.A.H.M.S. Diagnostica GmBH (Berlin) for kindly providing 125I-TSH tracer (TRAK).
References 1. Hay ID, Morris JC. 1996 Toxic adenoma and toxic multinodular goiter. In: Braverman LE, Utiger RD, eds. Werner and Ingbar’s the thyroid. Philadelphia: Lippincott-Raven; 566 –572.
497
2. Hamburger JI. 1987 The autonomously functioning thyroid nodule: Goetsch’s disease. Endocr Rev. 8:439 – 450. 3. Wiener JD. 1987 Plummer’s disease: localized thyroid autonomy. J Endocrinol Invest. 10:207–224. 4. Parma J, Duprez L, Van Sande J, et al. 1993 Somatic mutations in the thyrotropin receptor gene cause hyperfunctioning thyroid adenomas. Nature. 365:649 – 651. 5. Paschke R, Tonacchera M, Van Sande J, Parma J, Vassart G. 1994 Identification and functional characterization of two new somatic mutations causing constitutive activation of the TSH receptor in hyperfunctioning autonomous adenomas of the thyroid. J Clin Endocrinol Metab. 79:1785–1789. 6. Parma J, Van Sande J, Swillens S, Tonacchera M, Dumont JE, Vassart G. 1995 Somatic mutations causing constitutive activity of the thyrotropin receptor are the major cause of hyperfunctioning thyroid adenomas: identification of additional mutations activating both the cyclic adenosine 39,59-monophosphate and inositolphosphate-Ca11 cascades. Mol Endocrinol. 9:725–733. 7. Porcellini A, Ciullo I, Laviola L, Amabile A, Fenzi G, Avvedimento V. 1994 Novel mutations of thyrotropin receptor gene in thyroid hyperfunctioning adenomas. J Clin Endocrinol Metab. 79:657– 661. 8. Takeshita A, Nagayama Y, Yokoyama N, et al. 1995 Rarity of oncogenic mutations in the thyrotropin receptor of autonomously functioning thyroid nodules in Japan. J Clin Endocrinol Metab. 1195:80:2607–2610. 9. Porcellini A, Tassi V, Ciullo I, et al. 1995 Studies on the prevalence of TSH receptor mutations in a large series of consecutive hyperfunctioning adenomas. Thyroid. 5[Suppl 1]:S-8. (Abstract). 10. Russo D, Arturi F, Suarez HG, et al. 1996 Thyrotropin receptor gene alterations in thyroid hyperfunctioning adenomas. J Clin Endocrinol Metab. 81:1548 –1551. 11. Kopp P, Wilkes B, Gu WX, Jameson JL. 1997 Absence of mutations in the TSH receptor and the Gsa subunit in nodules and adenomas of multinodular goiters and identification of a new activating mutation (Tyr 601 Asp) in a solitary toxic adenoma. Thyroid 6[Suppl 1]:S-9. (Abstract). 12. Brunn J, Blocjk U, Ruf J, Bos I Kunze WP, Scriba PC. 1983 Volumetrie der Schildrusenlappen mittels real-time sonographie. Dtsch Med J. 287:1206 –1207. 13. Tonacchera M, Van Sande J, Cetani F, et al. 1996 Functional characteristics of three new germline mutations of the TSH receptor gene causing autosomal dominant toxic hyperplasia. J Clin Endocrinol Metab. 81:547–554. 14. Tabor S, Richardson CC. 1989 Selective inactivation of the exonuclease activity of bacteriophage T7 DNA polymerase by in vitro mutagenesis. J Biol Chem. 264:6447– 6458. 15. Vitti P, Chiovato L, Ceccarelli P, et al. 1986 Thyroid stimulating antibody mimics thyrotropin in its ability to desensitize 39-59-monophosphate response to acute stimulation in continuously cultured thyroid cells (FRT-L5). J Clin Endocrinol Metab. 454 – 458. 16. Rapoport B, Seto P. 1985 Bovine thyrotropin has a specific bioactivity 5- to 10-fold that of previous estimates for highly purified hormone. Endocrinology. 116:1379 –1382. 17. Swillens S. 1995 Interpretation of binding curves obtained with high receptor concentrations: practical aid for computer analysis. Mol Pharmacol. 47:1197–1203. 18. Duprez L, Parma J, Dumont JE, Hermans J, Vassart G. 1996 Diversity and prevalence of somatic mutations in the TSH receptor gene as a cause of toxic adenoma. J Endocrinol Invest. 19[Suppl 6]:69. (Abstract). 19. Paschke R, Fuehrer D, Holzapfel HP. 1996 Identification of different thyrotropin receptor mutations in toxic multinodular goiter. J Endocrinol Invest. 19[Suppl 6]:28. (Abstract). 20. Van Sande J, Parma J, Tonacchera M, Swillens S, Dumont JE, Vassart G. 1995 Somatic and germline mutations of the TSH receptor gene in thyroid diseases. J Clin Endocrinol Metab. 80:2577–2585. 21. Kosugi S, Shenker A, Mori T. 1994 Constitutive activation of cyclic AMP but not phosphatidylinositol signaling caused by four mutations in the 6th transmembrane helix of the human TSH receptor. FEBS Lett. 356:291–294. 22. Porcellini A, Ciullo I, Pannain S, Fenzi GF, Avvedimento E. 1995 Somatic mutations in the VI transmembrane segment of the thyrotropin receptor constitutively activate cAMP signalling in thyroid hyperfunctioning adenomas. Oncogene. 11:1089 –1093. 23. Peter HJ, Studer H, Forster R, Gerber H. 1982 The pathogenesis of hot and cold follicles in multinodular goiters. J Clin Endocrinol Metab. 55:941–946. 24. Studer H, Peter HJ, Gerber H. 1989 Natural heterogeneity of thyroid cells: the basis for understanding thyroid function and nodular goiter growth. Endocr Rev. 10:125–135. 25. Studer H, Gerber H, Zbaeren J, Peter HJ. 1992 Histomorphological and immunohistochemical evidence that human nodular goiters grow by episodic replication of multiple clusters of thyroid follicular cells. J Clin Endocrinol Metab. 875:1151–1158. 26. Studer H, Derwahl M. 1995 Mechanisms of nonneoplastic endocrine hyperplasia: a changing concept: a review focused on the thyroid gland. Endocr Rev. 16:411– 426. 27. Belfiore A, Sava L, Runello F, Tomaselli L, Vigneri R. 1983 Solitary autonomously functioning thyroid nodules and iodine deficiency. J Clin Endocrinol Metab. 56:283–287.
498
TONACCHERA ET AL.
28. Dremier S, Coppee F, Delange F, Vassart G, Dumont JE, Van Sande J. 1996 Thyroid autonomy; mechanism and clinical effects. J Clin Endocrinol Metab. 81:4187– 4193. 29. Als C, Listewnik M, Rosler H, Bartkowiak E. 1995 Immunogenic and non immunogenic hyperthyroidism. Nucl Med. 34:92–99. 30. Baltisberger BL, Minder CE, Burgi H. 1995 Decrease of incidence of toxic nodular goiter in a region of Switzerland after full correction of mild iodine deficiency. Eur J Endocrinol. 132:546 –549. 31. Tonacchera M, Cetani F, Parma J, Van Sande J, Vassart G, Dumont J. 1996 Oncogenic mutations in thyroid adenoma: methodological criteria. Eur J Endocrinol. 135:444 – 446.
JCE & M • 1998 Vol 83 • No 2
32. Tonacchera M, Van Sande J, Parma J, et al. 1996 TSH receptor and disease. Clin Endocrinol (Oxf). 44:621– 633. 33. O’Sullivan C, Barton CM, Staddon S, Brown CL, Lemoine NR. 1991 Activating point mutations of the gsp oncogene in human thyroid adenomas. Mol Carcinogen. 4:345–349. 34. Dumont JE, Lamy F, Roger P, Maenhaut C. 1992 Physiological and pathological regulation of thyroid cell proliferation and differentiation by thyrotropin and other factors. Physiol Rev. 72:667– 697. 35. Parma J, Duprez L, Van Sande J, et al. 1997 Diversity and prevalence of somatic mutations in the thyrotropin receptor and Gsa genes as a cause of toxic thyroid adenomas. J Clin Endocrinol Metab. 82:2695–2701.