Am J Physiol Regul Integr Comp Physiol 302: R876 –R885, 2012. First published December 28, 2011; doi:10.1152/ajpregu.00330.2011.
Medial prefrontal cortex endocannabinoid system modulates baroreflex activity through CB1 receptors Nilson C. Ferreira-Junior, Alessandra G. Fedoce, Fernando H. F. Alves, Fernando M. A. Corrêa, and Leonardo B. M. Resstel Department of Pharmacology, School of Medicine of Ribeirão Preto, University of São Paulo, Ribeirão Preto, São Paulo, Brazil Submitted 22 June 2011; accepted in final form 23 December 2011
Ferreira-Junior NC, Fedoce AG, Alves FHF, Corrêa FMA, Resstel LBM. Medial prefrontal cortex endocannabinoid system modulates baroreflex activity through CB1 receptors. Am J Physiol Regul Integr Comp Physiol 302: R876 –R885, 2012. First published December 28, 2011; doi:10.1152/ajpregu.00330.2011.—Neural reflex mechanisms, such as the baroreflex, are involved in the regulation of cardiovascular system activity. Previous results from our group (Resstel LB, Correa FM. Medial prefrontal cortex NMDA receptors and nitric oxide modulate the parasympathetic component of the baroreflex. Eur J Neurosci 23: 481– 488, 2006) have shown that glutamatergic synapses in the ventral portion of the medial prefrontal cortex (vMPFC) modulate baroreflex activity. Moreover, glutamatergic neurotransmission in the vMPFC can be modulated by the endocannabinoids system (eCBs), particularly the endocannabinoid anandamide, through presynaptic CB1 receptor activation. Therefore, in the present study, we investigated eCBs receptors that are present in the vMPFC, and more specifically whether CB1 receptors modulate baroreflex activity. We found that bilateral microinjection of the CB1 receptor antagonist AM251 (100 or 300 pmol/200 nl) into the vMPFC increased baroreflex activity in unanesthetized rats. Moreover, bilateral microinjection of either the anandamide transporter inhibitor AM404 (100 pmol/200 nl) or the inhibitor of the enzyme fatty acid amide hydrolase that degrades anandamide, URB597 (100 pmol/200 nl), into the MPFC decreased baroreflex activity. Finally, pretreatment of the vMPFC with an ineffective dose of AM251 (10 pmol/200 nl) was able to block baroreflex effects of both AM404 and URB597. Taken together, our results support the view that the eCBs in the vMPFC is involved in the modulation of baroreflex activity through the activation of CB1 receptors, which modulate local glutamate release. anandamide; autonomic system; cannabinoids; infralimbic cortex; prelimbic cortex
(MPFC) is a limbic structure that is involved in the modulation of autonomic responses exerting influence on the cardiovascular system in rats (44, 57). The ventral portion of the MPFC (vMPFC), which is compounded by the infralimbic (IL), prelimbic (PL), and dorsal peduncular cortexes (41, 61), is involved in the modulation of baroreflex activity (49, 56). Glutamatergic terminals and ionotropic glutamate receptors were reported in the vMPFC of rats (18, 36). Furthermore, a previous study from our group showed that local injection of L-glutamate into the vMPFC evokes an activation of both sympathetic and parasympathetic activities on the heart of unanesthetized rats (48). Moreover, the glutaTHE MEDIAL PREFRONTAL CORTEX
Address for reprint requests and other correspondence: L. B. M. Resstel, Dept. of Pharmacology, School of Medicine of Ribeirão Preto, USP, Bandeirantes Ave. 3900, 14049-900, Ribeirão Preto, São Paulo, Brazil (e-mail:
[email protected]). R876
matergic system present in the vMPFC is involved in baroreflex modulation (45). In the central nervous system (CNS), the endocannabinoid anandamide is synthesized on demand in postsynaptic neurons, after calcium influx increase (13, 42). Anandamide immediately diffuses to the synaptic cleft, activating CB1 cannabinoid receptors, which are located in presynaptic terminals (59). The action of anandamide is limited by its reuptake through a putative anandamide transporter, being subsequently metabolized by the intracellular enzyme fatty acid amide hydrolase (FAAH) that is located in postsynaptic neurons (14, 43). These two mechanisms, which cooperate to attenuate anandamide signaling in the CNS, can be pharmacologically inhibited by drugs such as AM404 (anandamide re-uptake inhibitor) and URB597 (FAAH inhibitor). The CB1 cannabinoid receptor is one of the most abundant G protein-coupled receptors in the brain and is expressed at high levels in the hippocampus, cortex, and basal ganglia (22, 23, 54). Moreover, CB1 receptors are predominantly localized presynaptically, where they modulate neurotransmitter release (25, 58, 60). Several studies have shown that CNS glutamatergic neurotransmission can be modulated by the endocannabinoid system (eCBs) through CB1 receptors (5, 15, 20). The presence of CB1 receptors in the vMPFC of rats has been demonstrated (19, 22, 23, 34), and their inhibition by a CB1 antagonist increases the release of glutamate (5), thus suggesting that the eCBs, through CB1 receptors, inhibits glutamatergic synaptic transmission in the vMPFC. Thus, if glutamatergic neurotransmission is involved in vMPFC-related modulation of the baroreflex, and CB1 receptors can modulate the release of glutamate in the vMPFC, there is also the possibility that vMPFC CB1 receptors could modulate baroreflex activity. Therefore, in the present study, we evaluated the involvement of the eCBs present in the vMPFC in the modulation of cardiac baroreflex responses to blood pressure changes. MATERIALS AND METHODS
Ethical approval and animals. Experimental procedures were carried out following protocols approved by the Ethical Review Committee of the School of Medicine of Ribeirão Preto (protocol no. 128/2010), which comply with the “Guiding Principles for Research Involving Animals and Human Beings” of the American Physiological Society. Male Wistar rats weighing 230 –270 g were used in the present experiments. They were kept under a 12:12-h light-dark cycle (lights on between 6:00 AM and 6:00 PM) and had free access to water and standard rat food. Animal preparation. Four days before the experiment, rats were anesthetized with tribromoethanol (250 mg/kg ip, Sigma, St. Louis, MO). After a local anesthesia with 2% lidocaine, the skull was
0363-6119/12 Copyright © 2012 the American Physiological Society
http://www.ajpregu.org
vMPFC eCBs AND BAROREFLEX
surgically exposed, and stainless steel guide cannulas (26G) were bilaterally implanted into the vMPFC using a stereotaxic apparatus (Stoelting, Wood Dale, IL). Stereotaxic coordinates for cannula implantation in the vMPFC were selected from the rat brain atlas of Paxinos and Watson (41) and were: anterior-posterior ⫽ ⫹3.3 mm, lateral ⫽ 2.7 mm from the medial suture, and ventral ⫽ ⫺3.2 mm from the skull, with a lateral inclination of 24°. Cannulas were fixed to the skull with dental cement and one metal screw. After the surgery, animals were treated with a polyantibiotic preparation of streptomycins and penicillins (intramuscular, Pentabiotico, Fort Dodge, Campinas, São Paulo, Brazil) to prevent infection and also with the nonsteroidal anti-inflammatory drug flunixine meglumine (subcutaneously, Banamine, Schering Plough, Cotia, São Paulo, Brazil) for postoperative analgesia. One day before the experiment, rats were again anesthetized with tribromoethanol (250 mg/kg ip) and a catheter (a 4-cm segment of PE-10 that was heat-bound to a 13-cm segment of PE-50, Clay Adams, Parsippany, NJ) was inserted into the abdominal aorta through the femoral artery, for blood pressure recording. A second catheter was implanted into the femoral vein for the infusion of vasoactive drugs to evoke arterial blood pressure changes. Both catheters were tunneled under the skin and exteriorized on the animal’s dorsum. After the surgery, the treatment with anti-inflammatory drugs was repeated. Measurement of cardiovascular responses. The pulsatile arterial pressure of freely moving animals was recorded using an HP-7754A preamplifier (Hewlett Packard, Palo Alto, CA) and an acquisition board (Biopac M-100, Goleta, CA) connected to a computer. Mean arterial pressure (MAP) and heart rate (HR) values were derived from pulsatile recordings and processed online. Drug injection. The needles (33G, Small Parts, Miami Lakes, FL) used for the microinjection of drugs into the vMPFC were 1 mm longer than the guide cannulas and were connected to a 1-l syringe (7002-H, Hamilton, Reno, NV) through a segment of PE-10 tubing. The needle was carefully inserted into the guide cannula, and drugs were injected in a final volume of 200 nl over a 5-s period. After a 30-s period, the needle was removed and inserted into the second guide cannula for the microinjection into the contralateral vMPFC. Baroreflex stimulation. The baroreflex was activated by an intravenous infusion of phenylephrine (50 g/kg; 0.34 ml/min) or sodium nitroprusside (SNP; 50 g/kg; 0.8 ml/min) using an infusion pump (KD Scientific, Holliston, MA). Either phenylephrine or SNP infusions lasted 50 – 60 s and caused blood pressure increase or decreases, respectively (4, 49). Method of baroreflex evaluation. Baroreflex curves were constructed matching MAP variations with HR responses. Paired values of MAP (⌬MAP) and HR (⌬HR) variations were plotted to generate sigmoid curves for each rat, which were used to determine the baroreflex activity (49). To analyze bradycardic and tachycardic responses separately, HR values matching 10, 20, 30, and 40 mmHg of MAP changes were calculated (3, 11). Values were plotted to create linear regression curves for each rat, and their slopes were compared with test possible changes in the baroreflex gain. Drugs. The following drugs were used: the anandamide transporter inhibitor 4-hydroxyphenylarachidonylamide (AM404; Tocris, Ellisville, MO) was dissolved in Tocrisolve TM 100 (a solvent that contains a 1:4 ratio of soya oil-water, emulsified with the block copolymer Pluronic F68), as recommended by the manufacturer. The CB1 receptor antagonist N-(piperidin-1-yl)-5-(4-iodophenyl)-1-(2,4dichlorophenyl)-4-methyl-1H-pyrazole-3-carboxamide (AM251; Tocris) was dissolved in 10% DMSO in saline (0.9% NaCl). The inhibitor of the enzyme that degrades anandamide, the enzyme FAAH, the 3=(aminocarbonyl)(1,1=-biphenyl)-3-yl-cyclohexylcarbamate (URB597; Cayman Chemical) was dissolved in 10% DMSO in saline (0.9% NaCl). Phenylephrine-HCl (Sigma) and SNP (Sigma) were dissolved in saline (0.9% NaCl). Tribromoethanol (Sigma) and urethane (Sigma) were dissolved in distilled water. Solutions were prepared
R877
immediately before use and were kept on ice and protected from the light during experimental sessions. Experimental protocols. All groups of animals used in our study received three sets of phenylephrine or SNP infusion to determine control values of baroreflex activity. In the sequence, the first group received a microinjection of 200 nl of 10% DMSO dissolved in saline (0.9% NaCl); the second group received a microinjection of 200 nl of AM251 [10, 100, or 300 pmol (30)]; the third group received a microinjection of 200 nl of AM404 [50 or 100 pmol (30)]; the fourth group received a microinjection of 200 nl of URB597 [100 pmol (31)]; the fifth group received bilateral microinjections of 200 nl of AM251 (10 pmol) and 5 min later AM404 (100 pmol) or URB597 (100 pmol). In all experimental groups, phenylephrine and SNP infusions were repeated 10 and 60 min after the microinjection of drugs. Histological procedure. At the end of experiments, rats were anesthetized with urethane (1.25 g/kg ip), and 200 nl of 1% Evan’s blue dye was bilaterally injected into the vMPFC as a marker of injection sites. The chest was surgically opened, the descending aorta occluded, the right atrium severed, and the brain was perfused through the left ventricle with 10% formalin. Brains were postfixed for 24 h at 4°C, and 40-m sections were cut using a cryostat (CM-1900, Leica, Wetzlar, Germany). The actual placement of the injection needle was verified in serial sections, according to the rat brain atlas of Paxinos and Watson (41). Data analysis. Baseline cardiovascular values, before and after pharmacological treatment of the vMPFC, were compared using the Student’s t-test. Values are shown as means ⫾ SE. The baroreflex was analyzed using sigmoid curves, which were characterized as four parameters: 1) P1 (beats/min) lower HR plateau and P2 (beats/min) upper HR plateau; 2) HR range (beats/min), difference between upper and lower plateau levels; 3) median blood pressure (BP50, mmHg), which is the MAP at 50% of the HR range; and 4) average gain (G; beats·min⫺1·mmHg⫺1), which is the average slope of the curves between ⫹1 and ⫺1 standard derivations from BP50 (21, 29). Significant differences among sigmoid curves or linear regression parameters were analyzed using one-way ANOVA followed by the Dunnett’s post hoc test. The slope of linear regression curves (⌬HR vs. ⌬MAP) before and 10 and 60 min after the microinjection of each treatment was determined, and results were analyzed to detect alterations in the cardiac baroreflex G, using one-way ANOVA followed by the Dunnett’s post hoc test. Results of statistical tests with P ⬍ 0.05 were considered significant. RESULTS
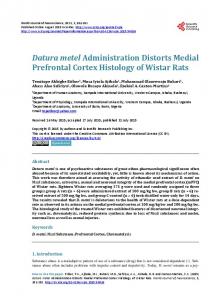
Figure 1 shows a representative photomicrograph of a vMPFC coronal section and diagrammatic representations with the microinjection sites of all experimental groups. The bilateral administration of 10% DMSO (vehicle) into the vMPFC (n ⫽ 7) did not affect basal levels of both MAP [before ⫽ 88.6 ⫾ 1.7 and after ⫽ 86.7 ⫾ 2.1 mmHg; t-test (t) ⫽ 1.0; P ⬎ 0.05] and HR (before ⫽ 381.1 ⫾ 19.3 and after ⫽ 377.3 ⫾ 17.9 beats/min; t ⫽ 1.0; P ⬎ 0.05). Furthermore, linear regression analysis indicated no difference between slopes of bradycardic (before ⫽ ⫺1.57 ⫾ 0.22 and after ⫽ ⫺1.53 ⫾ 0.19 beats·min⫺1·mmHg⫺1; t ⫽ 0.5; P ⬎ 0.05) and tachycardic (before ⫽ ⫺1.37 ⫾ 0.17 and after ⫽ ⫺1.48 ⫾ 0.20 beats·min⫺1·mmHg⫺1; t ⫽ 1.8; P ⬎ 0.05) responses of the baroreflex generated before and after vMPFC treatment with DMSO. Similar to the DMSO, the solvent of AM404, Tocrisolve TM 100, had no effect on the baroreflex activity. Bilateral administration of the CB1 receptor antagonist AM251 in the structures surrounding the vMPFC (n ⫽ 4) did
AJP-Regul Integr Comp Physiol • doi:10.1152/ajpregu.00330.2011 • www.ajpregu.org
R878
vMPFC eCBs AND BAROREFLEX
Fig. 1. Photomicrograph of a ventral portion of the medial prefrontal cortex (vMPFC) coronal section and diagrammatic representations with the microinjection sites of vehicle, AM251, AM404, and URB597 into (solid circles) and structures surrounding (open circles) the vMPFC, based on the rat brain atlas of Paxinos and Watson (41). Cg1, cingulated cortex, area 1; PL, prelimbic cortex; IL, infralimbic cortex; DP, dorsal peduncular cortex; CC, corpus callosum.
not affect the slopes of both bradycardic (before ⫽ ⫺2.21 ⫾ 0.15 and after ⫽ ⫺2.45 ⫾ 0.16 beats·min⫺1·mmHg⫺1; t ⫽ 1.1; P ⬎ 0.05) and tachycardic (before ⫽ ⫺2.27 ⫾ 0.28 and after ⫽ ⫺2.42 ⫾ 0.15 beats·min⫺1·mmHg⫺1; t ⫽ 0.4; P ⬎ 0.05) responses of the baroreflex. Bilateral injection of an inhibitor of an enzyme that degrades anandamide, URB597, or an inhibitor of the anandamide transporter, AM404, into structures surrounding the vMPFC (n ⫽ 4) did not affect the slopes of bradycardic (before ⫽ ⫺1.90 ⫾ 0.16 and after ⫽ ⫺2.11 ⫾ 0.28 beats·min⫺1·mmHg⫺1; t ⫽ 0.6; P ⬎ 0.05) and tachycardic
(before ⫽ ⫺2.42 ⫾ 0.23 and after ⫽ ⫺2.41 ⫾ 0.19 beats·min⫺1·mmHg⫺1; t ⫽ 0.1; P ⬎ 0.05) responses. CB1 receptor antagonist AM251. Bilateral microinjection of three doses of the CB1 receptor antagonist AM251 into the vMPFC did not affect the basal levels of either MAP or HR (Table 1). Nonlinear regression analysis indicated that a dose of 10 pmol (n ⫽ 6) had no effect on the nonlinear baroreflex parameters analyzed (Fig. 2 and Table 2), while doses of 100 (n ⫽ 8) and 300 pmol (n ⫽ 10) were able to increase the baroreflex activity (Fig. 2 and Table 2). Moreover, we observed a significant correlation between doses and the increase in the baroreflex activity [P1: r2 ⫽ 0.67, degrees of freedom (df) ⫽ 20, P ⬍ 0.05; P2: r2 ⫽ 0.78, df ⫽ 20, P ⬍ 0.05; range: r2 ⫽ 0.5, df ⫽ 20, P ⬍ 0.05; and G: r2 ⫽ 0.5, df ⫽ 20, P ⬍ 0.05]. The effect of AM251 on the baroreflex activity was reverted after 60 min (Fig. 2 and Table 2). For further analysis of the baroreflex response, the effect of either MAP increases or decreases on the HR that were observed before and after bilateral microinjection of different doses of AM251 into the vMPFC was analyzed separately using linear regression (Fig. 2). Again, a dose of 10 pmol did not affect the linear regression slope of both bradycardic [before ⫽ ⫺1.78 ⫾ 0.27 and 10 min after ⫽ ⫺1.97 ⫾ 0.29 beats·min⫺1·mmHg⫺1; F(2,17) ⫽ 0.23, P ⬎ 0.05] and tachycardic [before ⫽ ⫺2.71 ⫾ 0.33 and 10 min after ⫽ ⫺2.63 ⫾ 0.62 beats·min⫺1·mmHg⫺1; F(2,17) ⫽ 0.02, P ⬎ 0.05] responses. However, a dose of 100 pmol increased the slope of the linear regression of both bradycardic [before ⫽ ⫺1.51 ⫾ 0.11 and 10 min after ⫽ ⫺2.01 ⫾ 0.10 beats·min⫺1·mmHg⫺1, F(2,23) ⫽ 57.85, P ⬍ 0.001] and tachycardic [before ⫽ ⫺2.28 ⫾ 0.16 and 10 min after ⫽ ⫺2.84 ⫾ 0.13 beats·min⫺1·mmHg⫺1; F(2,23) ⫽ 50.36, P ⬍ 0.001] responses. Similarly, a dose of 300 pmol also increased the slope of the linear regression of both bradycardic [before ⫽ ⫺1.80 ⫾ 0.11 and 10 min after ⫽ ⫺2.50 ⫾ 0.24 beats·min⫺1·mmHg⫺1; F(2,29) ⫽ 4.90, P ⬍ 0.05] and tachycardic [slope before ⫽ ⫺2.59 ⫾ 0.21; slope 10 min after ⫽ ⫺3.31 ⫾ 0.13 beats·min⫺1·mmHg⫺1; F(2,29) ⫽ 4.30, P ⬍ 0.05] responses. Nonlinear regression analysis showed a significant correlation between doses and the increase in both bradycardic (r2 ⫽ 0.87, df ⫽ 20, P ⬍ 0.05) and tachycardic (r2 ⫽ 0.78, df ⫽ 20, P ⬍ 0.05) slope values. The slope values were back at the control level 60 min after AM251 administration (10 pmol: bradycardia ⫽ ⫺1.76 ⫾ 0.12 beats·min⫺1·mmHg⫺1 and tachycardia ⫽ ⫺2.61 ⫾ 0.19 beats·min⫺1·mmHg⫺1; P ⬎ 0.05; 100 pmol: bradycardia ⫽ ⫺1.51 ⫾ 0.11 beats·min⫺1·mmHg⫺1 and tachycardia ⫽ ⫺2.11 ⫾ 0.16 beats·min⫺1·mmHg⫺1; P ⬎ 0.05; 300 pmol: bradycardia ⫽ ⫺1.76 ⫾ 0.19 beats·min⫺1·mmHg⫺1 and tachycardia ⫽ ⫺2.84 ⫾ 0.18 beats·min⫺1·mmHg⫺1; P ⬎ 0.05). The group of animals that received a microinjection of 300 pmol of AM251 was subdivided into animals that received the microinjection into the PL or into the IL. The effects of AM251 were not different on linear regression slope when administrated into the PL or IL for both bradycardic (PL ⫽ ⫺2.43 ⫾ 0.22 beats·min⫺1·mmHg⫺1 and IL ⫽ ⫺2.53 ⫾ 0.28 beats·min⫺1·mmHg⫺1; t ⫽ 0.3; P ⬎ 0.05) and tachycardic (PL ⫽ ⫺3.01 ⫾ 0.21 beats·min⫺1·mmHg⫺1 and IL ⫽ ⫺3.20 ⫾ 0.21 beats·min⫺1·mmHg⫺1; t ⫽ 0.7; P ⬎ 0.05) responses. Anandamide transporter inhibitor AM404. Bilateral microinjection of two doses of the anandamide transporter inhibitor AM404 into the vMPFC did not affect the basal levels of either MAP or HR (Table 1). The analysis of nonlinear regression
AJP-Regul Integr Comp Physiol • doi:10.1152/ajpregu.00330.2011 • www.ajpregu.org
R879
vMPFC eCBs AND BAROREFLEX
Table 1. Effect of bilateral microinjection of AM251, AM404, or URB597 into the vMPFC on the basal values of MAP and HR AM251
MAP Before After HR Before After
AM404
10 pmol
100 pmol
300 pmol
50 pmol
100 pmol
URB597, 100 pmol
t ⫽ 0.5, P ⬎ 0.05 98 ⫾ 4 96 ⫾ 4 t ⫽ 0.1, P ⬎ 0.05 362 ⫾ 10 361 ⫾ 8
t ⫽ 1.3, P ⬎ 0.05 88 ⫾ 3 91 ⫾ 2 t ⫽ 0.6, P ⬎ 0.05 355 ⫾ 15 361 ⫾ 12
t ⫽ 1.3, P ⬎ 0.05 104 ⫾ 3 102 ⫾ 2 t ⫽ 0.7, P ⬎ 0.05 375 ⫾ 10 381 ⫾ 10
t ⫽ 1.0, P ⬎ 0.05 97 ⫾ 3 95 ⫾ 3 t ⫽ 1.0, P ⬎ 0.05 401 ⫾ 24 398 ⫾ 26
t ⫽ 0.8, P ⬎ 0.05 100 ⫾ 2 98 ⫾ 2 t ⫽ 1.5, P ⬎ 0.05 339 ⫾ 12 346 ⫾ 10
t ⫽ 1.7, P ⬎ 0.05 96 ⫾ 4 93 ⫾ 5 t ⫽ 1.5, P ⬎ 0.05 399 ⫾ 18 404 ⫾ 19
Values are means ⫾ SE. vMPFC, ventral portion of the medial prefrontal cortex (n ⫽ 5/10); MAP, mean arterial pressure; HR, heart rate; AM251, N-(piperidin-1-yl)-5-(4-iodophenyl)-1-(2,4-dichlorophenyl)-4-methyl-1H-pyrazole-3-carboxamide; AM404, 4-hydroxyphenylarachidonylamide; URB597, 3=(aminocarbonyl)(1,1=-biphenyl)-3-yl-cyclohexylcarbamate; t, t-test.
indicated that 50 pmol of AM404 (n ⫽ 5) did not affect the baroreflex activity (Fig. 3; Table 3). Moreover, linear regression analysis showed that the slope of both bradycardic [before ⫽ ⫺1.78 ⫾ 0.27 and 10 min after ⫽ ⫺1.97 ⫾ 0.29 beats·min⫺1·mmHg⫺1; F(2,14) ⫽ 1.14; P ⬎ 0.05] and tachycardic [before ⫽ ⫺2.70 ⫾ 0.30 and 10 min after ⫽ ⫺2.60 ⫾ 0.60 beats·min⫺1·mmHg⫺1; F(2,14) ⫽ 0.25; P ⬎ 0.05] responses were not affected by the same dose of AM404 (Fig. 3).
However, a dose of 100 pmol (n ⫽ 6) decreased the baroreflex activity evaluated in nonlinear regression, which was normalized after 60 min (Fig. 3 and Table 3). Similarly, this dose also decreased the slope of the linear regression of both bradycardic [before ⫽ ⫺2.06 ⫾ 0.21 and 10 min after ⫽ ⫺1.28 ⫾ 0.14 beats·min⫺1·mmHg⫺1, F(2,17) ⫽ 5.19; P ⬍ 0.05] and tachycardic [before ⫽ ⫺2.96 ⫾ 0.22 and 10 min after ⫽ ⫺2.21 ⫾ 0.20 beats·min⫺1·mmHg⫺1; F(2,17) ⫽ 3.14; P ⬍ 0.05] re-
Fig. 2. A, C, and E: sigmoid curves correlating mean arterial pressure (⌬MAP) and heart rate (⌬HR) before (r2 ⫽ 0.91, 0.93, 0.81) and 10 min (r2 ⫽ 0.84, 0.95, 0.92) and 60 min (r2 ⫽ 0.96, 0.93, 0.94) after bilateral microinjection of 10 pmol (n ⫽ 6; A), 100 pmol (n ⫽ 8; C), or 300 pmol (n ⫽ 10; E) of AM251 into the vMPFC. The symbols correspond to median blood pressure (BP50). B, D, and F: regression curves correlating the responses of ⌬MAP and ⌬HR before and 10 min and 60 min after bilateral microinjection of AM251 into the vMPFC. Correlation r2 values for bradycardic regression curves were 0.66, 0.85, and 0.66 for data recorded before; 0.67, 0.93, and 0.59 for data recorded 10 min after; and 0.90, 0.87, and 0.69 for data recorded 60 min after microinjection of AM251 10 (B) or 100 pmol (D) or 300 pmol (F) into the vMPFC. Correlation r2 values for tachycardic regression curves were 0.75, 0.96, and 0.72 for data recorded before; 0.45, 0.94, and 0.84 for data recorded 10 min after; and 0.90, 0.85, and 0.87 for data recorded 60 min after microinjection of AM251 into the vMPFC. Values are means ⫾ SE. bpm, Beats/min. AJP-Regul Integr Comp Physiol • doi:10.1152/ajpregu.00330.2011 • www.ajpregu.org
R880
vMPFC eCBs AND BAROREFLEX
Table 2. Parameters derived from the sigmoidal curve generated before and 10 and 60 min after bilateral microinjection of 10, 100, or 300 pmol of AM251 into the vMPFC AM251
10 pmol Before 10 min 60 min 100 pmol Before 10 min 60 min 300 pmol Before 10 min 60 min
after after after after after after
G, beats 䡠 min⫺1 䡠 mmHg⫺1
P1, beats/min
P2, beats/min
Range, beats/min
BP50, mmHg
F(2,17) ⫽ 0.51 ⫺2.06 ⫾ 0.14 ⫺2.24 ⫾ 0.19 ⫺2.08 ⫾ 0.07 F(2,23) ⫽ 12.63 ⫺1.36 ⫾ 0.06 ⫺1.71 ⫾ 0.06* ⫺1.34 ⫾ 0.06 F(2,29) ⫽ 19.48 ⫺1.90 ⫾ 0.10 ⫺2.70 ⫾ 0.11* ⫺2.05 ⫾ 0.08
F(2,17) ⫽ 0.06 ⫺71 ⫾ 6 ⫺74 ⫾ 9 ⫺74 ⫾ 5 F(2,23) ⫽ 11.02 ⫺55 ⫾ 3 ⫺70 ⫾ 4* ⫺54 ⫾ 2 F(2,29) ⫽ 4.12 ⫺57 ⫾ 14 ⫺98 ⫾ 11* ⫺65 ⫾ 6
F(2,17) ⫽ 0.03 104 ⫾ 9 105 ⫾ 17 101 ⫾ 7 F(2,23) ⫽ 9.39 82 ⫾ 5 102 ⫾ 3* 77 ⫾ 5 F(2,29) ⫽ 4.13 99 ⫾ 7 125 ⫾ 7* 107 ⫾ 6
F(2,17) ⫽ 0.04 175 ⫾ 10 178 ⫾ 13 175 ⫾ 5 F(2,23) ⫽ 16.71 137 ⫾ 6 173 ⫾ 5* 131 ⫾ 6 F(2,29) ⫽ 6.37 167 ⫾ 10 223 ⫾ 16* 173 ⫾ 10
F(2,17) ⫽ 0.02 ⫺6.1 ⫾ 2.6 ⫺5.6 ⫾ 2.0 ⫺6.0 ⫾ 1.6 F(2,23) ⫽ 0.98 ⫺7.7 ⫾ 2.0 ⫺6.6 ⫾ 0.9 ⫺7.2 ⫾ 1.9 F(2,29) ⫽ 0.10 ⫺5.3 ⫾ 2.3 ⫺4.6 ⫾ 1.8 ⫺5.8 ⫾ 1.8
Values are means ⫾ SE; n ⫽ 6 for 10 pmol, n ⫽ 8 for 100 pmol, and n ⫽ 10 for 300 pmol of AM251. G, average gain; P1, lower HR plateau; P2, upper HR plateau; BP50, median blood pressure. *P ⬍ 0.05, significant difference from values before AM251 administrations, one-way ANOVA followed by Dunnett’s posttest.
sponses (Fig. 3). The recovery of the baroreflex was observed 60 min after administration of AM404 (bradycardia: ⫺2.11 ⫾ 0.24 beats·min⫺1·mmHg⫺1, P ⬎ 0.05; and tachycardia: ⫺2.73 ⫾ 0.23 beats·min⫺1·mmHg⫺1, P ⬎ 0.05) (Fig. 3). Finally, the decrease of baroreflex activity, evaluated in nonlinear regression, evoked by a dose of 100 pmol of AM404, was inhibited by vMPFC pretreatment with 10 pmol of the CB1 receptor antagonist AM251 (n ⫽ 5) (Fig. 3 and Table 3). In the same way, the decrease of slope observed in both bradycardic [before ⫽ ⫺1.71 ⫾ 0.16 and 10 min after ⫽ ⫺1.66 ⫾ 0.11 beats·min⫺1·mmHg⫺1; F(2,14) ⫽ 0.33; P ⬎ 0.05] and tachycardic [before ⫽ ⫺3.00 ⫾ 0.20 and 10 min after ⫽ ⫺2.85 ⫾ 0.08 beats·min⫺1·mmHg⫺1; F(2,14) ⫽ 1.33; P ⬎ 0.05] responses were inhibited by treatment with AM251 (Fig. 3). Enzyme that degrades anandamide inhibitor URB597. Bilateral microinjection into the vMPFC of an inhibitor of the enzyme that degrades anandamide URB597 did not affect the basal levels of either MAP or HR (Table 1). Nonlinear regression analysis indicated that 100 pmol of URB597 (n ⫽ 6) decreased the baroreflex activity, which was normalized after 60 min (Fig. 4 and Table 4). Similarly, 100 pmol of URB597 also decreased the slope of the linear regression of both bradycardic [before ⫽ ⫺2.02 ⫾ 0.17 and 10 min after ⫽ ⫺1.29 ⫾ 0.29 beats·min⫺1·mmHg⫺1; F(2,17) ⫽ 4.49; P ⬍ 0.05] and tachycardic [before ⫽ ⫺2.42 ⫾ 0.22 and 10 min after ⫽ ⫺1.41 ⫾ 0.24 beats·min⫺1·mmHg⫺1; F(2,17) ⫽ 6.47; P ⬍ 0.001] responses (Fig. 4). Recovery of the baroreflex was observed 60 min after administration of URB597 (bradycardia: ⫺2.05 ⫾ 0.10 beats·min⫺1·mmHg⫺1, P ⬎ 0.05; and tachycardia: ⫺2.29 ⫾ 0.18 beats·min⫺1·mmHg⫺1, P ⬎ 0.05) (Fig. 4). Similar to the observation with AM404, an anandamide transporter inhibitor, the reduction of baroreflex activity, evaluated in nonlinear regression, evoked by URB597, was inhibited by vMPFC pretreatment with 10 pmol of the CB1 receptor antagonist AM251 (n ⫽ 7) (Fig. 4 and Table 4). Similarly, the decrease of slope observed in both bradycardic [before ⫽ ⫺1.48 ⫾ 0.24 and 10 min after ⫽ ⫺1.49 ⫾ 0.20 beats·min⫺1·mmHg⫺1; F(2,20) ⫽ 0.45; P ⬎ 0.05] and tachycardic [slope before ⫽ ⫺2.27 ⫾ 0.35 and 10 min after ⫽ ⫺2.38 ⫾ 0.31 beats·min⫺1·mmHg⫺1; F(2,20) ⫽ 0.79; P ⬎ 0.05] responses was inhibited by treatment with AM251 (Fig. 4).
DISCUSSION
The present study showed that the vMPFC eCBs has an influence on baroreflex activity. This is supported by the observation that a blockade of CB1 receptors increased baroreflex activity, as well as by the observation that increases in endogenous anandamide levels, which were evoked by inhibition of either the enzyme that degrades anandamide (FAAH) or anandamide reuptake induces a decrease in the baroreflex response that is dependent on CB1 receptor activation. These findings indicate that the eCBs system in the vMPFC plays a complex role in the modulation of baroreflex activity. Previous results had shown that vMPFC inhibition, caused by lidocaine, affected the parasympathetic without interfering with the sympathetic component of the baroreflex activity (49). The reasons for these contradictory results could involve the fact that lidocaine affects both fibers of passage and synapses terminations by blocking voltage-gated Na⫹ channels (33), whereas the eCBs modulates the release of neurotransmitters (20). The analyses of baroreflex sigmoid curves generated before and 10 min after bilateral microinjection of the CB1 receptor antagonist AM251 at doses of 100 and 300 pmol, but not 10 pmol, resulted in an increase of the lower HR plateau (P1), upper HR plateau (P2), ⌬P (range HR), and the slope of the sigmoid curve (G), without changes in BP50. The P1 rise was due to an increase in the baroreflex parasympathetic activity, which strengthened the reflex bradycardia in response to blood pressure increases (21). The P2 rise was a consequence of the increased sympathetic activity, which promoted an enhancement in the tachycardic response associated with a reduction in the blood pressure (21), while the increase in the ⌬P was result of P1 and P2 increases (9). Moreover, these increases in both the parasympathetic and sympathetic baroreflex components caused a cardiac baroreflex G facilitation associated with blood pressure variations. To further analyze the baroreflex response, tachycardic and bradycardic responses were analyzed separately using linear regression. The linear regression analysis confirmed that the slope of HR associated with blood pressure variations was increased. Together, these results suggest an inhibitory influence of the CB1 receptors present in the vMPFC on both bradycardic and tachycardic responses of the baroreflex. The
AJP-Regul Integr Comp Physiol • doi:10.1152/ajpregu.00330.2011 • www.ajpregu.org
R881
vMPFC eCBs AND BAROREFLEX
Fig. 3. A, C, and E: sigmoid curves correlating ⌬MAP and ⌬HR before (r2 ⫽ 0.94, 0.94, 0.95) and 10 min (r2 ⫽ 0.92, 0.92, 0.97) and 60 min (r2 ⫽ 0.94, 0.94, 0.95) after bilateral microinjection of 50 pmol (n ⫽ 5; A) or 100 pmol (n ⫽ 6; C) of AM404 or 100 pmol of AM404 after 10 pmol of AM251 (n ⫽ 5; E) into the vMPFC. The symbols correspond to BP50. B, D, and F: regression curves correlating the responses of ⌬MAP and ⌬HR before and 10 min and 60 min after bilateral microinjection of AM404 into the vMPFC. Correlation r2 values for bradycardic regression curves were 0.90, 0.81, and 0.87 for data recorded before; 0.76, 0.79, and 0.93 for data recorded 10 min after; and 0.78, 0.81, and 0.83 for data recorded 60 min after microinjection of 50 pmol (B) or 100 pmol of AM404 (D) or AM404 after AM251 (F) into the vMPFC. Correlation r2 values for tachycardic regression curves were 0.80, 0.87, and 0.93 for data recorded before; 0.61, 0.82, and 0.99 for data recorded 10 min after; and 0.85, 0.85, and 0.94 for data recorded 60 min after microinjection of 50 pmol or 100 pmol of AM404 or AM404 after AM251 into the vMPFC. Values are means ⫾ SE.
baroreflex activity was back to normal 60 min after microinjections into the vMPFC, thus pointing to the reversibility of the CB1 antagonism caused by the antagonist AM251. Early reports have shown some differences between IL and PL, areas that comprise the vMPFC, in the modulation of
cardiovascular and behavioral responses (16, 17, 26, 27). Tavares and colleagues showed that a pharmacological blockade of PL synapses increased the HR response associated with restraint stress, while the blockade of IL synapses reduced the HR increases observed in animals exposed to restraint stress
Table 3. Parameters derived from the sigmoidal curve generated before and 10 and 60 min after bilateral microinjection of 50 or 100 pmol of AM404 and 100 pmol of AM404 after 10 pmol of AM251 into the vMPFC AM404, 50 pmol Before 10 min after 60 min after AM404, 100 pmol Before 10 min after 60 min after AM251 ⫹ AM404 Before 10 min after 60 min after
G, beats 䡠 min⫺1 䡠 mmHg⫺1
P1, beats/min
P2, beats/min
Range, beats/min
BP50, mmHg
F(2,14) ⫽ 1.73 ⫺1.83 ⫾ 0.06 ⫺2.02 ⫾ 0.09 ⫺1.94 ⫾ 0.05 F(2,17) ⫽ 33.22 ⫺2.10 ⫾ 0.10 ⫺1.38 ⫾ 0.08* ⫺2.28 ⫾ 0.07 F(2,14) ⫽ 2.03 ⫺1.88 ⫾ 0.09 ⫺1.68 ⫾ 0.06 ⫺1.82 ⫾ 0.06
F(2,14) ⫽ 1.40 ⫺90 ⫾ 7 ⫺81 ⫾ 9 ⫺85 ⫾ 11 F(2,17) ⫽ 9.79 ⫺78 ⫾ 5 ⫺49 ⫾ 5* ⫺82 ⫾ 8 F(2,14) ⫽ 0.64 ⫺65 ⫾ 6 ⫺59 ⫾ 4 ⫺67 ⫾ 6
F(2,14) ⫽ 0.18 81 ⫾ 9 73 ⫾ 12 75 ⫾ 6 F(2,17) ⫽ 4.31 110 ⫾ 7 81 ⫾ 7* 104 ⫾ 8 F(2,14) ⫽ 1.59 110 ⫾ 5 104 ⫾ 3 100 ⫾ 4
F(2,14) ⫽ 0.25 171 ⫾ 15 154 ⫾ 20 160 ⫾ 15 F(2,17) ⫽ 8.52 187 ⫾ 11 129 ⫾ 10* 186 ⫾ 13 F(2,14) ⫽ 0.36 175 ⫾ 9 171 ⫾ 6 164 ⫾ 11
F(2,14) ⫽ 0.16 ⫺3.4 ⫾ 0.8 ⫺2.9 ⫾ 0.9 ⫺2.7 ⫾ 0.8 F(2,17) ⫽ 0.07 ⫺5.8 ⫾ 0.6 ⫺6.1 ⫾ 0.9 ⫺5.7 ⫾ 1.1 F(2,14) ⫽ 0.10 ⫺9.4 ⫾ 2.1 ⫺9.6 ⫾ 1.0 ⫺8.7 ⫾ 1.2
Values are means ⫾ SE; n ⫽ 5 for 50 pmol and n ⫽ 6 for 100 pmol of AM404 and n ⫽ 6 for 100 pmol of AM404 after 10 pmol of AM251 into the vMPFC. *P ⬍ 0.05, significant difference from values before AM404 administrations, one-way ANOVA followed by Dunnett’s posttest. AJP-Regul Integr Comp Physiol • doi:10.1152/ajpregu.00330.2011 • www.ajpregu.org
R882
vMPFC eCBs AND BAROREFLEX
Fig. 4. A and C: sigmoid curves correlating ⌬MAP and ⌬HR before (r2 ⫽ 0.91, 0.85) and 10 min (r2 ⫽ 0.88, 0.88) and 60 min (r2 ⫽ 0.97, 0.93) after bilateral microinjection of 100 pmol of URB597 (n ⫽ 6; A) or 100 pmol of URB597 after 10 pmol of AM251 (n ⫽ 7; C) into the vMPFC. The symbols correspond to BP50. B and D: linear regression curves correlating the responses of ⌬MAP and ⌬HR before and 10 min and 60 min after bilateral microinjection of 100 pmol of URB597 into the vMPFC. Correlation r2 values for bradycardic regression curves were 0.86 and 0.59 for data recorded before; 0.47 and 0.68 for data recorded 10 min after; and 0.94 and 0.85 for data recorded 60 min after microinjection of URB597 (B) or AM251 ⫹ URB597 (D) into the vMPFC. Correlation r2 values for tachycardic regression curves were 0.60 and 0.62 for data recorded before; 0.62 and 0.69 for data recorded 10 min after; and 0.87 and 0.83 for data recorded 60 min after microinjection of URB597 or AM251⫹URB597 into the vMPFC. Values are means ⫾ SE.
(53). Corroborating these findings, Friztak and Neafsey (16) described that HR increases observed during fear conditioning had a different influence of the IL and PL. Therefore, to test if the eCBs, and particularly CB1 receptors, in both the PL and IL cortex could modulate the baroreflex activity differently, animals that received a dose of 300 pmol of the CB1 receptor antagonist AM251 were separated according to the site of microinjection into two groups, PL and IL. The same effects of CB1 receptor antagonism on baroreflex activity were observed when AM251 was administrated in the PL or IL. Even if 200-nl injection volumes could be significantly large, the injection sites in the PL cortex were located more dorsally, and the injections into the IL cortex were made more ventrally. Moreover, the bilateral administration of CB1 receptor antagonist AM251 into structures surrounding the vMPFC, which are near to both areas, did not affect baroreflex activity. Therefore, it is less probable that the effects of drugs would be due to their
spread from the site of injection to one unspecific point, in this case located between the IL and PL. These findings are in agreement with observations that the IL or PL electrical or chemical stimulation evoked similar cardiovascular responses (38, 39, 46, 55). Moreover, some studies using contextual fear conditioning showed that IL and PL had the same role in defensive responses, including cardiovascular responses evoked by these stress situations (7, 32, 50). Thus our findings show a homogeneous influence of the vMPFC subarea eCBs on baroreflex activity. We also evaluated the effects evoked by an increase of vMPFC endogenous anandamide levels on baroreflex activity. There are two mechanisms that cooperate to attenuate anandamide signaling in the CNS: carrier-mediated transport into cells and intracellular hydrolysis. Anandamide can diffuse passively through lipid membranes entering cells, but this process is accelerated by a rapid and selective carrier system
Table 4. Parameters derived from the sigmoidal curve generated before and 10 and 60 min after bilateral microinjection of 100 pmol of URB597 and the same dose after 10 pmol of AM251 into the vMPFC URB597 Before 10 min after 60 min after AM251 ⫹ URB597 Before after 10 min after 60 min after
G, beats 䡠 min⫺1 䡠 mmHg⫺1
P1, beats/min
P2, beats/min
Range, beats/min
BP50, mmHg
F(2,17) ⫽ 14.15 ⫺2.26 ⫾ 0.12 ⫺1.66 ⫾ 0.10* ⫺2.30 ⫾ 0.06 F(2,20) ⫽ 0.04 ⫺1.48 ⫾ 0.10 ⫺1.51 ⫾ 0.09 ⫺1.50 ⫾ 0.06
F(2,17) ⫽ 6.33 ⫺77.3 ⫾ 3.6 ⫺60.0 ⫾ 3.9* ⫺78.8 ⫾ 4.9 F(2,20) ⫽ 0.04 ⫺56.0 ⫾ 7.4 ⫺55.4 ⫾ 5.6 ⫺57.9 ⫾ 4.8
F(2,17) ⫽ 5.94 94.2 ⫾ 10.1 61.8 ⫾ 7.3* 96.7 ⫾ 6.0 F(2,20) ⫽ 0.09 84.6 ⫾ 11.2 87.3 ⫾ 10.1 81.6 ⫾ 6.9
F(2,17) ⫽ 5.28 171.5 ⫾ 14.7 121.8 ⫾ 12.9* 175.5 ⫾ 11.2 F(2,20) ⫽ 0.10 140.6 ⫾ 16.8 142.7 ⫾ 14.1 139.4 ⫾ 10.0
F(2,17) ⫽ 0.16 ⫺2.0 ⫾ 0.4 ⫺2.1 ⫾ 0.5 ⫺2.5 ⫾ 1.0 F(2,20) ⫽ 0.04 ⫺6.3 ⫾ 1.7 ⫺6.8 ⫾ 1.9 ⫺6.2 ⫾ 1.3
Values are means ⫾ SE; n ⫽ 6 for 100 pmol of URB597 and n ⫽ 7 for the same dose after 10 pmol of AM251 into the vMPFC. *P ⬍ 0.05, significant difference from values before AM404 administrations, one-way ANOVA followed by Dunnett’s posttest. AJP-Regul Integr Comp Physiol • doi:10.1152/ajpregu.00330.2011 • www.ajpregu.org
vMPFC eCBs AND BAROREFLEX
that is present in both neurons and glial cells (6, 24). Moreover, there are also intracellular enzymes that degrade anandamide, such as the FAAH, an intracellular membrane-bound serine hydrolase that breaks down anandamide into arachidonic acid and ethanolamine (8, 52). Therefore, compared with antagonism of CB1 receptors, a vMPFC anandamide level increase, evoked by either AM404 (an inhibitor of anandamide transporter) or URB597 (FAAH inhibitor), produced an opposite effect on baroreflex activity, which was characterized by a decrease of P1, P2, ⌬P, and G sigmoidal parameters. Moreover, in the linear regression analyses, we observed a decrease in both tachycardic and bradycardic responses associated with blood pressure variation. These effects on baroreflex, evoked by increased anandamide levels in the vMPFC, were inhibited by a preadministration of an ineffective dose of AM251. Therefore, our data show that CB1 receptor activation in the vMPFC has an inhibitory influence on baroreflex activity, and that the increase of anandamide levels in the vMPFC decreases the baroreflex response, which is dependent on CB1 receptors. On the other hand, the blockade of CB1 receptors increases the baroreflex response. Together, these findings suggest that activation of CB1 receptors in the vMPFC could be modulating the baroreflex response, reinforcing the proposed role of this brain area in this process (49, 56). It has been described that glutamatergic neurotransmission in the CNS can be modulated by the eCBs (15, 20). In the vMPFC, CB1 receptors are localized presynaptically in glutamatergic neuron terminations (5, 12) and a CB1 receptor agonist decreases glutamate release, whereas a CB1 receptor antagonist increases it (5). Moreover, systemic administration of a CB1 receptor antagonist increases neuronal activation in the vMPFC (2). These results suggest that glutamatergic releases in the vMPFC are tonically inhibited by endogenous cannabinoids through CB1 receptors. In agreement with these data, it was described that antagonism of N-methyl-D-aspartate (NMDA) glutamatergic receptors in the vMPFC decreases parasympathetic baroreflex activity (45), as we observed with increases of CB1 receptor activation by endogenous anandamide. However, the role of NMDA glutamatergic receptors in the vMPFC on sympathetic baroreflex activity was not investigated, and more experiments are necessary. Finally, findings from our group showed that the glutamatergic system present in the vMPFC is involved with activation of the cardiac sympathetic and parasympathetic nervous system (46). Together, the previous results and the present findings support the idea that the eCBs could play an important role in baroreflex activity by controlling glutamatergic synaptic transmission in the vMPFC. This interaction between glutamate and the eCBs in the vMPFC has been described previously. The systemic administration of CB1 receptor agonists promotes anxiolytic-like effects associated with increases of the anandamide levels in the vMPFC (40). In addition, results from our group showed that expression of mRNA for CB1 receptors in the vMPFC is increased in animals exposed to a protocol of contextual fear conditioning. Moreover, when these animals were treated with the CB1 receptor antagonist AM251 in the vMPFC, they exhibit an increase of both cardiovascular and behavior responses associated with reexposure to the aversive context (30). Finally, the local administration of an antagonist of NMDA receptors in the vMPFC evokes a decrease of both
R883
cardiovascular and behavior responses associated with contextual fear conditioning (47). Thus these data show that vMPFC CB1 receptor inhibition increases aversive responses, possibly by increasing glutamate release, and NMDA receptor antagonism has an opposite effect, suggesting that glutamatergic and eCBs interaction has an influence on anxiety-behavior responses. Several studies have shown that, during defense reactions, there is a change in the baroreflex response (10, 28, 51). The vMPFC is involved in the integration of autonomic and emotional responses (16, 35, 44). Al Maskati and colleagues (1) reported that stimulation of the vMPFC of rats was able to inhibit the cardiovascular component (hypertension and tachycardia) related to defense reactions evoked by stimulation of either the hypothalamus or the amygdala, as well as to suppress other cardiovascular components, such as renal vasoconstriction and vasodilatation in skeletal muscles. Therefore, since modulation of the baroreflex response is important for adjustment of cardiac responses during stressful situations (37) and the vMPFC eCBs is involved with modulation of baroreflex activity, autonomic and behavior responses associated with defensive reactions, possibly by modulating local glutamate release, could involve the vMPFC eCBs in the modulation of baroreflex adjustments associated with emotional responses. Thus, even though there is a cardiac baroreflex activity ongoing during basal (resting) conditions, our findings, together with previous results, suggest that the vMPFC could be modulating baroreflex activity during threat situations. Supporting this view, previous studies have described that, either an acute inhibition or a chronic lesion of the vMPFC did not affect baroreflex basal activity, thus suggesting no tonic influence of the vMPFC on the baroreflex (38, 44, 56, 57). However, more experiments are necessary to investigate this hypothesis. Perspective and Significance In summary, the present results suggest that eCB-mediated neurotransmission in the vMPFC modulates baroreflex activity. They also agree with the proposal that the eCBs acts to modulate glutamate release and suggest that the vMPFC could be a brain site for baroreflex modulation during defensive behavior. ACKNOWLEDGMENTS The authors thank L. H C. Argentin, I. A C. Fortunato, and S. S. Guilhaume for technical help. GRANTS N. C. Ferreira-Junior and A. G. Fedoce have a Coordenação de Aperfeiçoamento de Pessoal de Nivel Superior fellowship; F. H. F. Alves has a Fundação de Amparo a` Pesquisa do Estado de São Paulo (FAPESP) postdoctoral fellowship (2011/07332-3). The present research was also supported by grants from the Conselho Nacional de Desenvolvimento Científico e Tecnológico (305996/2008-8 and 470042/2009-5), FAPESP (2009/03187-9), and Fundação de Apoio ao Ensino, Pesquisa e Assistência do Hospital das Clínicas da FMRP-USP (FAEPA). DISCLOSURES No conflicts of interest, financial or otherwise, are declared by the author(s). AUTHOR CONTRIBUTIONS N.C.F.-J. and L.B.R. conception and design of research; N.C.F.-J., A.d.G.F., and F.H.F.A. performed experiments; N.C.F.-J., F.H.F.A., F.M.d.A.C., and L.B.R. analyzed data; N.C.F.-J., F.M.d.A.C., and L.B.R. interpreted results of experi-
AJP-Regul Integr Comp Physiol • doi:10.1152/ajpregu.00330.2011 • www.ajpregu.org
R884
vMPFC eCBs AND BAROREFLEX
ments; N.C.F.-J. and L.B.R. prepared figures; N.C.F.-J., A.d.G.F., F.H.F.A., F.M.d.A.C., and L.B.R. drafted manuscript; N.C.F.-J., A.d.G.F., F.H.F.A., F.M.d.A.C., and L.B.R. approved final version of manuscript; F.H.F. A., F.M.d.A.C., and L.B.R. edited and revised manuscript. REFERENCES 1. al Maskati HA, Zbrozyna AW. Stimulation in prefrontal cortex area inhibits cardiovascular and motor components of the defence reaction in rats. J Auton Nerv Syst 28: 117–125, 1989. 2. Alonso R, Voutsinos B, Fournier M, Labie C, Steinberg R, Souilhac J, Le Fur G, Soubrie P. Blockade of cannabinoid receptors by SR141716 selectively increases Fos expression in rat mesocorticolimbic areas via reduced dopamine D2 function. Neuroscience 91: 607–620, 1999. 3. Alves FH, Crestani CC, Resstel LB, Correa FM. Insular cortex alpha1adrenoceptors modulate the parasympathetic component of the baroreflex in unanesthetized rats. Brain Res 1295: 119 –126, 2009. 4. Alves FH, Crestani CC, Resstel LB, Correa FM. N-methyl-D-aspartate receptors in the insular cortex modulate baroreflex in unanesthetized rats. Auton Neurosci 147: 56 –63, 2009. 5. Auclair N, Otani S, Soubrie P, Crepel F. Cannabinoids modulate synaptic strength and plasticity at glutamatergic synapses of rat prefrontal cortex pyramidal neurons. J Neurophysiol 83: 3287–3293, 2000. 6. Beltramo M, Stella N, Calignano A, Lin SY, Makriyannis A, Piomelli D. Functional role of high-affinity anandamide transport, as revealed by selective inhibition. Science 277: 1094 –1097, 1997. 7. Corcoran KA, Quirk GJ. Activity in prelimbic cortex is necessary for the expression of learned, but not innate, fears. J Neurosci 27: 840 –844, 2007. 8. Cravatt BF, Giang DK, Mayfield SP, Boger DL, Lerner RA, Gilula NB. Molecular characterization of an enzyme that degrades neuromodulatory fatty-acid amides. Nature 384: 83–87, 1996. 9. Crestani CC, Alves FH, Busnardo C, Resstel LB, Correa FM. N-methylD-aspartate glutamate receptors in the hypothalamic paraventricular nucleus modulate cardiac component of the baroreflex in unanesthetized rats. Neurosci Res 67: 317–326, 2010. 10. Crestani CC, Alves FH, Resstel LB, Correa FM. The bed nucleus of the stria terminalis modulates exercise-evoked cardiovascular responses in rats. Exp Physiol 95: 69 –79, 2010. 11. Crestani CC, Deolindo MV, Alves FH, Resstel LB, Correa FM. Non-N-methyl-D-aspartate glutamate receptors in the lateral hypothalamus modulate cardiac baroreflex responses in conscious rats. Clin Exp Pharmacol Physiol 36: 1079 –1085, 2009. 12. Devane WA, Dysarz FA, 3rd Johnson MR, Melvin LS, Howlett AC. Determination and characterization of a cannabinoid receptor in rat brain. Mol Pharmacol 34: 605–613, 1988. 13. Di Marzo V, Bifulco M, De Petrocellis L. The endocannabinoid system and its therapeutic exploitation. Nat Rev Drug Discov 3: 771–784, 2004. 14. Di Marzo V, Fontana A, Cadas H, Schinelli S, Cimino G, Schwartz JC, Piomelli D. Formation and inactivation of endogenous cannabinoid anandamide in central neurons. Nature 372: 686 –691, 1994. 15. Feigenbaum JJ, Bergmann F, Richmond SA, Mechoulam R, Nadler V, Kloog Y, Sokolovsky M. Nonpsychotropic cannabinoid acts as a functional N-methyl-D-aspartate receptor blocker. Proc Natl Acad Sci U S A 86: 9584 –9587, 1989. 16. Frysztak RJ, Neafsey EJ. The effect of medial frontal cortex lesions on cardiovascular conditioned emotional responses in the rat. Brain Res 643: 181–193, 1994. 17. Frysztak RJ, Neafsey EJ. The effect of medial frontal cortex lesions on respiration, “freezing,” and ultrasonic vocalizations during conditioned emotional responses in rats. Cereb Cortex 1: 418 –425, 1991. 18. Gigg J, Tan AM, Finch DM. Glutamatergic hippocampal formation projections to prefrontal cortex in the rat are regulated by GABAergic inhibition and show convergence with glutamatergic projections from the limbic thalamus. Hippocampus 4: 189 –198, 1994. 19. Hajos N, Freund TF. Distinct cannabinoid sensitive receptors regulate hippocampal excitation and inhibition. Chem Phys Lipids 121: 73–82, 2002. 20. Hampson AJ, Bornheim LM, Scanziani M, Yost CS, Gray AT, Hansen BM, Leonoudakis DJ, Bickler PE. Dual effects of anandamide on NMDA receptor-mediated responses and neurotransmission. J Neurochem 70: 671–676, 1998. 21. Head GA, McCarty R. Vagal and sympathetic components of the heart rate range and gain of the baroreceptor-heart rate reflex in conscious rats. J Auton Nerv Syst 21: 203–213, 1987.
22. Herkenham M, Lynn AB, Johnson MR, Melvin LS, de Costa BR, Rice KC. Characterization and localization of cannabinoid receptors in rat brain: a quantitative in vitro autoradiographic study. J Neurosci 11: 563–583, 1991. 23. Herkenham M, Lynn AB, Little MD, Johnson MR, Melvin LS, de Costa BR, Rice KC. Cannabinoid receptor localization in brain. Proc Natl Acad Sci U S A 87: 1932–1936, 1990. 24. Hillard CJ, Edgemond WS, Jarrahian A, Campbell WB. Accumulation of N-arachidonoylethanolamine (anandamide) into cerebellar granule cells occurs via facilitated diffusion. J Neurochem 69: 631–638, 1997. 25. Howlett AC. Pharmacology of cannabinoid receptors. Annu Rev Pharmacol Toxicol 35: 607–634, 1995. 26. Jaskiw GE, Weinberger DR. Ibotenic acid lesions of the medial prefrontal cortex potentiate FG-7142-induced attenuation of exploratory activity in the rat. Pharmacol Biochem Behav 36: 695–697, 1990. 27. Jinks AL, McGregor IS. Modulation of anxiety-related behaviours following lesions of the prelimbic or infralimbic cortex in the rat. Brain Res 772: 181–190, 1997. 28. Knuepfer MM, Printz MP, Stock G. Increased sensitivity to arousal in spontaneously hypertensive rats is partially dependent upon the amygdala. Clin Exp Hypertens A 13: 505–523, 1991. 29. Korner PI, Shaw J, West MJ, Oliver JR. Central nervous system control of baroreceptor reflexes in the rabbit. Circ Res 31: 637–652, 1972. 30. Lisboa SF, Reis DG, da Silva AL, Correa FM, Guimaraes FS, Resstel LB. Cannabinoid CB1 receptors in the medial prefrontal cortex modulate the expression of contextual fear conditioning. Int J Neuropsychopharmacol 13: 1163–1173, 2010. 31. Lisboa SF, Resstel LB, Aguiar DC, Guimaraes FS. Activation of cannabinoid CB1 receptors in the dorsolateral periaqueductal gray induces anxiolytic effects in rats submitted to the Vogel conflict test. Eur J Pharmacol 593: 73–78, 2008. 32. Lisboa SF, Stecchini MF, Correa FM, Guimaraes FS, Resstel LB. Different role of the ventral medial prefrontal cortex on modulation of innate and associative learned fear. Neuroscience 171: 760 –768, 2010. 33. Lomber SG. The advantages and limitations of permanent or reversible deactivation techniques in the assessment of neural function. J Neurosci Methods 86: 109 –117, 1999. 34. Mailleux P, Vanderhaeghen JJ. Distribution of neuronal cannabinoid receptor in the adult rat brain: a comparative receptor binding radioautography and in situ hybridization histochemistry. Neuroscience 48: 655–668, 1992. 35. Neafsey EJ. Prefrontal cortical control of the autonomic nervous system: anatomical and physiological observations. Prog Brain Res 85: 147–165; discussion 165–146, 1990. 36. Nicolle MM, Baxter MG. Glutamate receptor binding in the frontal cortex and dorsal striatum of aged rats with impaired attentional setshifting. Eur J Neurosci 18: 3335–3342, 2003. 37. Nosaka S. Modifications of arterial baroreflexes: obligatory roles in cardiovascular regulation in stress and poststress recovery. Jpn J Physiol 46: 271–288, 1996. 38. Owens NC, Sartor DM, Verberne AJ. Medial prefrontal cortex depressor response: role of the solitary tract nucleus in the rat. Neuroscience 89: 1331–1346, 1999. 39. Owens NC, Verberne AJ. Regional haemodynamic responses to activation of the medial prefrontal cortex depressor region. Brain Res 919: 221–231, 2001. 40. Patel S, Hillard CJ. Pharmacological evaluation of cannabinoid receptor ligands in a mouse model of anxiety: further evidence for an anxiolytic role for endogenous cannabinoid signaling. J Pharmacol Exp Ther 318: 304 –311, 2006. 41. Paxinos G, Watson C. The Rat Brain in Stereotaxic Coordinates. Boston, MA: Academic, 2007. 42. Piomelli D. The molecular logic of endocannabinoid signalling. Nat Rev Neurosci 4: 873–884, 2003. 43. Piomelli D, Beltramo M, Glasnapp S, Lin SY, Goutopoulos A, Xie XQ, Makriyannis A. Structural determinants for recognition and translocation by the anandamide transporter. Proc Natl Acad Sci U S A 96: 5802–5807, 1999. 44. Resstel LB, Correa FM. Involvement of the medial prefrontal cortex in central cardiovascular modulation in the rat. Auton Neurosci 126 –127: 130 –138, 2006. 45. Resstel LB, Correa FM. Medial prefrontal cortex NMDA receptors and nitric oxide modulate the parasympathetic component of the baroreflex. Eur J Neurosci 23: 481–488, 2006.
AJP-Regul Integr Comp Physiol • doi:10.1152/ajpregu.00330.2011 • www.ajpregu.org
vMPFC eCBs AND BAROREFLEX 46. Resstel LB, Correa FM. Pressor and tachycardic responses evoked by microinjections of L-glutamate into the medial prefrontal cortex of unanaesthetized rats. Eur J Neurosci 21: 2513–2520, 2005. 47. Resstel LB, Correa FM, Guimaraes FS. The expression of contextual fear conditioning involves activation of an NMDA receptor-nitric oxide pathway in the medial prefrontal cortex. Cereb Cortex 18: 2027–2035, 2008. 48. Resstel LB, Fernandes KB, Correa FM. alpha-Adrenergic and muscarinic cholinergic receptors are not involved in the modulation of the parasympathetic baroreflex by the medial prefrontal cortex in rats. Life Sci 77: 1441–1451, 2005. 49. Resstel LB, Fernandes KB, Correa FM. Medial prefrontal cortex modulation of the baroreflex parasympathetic component in the rat. Brain Res 1015: 136 –144, 2004. 50. Resstel LB, Joca SR, Guimaraes FG, Correa FM. Involvement of medial prefrontal cortex neurons in behavioral and cardiovascular responses to contextual fear conditioning. Neuroscience 143: 377–385, 2006. 51. Schlor KH, Stumpf H, Stock G. Baroreceptor reflex during arousal induced by electrical stimulation of the amygdala or by natural stimuli. J Auton Nerv Syst 10: 157–165, 1984. 52. Schmid PC, Zuzarte-Augustin ML, Schmid HH. Properties of rat liver N-acylethanolamine amidohydrolase. J Biol Chem 260: 14145–14149, 1985.
R885
53. Tavares RF, Correa FM, Resstel LB. Opposite role of infralimbic and prelimbic cortex in the tachycardiac response evoked by acute restraint stress in rats. J Neurosci Res 87: 2601–2607, 2009. 54. Tsou K, Brown S, Sanudo-Pena MC, Mackie K, Walker JM. Immunohistochemical distribution of cannabinoid CB1 receptors in the rat central nervous system. Neuroscience 83: 393–411, 1998. 55. Verberne AJ. Medullary sympathoexcitatory neurons are inhibited by activation of the medial prefrontal cortex in the rat. Am J Physiol Regul Integr Comp Physiol 270: R713–R719, 1996. 56. Verberne AJ, Lewis SJ, Worland PJ, Beart PM, Jarrott B, Christie MJ, Louis WJ. Medial prefrontal cortical lesions modulate baroreflex sensitivity in the rat. Brain Res 426: 243–249, 1987. 57. Verberne AJ, Owens NC. Cortical modulation of the cardiovascular system. Prog Neurobiol 54: 149 –168, 1998. 58. Wilson RI, Kunos G, Nicoll RA. Presynaptic specificity of endocannabinoid signaling in the hippocampus. Neuron 31: 453–462, 2001. 59. Wilson RI, Nicoll RA. Endocannabinoid signaling in the brain. Science 296: 678 –682, 2002. 60. Wilson RI, Nicoll RA. Endogenous cannabinoids mediate retrograde signalling at hippocampal synapses. Nature 410: 588 –592, 2001. 61. Zilles K, Wree A. Cortex: area and laminar structure. In: The Rat Nervous System. Orlando, FL: Academic, 1985, p. 649 –685.
AJP-Regul Integr Comp Physiol • doi:10.1152/ajpregu.00330.2011 • www.ajpregu.org