Journal of Consulting and Clinical Psychology 2006, Vol. 74, No. 3, 545–554
Copyright 2006 by the American Psychological Association 0022-006X/06/$12.00 DOI: 10.1037/0022-006X.74.3.545
Internet-Based Health Information Consumer Skills Intervention for People Living With HIV/AIDS Seth C. Kalichman, Charsey Cherry, Demetria Cain, Howard Pope, Moira Kalichman, and Lisa Eaton
Lance Weinhardt Medical College of Wisconsin
University of Connecticut
Eric G. Benotsch University of Colorado Medical information can improve health, and there is an enormous amount of health information available on the Internet. A randomized clinical trial tested the effectiveness of an intervention based on social– cognitive theory to improve information use among people living with HIV/AIDS. Men and women (N ⫽ 448) were placed in either (a) an 8-session intervention that focused on Internet information consumer skills or (b) a time-matched support group and were followed to 9 months postintervention. The Internet skills group demonstrated greater Internet use for health, information coping, and social support compared with the control group. The authors conclude that people with HIV infection may benefit from increased access to health information on the Internet and that vulnerability to misinformation and fraud can be reduced through behavioral interventions. Keywords: AIDS coping, Internet health information, digital divide
net for health information report having more supportive resources, use more active coping strategies, and have higher CD4 cell counts and lower HIV viral loads than HIV-positive persons who do not use the Internet for health information (Kalichman et al., 2005). Unfortunately, information available online is not equally accessible to everyone. Less educated, economically disadvantaged, and socially marginalized individuals are least likely to access the Internet (Bolt & Crawford, 2000; Kalichman, Weinhardt, Benotsch, Rompa, et al., 2002; Schloman, 2004). The Internet is also an unregulated medium with the potential to do harm, particularly to people facing chronic or life-threatening illnesses. Alongside life-saving information, there are misinformation and unfounded claims on the Internet that can detract from medical care (Kunst, Groot, Latthe, Latthe, & Khan, 2002). As many as 25% of complementary and alternative medicine Web sites contain statements that could lead to direct harm (Berland et al., 2001; Walji et al., 2004). In addition, better educated and more health-oriented individuals are more likely to access health information online (Dutta-Bergman, 2004). We have reported that better educated individuals are less vulnerable to misinformation and fraudulent claims found online (Benotsch, Kalichman, & Weinhardt, 2004; Kalichman, et al., 2006). Interventions are therefore needed that extend beyond merely increasing Internet access to people diagnosed with chronic conditions. Improving the interpretation and use of health information found online requires skills for locating and evaluating relevant health information. The intervention tested in this research is skills based and aims to develop self-efficacy and skills for health information seeking on the basis of principles from social– cognitive theory (Bandura, 1997); we posit that behavior changes, including coping behaviors, occur through a sense of agency for
Access to health information can have positive effects on the quality of life and health of people with chronic and lifethreatening illnesses. The Internet offers a powerful means for obtaining information about medical conditions and their treatments. In a national survey of Internet users, 40% of respondents reported having used the Internet for health-related functions in the previous year (Baker, Wagner, Singer, & Bundorf, 2003). Eighty percent of adult Internet users have searched for health information, with 63% searching for information on specific diseases and 47% searching for medical treatments (Fox & Fallows, 2003). Among individuals diagnosed with chronic conditions who use the Internet, nearly half search online for information and advice regarding their illness (Wagner, Baker, Bundorf, & Singer, 2004). Health information found online can enable people with chronic illnesses to access the exact information they are seeking, including identifying coping and support resources (Baker et al., 2003). For example, people living with HIV infection who use the Inter-
Seth C. Kalichman, Charsey Cherry, Demetria Cain, Howard Pope, Moira Kalichman, and Lisa Eaton, Department of Psychology, University of Connecticut; Lance Weinhardt, Center for AIDS Intervention Research, Medical College of Wisconsin; Eric G. Benotsch, Department of Psychology, University of Colorado. National Institute of Mental Health Grant R01-MH63666 supported this research. We thank the AIDS Survival Project of Atlanta, Jeff Graham, Dan Dunable, Sheri Crump, Vernon (Amandi) Harmon, Phillip Meeks, Sheridan Gordon, Chris (Akil) Lee, and the National Society of Black Engineers/Georgia Institute of Technology Chapter for their assistance with this study. Correspondence concerning this article should be addressed to Seth C. Kalichman, Department of Psychology, University of Connecticut, 406 Babbidge Road, Storrs, CT 06269. E-mail:
[email protected] 545
KALICHMAN ET AL.
546
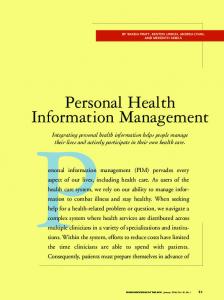
performing specific acts under specified conditions (Lazarus & Folkman, 1984). In earlier research, we demonstrated that, among people living with HIV infection, using the Internet to search for health-related information was associated with self-efficacy for informationseeking and problem-focused coping and greater social support (Kalichman et al., 2003, 2005). We have proposed a conceptual model predicting that increased access to health information and health information consumer skills will increase information seeking, support seeking, and other active coping strategies, which, in turn, will facilitate emotional well-being and social support among people with chronic illnesses (Kalichman et al., 2003; Kalichman, Weinhardt, & Benotsch, 2002). Figure 1 shows a schematic of the model articulated in our intervention and its expected outcomes. Social– cognitive intervention components for building skills for using the Internet for health and support resources are expected to increase self-efficacy and skills for Internet use as well as improve active coping and information-seeking coping. The schematic also shows that self-efficacy and skills for using the Internet for health and support resources will result in Internet use for these functions. Active coping and information-seeking coping influence Internet use and impact social support and emotional well-being. Findings from preliminary tests of this model were consistent with previous research that showed that information-seeking and active coping were associated with beneficial health outcomes for people with chronic medical conditions (Devins & Binik, 1996). The findings are also consistent with research that indicates potential health benefits of using information technologies for health information (Gustafson, Hawkins, & Boberg, 2002). The current study, although it does not empirically test the depicted model, uses the model shown in Figure 1 to test a community-based intervention to assist people with HIV in using the Internet for health and support improvement functions. The purpose of the current study is to test the effects of an intervention designed to (a) improve health information consumer skills and increase Internet use and (b) improve information seeking, active coping, social support, and emotional well-being among people living with HIV/AIDS. We test an intervention that was derived from social– cognitive theory (Bandura, 1997) concepts for behavioral skills building that focuses on increasing selfefficacy and skills for using the Internet to identify, evaluate, and use quality health information (see Figure 1). The intervention trial uses a two-arm randomized design with follow-ups every 3 months for 9 months postintervention. On the basis of social– cognitive theory, which posits that skills-building experiences enhance self-
Figure 1.
efficacy and foster behavior change (Bandura, 1997), we hypothesized that the Internet health information consumer skillsbuilding intervention would increase self-efficacy for seeking health information and increase Internet health informationseeking skills and behaviors. Consistent with our conceptual model, use of the Internet for health and support were among the outcomes expected from the intervention. On the basis of our conceptual model, which predicts that increased use of the Internet for health information and support will improve active coping and mental health–related quality of life, we further hypothesized that the Internet skills intervention would increase information seeking and active coping as well as improve social support and reduce symptoms of affective depression among people living with HIV infection.
Method Participants The study was conducted in Atlanta, Georgia; 62% of AIDS cases in Georgia are reported in the Atlanta metropolitan area. In Georgia, 73% of people with AIDS are men, 81% are African American, and 41% are between the ages of 30 and 39 years. The study participants were 320 men, 116 women, and 12 transgender individuals who had used the Internet for any purpose fewer than three times in the month before screening. Sample size was determined by power analysis with effect sizes from past interventions for mental health outcomes with people living with HIV/AIDS (Kalichman et al., 2001). All participants had tested HIV positive. The mean age of participants was 42.5 years (SD ⫽ 6.9), and the average number of years of education was 12.2 (SD ⫽ 1.9). All participants were fluent in English. The majority of participants were African American (n ⫽ 399; 89%), with 36 (8%) White participants and 13 (3%) of other racial backgrounds. Most participants (n ⫽ 354; 80%) reported an annual income below $10,000. With respect to HIV transmission risk history, 40% of the sample consisted of men who had a history of having sex with men, and 20% of the sample had a history of injection drug use. Sixty-eight percent of the sample was taking antiretroviral medications. The mean number of years since testing HIV positive was 10.2 (SD ⫽ 5.6); 54% had CD4 cell counts under 200, and 28% had undetectable viral loads.
Recruitment and Randomization Men and women were recruited from AIDS service organizations, health care providers, social service agencies, and infectious disease clinics throughout Atlanta. Recruitment occurred between March 2002 and May 2004. Participants were required to show a photo identification and proof of HIV status (e.g., HIV-positive test result, HIV clinic card, or HIV medication prescription) and were screened for (a) reading literacy with the
Schematic model for Internet skills-building intervention and expected outcomes.
INTERVENTION TO IMPROVE INTERNET USE Test for Functional Health Literacy for Adults (Parker, Baker, Williams, & Nurss, 1995; ␣ ⫽ .89 in current sample) and (b) having used the Internet fewer than three times in the past month. Figure 2 shows the participant flow through the study. A total of 835 individuals were screened for the study. Persons who scored below 75% correct on the Test for Functional Health Literacy for Adults (n ⫽ 18) and individuals who indicated having used the Internet three or more times in the past month (n ⫽ 290) were offered enrollment in alternative studies. Of the 527 persons scheduled for baseline, 448 (85%) completed the assessment and were randomized to conditions. Randomization was accomplished by a random-numbergenerated sequence of condition-coded labels to assign participants to conditions. Participants received $35 for completing the baseline assessment, with $5 added to the amount of each of the 3-, 6-, and 9-month follow-ups.
Establishing a Community Technology Access Center (CTAC) All participants had to be assured equal, secure, and private Internet access during the study to allow for a viable test of the intervention outcomes. We therefore established a CTAC at an AIDS service agency
Figure 2.
547
that also served as the site for the intervention trial. The CTAC was located adjacent to the AIDS service agency’s treatment resource library and was equipped with 11 state-of-the-art workstations and an instructional computer linked to an LCD projector. There were no content filters or usemonitoring systems enabled on the computers to allow complete and private access to the Internet. The CTAC was open to all agency clients as well as the public when intervention groups were not in session. CTAC users were asked to sign in and sign out at each visit. Participants were not required to log onto computers and were afforded complete privacy in their Internet use.
Intervention Conditions Several aspects of the experimental and comparison groups were held constant across conditions. Both interventions consisted of eight 120-min group sessions that met twice weekly for 4 consecutive weeks. Group sessions for both conditions consisted of 6 to 10 participants with one male and one female community-based group facilitator, at least one of whom was an HIV-positive peer counselor. Facilitators crossed conditions, and adherence to intervention protocols and contamination were monitored in postsession briefings and weekly facilitator supervision. Sessions were
Flow diagram of participant progress through the randomized clinical trial.
548
KALICHMAN ET AL.
conducted with men and women in mixed-gender groups. All participant incentives were the same for both conditions. Internet skills-building intervention. The Internet skills-building intervention met in the CTAC. The first two sessions provided an introduction to the group and an introduction to computers and the Internet. This segment included exercises to motivate interest in using the Internet and group activities for searching for information of personal interest. There was considerable time dedicated to exploring different Web browsers and their functions. The first two sessions of the intervention aimed to reduce anxieties about using computers, gain familiarity with the Internet, and motivate interest in using the Internet. Participants also established e-mail accounts, explored chat rooms and instant messaging, and discussed the opportunities and hazards of online relationships. In Session 3, participants were instructed in criteria for evaluating the quality of information obtained online (Eysenbach & Diepgen, 1998; Kim, Eng, Deering, & Maxfield, 1999), derived from nine common Web site evaluation criteria: content accuracy, disclosure of authors, source credibility, currency of information, Web page design, usability, documentation of claims, number and quality of links, and contact information. We selected Price and Entin’s (1999) Web site evaluation schema to train participants because it is structured within an easy to remember acronym: purpose–information–links– originator–timeliness (PILOT). Participants practiced applying the PILOT criteria to Web sites that they located while in group. In the context of interactive group discussions, the facilitators walked participants through the application of the PILOT criteria using search results obtained in session from topics volunteered by group participants. Participants searched the Internet using an LCDprojected Internet connection with a wireless keyboard and mouse. This procedure allowed facilitators to model searching the Internet and using the PILOT criteria and also allowed group members to offer feedback and reinforcement for Internet searches. Participants also shared ideas for evaluating quality of information, such as checking information across Web sites and contacting information sources to answer questions. The next major segment of the intervention was a transition from using the Internet to seek any information to using the Internet as a tool for health and support improvement (Sessions 4 –7). This segment continued to use many of the same techniques established in earlier activities, including facilitator modeling, practice in small groups, and Internet access outside of the CTAC. Participants were instructed in searching for health information, care and support resources, and clinical trials. The PILOT criteria were again applied to evaluating health and support Web sites. Role plays were conducted with guided feedback, and participants practiced strategies for integrating health information identified on the Internet into their routine health care, including developing communication skills for taking information located online to their health care providers. For example, participants conducted searches of health information, evaluated search results, and role played taking information to their doctor. The intervention concluded with a personalized, integrated summary of Internet uses, quality evaluation, social uses, and critical thinking skills. The final session included reviewing skills associated with developing online social support and strategies for gaining access to the Internet at home and elsewhere The intervention was extensively pilot tested during its development (manuals are available from Seth C. Kalichman). Health information support group. The control condition was a timeand contact-matched social support group for men and women living with HIV infection, modeled after information support groups offered in the community (Buck, 1991). The control condition did not introduce cognitive or behavioral components for improving health information evaluation skills. The sessions included an information update on HIV disease, management of health problems, and nutrition and its role in health maintenance. Medication access and adherence strategies were also emphasized in this condition. Participants examined means for managing medication regimens and discussed requesting medication information from their health care providers. Health goals and health improvement strategies were
reviewed prior to the end of the final group session. Participants in the control condition met in a support group room in the same building as the CTAC, had full access to the CTAC, and received a tour of the CTAC.
Measures Measures were collected according to an instructor-guided selfadministration procedure. That is, measures were administered in groups of 4 to 8 persons. Participants were shown page by page how to complete the study measures with a projected facsimile of the instruments and instructions. This procedure was adapted from previous research (e.g., Kalichman, Weinhardt, Benotsch, Rompa, et al., 2002) to ensure that instructions for each measure were carefully described and that participants were given privacy with minimal demand characteristics when responding. All of the participants in this study were able to read and self-administer the measures within approximately 1 hr. All measures were administered at baseline and at all follow-up assessments, except for the group experience measures, which were only administered at immediate postintervention, and the Internet skills evaluation assessment, which was administered at baseline and at the 3-month follow-up. Demographics and health characteristics. Participants were asked their gender, age, years of education, income, race, and HIV risk history. Participants also reported the year they first tested HIV positive, their most recent CD4 cell count, their viral load, and their experience of 14 HIV disease-related symptoms. These measures have demonstrated evidence for reliability and validity (Kalichman, Rompa, & Cage, 2000a). Group experience survey. Participants completed group experience measures at the end of the intervention. Seven items assessed perceptions of group environment; for example, “There was a feeling of togetherness in the group” and “The group had a positive spirit” (␣ ⫽ .93). Three items assessed perceptions of the group facilitators; for example, “The group leaders cared about people like me” and “I felt that I could trust the group leaders” (␣ ⫽ .85). Participants responded to items on 4-point scales (1 ⫽ strongly disagree to 4 ⫽ strongly agree), with scores representing the mean response ranging from 1 to 4. Self-efficacy for information seeking. Participants completed four items assessing beliefs that they could effectively perform specific information-related behaviors, such as finding information about HIV treatments, evaluating the accuracy of health information, and using the Internet to find health information. They responded to items on scales ranging from 0 (cannot do at all) to 10 (certain I can do), with scores representing mean responses ranging from 0 to 10 (alphas ranged from .77 to .83 across assessment points). Health information evaluation skills. Health information Web pages were obtained directly from the Web for use as stimulus materials for the following measures. The Web sites were downloaded in August 2001 and extensively tested in pilot studies (Benotsch et al., 2004; Kalichman et al., 2006). We selected one Web page that described widely accepted HIV/AIDS treatment guidelines: the Journal of the American Medical Association (JAMA) patient page on drug treatment options for HIV, posted on the www.medem.com Web site. We selected a second Web page that made scientifically unsupported claims of a successful treatment or cure for AIDS from goat’s blood serum (http://www.quantumbalancing.com/AIDS_CURE .htm). Participants rated the two Web pages on five dimensions of Web site quality:accuracy, amount of detail, trustworthiness– credibility, relevance, and usefulness (Kim et al., 1999), using 10-point scales ranging from 1 (not at all) to 10 (very). Participants made all ratings immediately after they read the respective Web pages. We computed perceived Web site quality rating index scores by taking the arithmetic means of the five ratings for each Web page. Scores for the JAMA and AIDS Cure Web pages were both internally consistent (baseline ␣s ⫽ .80 and .92; follow-up ␣s ⫽ .90 and .95, respectively). We also calculated the difference between quality ratings for the two Web pages (JAMA ⫺ AIDS Cure) at the follow-up
INTERVENTION TO IMPROVE INTERNET USE assessment. This difference score provides a marker for discrimination between the two Web sites, with higher scores indicating greater quality ascribed to the JAMA Web page relative to the AIDS Cure Web page. Internet use. Participants indicated the number of times they had used the Internet in the previous 3 months. We also asked participants the number of times they had used the Internet outside of the CTAC over the past week in assessments administered at the end of Intervention Sessions 2, 4, and 6. Participants reported the number of times they had used the Internet for any purpose and to search for health-related information and clinical trials over the previous 3 months. We also asked participants how many times they had used e-mail and the number of times they had talked to their physician about health information found on the Internet during that time. Participants were instructed to think back over the previous 3 months using important events as markers to increase recall accuracy. Responses to the Internet use measures were made with numerical values representing frequencies of acts on open-ended response formats to reduce arbitrary anchor biases (Catania, Gibson, Chitwood, & Coates, 1990). Information-seeking coping. To assess information-seeking coping, we adapted a measure reported by Miller, Brody, and Summerton (1988). This scale examines reactions to changes in health status presented in a vignette depicting a situation in which a person’s viral load has increased and a physician recommends changing antiretroviral medication regimens. The scenario reads as follows: Vividly imagine that you have gone to your doctor. Your doctor tells you that the results of your viral load test shows that your viral load has gone up and he wants to start you right away on a new anti-HIV medication. The three information-seeking items asked, “How likely would you be to ask your doctor questions about treatment?” “How likely would you be to try to find out as much information as possible?” and “How likely would you be to ask friends about medications?” Responses were recorded on 10-point scales of likelihood to perform each act, ranging from 0 (not at all) to 9 (very much), with mean scores ranging from 0 to 9 (alphas ranged from .76 to .88 across assessments). Ways of coping. On a measure drawn from the Ways of Coping Inventory (Lazarus & Folkman, 1984), participants responded to 17 items that represented problem-focused, information coping, and social coping behaviors in response to a specific stressor. They responded to coping items on 4-point scales ranging from 0 (not at all) to 3 (most of the time). Participants were instructed to (a) think about situations that had caused them recent stress, (b) indicate the situation that had caused them the greatest stress, and (c) indicate how much they used each coping strategy. Seven items represented problem-focused coping; for example, “I confronted the situation and fought for the help that I needed” and “I knew what had to be done and worked harder at it” (alphas ranged from .84 to .90 over assessments). The Information Coping scale consisted of five items; for example, “I talked with someone to find out more information” and “I talked with my doctor about the problem“ (alphas ranged from .71 to .73 across assessments). Finally, the Social Coping scale consisted of five items; for example, “I talked with someone who could help” and “I asked a friend or relative for advice” (alphas ranged from .61 to .71 over assessments). Scores represented mean responses ranging from 0 to 3, and the three coping scales were moderately correlated (correlations ranged from .52 to .59). Social support. The Social Support Questionnaire consists of 15 items that assess perceived social support (Brock, Sarason, Sarason, & Pierce, 1996). Items include availability of support and validation of support, such as, “There are several people that I trust to help me solve problems” and “I feel a strong emotional bond with at least one other person.” Participants responded to these items on 4-point scales ranging from 1 (definitely true) to 4 (definitely false); responses were summed to a score with a range of 15 to 60 (alphas ranged from .84 to .89 over assessment points).
549
Affective depression. The Centers for Epidemiological Studies– Depression Scale (CES-D) is a 20-item scale that assesses symptoms of depression over the previous 7 days, with scores ranging from 0 (no days) to 3 (5–7 days; Radloff & Locke, 1986). Because the somatic depression items on the CES-D overlap with HIV-related symptoms (Kalichman, Rompa, & Cage, 2000b), we scored six affective symptoms of depression items to avoid overlap with HIV disease-related symptoms (CES-D items were “I felt depressed,” “I thought my life had been a failure,” “I felt fearful,” “I felt lonely,” “I had crying spells,” and “I felt that people disliked me”). Scores ranged from 0 to 18 (alphas ranged from .81 to .82 across assessments).
Statistical Procedures and Data Analyses Prior to conducting the main study outcome analyses, we performed a series of preliminary analyses. First, we inspected all of the outcome variables for skewed distributions. We transformed variables that were significantly skewed using the formula log10 (x ⫹ 1), as recommended by Winer (1971), with nontransformed observed values presented in the tables. To test for differential attrition across conditions, we conducted a 2 (attrition: lost vs. retained) ⫻ 2 (condition: Internet skills intervention vs. health information control) contingency table chi-square test. We also conducted attrition bias analyses, following procedures described by Jurs and Glass (1971), in which we tested differences on baseline measures using 2 (attrition) ⫻ 2 (condition) analyses of variance. We also examined differences between conditions for perceptions of the group environment and group facilitators, using independent t tests. To test the study hypotheses, we conducted 2 (condition) ⫻ 4 (repeated assessments) mixed model analyses. We examined analyses for the information evaluation skills using a 2 (condition) ⫻ 2 (repeated assessments: baseline and 3-month follow-up) mixed model. For each analysis, we examined the main effects of intervention condition and assessment point as well as the interaction between intervention conditions and assessment point (time). We conducted planned comparisons only on variables that we found to be significant in the overall mixed models. For all analyses, we used an intent-to-treat approach by following participants at all assessment points. Missing values resulted from attrition and were estimated with a linear regression procedure for multiple imputations. All analyses controlled for participant gender because of gender-specific uses of the Internet. Number of group sessions attended was also controlled. Group assignment within conditions was also included in the analyses to control for random effects of group composition. Tests for differences between conditions at each time point on Internet use, coping, social support, and affective depression outcomes were conducted only when the Intervention Condition ⫻ Time interactions were significant. Eta-square is reported as an index of effect size.
Results Group Attendance, Attrition, and Group Experience A total of 448 participants who used the Internet fewer than three times in the previous month completed baseline assessments and were randomly assigned to one of two intervention conditions (see Figure 1). A total of 98 participants dropped out of the intervention conditions—59 (27%) from the Internet skills condition, compared with 39 (17%) of the participants in the health information support condition, 2(1, N ⫽ 448) ⫽ 6.9, p ⬍ .01. Participant retention at the 3-month, 6-month, and 9-month follow-up assessments was 343 (76%), 330 (74%), and 325 (73%), respectively. Thus, although dropout rates from the interventions differed between conditions, there were no differences
KALICHMAN ET AL.
550
between conditions in follow-up rates at any of the follow-up assessments. Participants in the Internet skills training groups attended an average of 6.0 (75%) of the 8 group sessions, compared with an average attendance of 6.5 (81%) sessions for the control group, t(446) ⫽ 2.2, p ⬍ .05. Analyses showed that the two conditions did not differ on gender, race, age, education, literacy scores, income, years since testing HIV positive, and HIV risk history, indicating that the randomization procedure appeared to achieve equal groups (see Table 1). Groups also did not differ in baseline use of the Internet (see Table 2); baseline Internet information quality ratings (see Table 2); or baseline coping, social support, or affective depression scores (see Table 3). There were no effects of attrition on the baseline measures, which indicates that the participants who dropped from groups or were lost to follow-up did not differ from those retained. There were also no Intervention Condition ⫻ Attrition interactions on baseline measures, which shows that the differential dropout from the intervention could not be accounted for by participant characteristics. Participants in the Internet skills group (M ⫽ 3.5, SD ⫽ 0.5) and control group (M ⫽ 3.5, SD ⫽ 0.4) did not differ in their sense of group cohesiveness, t(348) ⫽ 1.6, ns. The Internet skills group (M ⫽ 3.5, SD ⫽ 0.5) and the control group (M ⫽ 3.6, SD ⫽ 0.4) also did not differ on perceptions of group facilitators, t(348) ⫽ 1.1, ns.
Internet Access, Self-Efficacy, Skills, and Use Internet access and CTAC use. Participants showed a steady increase in Internet access outside of the CTAC, as assessed at the end of the group sessions over the intervention period, 2(2, N ⫽ 348) ⫽ 47.6, p ⬍ .001. At the second intervention session, 36
(23%) participants in the Internet skills training group indicated that they had accessed the Internet outside of the CTAC, compared with 21 (11%) participants in the comparison group, 2(1, N ⫽ 347) ⫽ 8.3, p ⬍ .01. At the fourth session, 47 (36%) participants in the Internet group and 34 (24%) participants in the comparison group were accessing the Internet, 2(1, N ⫽ 347) ⫽ 4.2, p ⬍ .05. By the sixth session, 53 (43%) members of the Internet skills group and 32 (23%) members of the comparison group were using the Internet outside of the CTAC, 2(1, N ⫽ 347) ⫽ 13.1, p ⬍ .01. Coding the CTAC attendance logs showed that 63 (29%) Internet skills training and 56 (24%) control group members had used the CTAC, a nonsignificant difference. Among CTAC users, the average number of times that they visited the CTAC for the Internet skills group was 4.0 (SD ⫽ 5.6), and for the health support group, the average number of CTAC visits was 4.4, t(117) ⫽ 0.5, ns. Conditions also did not differ in the amount of time participants spent using the CTAC (Internet skills group: M ⫽ 34.7 min, SD ⫽ 32.7; comparison condition: M ⫽ 29.9 min, SD ⫽ 32.4), t(135) ⫽ 0.6, ns. The Internet skills and control conditions therefore demonstrated equal access to the Internet via the CTAC. Self-efficacy for health information use. Results showed a significant interaction between assessment time and intervention condition on self-efficacy for health information use (see Table 2). Planned comparisons showed that the Internet skills intervention demonstrated greater self-efficacy at each follow-up. Health information evaluation skills. Analyses showed that the Intervention Condition ⫻ Time interaction for the JAMA Web page quality ratings was not significant (see Table 2). In contrast, there was an Intervention Condition ⫻ Assessment Time interaction for the AIDS Cure Web site quality ratings; Internet skills group participants rated the AIDS Cure information as having
Table 1 Demographic and Health Characteristics of Participants Randomly Assigned to the Internet Skills-Building and Health Information Support Groups at Baseline Internet skills-building group (n ⫽ 217) Characteristic Age Years of education % correct TOFHLA score Years tested HIV positive
Male Female African American White Other race/ethnicity 12 years or more education Income under $10,000 Unemployed/disabled Injection drug use history Men with a history of having sex with men Note.
Health information support group (n ⫽ 231)
M
SD
M
SD
t(df ⫽ 446)
42.3 12.4 85.5 10.8
7.3 1.9 15.6 5.8
42.6 12.1 83.3 10.5
6.7 1.8 20.3 5.7
0.4 1.4 1.3 0.5
n
%
n
%
2(N ⫽ 448)
df
155 63 196 16 6 165 171 188 43 100
71 29 90 7 3 76 80 88 20 48
177 53 205 20 4 167 183 214 44 108
77 23 90 8 2 73 81 92 19 47
2.1
1
1.3 0.7 0.7 2.3 0.1 0.1
2 3 3 1 1 1
TOFHLA ⫽ Test of Functional Health Literacy for Adults.
INTERVENTION TO IMPROVE INTERNET USE
551
Table 2 Self-Efficacy, Information Quality Evaluation Scores, and Internet Use During the Previous 3 Months at Baseline and Follow-Ups
Variable Self-efficacy Baseline 3 months 6 months 9 months Quality evaluation skills for the JAMA Web page Baseline 3 months Quality evaluation skills for the AIDS Cure Web page Baseline 3 months Difference score for JAMA and AIDS Cure ratings at 3 monthsb Total Internet use Baseline 3 months 6 months 9 months Searched for health information Baseline 3 months 6 months 9 months Searched for clinical trials Baseline 3 months 6 months 9 months Used e-mail Baseline 3 months 6 months 9 months Brought information to provider Baseline 3 months 6 months 9 months
Internet skills-building group
Health information support group
M
SD
M
SD
5.8 6.6a 6.6a 6.3a
2.6 2.4 2.5 2.6
5.4 5.3 5.5 5.2
2.5 2.7 2.5 2.4
8.6 7.8
1.4 1.9
8.6 8.0
7.6 6.2
2.4 2.8
1.6
Time ⫻ Condition
Time
2
F(3, 441)
2
0.5
.004
3.2*
.024
1.2 1.7
1.3
.005
1.9
.005
7.6 7.0
2.3 2.7
0.3
.001
7.9**
.027
2.9
1.0
2.4
3.9*
.013
1.2 10.1 10.0a 9.6
3.6 21.0 24.7 30.7
1.3 6.3 5.2 6.1
3.6 34.8 15.4 23.1
3.2*
.023
2.9*
.021
0.3 3.1a 2.7a 2.1a
1.0 6.5 5.8 4.9
0.2 0.9 1.1 0.6
0.8 3.0 3.0 2.3
6.6**
.046
10.7**
.073
0.1 1.2a 1.5a 1.0a
0.8 3.8 8.0 4.3
0.1 0.3 0.3 0.4
0.7 1.8 1.6 1.7
3.2*
.023
3.6*
.026
0.3 4.9a 5.4a 5.3a
1.4 14.2 17.9 17.3
0.4 2.4 2.2 2.7
2.3 12.1 8.1 11.2
2.7*
.019
3.8**
.027
0.1 0.5a 1.0a 0.8a
0.5 1.2 6.5 3.5
0.1 0.1 0.3 0.1
0.6 0.8 1.1 1.0
1.9
.014
6.1**
.043
F(3, 441)
Note. All F ratios are adjusted for participant gender, group session attendance, and group effects. Time ⫽ main effect for assessment point; Time ⫻ Condition ⫽ Assessment Point ⫻ Intervention interaction; JAMA ⫽ Journal of the American Medical Association. a Significant differences between groups, p ⬍ .05. b F and 2 for difference between conditions. * p ⬍ .05. ** p ⬍ .01.
lower quality than the comparison intervention over time. Internet skills group participants also demonstrated significantly greater discrimination between the JAMA and AIDS Cure Web pages at the 3-month follow-up (see Table 2). Internet use. There was a significant interaction between intervention conditions and assessment point for the amount of time participants used the Internet (see Table 2). Planned comparisons showed that the Internet skills group demonstrated greater Internet use than the control condition at the 6-month follow-up. As shown in Table 2, there was a significant interaction between intervention condition and assessment time for using the Internet for health, clinical trials, and e-mail, and the interaction effect on bringing
information to health care providers was also significant. For each variable, the Internet skills-building intervention was significantly greater than the health information support group condition at all three follow-ups.
Coping, Social Support, and Depression Information-seeking coping and ways of coping. Analyses showed that, in response to the health care visit scenario, there was a main effect on information-seeking coping for assessment point, and this effect was qualified by an interaction between intervention condition and assessment point (see Table 3). The Internet skills
KALICHMAN ET AL.
552
Table 3 Information-Seeking Coping, Ways of Coping, Social Support, and Affective Depression for Internet Skills-Building and Health Information Groups Internet skills-building group Scale Information-seeking coping Baseline 3 months 6 months 9 months Ways of Coping Inventory Problem-Focused Coping Baseline 3 months 6 months 9 months Information Coping Baseline 3 months 6 months 9 months Social Coping Baseline 3 months 6 months 9 months Social Support Questionnaire Baseline 3 months 6 months 9 months Affective depression Baseline 3 months 6 months 9 months
Health information support group
Time ⫻ Condition
Time
F(3, 441)
2
1.7
.013
2.9*
.020
0.7 0.8 0.7 0.7
4.6**
.033
1.0
.008
1.6 1.6 1.6 1.6
0.7 0.7 0.6 0.7
3.9**
.028
3.1*
.022
0.8 0.7 0.7 0.8
1.7 1.8 1.9 1.8
0.8 0.8 0.7 0.7
1.2
.009
1.8
.013
43.8 45.0a 45.0a 44.9a
8.1 8.0 8.5 8.2
42.6 43.2 41.8 42.8
8.5 7.8 8.7 8.4
1.8
.013
3.6**
.024
5.4 4.8 4.6a 4.8
4.7 4.6 3.9 4.2
5.0 5.1 5.0 4.9
3.9 4.0 3.8 4.1
1.1
.008
2.6**
.018
M
SD
M
SD
7.8 7.7a 7.6a 7.2
1.4 1.5 1.6 1.6
7.7 7.4 7.1 7.1
1.6 1.9 1.9 1.8
1.8 2.0 2.0 1.9
0.7 0.7 0.7 0.8
1.9 1.8 1.9 1.8
1.6 1.9a 1.8a 1.8a
0.6 0.7 0.7 0.7
1.8 2.0 2.0 1.9
F(3, 441)
2
Note. All F ratios are adjusted for participant gender, group session attendance, and group effects. Time ⫽ main effect for assessment point; Time ⫻ Condition ⫽ Assessment Point ⫻ Intervention interaction. a Significant differences between groups, p ⬍ .05. * p ⬍ .05. ** p ⬍ .01.
group differed from the control condition at 3-month and 6-month follow-ups but not at the 9-month follow-up. For the Ways of Coping Inventory scales, we found a significant increase in problem-focused and information coping over time, which was qualified by a significant Condition ⫻ Time interaction for information coping; the Internet skills intervention demonstrated significantly greater information coping than the control condition at all three follow-up assessments. There were no effects of time or intervention condition on the Social Coping scale. Social support and affective depression. Analyses showed a significant interaction between assessment time and intervention condition on social support (see Table 3). Planned comparisons showed that the Internet skills-building group reported significantly greater social support at all three follow-up assessments than the health information support group. Results showed a significant Intervention Condition ⫻ Assessment interaction on affective depression scores. Participants in the Internet skills intervention reported fewer symptoms of affec-
tive depression over time than did the comparison group, with significant differences between conditions occurring at the 6-month follow-up (see Table 3).
Discussion The current study supports the efficacy of a social– cognitive– behavioral intervention to improve health information seeking and information consumer skills among people living with HIV/AIDS. The Internet skills-building intervention was significantly more likely to increase Internet use outside the CTAC as well as searching for health information and social support functions online compared with the control condition. Increased use of the Internet for health and support functions was sustained over the 9-month observation period. Participants in the Internet skills-building group improved health information evaluation skills and were more likely to bring health information found online to their health care providers. Both outcomes could potentially reduce vulnerability to misinformation and fraudulent claims found online.
INTERVENTION TO IMPROVE INTERNET USE
Consistent with the goals of our intervention, participants in the Internet skills intervention demonstrated increased informationseeking coping. Contrary to our hypotheses, we did not observe generalization of information coping skills to problem-focused and social coping. The coping outcomes therefore appear quite specific to the intervention content. Confirming the study hypotheses, we did observe significant increases in social support among individuals in the Internet skills group that were sustained over 9 months and less affective depression at the 6-month follow-up. Our conceptual model suggests that these effects are the product of the intervention and the ongoing effects of health and social support use of the Internet. These findings suggest that assisting people living with HIV/AIDS in accessing and effectively using the Internet can impact on at least some aspects of emotional wellbeing. These results are also consistent with the associations of health-related Internet use, ways of coping, and social support observed in correlation studies (Kalichman et al., 2005). The results of this trial complement research that has tested computerized information systems for people with chronic illness. Interventions, such as the Comprehensive Health Enhancement Support System, that provide health information and opportunities for online support have shown promising effects in improving the health and well-being of people with a variety of chronic conditions, including breast cancer, heart disease, prostate cancer, asthma, and HIV/AIDS (Gustafson et al., 2002). However, unlike computerized systems that contain selected information and closed communication networks that ensure quality, the Internet has no such assurances; people commonly encounter misinformation and fraudulent claims when searching for health information on the Internet. Building skills for conducting Internet searches and critically evaluating information obtained online should therefore be considered an essential part of any effort to increase Internet access for people with chronic medical conditions. We also observed differential dropout rates from the Internet skills intervention that could not be accounted for by participant characteristics or by a breakdown in randomization. Significantly more participants dropped out of the Internet skills intervention, and overall attendance was poorer for this intervention than for the control condition. The Internet skills-building intervention was therefore not of interest to everyone. Efforts to increase access to health information and empower people to use health information must provide alternatives that do not rely solely on computers and the Internet. Patient education materials, health education counseling, and time spent with health care professionals to build health information consumer skills cannot be replaced for everyone by increased Internet access.
Limitations The current intervention trial was limited by its use of a convenience sample of people living with HIV/AIDS. The participants in this study cannot be considered representative of people living with HIV/AIDS who are not using the Internet. Our participants were also more likely to be older and represented more advanced stages of HIV disease. We relied on self-report measures for assessing health status, including CD4 cell counts and viral load, rather than using biological samples or chart abstracted data. We also assessed Internet use by self-report, without corroborating search functions through Web site monitoring. We had considered
553
including log-in portals and other technology to monitor Internet use and Web site content access but decided against these measures to protect participants’ privacy rights. This study also did not provide participants with computers or other means of Internet access at home, which limits the generalizability of findings to home use. The current study was also neither designed nor powered to empirically test the conceptual model that suggests that Internet use for health and social support accounts for improvements in social and emotional well-being. Despite these limitations, the current findings have implications for improving health information access for people with chronic illnesses.
Implications for Interventions Patients with chronic medical conditions can use the Internet to improve their health and psychological adjustment. Efforts to increase Internet access for people with chronic health conditions must attend to the inevitable exposure to misinformation and fraud that people encounter when searching for health information on the Internet. Increasing community Internet access by establishing CTACs in health centers, such as AIDS service organizations, dialysis clinics, supportive agencies, and rehabilitation centers, may improve equal opportunities to receive what can often be life-saving health information. However, facilities that increase Internet access should also implement interventions for their clients that include critical thinking and information evaluation skills. Patients should also be encouraged to put information into action by bringing it to health care providers and integrating it into their health care. Creating opportunities for equal access to health information and equipping chronically ill Internet users and their families with critical thinking and information consumer skills should be a priority for future interventions.
References AIDS cure Web site. (2000). Retrieved August 2001 from http://www .quantumbalancing.com/AIDS_CURE.htm American Medical Association. (2001). JAMA patient page on drug treatment options for HIV. Retrieved August 2001 from the Medem Network Web site: http://www.medem.com/medlb/article_detaillb.cfm?article_ID ⫽ZZZKBZN2NAC&sub_cat⫽279 Baker, L., Wagner, T., Singer, S., & Bundorf, M. (2003). Use of the Internet and E-mail for health care information: Results from a national survey. Journal of the American Medical Association, 289, 2400 –2406. Bandura, A. (1997). Self-efficacy: The exercise of control. New York: Freeman. Benotsch, E. G., Kalichman, S. C., & Weinhardt, L. (2004). HIV/AIDS patients’ evaluation of health information on the Internet. Journal of Consulting and Clinical Psychology, 72, 1004 –1011. Berland, G. K., Elliot, M. N., Morales, L. S., Algazy, J. I., Kravitz, R. L., Broder, M. S., et al. (2001). Health information on the Internet: Accessibility, quality, and readability in English and Spanish. Journal of the American Medical Association, 285, 2612–2621. Bolt, D., & Crawford, R. (2000). Digital divide: Computers and our children’s future. New York: TV Books. Brock, D., Sarason, I., Sarason, B., & Pierce, G. (1996). Simultaneous assessment of perceived global and relationship-specific support. Journal of Social & Personal Relationships, 13, 143–152. Buck, B. A. (1991, October). Support groups for hospitalized AIDS patients. AIDS Patient Care, 3, 255–258. Catania, J. A., Gibson, D., Chitwood, D., & Coates, T. J. (1990). Meth-
554
KALICHMAN ET AL.
odological problems in AIDS behavioral research: Influences on measurement error and participation bias in studies of sexual behavior. Psychological Bulletin, 108, 339 –362. Devins, G., & Binik, Y. M. (1996). Facilitating coping with chronic physical illness. In M. Zeidner & N. Endler (Eds.), Handbook of coping: Theory, research, applications (pp. 640 – 696). New York: Wiley. Dutta-Bergman, M. (2004). Health attitudes, health cognitions, and health behaviors among Internet health information seekers: Population-based survey. Journal of Medical Internet Research, 6, e15. Eysenbach, G., & Diepgen, S. (1998). Towards quality management of medical information on the internet: Evaluation, labeling, and filtering of information. British Medical Journal, 317, 1496 –1502. Fox, S., & Fallows, D. (2003). Internet health resources. Retrieved August 2004 from the Pew Internet & American Life Project Web site: http:// www.pewinternet.org/pdfs/PIP_Health_Report_July_2003.pdf Gustafson, D. H., Hawkins, R. P., & Boberg, E. W. (2002). CHESS: 10 years of research and development in consumer health informatics for broad populations, including the underserved. International Journal of Medical Informatics, 65(3), 169 –177. Jurs, S. G., & Glass, G. (1971). The effect of experimental mortality on the internal and external validity of the randomized comparative experiment. Journal of Experimental Education, 40, 62– 66. Kalichman, S. C., Benotsch, E., Weinhardt, L., Austin, J., Luke, W., & Cherry, C. (2003). Health-related Internet use, coping, social support, and health indicators in people living with HIV-AIDS: Preliminary results from a community-survey. Health Psychology, 22, 111–116. Kalichman, S. C., Cain, D., Cherry, C., Pope, H., Eaton, L., & Kalichman, M. (2005). Internet use among people living with HIV/AIDS: Coping and health-related correlates. AIDS Patient Care and STDs, 19, 21–30. Kalichman, S. C., Cherry, C., Cain, D., Weinhardt, L., Benotsch, E., Pope, H., & Kalichman, M. (2006). Health information on the Internet and people living with HIV/AIDS: Information evaluation and coping styles. Health Psychology, 25, 205–210. Kalichman, S. C., Rompa, D., & Cage, M. (2000a). Distinguishing between overlapping somatic symptoms of depression and HIV disease in people living with HIV-AIDS. Journal of Nervous and Mental Diseases, 188, 662– 670. Kalichman, S. C., Rompa, D., & Cage, M. (2000b). Validity of selfreported CD4 lymphocyte count and viral load test results in people living with HIV-AIDS. International Journal of STD and AIDS, 11, 579 –585. Kalichman, S. C., Rompa, D., Cage, M., DiFonzo, K., Simpson, D., Austin, J., et al. (2001). Effectiveness of an intervention to reduce HIV transmission risks in HIV positive persons. American Journal of Preventive Medicine, 21, 84 –92.
Kalichman, S. C., Weinhardt, L., & Benotsch, E. (2002). Closing the digital divide in HIV-AIDS care: Development of a theory-based intervention to increase Internet access. AIDS Care, 14, 523–537. Kalichman, S. C., Weinhardt, L., Benotsch, E., Rompa, D., DiFonzo, K., Luke, W., et al. (2002). Internet access and Internet use for health information among people living with HIV-AIDS. Patient Education and Counseling, 46, 109 –116. Kim, P., Eng, T. R., Deering, M. J., & Maxfield, A. (1999). Published criteria for evaluating health related Web sites: Review. British Medical Journal, 318, 647– 649. Kunst, H., Groot, D., Latthe, P., Latthe, M., & Khan, K. (2002). Accuracy of information on apparently credible Websites: Survey of five common health topics. British Medical Journal, 324, 581–582. Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York: Springer. Miller, S. M., Brody, D. S., & Summerton, J. (1988). Styles of coping with threat: Implications for health. Journal of Personality and Social Psychology, 54, 142–148. Parker, R. M., Baker, D. W., Williams, M. V., & Nurss, J. R. (1995). The test of functional health literacy in adults: A new instrument for measuring patients’ literacy skills. Journal of General Internal Medicine, 10, 537–541. Price, J., & Entin, S. (1999). The complete idiot’s guide to online health and fitness. New York: Alpha Books. Radloff, L. S., & Locke, B. Z. (1986). The community mental health assessment survey and CES-D Scale. In M. M. Weissman, J. K. Meyers, & C. E. Ross (Eds.), Community surveys of psychiatric disorders (pp. 177–187). New Brunswick, NJ: Rutgers University Press. Schloman, B. F. (2004). The digital divide: How wide and how deep? Online Journal of Issues in Nursing, 9, e7. Retrieved May 2005 from http:///www.nursingworld.org/ojin/ Wagner, T., Baker, L., Bundorf, M., & Singer, S. (2004). Use of the Internet for health information by the chronically ill. Preventing Chronic Illness, 1, 1–13. Walji, M., Sagaram, A., Sagaram, D., Meric-Bernstam, F., Johnson, C., Mirza, N., & Bernstam, E. (2004). Efficacy of quality criteria to identify potentially harmful information: A cross-sectional survey of complementary and alternative medicine Web sites. Journal of Medical Internet Resources, 29, e21. Winer, B. J. (1971). Statistical principles in experimental design. New York: McGraw-Hill.
Received July 7, 2005 Revision received February 2, 2006 Accepted February 7, 2006 䡲