J Cancer Surviv https://doi.org/10.1007/s11764-017-0661-9
Modifiable correlates of perceived cognitive function in breast cancer survivors up to 10 years after chemotherapy completion Ashley Henneghan 1 & Alexa Stuifbergen 1 & Heather Becker 1 & Shelli Kesler 2 & Elisabeth King 3
Received: 7 August 2017 / Accepted: 22 October 2017 # Springer Science+Business Media, LLC 2017
Abstract Background Cognitive changes following breast cancer treatment are likely multifactorial and have been linked to emotional factors, biophysiological factors, and fatigue, among others. Little is known about the contributions of modifiable factors such as stress, loneliness, and sleep quality. The purpose of this study was to explore the direct and indirect effects of perceived stress, loneliness, and sleep quality on perceived cognitive function (PCF) in breast cancer survivors (BCS) after chemotherapy completion. Methods In this observational study, BCS 6 months to 10 years post chemotherapy were recruited from the community. We measured perceived stress, loneliness, sleep quality, anxiety, depression, fatigue, and PCF. Data analyses included descriptive statistics, correlations, and mediation analyses utilizing ordinary least square regression. Results Ninety women who were on average 3 years post chemotherapy completion participated in the study. Moderate to largely negative correlations were found between PCF and the psychosocial and sleep variables (r values ranged from − 0.31 to − 0.70, p values < .0009). Mediation analyses revealed that stress and daytime sleepiness both directly and indirectly impact PCF and that loneliness and sleep quality only have indirect effects (through anxiety and fatigue).
* Ashley Henneghan
[email protected]
1
School of Nursing, University of Texas at Austin, 1710 Red River, Austin, TX 78701, USA
2
Department of Neuro-Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, USA
3
Texas Oncology, Austin, TX, USA
Conclusion Our findings suggest that perceived cognitive changes following breast cancer treatment are multifactorial and that higher stress levels, loneliness, daytime sleepiness, and poorer sleep quality are linked to worse perceived cognitive functioning. Also, stress, loneliness, and sleep quality may affect cognitive functioning through a shared psychobiological pathway. Implications for cancer survivors Interventions targeting stress, loneliness, and sleep quality may improve perceived cognitive functioning in breast cancer survivors. Keywords Breast cancer survivors . Fatigue . Perceived cognitive function . Loneliness . Sleep . Stress
Introduction Cognitive dysfunction is one of the most distressing, feared, and prevalent problems that breast cancer survivors (BCS) experience both during and after treatment [1, 2]. Cognitive dysfunction includes problems with memory, attention, processing speed, and executive functioning [2]. These problems can persist up to 20 years or more after cancer treatment ends [3]. Both objective tests and self-report questionnaires have been used to measure cognitive dysfunction but are generally unrelated to each other [4]. More recently, a shift towards understanding perceived cognitive function (PCF) has been made because of concerns that objective tests lack sensitivity for detecting the cognitive dysfunction that patients report [5]. Most often, cognitive changes reported by BCS are attributed to the toxicities of cancer treatment [6] and there is some evidence to support this hypothesis [7]. However, there is consensus in the scientific community that this phenomenon is likely multifactorial [8, 9].
J Cancer Surviv
In the years following cancer treatment, other emotional, behavioral, and social factors are likely contributing to persistent cognitive dysfunction. Emotional factors including depression and anxiety [10], along with fatigue [4, 11–13], have been associated with self-reports of cognitive dysfunction in BCS. Other psychosocial and behavioral factors include perceived stressors, feelings of loneliness, and sleep quality. The associations between these factors and PCF have been made in similar populations [14–18] but have not yet been simultaneously evaluated in BCS 6 months to 10 years after the end of treatment. Stress, poor sleep quality, and loneliness are interrelated with emotional factors and fatigue, and depressive symptoms have been found to mediate the effects of stress and sleep on fatigue in BCS [19]. Therefore, it is plausible that emotional responses to stress, sleep quality, and loneliness could mediate the effects of these factors on PCF. The purpose of this study was to explore the direct and indirect effects (through feelings of anxiety, depression, and fatigue) of perceived stress, perceived loneliness, and sleep quality on PCF in BCS after chemotherapy completion.
Measures Anxiety, depression, and fatigue Three scales were used from the Patient-Reported Outcomes Measurement Information System (PROMIS) Item Bank v1.0 to operationalize anxiety, depression, and fatigue (emotional distress-anxiety-short form 8a, emotional distressdepression-short form 8a, and fatigue-short form 8a) [20]. For all three scales, scores can range from 8 to 40 with higher scores indicating elevated symptoms. Raw scores were used in analyses, but scores were transformed into standardized t scores for descriptive purposes and described in the BResults^ section. Stress The perceived stress scale (PSS) was used to operationalize perceived stress in this study. Scores can range from 0 to 40 with higher scores indicating higher perceived stress [21]. Loneliness The UCLA loneliness scale revised V. 3 (UCLAR) [22] was used to operationalize loneliness in this study. Total scores can range from 20 to 80 with higher scores indicating a greater degree of loneliness.
Methods Sample Following approval from The University of Texas at Austin institutional review board, participant recruitment occurred from May 2016 to January 2017. Women with a history of non-inflammatory, non-metastatic, primary breast cancer (stages I–III) who received chemotherapy and had been without recurrence from 6 months to 10 years, between the ages of 21 and 65, were recruited. Participants who were receiving hormonal treatments, able to read and write in English, and of any ethnic or racial group were included. Women on systemic steroids, those with physician-diagnosed inflammatory disease (e.g., diabetes mellitus, arthritis) or pre-cancer history of sleep disorders, learning disabilities, or other neurological or psychiatric disorders that could interfere with cognitive function were excluded. Flyers were posted and distributed at community oncology centers, a local breast cancer resource center, the local chapter of the Oncology Nursing Society, and via the Army of Women (Dr. Susan Love Research Foundation). Potential participants were screened for eligibility via telephone, and those who were eligible and provided verbal consent were mailed or emailed a written consent form. After written consent was received, participants were emailed a link for the online survey that included demographic- and treatment-related questions and questionnaires for the psychosocial variables, sleep quality, and perceived cognitive function. Surveys were completed in approximately 30 min of time.
Sleep quality The Pittsburgh sleep quality index [23] was used to evaluate sleep quality. Scores for the Pittsburgh sleep quality index (PSQI) can range from 0 to 21 with higher scores indicating worse sleep quality. Scores greater than or equal to 6 on the PSQI suggest that one is a Bpoor sleeper^; therefore, PSQI total scores were dichotomized into greater than or equal to 6 (poor sleepers) and less than 6 (good sleepers) for descriptive purposes. Perceived cognitive function The functional assessment of cancer therapy-cognitive function instrument version 3 (FACT-Cog) [24] was used to measure PCF. This version of the FACT-Cog includes 37 items, consisting of 4 subscales (perceived cognitive impairments, comments from others, perceived cognitive abilities, and impact on quality of life). Total scores can range from 0 to 148, with lower scores indicating poorer functioning. Statistical analyses The analyses for this study were performed using SPSS 24.0 (IBM) and included (1) descriptive statistics; (2) bivariate correlation analyses between the FACT-Cog subscales, the psychosocial variables, and sleep quality; and (3) mediation analyses using ordinarily least squares to better understand how the psychosocial and sleep variables impact PCF in breast cancer survivors. A Bonferroni adjustment was used to control for multiple comparisons in the Pearson correlation analyses. Those p values less than .0009 were considered significant
J Cancer Surviv
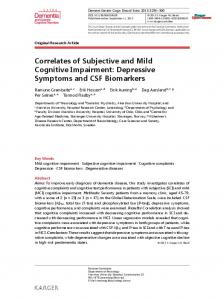
and are denoted by asterisk (*) in Table 3. We used the parallel multiple-mediator modeling analyses described by Hayes [25]. This analysis allows for inferential quantification of the indirect effects of an independent variable on a dependent variable through multiple mediators. Specifically, ordinarily least square regression procedures were used to test the direct and indirect effects (through feelings of anxiety, depression, and fatigue) of perceived stress, perceived loneliness, and sleep quality on PCF. Hayes’ approach utilizes biascorrected bootstrap confidence intervals (bootstrapping = 5000) to estimate and interpret the effect size of the direct and indirect effects of the independent variables on the dependent variables. The direct effects of the independent variable on PCF were determined by the regression coefficient magnitude and significance (p < .05), and the indirect effects (through anxiety, depression, and fatigue) were determined by a significant effect size (95% bootstrap CI does not include 0). The direct and indirect effects (through feelings of anxiety, depression, and fatigue) of perceived stress, perceived loneliness, and perceived sleep quality on PCF were tested. The mediation analysis is conceptually illustrated in Fig. 1. Three separate multiple-mediator models were tested, each with a different independent variable (PSS, UCLA-R, PSQI). FACT-Cog total scores were utilized as the dependent variable, and the same three mediators (PROMIS anxiety, PROMIS depression, PROMIS fatigue) were used in all the mediation models. Since no correlation between demographic and clinical variables and FACT-Cog scores remained significant after the p value was adjusted for multiple comparisons (p values > .0009), no covariates were in the mediator models.
Results One hundred and thirty-seven women responded to the recruitment flyer and were screened. Of these, 23 did not meet inclusion criteria (stage IV breast cancer, did not complete chemotherapy within the specified time period, had inflammatory comorbidities, or were older than 65 years of age). Twenty-four never returned the questionnaire, resulting in a final sample of 90. Descriptive statistics Demographic and treatment characteristics for the 90 participants in this study are displayed in Table 1. The sample was on average 49 years of age (SD 8.99). The majority was white (88.9%), non-Hispanic (94.4%), college-educated (78.9%), and partnered (65.6%). Almost half was living on a household income of < $99,000 (48.9%). The majority of the women had a history of stage II or III (77.8%) invasive ductal carcinoma breast cancer (73.4%) that
was hormone receptor-positive (80%). Almost all were treated with surgery (98.9%); the majority had radiation therapy (64.4%) in addition to anthracycline-based chemotherapy (56.7%) and was treated with some type of hormonal therapy during their course of treatment (78.9%). Approximately 75.5% had gone through menopause already, and 61.1% was currently on hormonal therapy at the time of data collection. On average, the women in the sample had completed chemotherapy 41 months prior, and approximately 81% was within 6 years of chemotherapy completion. Study variables The key study variable descriptive statistics for raw instrument scores are displayed in Table 2. The scores for all the PROMIS scales (anxiety, depression, fatigue) were transformed into t scores per the PROMIS manual [20], so that a score of 50 is equivalent to the population mean and the standard deviation is 10. For PROMIS anxiety, the sample mean was 49.5 (SD 13); for PROMIS depression, 44.03 (SD 10.57); and for PROMIS fatigue, 56.17 (SD 11.71). When the sample was dichotomized into Bpoor^ sleepers (scores ≥ 6) and not Bpoor^ sleepers (scores < 6) per PSQI scores, 63.3% of the sample was categorized as being poor sleepers. Correlations Similar patterns of moderate to largely negative correlations were found between FACT-Cog total, PCI and PCA subscales, and the psychosocial and sleep variables (r values ranged from − 0.31 to − 0.70, p values < .0009) and are displayed in Table 3. Given the stronger corrections with the total compared to the various subscale scores for the FACT-Cog, we used the total score as the dependent variable in the mediation analyses. None of the correlations between FACT-Cog and the demographics or treatment variables remained significant after the Bonferroni adjustment was made. Mediation analyses For PSS, the mediation model explained 60.2% of the variance in FACT-Cog scores (p < .00001). In this model, when all the predictors were evaluated simultaneously, only PSS (B = − 1.45, SE = 0.58, t = − 2.52, p < .02) and PROMIS fatigue (B = − 1.66, SE = 0.41, t = − 4.09, p < .00001) remained significant predictors of FACT-Cog scores. PSS had a significant direct effect on FACT-Cog scores (direct effect = − 1.45, bootstrap SE = 0.58, t = − 2.52, p < .02), meaning that a participant who scores 1 point higher on the PSS scale scored on average 1.5 points lower on the FACTCog. There was a significant negative indirect effect of PSS on FACT-Cog through PROMIS fatigue (indirect effect = − 0.95, bootstrap SE = 0.27, 95% bootstrap CI = − 1.55, − 0.48), meaning that a participant who scores 1 point higher on PSS scored, on average, 1 point lower on FACT-Cog through
J Cancer Surviv m1 Anxiety A1
A2 X1 Stress (a) Loneliness (b) Sleep Quality (c)
m2 Depression
B1
ey
B2
Y Perceived Cognitive Functioning
C
A3
B3
m3 Fatigue
Fig. 1 Mediation model. Conceptual statistical model used to explore the mediation pathways where X1 are the independent variables a perceived stress (PSS), b loneliness (UCLA-R), and c sleep quality (PSQI); m1–m3 are the mediators (anxiety, depression, and fatigue; PROMIS scales); Y is the dependent variable (PCF; FACT-Cog); and C represents the direct
effect of the independent variables on the dependent variable. A1 and B1 represent the indirect effect through anxiety, A2 and B2 represent the indirect effect through depression, and A3 and B3 represent the indirect effect through fatigue. ey represents error
feelings of fatigue. There were no significant negative indirect effect of PSS on FACT-Cog through PROMIS anxiety or PROMIS depression (95% CI values crossed 0). For UCLA-R, the model explained 56.7% of the variance in FACT-Cog scores (p < .00001). In this model, PROMIS anxiety (B = − 1.17, SE = 0.49, t = − 2.42, p < .02) and PROMIS fatigue (B = − 1.96, SE = 0.42, t = − 4.73, p < .00001) remained significant predictors of FACT-Cog scores when all predictors were simultaneously entered into the model. UCLA-R did not have a significant direct effect on FACT-Cog scores (p = .34) but did have significant negative indirect effects through PROMIS anxiety (indirect effect = − 0.33, bootstrap SE = 0.16, 95% bootstrap CI = − 0.70, − 0.07) and PROMIS fatigue (indirect effect = − 0.75, bootstrap SE = 0.21, 95% Bootstrap CI = − 1.22, − 0.40), meaning that a participant who scores 1 point higher on UCLA-R scored, on average, 0.33 points lower on FACT-Cog through feelings of anxiety. A participant who scores 1 point higher on UCLA-R scored, on average, 0.75 points lower on FACT-Cog through feelings of fatigue. There was no significant indirect effect of UCLA-R on FACTCog through PROMIS depression (95% CI crossed 0). The PSQI model explained 56.4% of the variance in FACTCog scores (p < .00001). In this model, only PROMIS fatigue (B = − 1.82, SE = 0.42, t = − 4.39, p < .0001) remained a significant predictor of FACT-Cog scores when all predictors were entered into the model. PSQI did not have a significant direct effect on FACT-Cog scores (p = .52) but did have a significant negative indirect effect through PROMIS anxiety (indirect effect = − 0.89, bootstrap SE = 0.49, 95% bootstrap CI = − 2.00, − 0.04) and PROMIS fatigue (indirect effect = − 2.23, bootstrap SE = 0.60, 95% Bootstrap CI = − 3.56, − 1.20), meaning that a participant who scores 1 point higher on PSQI scored, on average, about 1 point lower on FACT-Cog through feelings of anxiety. A participant
who scores 1 point higher on PSQI scored, on average, 2 points lower on FACT-Cog through feelings of fatigue. There were no significant indirect effect of PSQI on FACTCog through PROMIS depression (95% CI crossed 0).
Discussion This study contributes to our understanding of perceived cognitive dysfunction by BCS for up to 10 years following the end of chemotherapy, in a community setting, using a wellvalidated measure of self-reported cognitive dysfunction. Additionally, this study adds to the growing body of research that has evaluated how emotional factors [10], fatigue [4, 11–13], stress [14], and sleep quality [17, 18] relate to cancer-related cognitive dysfunction and extends our knowledge of how loneliness influences PCF in survivors.
Anxiety, depression, and fatigue To our knowledge, this study is the first to utilize the PROMIS scales to measure anxiety, depression, and fatigue in BCS. Our findings are consistent with Cessna et al. [26] who recently reported on adequate psychometric properties of the PROMIS fatigue short form in a group of prostate and blood cancer survivors. When the total scale scores were transformed into t scores, surprisingly, participants in this study reported lower levels of anxiety and depression than the general population but had higher levels of fatigue. It is possible that these BCS, who were assessed on average 3 years after treatment completion, have Bnormalized^ in terms of their anxiety and depressive symptoms.
J Cancer Surviv Table 1 Demographic and clinical characteristics (N = 90)
Characteristic
Number (%)
Age
Mean (SD)
Min, max
49.19 (8.99)
24, 65
16.67 (2.17)
12, 22
41.88 (32.41)
6.83, 125.61
Race White African American Asian
80 (88.9%) 6 (6.7%) 4 (4.4%)
Ethnicity Hispanic Non-Hispanic
5 (5.6%) 85 (94.4%)
Years of education Highest degree High school/vocational
11 (12.2%)
Associates Bachelors
8 (8.9%) 41 (45.6%)
Graduate Marital status
30 (33.3%)
Married/living with significant other Divorced/separated Never married Have children
59 (65.6%) 13 (14.4%) 18 (20%) 57 (63.3%)
Employment status Work full-time/full-time student
56 (62.2%)
Work part-time Full-time homemaker
21 (24.5%) 4 (4.4%)
Unemployed
4 (4.4%)
Retired Household income (n = 88, 2 missing) $0–50,000 $50,000–99,999 $100,000–149,000
4 (4.4%) 11 (12.2%) 33 (36.7%) 20 (22.2%)
$150,000–199,999 $200,00 or more BC type IDC DCIS ILC Multiple (IDC/DCIS/ILC) Stage 1 2 3 ER receptor +
10 (11.1%) 14 (15.6%)
HER 2 + Chemo regimens Anthracycline-based Non-anthracycline-based Months since chemo 6–12 months 1–2 years 2–4 years
33 (36.7%)
60 (66.7%) 17 (18.9%) 7 (7.8%) 6 (6.7%) 19 (21.1%) 51 (56.7%) 19 (21.3%) 72 (80%)
51 (56.7%) 38 (42.2%) 18 (20%) 16 (17.8%) 26 (28.9%)
J Cancer Surviv Table 1 (continued) Characteristic
Number (%)
4–6 years
13 (14.4%)
6–10 years History of hormonal treatment (n = 71)
16 (17.8%)
Tamoxifen Non-tamoxifen
48 (67.6%) 23 (32.4%)
Mean (SD)
Min, max
Treatment modalities Surgery Radiation
89 (98.9%) 58 (64.4%)
Hormones
71 (78.9%)
Herceptin Menopausal status Pre
31 (34.4%)
Peri
10 (11.1%)
Gone through
19 (21.1%)
Chemically/surgically induced Currently on hormonal therapy
49 (54.4%) 55 (61.1%)
12 (13.3%)
IDC invasive ductal carcinoma, DCIS ductal carcinoma in situ, ILC invasive lobular carcinoma, HER 2 human epidermal growth factor receptor 2, ER estrogen receptor, BC breast cancer
Stress, loneliness, and sleep
Perceived cognitive function
Perceived stress scores were comparable to other studies in BCS [19]. Total scores on UCLA-R fell in the middle of the possible range. Notably, the mean UCLA-R score in this study was much higher than that reported in another study with BCS who were within 3 years post treatment [16]. As time passes after cancer treatment is finished, social support may slowly decline. The mean PSQI in this study was higher than that reported by Xiao et al. [19], and when scores were dichotomized into Bgood^ and Bpoor^ sleepers, approximately 63% of the sample was considered poor sleepers.
In this sample, FACT-Cog scores were higher than one study [27], yet lower than another study [28]. Worse PCF in this sample could be due to the fact that the cohort of women was younger than those in the aforementioned studies or that the women were aware that the focus of our study was on cognitive problems. Research supports that younger survivors report more severe emotional distress and decreased quality of life than older survivors [5]. These comparisons should be interpreted with caution as one study was conducted with BCS in Singapore.
Table 2 Study variable descriptive statistics of raw scores (N = 90)
Measure
Mean (SD)
Min, max
Median
Cronbach’s alpha
PROMIS anxiety
16.67 (8.27)
8, 40
15
0.96
PROMIS depression PROMIS fatigue PSS UCLA-R PSQI total FACT-Cog totala PCI PCA
13.33 (6.23) 20.87 (8.09) 13.70 (8.12) 37.96 (11.29) 7.82 (4.47) 95.55 (34.61) 48.23 (20.85) 22.43 (8.82)
8, 32 8, 40 0, 33 20, 62 0, 19 19, 147 3, 79 4, 36
11 19.5 14.0 36 7.0 95.5 51.5 21.5
0.94 0.96 0.93 0.95 0.75 0.98 0.97 0.93
PROMIS Patient-Reported Outcomes Measurement Information System, PSS perceived stress scale, UCLA-R UCLA loneliness scale revised version 3, PSQI Pittsburgh sleep quality index, FACT-Cog functional assessment of cancer treatment-cognition version 3, PCI perceived cognitive impairments subscale, PCA perceived cognitive abilities subscale a
FACT-Cog total: lower scores indicate lower overall functioning; PCI: lower scores indicate worse cognitive impairments; PCA: higher scores, better abilities; lower scores, worse perceived abilities
J Cancer Surviv Table 3 Correlations between individual factors, predictor variables, and cognitive outcomes (N = 90) FACT-Cog
PCI
PCA
Age
0.14
0.13
0.13
BMI
− 0.25
− 0.29
− 0.19
0.10 0.01
0.08 − 0.00
0.14 0.01
Anthracycline chemoa Tamoxifen treatmentb Ethnicityc Race Breast cancer stage
0.03 − 0.16 − 0.15
0.04 − 0.18 − 0.15
0.00 − 0.15 − 0.14
− 0.09 − 0.03
− 0.07 − 0.02
− 0.09 − 0.06
Months since end of chemo Number of Treatment modalities
0.06 − 0.10
0.06 − 0.11
0.09 − 0.07
Anxiety
− 0.56*
− 0.52*
− 0.47*
Depressive Fatigue
− 0.59* − 0.67*
− 0.55* − 0.62*
− 0.49* − 0.61*
UCLA-R PSS PSQI
− 0.51* − 0.70* − 0.54*
− 0.51* − 0.66* − 0.51*
− 0.40* − 0.60* − 0.46*
Years of education Employment
Pearson’s correlations used for interval-level variables and Kendall’s tau for categorical-level variables BMI body mass index, Anxiety PROMIS anxiety scale, Depressive PROMIS depression scale, Fatigue PROMIS fatigue scale, PSS perceived stress scale, UCLA-R UCLA loneliness scale revised version 3, PSQI Pittsburgh sleep quality index, FACT-Cog functional assessment of cancer treatment-cognition version 3, PCI perceived cognitive impairments subscale, PCA perceived cognitive abilities subscale *p < .0009, Bonferonni correction 0.05/51 a
0 = non-anthracycline, 1 = anthracycline
b
0 = no tamoxifen, 1 = tamoxifen
c
0 = non-Hispanic; 1 = Hispanic
Modifiable correlates of PCF following chemotherapy Moderate to largely significant negative relationships were found between all of the modifiable correlates, anxiety, depression, fatigue, and PCF. To better understand the nature of these relationships and potential psychological mechanisms, multiple mediation analyses were conducted. The findings of the mediation analysis are consistent with those found in the literature linking psychosocial, sleep, and emotional factors to PCF [5, 10, 16, 29, 30] and extend our knowledge of how these factors may impact PCF. There were also significantly moderate to large negative relationships between the psychosocial and sleep variables suggesting that there may be a shared pathway. The study results support that feeling more stress, social isolation, and experiencing worse sleep quality may contribute to poorer PCF in BCS and that these
effects are likely mediated by feelings of anxiety and fatigue. These modifiable factors (stress, perceived social isolation, and sleep quality) may be particularly relevant to BCS because survivors experience 1.5 times more stress than the general population [31]. BCS experience a unique type of loneliness following the completion of treatment termed Bsurvivor loneliness^ [32], and up to 87% of cancer patients experience sleep problems that persist long after treatment ends [33]. Furthermore, these factors could be amenable to treatments such as cognitive behavioral therapy. The relationships between psychological stress and cognitive function in the general and elderly populations are well-documented, and evidence also supports the connection between stress and PCF in oncology populations [29, 30]. In recent years, researchers have suggested that the etiology of cancer-related cognitive impairment might be explained by exposure to prolonged psychological stressors (including cancer and cancer treatment) overloading a persons’ neurological allostasis, resulting in neural biological changes and subsequent cognitive changes [34]. It has also been suggested that overloaded self-regulatory systems can impede cognitive functioning in BCS [35]. The findings from the correlation analyses in this study support these theories. The mediation analyses suggest that perceived stress is a predictor of PCF—directly and indirectly impacting PCF through feelings of fatigue. These findings are consistent with evidence supporting stress as a predictor of PCF in BCS [14] and support the science linking chronic stress to biological changes associated with increased fatigue [11] and worse cognitive functioning [36]. Furthermore, our findings are consistent with those by Cessna et al. [26] linking PSS scores to PROMIS fatigue in hematologic cancer survivors (r = 0.44, p < .05). Research indicates that perceived social isolation or loneliness is a risk factor for poorer cognitive performance and faster cognitive decline [37]. In BCS, loneliness has been linked to worse cognitive functioning and cognitive decline [12, 16]. Although a moderately significant relationship was found between loneliness and PCF in this study, the nuances of this relationship were better revealed in the mediation analyses and suggest that loneliness only indirectly affects PCF through feelings of anxiety and fatigue. This finding sheds light on the psychosocial mechanism of how loneliness impacts PCF in BCS. There is a general consensus that poorer sleep quality in older adults is related to worse cognitive outcomes [38] and that sleep loss can impact aspects of cognitive capacity and emotional regulation [39]. Consistent relationships between aspects of sleep quality and PCF have been reported—specifically, between sleep quality [17, 18], sleep disturbance [30],
J Cancer Surviv
and PCF—in cancer survivors. The current study supports these findings. Our findings also extend knowledge by demonstrating that these effects of sleep quality on PCF are mediated by feelings of anxiety and fatigue. Even though depression was strongly correlated with PCF, it was not a significant predictor of PCF when included in the multiple regression and mediation analyses. Rather, anxiety was the affective factor that significantly predicted PCF and mediated the effects of loneliness and sleep quality on PCF. These findings are contrary to those reported by Janelsins et al. [5] that depression was a significant predictor of PCF but may be attributed to timing of data collection during the cancer trajectory. Perhaps, depression is more involved in the manifestation of cognitive dysfunction earlier in survivorship and anxiety is a key factor in the later years, but further research needs to be conducted. Anxiety and depression are often grouped together as Bemotional distress^ in cancerrelated cognitive impairment research [10]. Although these two factors are typically strongly related, the findings from this study highlight the importance of keeping them as separate concepts in research. Our findings support the growing body of research linking fatigue and cognitive function in BCS [4, 11–13]. Importantly, fatigue was a significant mediator in all three of the models, suggesting that the effects of stress, loneliness, and sleep quality on PCF could share a common pathway—fatigue. The mediating effects of fatigue in this study are consistent with Oh’s [40] findings that fatigue had a greater impact on cognitive decline than depression. Both fatigue and cognitive dysfunction are distressing, prevalent, and persistent in BCS [36] and may be part of a symptom cluster that is amenable to interventions.
Conclusion Findings from this study can only be generalized to women with a history of non-metastatic, non-inflammatory breast cancer who received chemotherapy as part of their treatment regimen. Even though efforts were made to recruit a diverse sample for the study, the majority of the sample was non-Hispanic, white, well-educated, and financially stable; therefore, the external validity is limited demographically. The majority of the instruments in this study were self-report, and those data could have been influenced by recall bias. The study did not have either a non-chemotherapy or non-breast cancer comparison group, which limits the interpretations of the findings. Additionally, it was cross-sectional; therefore, causality cannot be assumed. The parallel multiple-mediator modeling used to evaluate the indirect effects of the psychosocial factors on PCF assumes that none of the mediators influences each other; in other words, they are
independent [25]. It is likely that anxiety and fatigue do influence the other, so this should be considered when interpreting the findings of the mediation analyses. Even though these analyses determined that stress, loneliness, and sleep quality impacted PCF through anxiety and fatigue, we cannot conclude that these are the only mechanisms by which the psychosocial factors affect PCF. It is possible that phenomena not measured in the present study could better explain the pathways between these variables. Additionally, this statistical analysis only allows for a single independent variable to be entered into a model at a time. Considering the variables in this study (stress, loneliness, and sleep quality), which are interrelated, separating them could be problematic. Furthermore, the relationships between predictor variables and the mediators could be bidirectional. An analysis that allows for all of these predictors to be modeled along with the mediators, such as structural equation modeling (SEM), may be more explanatory, but a larger sample would be needed for SEM. The factors evaluated in this study (stress, loneliness, and sleep quality) may be particularly relevant because BCS experience more stress than the general population and loneliness following the completion of treatment and the majority of cancer patients experience sleep problems that persist long after treatment ends. Importantly, these factors are responsive to interventions. Although there are distinct biological and psychological processes for stress, fatigue, anxiety, and loneliness, these processes can also overlap and have synergistic impacts on one’s cognitive functioning [5]. The findings from this study suggest that addressing one or more of the modifiable factors (stress, daytime sleepiness, fatigue, or anxiety) or treating these symptoms as a cluster may be an efficient way to intervene to decrease symptom burden and improve quality of life. Importantly, the constructs of stress and social isolation are very complex and a more in-depth evaluation of the concepts within each of these constructs is needed. The number of BCS in the USA is rising. Some BCS experience cognitive dysfunction for up to 10 years following the end of their chemotherapy. Providers must acknowledge survivors’ concerns and assess cognitive functioning throughout the cancer trajectory. It is essential that providers acknowledge that cancer-related cognitive changes may be influenced by many factors that extend far beyond receiving chemotherapy. Those providing primary care to BCS need to be aware that problems persist over time and should consider screening for cognitive concerns and making referrals when appropriate. Funding information Research reported in this publication was supported by the National Institute of Nursing Research of the National Institutes of Health under award number F31NR015707. The content is solely the
J Cancer Surviv responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Ashley M. Henneghan was supported by the Doctoral Degree Scholarship in Cancer Nursing, DSCN-15-072-01 from the American Cancer Society.
16.
17.
Compliance with ethical standards 18. Conflict of interest The authors declare that they have no conflict of interest.
19.
References 20. 1.
2.
3.
4.
5.
6.
7. 8.
9.
10.
11.
12.
13.
14.
15.
Ganz PA, Bower JE, Kwan L, et al. Does tumor necrosis factoralpha (TNF-α) play a role in post-chemotherapy cerebral dysfunction? Brain Behav Immun. 2013;30(Suppl):S99–S108. Janelsins MC, Kesler SR, Ahles TA, Morrow GR. Prevalence, mechanisms, and management of cancer-related cognitive impairment. Int Rev Psychiatry. 2014;26:102–13. Koppelmans V, Breteler MMB, Boogerd W, Seynaeve C, Gundy C, Schagen SB. Neuropsychological performance in survivors of breast cancer more than 20 years after adjuvant chemotherapy. J Clin Oncol. 2012;30:1080–6. Hutchinson AD, Hosking JR, Kichenadasse G, Mattiske JK, Wilson C. Objective and subjective cognitive impairment following chemotherapy for cancer: a systematic review. Cancer Treat Rev. 2012;38:926. Janelsins MC, Heckler CE, Peppone LJ, et al. Cognitive complaints in survivors of breast cancer after chemotherapy compared with age-matched controls: an analysis from a nationwide, multicenter, prospective longitudinal study. J Clin Oncol. 2017;35:506–14. Wefel JS, Kesler SR, Noll KR, Schagen SB. Clinical characteristics, pathophysiology, and management of noncentral nervous system cancer-related cognitive impairment in adults. CA Cancer J Clin. 2015;65:123–38. Dietrich J, Prust M, Kaiser J. Chemotherapy, cognitive impairment and hippocampal toxicity. Neuroscience. 2015;309:224. Ahles TA, Root JC, Ryan EL. Cancer- and cancer treatmentassociated cognitive change: an update on the state of the science. J Clin Oncol. 2012;30:3675–86. Jim HSL, Phillips KM, Chait S, et al. Meta-analysis of cognitive functioning in breast cancer survivors previously treated with standard-dose chemotherapy. J Clin Oncol. 2012;30:3578–87. Pullens MJJ, de Vries J, Roukema JA. Subjective cognitive dysfunction in breast cancer patients: a systematic review. PsychoOncology. 2010;19:1127–38. Bower JE, Lamkin DM. Inflammation and cancer-related fatigue: mechanisms, contributing factors, and treatment implications. Brain Behav Immun. 2013;30(Suppl):S48–57. Cheung YT, Lim SR, Ho HK, Chan A. Cytokines as mediators of chemotherapy-associated cognitive changes: current evidence, limitations and directions for future research. PLoS One. 2013;8: e81234. Hodgson KD, Hutchinson AD, Wilson CJ, Nettelbeck T. A metaanalysis of the effects of chemotherapy on cognition in patients with cancer. Cancer Treat Rev. 2013;39:297–304. Reid-Arndt SA, Cox CR. Stress, coping and cognitive deficits in women after surgery for breast cancer. J Clin Psychol Med Settings. 2012;19:127–37. Cheung YT, Shwe M, Tan YP, Fan G, Ng R, Chan A. Cognitive changes in multiethnic Asian breast cancer patients: a focus group study. Ann Oncol. 2012;23:2547–52.
21. 22. 23.
24.
25.
26.
27.
28.
29.
30.
31.
32. 33.
34.
Jaremka LM, Peng J, Bornstein R, et al. Cognitive problems among breast cancer survivors: loneliness enhances risk: loneliness and cognitive function. Psycho-Oncology. 2014;23:1356–64. Sanford SD, Beaumont JL, Butt Z, Sweet JJ, Cella D, Wagner LI. Prospective longitudinal evaluation of a symptom cluster in breast cancer. J Pain Symptom Manag. 2014;47:721–30. Von Ah D, Tallman EF. Perceived cognitive function in breast cancer survivors: evaluating relationships with objective cognitive performance and other symptoms using the functional assessment of cancer therapy-cognitive function instrument. J Pain Symptom Manage. 2015;49:697. Xiao C, Miller AH, Felger J, Mister D, Liu T, Torres MA. Depressive symptoms and inflammation are independent risk factors of fatigue in breast cancer survivors. Psychol Med 2017:1–11. Patient-Reported Outcomes Measurement Information System 2017; http://www.healthmeasures.net/explore-measurementsystems/promis/obtain-administer-measures. Accessed July 17, 2017. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24:385–96. Russell DWUCLA. Loneliness scale (version 3): reliability, validity, and factor structure. J Pers Assess. 1996;66:20–40. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. Wagner LI, Sweet JJ, Butt Z, Lai JS, Cella D. Measuring patient self-reported cognitive function: development of the functional assessment of cancer therapy–cognitive function instrument. J Support Oncol. 2009;7:7. Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. New York: The Guilford Press; 2013. Cessna JM, Jim HSL, Sutton SK, et al. Evaluation of the psychometric properties of the PROMIS cancer fatigue short form with cancer patients. J Psychosom Res. 2016;81:9–13. Bray VJ, Dhillon HM, Bell ML, et al. Evaluation of a web-based cognitive rehabilitation program in cancer survivors reporting cognitive symptoms after chemotherapy. J Clin Oncol. 2017;35:217– 25. Cheung YT, Foo YL, Shwe M, et al. Minimal clinically important difference (MCID) for the functional assessment of cancer therapy: cognitive function (FACT-Cog) in breast cancer patients. J Clin Epidemiol. 2014;67:811–20. Li J, Yu L, Long Z, Li Y, Cao F. Perceived cognitive impairment in Chinese patients with breast cancer and its relationship with posttraumatic stress disorder symptoms and fatigue: perceived cognitive impairment in Chinese patients with breast cancer. PsychoOncology. 2015;24:676–82. Myers JS, Wick JA, Klemp J. Potential factors associated with perceived cognitive impairment in breast cancer survivors. Support Care Cancer. 2015;23:3219–28. Parelkar P, Thompson NJ, Kaw CK, Miner KR, Stein KD. Stress coping and changes in health behavior among cancer survivors: a report from the American Cancer Society’s Study of Cancer Survivors-II (SCS-II). J Psychosoc Oncol. 2013;31:136. Rosedale M. Survivor loneliness of women following breast cancer. Oncol Nurs Forum. 2009;36:175–83. Palesh O, Peppone L, Innominato PF, Janelsins M, Jeong M, Sprod L, et al. Prevalence, putative mechanisms, and current management of sleep problems during chemotherapy for cancer. Nat Sci Sleep. 2012;4:151–62. https://doi.org/10.2147/NSS.S18895. Andreotti C, Root JC, Ahles TA, McEwen BS, Compas BE. Cancer, coping, and cognition: a model for the role of stress reactivity in cancer-related cognitive decline: cancer, coping, and cognition. Psycho-Oncology. 2015;24:617–23.
J Cancer Surviv 35.
36.
Arndt J, Das HHJ, Schagen S, Reid-Arndt S, Cameron L, Ahles T. Broadening the cancer and cognition landscape: the role of selfregulatory challenges. Psycho-Oncology. 2014;23:1–8. Bower JE, Ganz PA, Irwin MR, Kwan L, Breen EC, Cole SW. Inflammation and behavioral symptoms after breast cancer treatment: do fatigue, depression, and sleep disturbance share a common underlying mechanism? J Clin Oncol. 2011;29: 3517–22. https://doi.org/10.1200/JCO.2011.36.1154.
37. 38. 39. 40.
Cacioppo JT, Hawkley LC. Perceived social isolation and cognition. Trends Cogn Sci. 2009;13:447–54. Yaffe K, Falvey C, Hoang T. Connections between sleep and cognition in older adults. Lancet Neurol. 2014;13:1017–28. Killgore WDS. Effects of sleep deprivation on cognition. In: Vol 185. AMSTERDAM: Elsevier Science & Technology; 2010:105–129. Oh P. Predictors of cognitive decline in people with cancer undergoing chemotherapy. Eur J Oncol Nurs 2016.