0163-769X/05/$20.00/0 Printed in U.S.A.
Endocrine Reviews 26(1):44 – 62 Copyright © 2005 by The Endocrine Society doi: 10.1210/er.2003-0021
Natural Killer Cells in Pregnancy and Recurrent Pregnancy Loss: Endocrine and Immunologic Perspectives Chrysoula Dosiou and Linda C. Giudice Division of Endocrinology and Metabolism (C.D.), Department of Medicine; and Division of Reproductive Endocrinology and Infertility (L.C.G.), Department of Obstetrics and Gynecology, Stanford University Medical Center, Stanford, California 94305 The endocrine system and the immune system interact closely during implantation and maintenance of pregnancy. One of the most striking examples of this communication is at the level of the decidua (endometrium of pregnancy). Here, under the influence of sex steroids, there is a dramatic increase of a unique population of lymphocytes, the uterine natural killer (uNK) cells, in early pregnancy. These cells derive predominantly from a subset of peripheral blood NK cells, which under hormonal influence gets recruited to the uterus. In mice, uNK cells play an important role in the development of placental vasculature. The role of these cells in human pregnancy is still not definitively established; however, they are believed to
promote placental and trophoblast growth and provide immunomodulation at the maternal-fetal interface. In contrast to their presumptive role in the maintenance of a healthy pregnancy, uNK cells and peripheral NK cells are dysregulated in unexplained recurrent pregnancy loss. Herein, we review NK cell populations, their changes in number and function in altered endocrine environments during the menstrual cycle and pregnancy, the current data on their potential role in unexplained recurrent pregnancy loss, and mechanisms for potential therapies targeted to NK cell function for this enigmatic disorder. (Endocrine Reviews 26: 44 – 62, 2005)
I. Introduction II. Peripheral NK Cells A. Phenotype B. Hormonal regulation C. Function III. uNK Cells: A Unique NK Cell Subset A. Phenotype B. Hormonal regulation C. Function IV. NK Cells in RPL A. Peripheral NK cells in RPL B. uNK cells in RPL C. A model of NK cell function in pregnancy vs. RPL D. NK cells and current RPL therapies V. Eye to the Future
I. Introduction
R
ECURRENT PREGNANCY LOSS (RPL) is defined as three or more consecutive spontaneous abortions (1). It affects about 1% of the child-bearing population (2) and presents couples with this disorder a formidable challenge in successfully having a family. There have been numerous proposed causes of RPL: parental chromosomal abnormalities, uterine anatomic anomalies, endometrial infections, endocrine etiologies (luteal phase defect, thyroid dysfunction, uncontrolled diabetes mellitus), antiphospholipid syndrome, inherited thrombophilias, and alloimmune causes (3). Several reviews on the clinical manifestations of RPL have recently been published (3, 4). Among the various proposed etiologies, only parental karyotype abnormalities, antiphospholipid syndrome, and uterine anatomic abnormalities are universally accepted (3). One of these causes can be identified in about 50% of patients (5); however, in the remainder, the cause is unknown (3). An immune-based etiology underlying unexplained RPL has been proposed; however, the exact mechanism has not been elucidated. Therefore, therapy so far has been empirical and not evidence-based, with no specific treatment of proven efficacy to date (3, 4). In the past decade, considerable effort has been made to identify cellular constituents and processes putatively underlying immune-based RPL. NK cells have been the cells most extensively studied, primarily because they constitute the predominant leukocyte population present in the endometrium at the time of implantation and in early pregnancy. This review critically examines the evidence for hormonal regulation of peripheral and uNK cells, the role of NK cells in pregnancy, and their putative role in unexplained RPL.
First Published Online September 8, 2004 Abbreviations: CSF, Colony-stimulating factor; ER, estrogen receptor; GM-CSF, granulocyte-macrophage CSF; GR, glucocorticoid receptor; hCG, human chorionic gonadotropin; HLA, human leukocyte antigen; IFN, interferon; IRF, IFN-regulatory factor; KIR, killer inhibitory receptor; LIF, leukemia inhibitory factor; M-CSF, macrophage CSF; MHC, major histocompatibility complex; MIP, macrophage inflammatory protein; NK, natural killer; PBMC, peripheral blood mononuclear cell(s); PIBF, progesterone induced blocking factor; PR, progesterone receptor; RCT, randomized controlled trial; RPL, recurrent pregnancy loss; Th, T helper; uNK, uterine NK; VEGF, vascular endothelial growth factor. Endocrine Reviews is published bimonthly by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving the endocrine community.
44
Dosiou and Giudice • NK Cells in Pregnancy and RPL
Endocrine Reviews, February 2005, 26(1):44 – 62 45
II. Peripheral NK Cells
HLA-A, HLA-B, and HLA-C expressed on any host cell; and 2) the CD94/NKG2 receptor, which recognizes the nonclassical MHC molecule, HLA-E (11).
A. Phenotype
NK cells comprise about 10 –15% of peripheral blood lymphocytes (6). They are a subset of lymphocytes with unique phenotypic characterization and functional properties. Their prototypic cell surface antigens are CD16 and CD56. CD16 is a low-affinity receptor for IgG complexes (FcRIII) and is expressed on the majority of NK cells as well as on neutrophils, a small T cell population, and some activated macrophages. CD16 is the receptor responsible for NK-mediated antibody-dependent cellular cytotoxicity. CD56 is an isoform of the neural cell adhesion molecule NCAM, expressed on essentially all NK cells, a small population of cytotoxic T lymphocytes, and some neural-derived tissues (7). Based on the intensity of CD56 expression, NK cells can be divided in two populations (8). The majority (about 90%) of peripheral blood NK cells are CD56dim and express high levels of CD16; the other 10% of peripheral blood NK cells are CD56bright and express low levels or no CD16 (8). CD56dim cells are more cytotoxic, whereas the CD56bright subset is the main source of NK cell-derived immunoregulatory cytokines (8). A comprehensive review of these two NK populations, their distinct phenotypes, and immunoregulatory functions is discussed elsewhere (8). Some receptors expressed nearly universally on NK cells include CD2, CD7, CD11b, CD18, CD38, CD45, and the IL-2R (Table 1). A variety of other antigens such as CD57, CD44, CD25, c-kit, IL-1RI, CXCR3, CXCR1, CD62L, and others are differentially expressed among NK cell subsets (7, 8). The actions of NK cells are finely regulated via a network of activating and inhibitory receptors. Several activating NK cell receptors have been identified including CD16, killer inhibitory receptor (KIR)2DS, and NKp46 (9). Upon interaction with their ligands [IgG for CD16, human leukocyte antigen (HLA)-C for KIR2DS, and unknown ligand for NKp46], these receptors transduce activating signals through transmembrane adaptor proteins such as CD3, Fc⑀RI␥, and DAP12 (9, 10). In addition to activating receptors, NK cells express a variety of inhibitory receptors that interact with class I molecules and deliver inhibitory signals to NK cells upon recognition of major histocompatibility complex (MHC)-I-bearing targets. Such receptors have been recently identified and consist of: 1) the KIRs, which recognize mainly TABLE 1. Expression of surface antigens on NK cells Antigen
Peripheral NKa (CD56dim)
uNKa (CD56bright)
CD2 (early T cell marker) CD7 (early T cell marker) CD18 (integrin) CD16 (NK marker) CD45 (hematopoietic cell) CD56 (NK marker) CD57 (NK marker) CD62L (adhesion molecule) CD69 (activation marker) KIR (NK marker) c-kit (cytokine receptor) IL-2 R (cytokine receptor)
⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹/⫺ ⫺ ⫹ ⫺ ⫹
⫹ ⫹ ⫹ ⫺ ⫹ ⫹ ⫺ ⫺ ⫹ ⫹ ⫹ ⫹
a
Predominant population is described (7, 8, 63, 65).
B. Hormonal regulation
1. Changes during the normal menstrual cycle and pregnancy in humans. There are no significant changes in the numbers of peripheral NK cells between the follicular and the luteal phases of the menstrual cycle in women (12, 13). Studies investigating changes in peripheral NK cell activity during the menstrual cycle have been equivocal, showing either no change during the cycle (13) or a reduction of NK cell activity in the luteal phase that is, however, unrelated to progesterone levels (14). During normal human pregnancy, peripheral blood NK cells decrease in number, mainly as a result of a decrease in the CD16⫹ subset (15, 16). In addition, peripheral NK cells from pregnant women exhibit decreased lytic activity compared with NK cells from controls (17). Furthermore, there is increased expression of inhibitory receptors (various KIRs including CD94/NKG2A) among peripheral T cells and NK cells in the first weeks of pregnancy, reaching a maximum within the third month of gestation, with a subsequent decline to basal levels by the end of pregnancy (18). The changes in peripheral NK cell numbers, phenotype, and activity during pregnancy suggest that NK cells are hormonally regulated. Candidate hormones for such regulation include estrogen, progesterone, and prolactin. Herein, we review the experimental evidence for such hormonal regulation, because abnormalities in this process may be underlying the changes occurring in the NK cell population in RPL. 2. Studies with estrogen in mice. Initial in vivo studies on the effects of 17-estradiol on castrated mice showed significant inhibition of NK cell activity after continuous sc exposure to estrogen for at least 4 wk (19, 20). This was believed to be due to decreased generation of NK cells from the bone marrow (19, 20). Direct addition of 17-estradiol (102 to 104 ng/ml) to lymphocytes of untreated mice in vitro did not suppress killing (19). Additional in vivo studies in mice confirmed such a suppression of NK cell activity by estrogens, which also correlated with enhancement of tumor growth or metastasis in estrogen-treated animals (21–23). A recent study of ovariectomized mice treated with estrogen confirmed the above results by demonstrating that purified splenic NK cells had a significant reduction in cytotoxicity compared with control ovariectomized animals (24). The fact that these authors, in contrast to the previous studies, used purified NK cells in their cytotoxicity assays allowed them to attribute the decreased cytotoxicity to a decrease in individual NK cell activity and not to changes in the numbers of NK cells (24). Finally, studies by Screpanti et al. (25) in mice receiving injections of 17-estradiol every other day concluded that duration of treatment determines the direction of regulation, with initial stimulation of NK cell activity, followed by suppression after 1 month of treatment. 3. In vitro studies with estrogen, progesterone, and prolactin. In vitro studies with estradiol have yielded slightly different
46
Endocrine Reviews, February 2005, 26(1):44 – 62
results. When the effects of 17-estradiol (10⫺8 to 10⫺6 m) on the human NK cell line YT-N17 (which resembles uNK cells rather than peripheral NK cells in phenotype) were studied, proliferation and NK cell activity were enhanced rather than suppressed (26). Baral et al. (27), in in vitro studies of mouse spleen NK cells against the YAC-1 murine lymphoma target, showed that incubation with estradiol (1 m) resulted in target sensitization together with effector cell inhibition, resulting overall in no change in cytolytic activity. Similarly, incubation of human peripheral blood lymphocytes with estrone, 17-estradiol, or estriol had no effect on NK cell activity (28). In summary, in vivo animal experiments have shown an inhibitory role of estrogen on peripheral NK cell lytic activity, which is partly due to suppression of NK cell output by the bone marrow and partly due to suppression of individual NK cell cytotoxicity. However, in vitro studies so far have failed to show conclusively a direct effect of estrogen on NK cells. Progesterone has long been considered “nature’s immunosuppressant” (29). Early studies suggested a dose-dependent decrease in peripheral NK activity by progesterone, with lymphocytes of pregnant women being the most sensitive targets of cytotoxicity suppression by progesterone at concentrations of 40 –500 nm (30). Subsequent experiments by Sulke et al. (31) showed some inhibition of lymphocyte cytotoxicity by estradiol and progesterone that was significant at supraphysiological hormone levels but was attributed by the authors to a nonspecific effect of the solvent ethanol. Uksila (28) showed no effect of progesterone (1–1000 nm) or estradiol (1–1000 nm) on NK cell activity. In a more recent study by Inoue et al. (32), culture of peripheral blood mononuclear cells (PBMC) with progesterone (10⫺6 m) had no effect on CD56⫹ proliferation. However, additional studies of peripheral blood lymphocytes using higher progesterone concentrations such as those present at the maternal-fetal interface (10⫺5 m) showed significant inhibition of lymphocyte proliferation in vitro, an effect not observed with lower progesterone concentrations (33). Furthermore, RU 486, a potent antiprogestin, has been shown to significantly augment NK cell cytolytic activity in vitro; this down-regulation is effectively blocked by progesterone at a concentration of 25 m (34). The discrepancies in the above studies may be attributable to the different doses of progesterone used. At the progesterone concentrations believed to be present in the uterus [up to 10⫺5 m at the maternal-fetal interface (35)], studies consistently show inhibition of lymphocyte proliferation (33) and inhibition of NK cytolytic activity in vitro (34). Prolactin is another hormone that has been implicated in the regulation of the immune system. Hyperprolactinemic states in vivo have been associated with either normal or depressed NK cell numbers and activity (36, 37). In vitro, prolactin stimulates peripheral NK cell proliferation and response to IL-2 at physiological concentrations, but inhibits response to IL-2 at high concentrations (38). This may explain the above observation of depression of NK cell numbers/ activity in hyperprolactinemic states in vivo. The prolactin receptor has been identified in peripheral NK cells in the rat (39) and human (40). The exact role of prolactin in NK cell regulation is unknown. Studies of PRL⫺/⫺ and PRLR⫺/⫺
Dosiou and Giudice • NK Cells in Pregnancy and RPL
mice suggest that prolactin is not essential in the development of the immune system and effective immune response in the mouse (41, 42); however, in those knockout mice different cytokines may compensate for the absence of prolactin and/or its receptor, and additional studies (e.g., reconstitution or replacement) are warranted. 4. Potential mechanisms. The effect of hormones on peripheral NK cells could be either direct, through receptors on NK cells, or indirect, through action on neighboring cells. a. Direct NK cell effect. In studies of peripheral NK cells, estrogen receptor ␣ (ER␣) and ER have been recently identified in splenic NK cells in the mouse (24). When ER␣knockout mice were treated with high doses of estradiol, they showed similar decrease in NK cell activity to controls, arguing for a role of ER or a novel receptor in mediating an inhibitory estrogen action on NK cells (24). On the other hand, there is evidence to suggest that estrogen may have an indirect stimulatory effect on NK cells, likely through action on ER␣-expressing T cells, as discussed in Section II.B.4.b. The overall effects of estrogen on NK cells are likely multifactorial, therefore, and depend on the type of cell affected as well as the kind of ER expressed by that cell. Review of the literature suggests that expression of progesterone receptors (PRs) by peripheral NK cells has not been examined. It is possible that progesterone action on NK cells is not through a classical steroid receptor pathway, but rather through direct effects on voltage-gated and calcium-activated K⫹ channels. The latter have been demonstrated to mediate the immunosuppressive effect of progesterone on T lymphocytes (43). It has also been suggested that the action of progesterone on T cells may be partly through the glucocorticoid receptor (GR) (44); such a mechanism is also possible in uNK cells, which express GR (45). Finally, progesterone may exert its actions through membrane receptors, which have been recently identified in spotted sea trout oocytes, but not yet identified in the immune system (46). b. T lymphocytes. In addition to direct effects of the hormonal system on NK cells, hormones could influence NK cells indirectly, via action on other cells that serve as intermediaries. In the periphery, the intermediaries could be T lymphocytes. T helper (CD4⫹) lymphocytes can be classified as either T helper 1 (Th1) or Th2, depending on their cytokine profile and their function (47– 49). Th1 cells predominantly produce interferon-␥ (IFN-␥), IL-2, and TNF- and are involved in cell-mediated immunity. Th2 cells produce IL-4, IL-5, IL-6, IL-10, and IL-13 and stimulate humoral immunity. Th1 cytokines inhibit Th2 cell proliferation, whereas Th2 cytokines block activation of Th1 cells (48). It is known that progesterone can directly affect T cell differentiation in vitro, suppressing development of the Th1 pathway and enhancing differentiation along the Th2 pathway (44). Th2 cytokines are believed to have various effects on NK cells, including inhibition of NK cell binding and cytotoxicity to vascular endothelium (50), inhibition of NK cell proliferation (51), and skewing of NK cell cytokine production toward a Th2 phenotype (52, 53) (Fig. 1). Furthermore, in response to progesterone, ␥␦ T cells produce progesterone-induced blocking
Dosiou and Giudice • NK Cells in Pregnancy and RPL
Endocrine Reviews, February 2005, 26(1):44 – 62 47
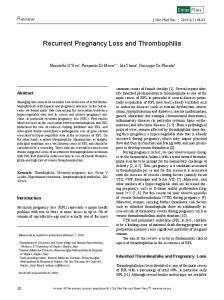
FIG. 1. A model of hormonal regulation of NK cells in pregnancy. In pregnancy, progesterone causes a decrease in peripheral NK cell numbers, activation, and cytotoxicity via direct action on NK cells and/or through promoting Th2 cytokine and PIBF production by T cells. It also facilitates NK cell homing to the endometrium, via inducing expression of homing receptors and addressins on peripheral NK cells and the endometrium, respectively, and possibly through induction of VEGF and MIP-1 expression by the endometrium. Endometrial stromal cells, under the influence of progesterone, produce IL-15, prolactin, and likely other unidentified factors, which may regulate uNK cell proliferation, differentiation, and production of cytokines and other molecules that support placental and trophoblast development and promote local immunomodulation. E, CD56bright CD16⫺ NK cells; , CD56dim CD16⫹ NK cells.
factor (PIBF) (54), which has been shown in mice to inhibit NK cell activity and have antiabortive effects (55). PIBF has been recently cloned and has been shown to enhance IL-10 production and suppress IL-12 production by human peripheral lymphocytes as well as to inhibit NK cytotoxic activity in vitro (56). In contrast, the effects of estrogen on T cells should theoretically result in NK cell stimulation rather than inhibition. In a recent study involving ER␣-knockout mice, estradiol has been shown to selectively enhance the development of IFN-␥-producing T cells through an ER␣-dependent mechanism (57). In fact, estrogen is known to increase activity of the IFN-␥ promoter and cause increased expression of IFN-␥ mRNA in concanavalin A-treated murine spleen cells (58). Through promoting IFN-␥ production by T cells, estrogen may, therefore, enhance peripheral NK cell function. This effect has not been observed in vivo in the studies described above; however, it is possible that the indirect stimulatory effect of estrogen is overridden by its direct inhibitory effect on NK cell activity. In summary, there is some evidence of hormonal regulation of peripheral NK cells (Fig. 1). This regulation may occur through direct actions of estrogen through ERs in peripheral NK cells, through direct actions of progesterone via an as yet unidentified receptor or receptor-independent mechanism, or through indirect pathways. These would involve progesterone action on peripheral T cells which could act through cytokines on peripheral NK cells. Still, the exact pathways of hormonal regulation of NK cells are a subject for future research.
C. Function
A defining characteristic of NK cells is their ability to lyse target cells without prior sensitization and without restriction by HLA antigens. Their functions involve: 1) antiviral activity; 2) anti-neoplastic activity; 3) regulation of hematopoiesis; and 4) graft-vs.-leukemia effect after bone marrow transplantation (6). Under resting conditions, peripheral NK cells express few cytokines; however, they can be induced to express granulocyte-macrophage colony-stimulating factor (GM-CSF), macrophage CSF (M-CSF), IL-3, IFN-␥, TNF-␣, and TNF- with various stimuli (59 – 61). Soluble mediators such as TNF-␣ and IFN-␥, secreted by activated NK cells, play important roles in induction of apoptosis and additional regulation of the immune response, respectively (6). NK cell function is mainly regulated by IL-2 and IFN-␥. IL-2 causes both NK cell proliferation and enhanced cytotoxicity. IFN-␥ augments NK cytolytic activity, but does not cause NK proliferation. The two cytokines act synergistically to augment NK cytotoxicity (6). III. uNK Cells: A Unique NK Cell Subset
Human uterine endometrium hosts a significant number of leukocytes, the percentage and phenotype of which change during the menstrual cycle. Leukocytes account for about 10% of stromal cells in the proliferative phase, 20% in the secretory phase, and 30% of endometrial stromal cells in early pregnancy (decidua) (62). The largest leukocyte pop-
48
Endocrine Reviews, February 2005, 26(1):44 – 62
ulation in the endometrium consists of NK cells named large granulated lymphocytes. These cells comprise over 70% of endometrial leukocytes in first trimester decidua (62). A. Phenotype
uNK cells resemble the dominant CD56 population of peripheral blood NK cells in some phenotypic characteristics; however, they have some phenotypic and functional differences (Table 1). They express CD56 as well as the killer activatory and inhibitory receptors, but lack expression of other typical NK markers such as CD16 or CD57 (63). They express early T cell markers such as CD2 and CD7, integrins such as CD11a and CD18, and IL-2R (64, 65). In addition, in contrast to the majority of peripheral NK cells, uNK cells express CD69, an early activation marker (64, 65). Given the high levels of CD56 expression in uNK, it has been suggested that they derive from the small CD56bright population in peripheral blood. There are some phenotypic differences between these two populations, most notably, uNK are KIR⫹, CD69⫹, CD62L⫺, whereas CD56bright peripheral NK cells are KIR⫺, CD69⫺, and CD62L⫹ (reviewed in Ref. 66). A recent microarray analysis comparing gene expression between the dominant uNK population (CD56bright) in the decidua with the CD56bright and CD56dim peripheral NK cell subsets identified significant differences, including selective expression of CD9, galectin-1, and glycodelin, in the decidual NK population but not in peripheral blood NK cells (67). uNK cells also were found to express significantly higher levels of multiple other genes, including tetraspanins, integrins, lectin-like receptors, and KIRs compared with peripheral CD56bright cells (67). This important study has provided an opportunity to mine functional differences of the CD56bright uNK and CD56bright peripheral blood populations. B. Hormonal regulation
1. Changes during the normal menstrual cycle and pregnancy in humans. Several changes occur in uNK cells during the normal menstrual cycle and human pregnancy. First, there is a significant increase in the number of uNK cells throughout the secretory phase, which peaks in early pregnancy when uNK cells comprise about 75% of uterine leukocytes (62). At the same time, as described above, the proportion of leukocytes in the endometrial stromal cell population more than triples between the proliferative phase and early pregnancy decidua (62). Second, uNK cell phenotype changes during the normal menstrual cycle and early pregnancy (68). Expression of the activation antigens CD69 and HLA-DR as well as of leukocyte function-associated antigen-1 molecules CD11a and CD18 is highest in the proliferative phase and decreases gradually during the menstrual cycle (68). Similarly, in pregnancy there is a decrease in expression of many markers of activation such as CD69, HLA-DR, as well as leukocyte function-associated antigen-1 and CD45RA by uNK cells (68). In addition, almost all uNK cells have been found to express one or more inhibitory receptors in early pregnancy (18).
Dosiou and Giudice • NK Cells in Pregnancy and RPL
2. In vivo mouse studies. Experiments in the mouse have shown that, at least in the murine model, the increase in uNK cell numbers during pregnancy is mainly due to recruitment of uNK cell precursors from the spleen, lymph nodes, and bone marrow, and not from self-renewal of the existing uNK population (69). The suggested mediators and intermediary cells involved in this process are discussed in Section III.B.4.c. Other in vivo studies of the role of estrogen and progesterone in the regulation of the uterine immune environment in PR knockout mice have demonstrated a general proinflammatory effect of estrogen, causing an influx of macrophages and neutrophils, which is antagonized by progesterone through its receptor (70, 71). The mechanism of such a progesterone-induced local immunosuppression is unclear. Hoxa-10, expressed by endometrial stromal cells under the influence of progesterone, has been recently implicated as an immunoregulatory mediator, because Hoxa-10 deficient mice exhibit, among other defects, significant proliferation of T cells in the periimplantation uterus (72). Whether and how the uNK cells contribute to the creation of a locally immunosuppressive environment and whether such activity is hormonally regulated has not been completely delineated. However, recent studies suggest both direct and indirect potential mechanisms of hormonal involvement, reviewed below (Section III.B.4.c). 3. In vitro studies. In vitro studies also provide supporting evidence for hormonal regulation of uNK cells. Culture of endometrial leukocytes in the presence of progesterone (10⫺8 to 10⫺6 m) results in expansion of the CD56⫹ population, whereas culture with prolactin, estradiol, or human chorionic gonadotropin (hCG) does not induce CD56⫹ cell proliferation (32). This study suggests that progesterone plays an important role in proliferation and differentiation of uNK cells (32). However, culture of highly purified endometrial CD56bright CD16neg NK cells with 17-estradiol or progesterone (10⫺6 m) has no effect on their proliferation, cytotoxicity, or IFN-␥ and TNF-␣ production (73). The discrepancy in the above studies could be due to an indirect effect of progesterone on uNK cells, via action on intermediary immune cells, such as T lymphocytes. Interestingly, no studies have examined the effect of progesterone on uNK at the highest progesterone concentrations (10⫺5 m), which are believed to be present in the uterus (35). Prolactin may also regulate uNK cell function and is discussed in Section III.B.4.c. 4. Potential mechanisms a. Direct uNK cell effect. In search of evidence for a direct hormonal effect on uNK cells, subsequent studies in the late 1990s attempted to identify the PR or ER␣ in human uNK cells but failed to do so (74, 75). However, after discovery of ER in 1996, Henderson et al. (45) identified steroid receptor expression in purified uNK cells. These cells were shown to have mRNA for ERcx/2, ER1, and the GR, but were negative for ER␣ and PR, confirming previous reports (Table 2). With dual immunofluorescent localization, protein expression of ER1 and GR was verified in uNK cells (45). Despite this discovery, the role, if any, of ER in uNK remains unclear. ER expression by uNK precursor cells does not seem to be necessary for their homing and differentiation poten-
Dosiou and Giudice • NK Cells in Pregnancy and RPL
Endocrine Reviews, February 2005, 26(1):44 – 62 49
TABLE 2. Expression of hormone receptors on NK cells
Similar modulation of its expression may be present in uNK cells and awaits experimental validation. In addition to direct hormonal regulation of uNK cells, there may be indirect hormonal regulation of uNK cell function, through hormonal effects on intermediary cells. Two such cell types in the endometrial environment are good candidates as hormonal targets: T lymphocytes and endometrial stromal cells.
Peripheral NK uNK
ER␣/ER
PR
PRLR
GR
⫹/⫹ ⫺/⫹a
?b ⫺
⫹ ⫹
⫹ ⫹
PRLR, Prolactin receptor. Refs. 24, 39, 40, 45, 74, 75, and 92. a ER1⫹, ERcx/2⫹. b Not studied.
tial, because bone marrow from ER␣-knockout (␣ERKO) and ERKO mice transplanted into RAG-2⫺/⫺/␥c⫺/⫺ mice, which lack all lymphocyte lineages, reconstitutes successfully the uNK population (76). Although the reconstituted uNK cells are capable of triggering appropriate modification of spiral arteries in the uterus (76), their functionality has not been fully assessed. Therefore, studies so far have not conclusively ruled out a role for ER in uNK cell function. One of the direct effects of female sex steroids on uNK cells may be regulation of gene expression of immunomodulatory proteins. As mentioned earlier, glycodelin is one of the genes selectively expressed by the human decidual NK population, and not by the peripheral CD56⫹ NK cells (67). Glycodelin is known to be a product of secretory endometrial glands, appearing first on the third day after the midcycle LH surge (d 16), whereas it is not expressed in proliferative endometrium (reviewed in Ref. 77). Its expression is believed to be up-regulated by progesterone, given its temporal regulation [expression 14.6 ⫻ higher on d 20 –24 compared with d 8 –10 of the cycle (78)], the presence of several progesterone response elements in its gene, and up-regulation in endometrial epithelial cells by progesterone in vitro (77). It is therefore likely that uNK cell production of glycodelin is increased by progesterone in the luteal phase of the cycle and in early pregnancy, providing another level of local immunosuppression at the maternal-fetal interface. It is also possible that other immunomodulatory substances produced by NK cells are also hormonally regulated. The expression of galectin-1, an immunosuppressant recently shown to be significantly up-regulated in the decidual NK population (67), is regulated by estrogen and progesterone in mouse uterine tissues (79).
b. T lymphocytes. T lymphocytes can regulate the cytokine environment in the endometrium. Th2 cytokines have also been shown to be present in periimplantation human endometrium (80) and at the maternal-fetal interface in the mouse (81), where they are believed to play a key role in the uterine cytokine network of pregnancy (63). Through promotion of a uterine Th2 environment, progesterone could indirectly affect uNK cell function, as described in Section II.B.4.b. c. Endometrial stromal cells. As described above, female sex steroids appear to regulate the number of uNK cells, as suggested by the temporal changes of uNK cell numbers during the menstrual cycle and pregnancy. The mechanism of this increase in uNK cell numbers has been addressed in both human and mouse models, and is likely the result of: 1) recruitment of peripheral NK cells to the uterus, and 2) proliferation of existing uNK cells (Table 3 and Fig. 1). Both of these processes involve endometrial stromal cells as intermediaries. Both human and animal studies support this hypothesis (see below). Human studies have suggested a potential role of macrophage inflammatory protein-1 (MIP-1) and vascular endothelial growth factor (VEGF) in the process of uterine recruitment of peripheral NK cells. MIP-1 is a chemokine with strong chemoattractant properties for peripheral blood NK cells. Progesterone is known to up-regulate production of MIP-1 in human endometrium (82). MIP-1 expression in human endometrium increases in the secretory phase, and there is strong correlation between its levels and the number of uNK cells (82). Furthermore, its secretion by cultured endometrial stromal cells can be induced in vitro by proges-
TABLE 3. Potential mechanisms of hormonal modulation of uNK cells Hormone
Progesterone
Estrogen
Prolactin
Mechanism
Study
bright
1. Promotion of CD56 NK cell homing to the uterus Enhancement of MIP-1 production by endometrial stromal cells Up-regulation of VEGF production by endometrial stromal cells Up-regulation of L-selectin and ␣4 integrin-dependent adhesion pathways for circulating CD56bright NK cells 2. Proliferation of endogenous uNK cells in situ Up-regulation of IL-15 production by endometrial stromal cells Up-regulation of cytokine production by endometrial lymphocyte populations that then induce uNK proliferation 3. Up-regulation of production of immunomodulatory molecules such as glycodelin by uNK 4. Induction of Th2 immune environment, resulting in alteration of uNK cytokine production and/or function Promotion of CD56bright NK cell homing to the uterus Up-regulation of L-selectin and ␣4 integrin-dependent adhesion pathways for circulating CD56bright NK cells
Kitaya et al., 2003 (82) Popovici et al., 2000 (85); Ancelin et al., 2002 (84) Chantakru et al., 2003 (86) Okada et al., 2000 (88); Verma et al., 2000 (89) Inoue et al., 1996 (32) Seppala et al., 2002 (77); Koopman et al., 2003 (67) Piccinni et al., 1998 (162)
Chantakru et al., 2003 (86)
Differentiation/maturation of uNK cells, possibly through stimulation of Ohteki et al., 1998 (94); Gubbay et al., 2002 (92) IRF-1 production by endometrial stromal cells, or via direct effect on uNK cells
50
Endocrine Reviews, February 2005, 26(1):44 – 62
terone. The specific receptor for MIP-1, CCR5, is strongly expressed by uNK, suggesting a functional role for MIP-1 as a chemoattractant for CD56bright NK cells to the uterus (83). All these features make MIP-1 an attractive candidate for uNK recruitment in human pregnancy (82). Progesterone has also been shown to stimulate VEGF and VEGF receptor expression by human endometrial stromal cells in an in vitro model of decidualization (84, 85). Through this mechanism, it may stimulate angiogenesis and increase tissue permeability of the secretory endometrium, facilitating peripheral NK cell homing (Fig. 1). In mouse models, both estrogen and progesterone have been shown to facilitate CD56bright cell homing to murine uterine tissue by up-regulating l-selectin and ␣4 integrindependent pathways, both on vascular endothelium and on the lymphocytes themselves (86). The role of MIP-1 in the mouse is less clear, however, because spleen cells from pregnant CCR5⫺/⫺ mice, which lack the receptor for MIP-1, can successfully reconstitute the uNK population in mice, suggesting that MIP-1 is not necessary for pre-uNK cell recruitment to the uterus in murine pregnancy (69). Under the influence of progesterone, endometrial stromal cells can also enhance proliferation and maturation of the existing uNK population through production of IL-15 and prolactin. It is known that IL-15 mRNA expression significantly increases during the secretory phase of the human endometrium, at the time of high progesterone levels (87). In in vitro studies of human endometrial stromal cells, incubation with either progesterone or a combination of progesterone and estradiol has resulted in enhancement of IL-15 production (88). Furthermore, human decidual NK cells express the IL-15 receptor and in response to IL-15 proliferate and augment their cytolytic activity against K562 (89). Because IL-2 is normally absent from the decidual microenvironment, it is likely that IL-15 is the cytokine responsible for uNK cell proliferation in vivo; it may therefore contribute to the increase in uNK cell numbers in the luteal and early pregnancy endometrium by stimulating uNK proliferation. Prolactin is produced by endometrial stromal cells between the midsecretory phase and menses, and in the event of pregnancy prolactin synthesis increases significantly to a peak around 20 –25 wk gestation (90). Expression of the prolactin receptor is localized to the stromal and glandular compartments and follows a similar temporal pattern as prolactin expression (91). It is therefore believed that the prolactin system plays an important role in implantation and the maintenance of pregnancy. The above pattern of expression coincides with the temporal increase in the numbers of uNK during the luteal phase and in pregnancy, suggesting a possible role of prolactin in that process. The exact function of prolactin on uNK cells remains to be defined, although it may regulate cell proliferation or NK maturation (92). These effects are likely through both direct and indirect mechanisms. Prolactin has been recently shown to induce phosphorylation of ERK in glandular epithelial cells and a number of endometrial cells including uNK cells (92). The prolactin receptor was identified in uNK cells by in situ immunofluorescence and in purified decidual NK cells by real-time PCR and Western blot analysis (92). Therefore, through inducing ERK phosphorylation directly on uNK cells, prolactin may reg-
Dosiou and Giudice • NK Cells in Pregnancy and RPL
ulate their differentiation and proliferation. In addition, prolactin stimulates production of IFN-regulatory factor-1 (IRF-1) by glandular epithelial cells (93). IRF-1 has been shown to be important for the maturation of peripheral NK cells (94) and is believed to be essential in supporting development of NK cells through transcriptional regulation of the IL-15 gene in the bone marrow microenvironment (95). However, the importance of IRF-1 regulation of IL-15 transcription in the uterus has recently been questioned in a mouse model, where the abnormalities seen in uNK cells in IRF-1⫺/⫺ mice (decreased in numbers, small, and hypogranular) were not reversed after treatment with IL-15 (96). Furthermore, IL-15 mRNA expression at implantation sites of pregnant IRF-1⫺/⫺ animals were similar to controls (96). IRF-1 may therefore affect uNK cell proliferation and maturation in other ways. Mechanisms such as up-regulation of addressins or other genes involved in uNK recruitment and homing to the uterus (e.g., vascular cell adhesion molecule) have been postulated (96, 97). Alternatively, IRF-1 could stimulate production of an as yet unidentified cytokine affecting uNK growth and development. Although the precise network of endometrial cytokines continues to be elucidated, a central role of prolactin in paracrine actions in human endometrium is intriguing and warrants additional investigation. Another member of the prolactin family, prolactin-like protein A, which is expressed by trophoblast cells, has been shown to bind to uNK cells in the rat and suppress cytolytic activities of a rat NK cell line in vitro (98). Its function in possible regulation of uNK cells in pregnancy also warrants additional investigation. In summary, there is considerable evidence of hormonal regulation uNK cells (Table 3 and Fig. 1). This regulation may occur through direct actions of estrogen through ERs that have been identified in uNK cells, through direct actions of progesterone via an as yet unidentified receptor or receptorindependent mechanism, or through indirect pathways. These could involve progesterone action on endometrial T cells and stromal cells. The latter could act through VEGF and MIP-1 to enhance recruitment of peripheral NK cells to the uterus, as well as through prolactin, IL-15, and other, as yet unidentified mediators to increase proliferation and differentiation of uNK cells (Fig. 1). Although these are attractive hypotheses, the exact pathways of hormonal regulation of NK cells remain to be delineated. C. Function
There are important functional differences between uNK and peripheral NK cells. In contrast to peripheral NK cells, decidual uNK cells exhibit weak lytic activity against the standard NK-sensitive target K562 (99, 100). However, they can be readily activated after IL-2 stimulation to kill effectively trophoblast cells, which are normally resistant to lysis (101). Finally, uNK cells express a different cytokine profile, compared with resting peripheral NK cells. mRNAs for granulocyte CSF, M-CSF, GM-CSF, TNF-␣, IFN-␥, TGF-, and leukemia inhibitory factor (LIF) have been found in decidual CD56⫹ cells (102, 103); in contrast, mRNAs for only TNF-␣ and TGF-1 are detected in peripheral blood NK cells in their resting state (102).
Dosiou and Giudice • NK Cells in Pregnancy and RPL
The exact function of uNK cells has not yet been unequivocally determined. In nonpregnant endometrium, there is a significant increase in the numbers of these cells from the midsecretory phase onward, where they are found close to stromal cells and around glands and blood vessels. Therefore, their involvement in the initiation of the process of decidualization has been suggested (104). In the absence of pregnancy, uNK cells undergo characteristic nuclear changes resembling apoptosis (105); it has therefore been proposed that their death may play an early role in endometrial breakdown occurring at menstruation (104, 105). During human pregnancy, they are found in close proximity to the implantation site, in close contact with the infiltrating extravillous trophoblast. Their increased numbers in early pregnancy, their hormonal dependence, and their close proximity to the infiltrating trophoblast all suggest that they play an important role in the regulation of the maternal immune response to the fetal allograft and the control of trophoblast growth and invasion during human pregnancy. In addition, studies of genetically modified mice as well as in vitro experiments suggest an important role of uNK cells in regulation of placental development. 1. Differences between human and mouse uNK cells. Some insights into the function of uNK cells have come from experiments in mice. It is important to note, however, that there are fundamental differences in uNK cells between mice and humans (reviewed extensively in Ref. 66). In humans, uNK cells are present in nonpregnant endometrium, increase in numbers during each menstrual cycle, and infiltrate diffusely throughout the decidua. In addition, in humans there is extensive invasion of the trophoblast into the decidual arteries and stroma. In contrast, murine uNK cells are present only in the pregnant decidua and are not present in nonpregnant endometrium. They are confined to the mesometrial side of implantation sites and are not present diffusely. Furthermore, in the early phase of mouse implantation, there is minimal invasion of the trophoblast into the decidual arteries and stroma (66). Given these differences, results from
Endocrine Reviews, February 2005, 26(1):44 – 62 51
animal studies should be interpreted with caution in extrapolation to humans. Nevertheless, animal experiments have revealed some interesting aspects of uNK biology that may give insight into their functions in humans. These are summarized below. 2. Insights from genetically modified mice. Early attempts to deplete NK cells in mice using antibodies targeting NK cell precursors had no effect on pregnancy outcome when given during the implantation period (106). Other experiments involving modulation of NK cell activity with various antibody treatments in pregnant mice documented that enhancement of NK cell activity was associated with an increase in fetal resorption rate, whereas suppression of NK cell activity was associated with decreased rates of resorption (107). However, a more definitive answer regarding the function of uNK cells in the murine pregnancy came from genetically modified mice lacking NK cell function. Studies of transgenic mice that are deficient in NK cells have demonstrated that NK cells play an important role in the normal development of the placental vasculature. Five strains with different gene defects, including TgE26 transgenics, RAG-2⫺/⫺/␥c⫺/⫺, IL-15⫺/⫺, p56lck⫺/⫺/IL-2R⫺/⫺, and IL-2R␥⫺/⫺ have been examined (96, 106, 108 –112). They all lack uNK cells and fail to form the mesometrial lymphoid aggregate of pregnancy. They all have hypocellularity and edema of the decidua basalis and have abnormal thickening of the spiral arteries (reviewed in Ref. 110). Despite these abnormalities, most of these strains have normal pregnancies and no fetal loss (Table 4). To prove that the abnormalities seen in these mice are due to a deficiency of uNK cells, reconstitution experiments using bone marrow from B and T cell-deficient severe combined immunodeficient donors, which have intact NK cell lineage, were performed (109). After engraftment, the implantation site abnormalities described above were reversed (109). Similar reconstitution studies of bone marrow transplantation from severe combined immunodeficient donors into RAG-2⫺/⫺/␥c⫺/⫺ mouse recipients (which lack NK, T, and B cells) reversed the
TABLE 4. Implantation site phenotype and pregnancy outcome in strains of genetically mutant mice lacking uNK cells Implantation site phenotype
Pregnancy outcome
TgE26
Strain
No metrial gland Acellular and edematous decidua Thick vessel walls Small placentae
64% fetal loss at midgestation
RAG-2⫺/⫺/␥c⫺/⫺
No metrial gland Hypocellular decidua Thickening of decidual arteries
No effect
IL-15⫺/⫺
No metrial gland Hypocellular decidua Thickening of decidual arteries
No effect on litter size Slight decrease in fetal weight
p56lck⫺/⫺/IL-2R⫺/⫺
No metrial gland Hypocellular decidua Thickening of decidual arteries Small placentae
Not reported
IL-2R␥⫺/⫺
No metrial gland Hypocellular decidua Thickening of decidual arteries Small placentae
Not reported
Refs. 96, 106, and 108 –112.
52
Endocrine Reviews, February 2005, 26(1):44 – 62
reproductive anomalies of the NK-deficient animals cited above (112). These experiments using transgenic mice lacking NK cells demonstrate that uNK cells play a role in spiral artery modification in the placenta; however, their function is not required for successful pregnancy. In support of the latter, IL-15⫺/⫺ mice, which completely lack uNK cells in their decidua resulting in the known decidual abnormalities described above, have normal gestation times and litter sizes, with only a mild reduction in fetal weight (111). Therefore, at least in the mouse, although uNK cells are important in normal development of the placental vasculature, they are not required for a successful pregnancy (111). Whether cytokines or other factors from uNK cells can derive partially from the endometrial stroma to rescue the phenotype remains to be determined. Additional experiments with knockout animals have identified a main mediator of uNK cell function in the mouse to be IFN-␥. IFN-␥ knockout mice show significant abnormalities in the decidual vasculature, similar to those observed in NK cell-deficient mice (112). Reconstitution of RAG-2⫺/⫺/ ␥c⫺/⫺ mice with bone marrow from IFN-␥⫺/⫺ mice, which restores normal numbers of uNK cells that are, however, unable to produce IFN-␥, does not reverse the decidual abnormalities (112). On the contrary, IFN-␥ administration to these animals reverses the decidual pathology, supporting a major role of IFN-␥ in uterine vascular remodeling during pregnancy (112). A recent study of IL-12⫺/⫺ and IL-18⫺/⫺ mice has established the importance of IL-12 and IL-18 together in the induction of IFN-␥ synthesis and subsequent pregnancy-induced spiral artery modification (113). From the above, it seems that although uNK cells are important in the development of a normal placental vasculature in the mouse, they are not necessary for a normal murine pregnancy. It could be that other mechanisms compensate for the uNK cell absence in that species. Nevertheless, the mouse model provides important information about uNK cells and cytokine networks in early pregnancy. However, whether it reflects what is occurring in normal and abnormal human pregnancy, in which placentation and vascular development differ from the mouse model, remains to be determined. 3. Potential functions in humans. Although in vivo data from humans are lacking, there have been a number of in vitro studies of human uNK cells that suggest three main potential functions of this cell population in the endometrium. These are discussed below. Most of these in vitro studies involve human uNK cells; a few studies using murine or rat uNK cells are also described, as necessary. a. Regulation of placental and trophoblast growth by cytokines. Human uNK cells are known to produce many cytokines that may influence the decidual and trophoblast microenvironment. As mentioned earlier, mRNAs for granulocyte CSF, M-CSF, GM-CSF, TNF-␣, IFN-␥, TGF-, and LIF have been found in human decidual CD56⫹ cells (102, 103). Receptors for GM-CSF, CSF-1, IFN-␥, and TNF-␣ have been demonstrated on human trophoblast cells, arguing for a role of uNK cell-derived cytokines on trophoblast growth and differentiation (114 –117). GM-CSF has been shown to increase [3H]thymidine up-
Dosiou and Giudice • NK Cells in Pregnancy and RPL
take by human trophoblast cells in culture (118) and stimulate DNA synthesis in cultures of murine trophoblast (119). CSF-1 increases production of hCG and human placental lactogen by the human trophoblast (120). In addition, both GM-CSF and CSF-1 have been shown to cause placental cell proliferation in a mouse model (121). TNF-␣ can inhibit DNA synthesis in human and rat trophoblast cell lines (122, 123). TGF- has been shown to suppress human trophoblast invasion in vitro through the induction of tissue inhibitors of metalloproteinases (124). LIF likely also plays an important role in implantation, because mice lacking a functional LIF gene cannot undergo implantation, whereas their blastocysts can successfully implant in pseudopregnant recipients (125). In addition to its effects on the placental vasculature in the mouse, IFN-␥ induces human trophoblast cells to become partially protected from lysis by IL-2-stimulated decidual NK cells (126). b. Local immunomodulation. Local immunomodulation is another potential function of the human uNK population. The recent analysis of gene expression of human decidual NK cells reporting overexpression of molecules with immunomodulatory potential such as galectin-1 and glycodelin A (67) supports such regulation of the immune uterine milieu by uNK. Galectin-1, a member of the galectin family, is known to inhibit T cell proliferation and survival and affect the cytokine environment by decreasing TNF-␣, IL-2, and IFN-␥ production from activated T cells and IL-12 production from infected macrophages (reviewed in Ref. 127). Glycodelin (also known as placental protein 14; progesterone-associated endometrial protein) has important immunoinhibitory properties (reviewed in Ref. 128); its mechanism of downregulation of T cell activation was recently described (129). c. Control of trophoblast invasion. A third potential role for uNK cells has been control of trophoblast invasion via cellmediated cytotoxicity. However, there is little evidence to support such a role. Human uNK cells are capable of cytotoxicity against classical NK cell targets such as K562, although to a reduced extent compared with peripheral NK cells (130, 131). Human trophoblast cells are resistant to lysis by decidual NK cells, unless the latter have been stimulated by IL-2 (101); however, IL-2 is not present in the endometrium to any great extent during normal human pregnancy (102). Although MHC class I molecules such as HLA-C, HLA-E, and HLA-G, capable of delivering inhibitory signals to NK cells, are present on trophoblast cells, antibodies blocking these interactions do not reverse the inhibition of trophoblast lysis, arguing for a different mechanism of trophoblast resistance to uNK-mediated lysis (66). Furthermore, mice lacking NK cytotoxic ability (beige mice and perforin knockout mice) have normal implantation sites and pregnancy outcomes (132, 133). It therefore seems unlikely that cytotoxicity against trophoblast is under normal conditions a primary function of uNK cells. In summary, uNK cells produce a variety of cytokines capable of directly influencing trophoblast growth and hormone production as well as implantation and vascularization of the decidua. In addition, they are capable of producing immunomodulatory proteins and may therefore play a role
Dosiou and Giudice • NK Cells in Pregnancy and RPL
in immunoregulation at the maternal-fetal interface. In genetically modified mice lacking uNK cells, pregnancy outcome is not compromised; therefore, at least in the mouse, uNK cell function is not necessary for a normal pregnancy. Whether uNK cells are necessary in the course of a normal human pregnancy remains to be determined. IV. NK Cells in RPL
Given the evidence for modulation of NK cells by the hormonal system as well as the involvement of uNK cells in normal pregnancy, NK cells have been the focus of investigation of many studies trying to understand the pathophysiology of unexplained RPL. Both peripheral NK cells and uNK cells have been examined. Evidence for a role of NK cells in the pathogenesis of unexplained RPL is described below. A. Peripheral NK cells in RPL
1. Role in Th1 immunity. It has been suggested that cellmediated (Th1) immunity toward trophoblast cells is suppressed in normal pregnancy, and that perhaps failure of such suppression contributes to loss of the pregnancy in cases of unexplained RPL. In support of this theory, PBMC from over 50% of women with a history of unexplained RPL have been shown to respond to trophoblast extracts in vitro by both proliferating and releasing embryotoxic factors that adversely affect embryo growth, whereas cells from women with normal pregnancies do not show such a response (134). In response to trophoblast antigens, PBMC from women with
Endocrine Reviews, February 2005, 26(1):44 – 62 53
RPL have been shown to produce IFN-␥, TNF-␣, and TNF-, whereas PBMC of reproductively normal women produce IL-10 instead (135). In addition, after in vitro stimulation of PBMC with phorbol myristate acetate and ionomycin, CD3⫹ CD8⫺ T helper cells from women with RPL have significantly higher Th1/Th2 cytokine ratios of IFN-␥/IL-4, TNF␣/IL-4, and TNF-␣/IL-10 compared with control multiparous women (136). The above findings suggest that Th1 immunity to trophoblast is associated with RPL, whereas Th2 immunity is associated with a successful pregnancy (135). Several other studies have verified this Th1/Th2 bias by showing a Th1 cytokine profile in mitogen-activated PBMC (137) and PBMC activated with placental antigens (138) in women with RPL, compared with a Th2 profile in women with successful pregnancies. Such Th1 immunity against trophoblast is inhibited by addition of progesterone in in vitro PBMC/trophoblast cocultures (139). A recent study identified NK cells together with T cells to be responsible for Th1 immunity against trophoblast (140). PBMC from women with RPL were cultured with and without a trophoblast extract, supernatants from these cultures were added to two cell mouse embryos, and blastocyst development was assessed. Cell preparations enriched for T cells or NK cells yielded supernatants that significantly inhibited blastocyst development compared with supernatants enriched for either B cells or macrophages (140). Thus, cytokines produced by peripheral blood NK cells in RPL can inhibit blastocyst development. 2. Activity, numbers, and phenotype. Several studies have tried to establish enhanced peripheral NK cell activity or elevated NK cell numbers as causes of recurrent miscarriage. Among
TABLE 5. Studies of peripheral NK cells in RPL Study
N
Inclusion criteria
Method
Results
Cr release assay
High preconceptional NK cell activity in women with RPL predictive of increased abortion rate (RR 3.5) in subsequent pregnancy Preconceptional NK cell cytotoxicity and numbers similar in RPL and controls; in RPL, NK cells ⬍12% associated with carrying subsequent pregnancy to term; higher numbers of CD56⫹CD16⫹ cells with increased cytotoxic NK cell activity in early pregnancy in RPL Higher CD69 expression and lower CD94 expression in NK cells of women with RPL compared to controls
Studies showing increased numbers and/or activity of peripheral NK cells in RPL Aoki et al., 1995 (142)
68
Two consecutive first-trimester SAB; no uterine, endocrine, genetic, or autoimmune cause
51
Emmer et al., 2000 (141)
43
Two or more consecutive idiopathic SAB before 16 wk; nl parental karyotype, APL, TFTs; no DM or PCOS
Flow cytometry, release assay
Ntrivalas et al., 2001 (143)
22
Two or more SAB; no anatomical, hormonal, infectious, autoimmune cause
Flow cytometry
51
Cr
51
Cr
Study showing no increase in peripheral NK cell numbers/activity in RPL Souza et al., 2002 (144)
9
Two or more consecutive SAB; nl parental karyotype, APL, pelvic US, HSG, EMBx, no endocrine cause
Flow cytometry, release assay
No difference in numbers of CD16⫹ or CD56⫹ cells between RPL and controls; NK cell activity slightly lower in RPL compared to controls
SAB, Spontaneous abortions; RR, relative risk; APL, antiphospholipid screen; nl, normal; TFTs, thyroid function tests; DM, diabetes mellitus; PCOS, polycystic ovarian syndrome; US, ultrasound; HSG, hysterosalpingogram; EMBx, endometrial biopsy.
54
Endocrine Reviews, February 2005, 26(1):44 – 62
Dosiou and Giudice • NK Cells in Pregnancy and RPL
these studies, only four have examined NK cells in women with unexplained RPL; these are described below in more detail (141–144) (Table 5). Other studies on this topic include women with all causes of RPL, and in many cases have included patients receiving various treatments such as iv Ig, lymphocyte immunotherapy, and others that can influence NK cell activity (15, 145–148). These are not included in this review. Aoki et al. (142) observed increased preconceptional NK cell activity, as measured by a chromium-51 release cytotoxicity assay, in 68 women with unexplained RPL compared with 47 controls. Among women with a history of RPL, enhanced NK cell activity (defined as mean ⫹ 1 sd of NK activity of controls and measured as percentage cytotoxicity) attributed a relative risk of 3.5 for miscarriage in the next pregnancy, compared with women with normal NK cell activity (142). In contrast, in another study, no differences were detected in preconceptional peripheral NK cytotoxicity (measured as lytic units) and numbers between women with RPL (n ⫽ 43) and controls, although a preconceptional peripheral NK cell percentage of less than 12% in women with RPL was significantly associated with a subsequent successful pregnancy (141). In early pregnancy, the investigators noted an increase in NK cell cytotoxicity, peaking at 8 wk, as well as an increase in the percentage of CD56⫹ CD16⫹ cells in women with RPL (141). In a much smaller study (n ⫽ 9), Souza et al. (144) reported a slightly reduced preconceptional peripheral NK cell activity in women with unexplained RPL compared with controls. The discrepancies observed in preconceptional NK activity between RPL patients and controls in these studies could derive from the use of fresh (142, 144)
vs. cryopreserved PBMC (141), as well as differences in the methods used to assess cytotoxicity. Ntrivalas et al. (143) examined the phenotype of peripheral blood NK cells in women with a history of RPL or infertility of uncertain etiology. Expression of CD69, an early activation marker, was significantly higher on NK cells from women with RPL compared with controls. This difference was significant across all subsets of NK cells studied (CD56dim, CD56bright, CD16neg). In addition, there was a significant decrease in the expression of the CD94/NKG2 inhibitory receptor in women with RPL compared with controls. There were no differences noted in the levels of CD25 (IL-2R␣), CD122 (IL-2R), CD128 (IL-8R), CD30, and CD154 (members of the TNF receptor family). An imbalance of CD69 and CD94 expression on peripheral blood NK cells in women with RPL may account for their pathology (143). In summary, RPL is associated with Th1 immunity, for which NK cells are partly responsible. Before ascribing a role of peripheral NK cells in RPL, it is important to note that NK cell numbers do not necessarily correlate with levels of NK cell cytotoxicity (149). In addition, NK cell numbers and activity can fluctuate according to different variables such as exercise and time of day (150, 151). Given these caveats, an increase in NK cell numbers and/or activity in the preconceptional period or in early pregnancy of women with RPL (141, 142) is of concern, although additional studies are needed to corroborate these findings. In addition, phenotypic changes are apparent in the NK cells of women with RPL, which may account for their increased activity (143). The mechanism through which these changes occur in RPL is still unknown, and the possibility of altered hormonal
TABLE 6. Studies of uNK cells in RPL Study
N
Inclusion criteria
Specimen
Method
Resultsa
Studies showing increase in uNK cells/subsets in RPL compared to normals Lachapelle et al., 1996 20 Three or more consecutive first- EMBx– d 18 –25 (152) trimester SAB; nl HSG, parental karyotype, EMBx, thyroid stimulating hormone, prolactin, APL Quenby et al., 1999 22 Three or more consecutive SAB; EMBx– d 19 –22 (155) nl parental karyotype and APL, no endocrine cause Clifford et al., 1999 29 History of RPL; nl parental EMBx– d 20 –23 (154) karyotype, uterine US, APL Emmer et al., 2002 (157)
9 Two or more consecutive SAB before 16 wk; nl parental karyotype, APL
Tissue collected after SAB/curettage of nonvital pregnancy
Flow cytometry
Similar % of NK cells; greater % of CD16⫹ CD56dim cells; smaller % of CD16⫺CD56bright cells Immunohistochemistry Higher % of CD16⫹ cells and CD56⫹ cells
Immunohistochemistry Increased numbers of CD56⫹ cells in women with losses ⬍13 wk Immunohistochemistry Increased expression of CD56 and CD16
Studies showing no increase in uNK cells/subsets in RPL compared to normals Shimada et al., 2004 (153)
20 Two or more primary SAB; nl HSG, US, APL, parental karyotype, EMBx; negative hematologic workup Michimata et al., 2002 17 Two consecutive first-trimester (156) SAB; nl HSG, US, APL, parental karyotype, EMBx, TFTs, prolactin
EMBx–midluteal
Flow cytometry
No difference in % of CD56⫹, CD56⫹CD16⫹ or CD56⫹CD16⫺ cells
EMBx– d 18 –21
Immunohistochemistry No difference in numbers of CD56⫹ or CD16⫹ cells
SAB, Spontaneous abortions; APL, antiphospholipid screen; nl, normal; TFTs, thyroid function tests; US, ultrasound; HSG, hysterosalpingogram; EMBx, endometrial biopsy. a Results report findings in women with RPL compared to controls.
Dosiou and Giudice • NK Cells in Pregnancy and RPL
sensitivity of NK cells and/or T cells to progesterone regulation has not been studied and is worthy of additional investigation. B. uNK cells in RPL
The role of uNK cells in unexplained RPL has also been a topic of investigation. Two flow cytometry studies and several immunohistochemistry studies examining this subject are published in the literature (Table 6). In all of these studies, endometrial specimens were obtained at similar times in the menstrual cycle in RPL patients and controls, to minimize the variability in uNK cells that normally occurs during the course of the menstrual cycle. Lachapelle et al. (152) analyzed the phenotype of endometrial T, B, and NK cells from endometrial specimens from 20 women with RPL compared with 15 fertile controls. The RPL population was defined as women with three or more unexplained, consecutive, first-trimester spontaneous abortions with the same partner. An extensive workup was performed to identify the cause of RPL in all subjects, and only those with negative workups were included. Endometrial samples were collected during the secretory phase and were processed fresh for evaluation by flow cytometry. The percentage of NK cells in the two populations was similar, although women with RPL had a greater percentage of CD16⫹CD56dim NK cells and a smaller percentage of CD16⫺CD56bright cells, which are normally the dominant endometrial NK population, compared with control patients (152). Because CD16 is responsible for antibody-dependent cytotoxicity and CD16⫹ cells have greater cytolytic activity than CD16⫺ NK cells, an increased number of CD16⫹ NK cells in the RPL population may be causative of pregnancy loss. Alternatively, because the CD16⫺CD56bright NK population is known to produce hormones that are important for placental growth, the decrease in this population in RPL women may create an unfavorable growth environment for the conceptus. Other differences were observed in the T cell and B cell populations, including a lower percentage of CD8⫹ T cells, a higher CD4/CD8 ratio, and a higher proportion of B lymphocytes in women with RPL (152). These latter differences support a role for suppressor CD8⫹ T cells in downregulating the maternal immune response in normal pregnancy, whereas B lymphocytes, which may secrete harmful antibodies to the fetoplacental unit, are normally decreased in numbers. A decrease in the CD8⫹ population and an increase in the B lymphocyte subset could be expected in a dysregulated state leading to miscarriage. More recently, a flow cytometry analysis of midluteal endometrial samples from 20 women with a history of two or more unexplained miscarriages showed no difference in the percentages of uNK cells, CD56⫹CD16⫺, or CD56⫹CD16⫹ uNK cell subsets compared with samples from control subjects, while observing a significant decrease in the percentage of T lymphocytes in RPL patients (153). Whether the observed decrease in T lymphocyte numbers was due to a decrease in the CD8⫹ subset, similar to the findings of Lachapelle et al., is not reported. Immunohistochemical analyses of uNK cells in RPL also have conflicting results. When frozen sections of luteal-phase endometrial biopsy specimens of women with unexplained
Endocrine Reviews, February 2005, 26(1):44 – 62 55
RPL were evaluated, an increase in the numbers of CD56⫹ cells compared with controls was observed in two studies (154, 155), and one of these also reported an increase in CD16⫹ cells (155). A third immunohistochemistry study that used formalin-fixed tissue embedded in paraffin showed no difference in the numbers of the endometrial CD56⫹ and CD16⫹ cell populations (156), supporting the results by flow cytometry. The discrepancies among these studies most likely derive from the different techniques used (frozen tissue vs. paraffin sections). In endometrial tissue obtained after spontaneous abortion in women with RPL, Emmer et al. (157) reported increased expression of both CD56 and CD16. This was accompanied by a decrease in HLA-G expression in trophoblast tissue. These observations are difficult to interpret, because they could either be the cause or the result of miscarriage, given the fact that they were obtained after the event. In summary, there is likely no difference in the percentage of total uNK cells in endometrial leukocytes of women with RPL compared with women without RPL. This is supported by the two studies using flow cytometry of endometrial leukocytes (152, 153), the best method to analyze and quantitate lymphocyte subsets, as well as by one of the immunohistochemical studies (156). Nevertheless, there may be a significantly different phenotype among uNK cells in RPL, with a greater proportion of cells being CD16⫹CD56dim (152, 155), which may have important functional implications in women with RPL. Larger studies are needed to verify this finding. Furthermore, aberrant hormonal regulation of these cells in the setting of RPL is a possibility and remains a challenge for future investigation. C. A model of NK cell function in pregnancy vs. RPL
A model of the physiological roles of peripheral and uNK in human pregnancy is presented in Fig. 1. Available data support that during the early stages of normal pregnancy, progesterone enhances migration of peripheral CD56bright NK cells to the uterus both by directly inducing expression of molecules facilitating such homing and by up-regulation of MIP-1 and VEGF production by endometrial stromal cells. In addition, MIP-1␣, produced by fetal cytotrophoblasts, may also attract CD56bright peripheral NK cells to the placenta during pregnancy, as shown in in vitro studies with human tissues (158). During this period, uNK cells also proliferate significantly in situ, under the influence of IL-15 and prolactin, made by endometrial stromal cells during the process of decidualization. The expanded uNK cell population then plays an important role through cytokine production in supporting proper trophoblast and placental growth (Fig. 1) as well as vascularization of the decidua. In addition, through production of immunomodulatory molecules they may participate in the creation of local immunosuppression at the maternal-fetal interface (67). These are most pronounced during the phase of trophoblast invasion into the stroma with redundancy in epithelial immunosuppressants, e.g., glycodelin, during blastocyst attachment and intrusion into the endometrium. During early pregnancy, peripheral NK cells are down-regulated, with a decrease in their numbers and activity and increased expression of inhibitory mol-
56
Endocrine Reviews, February 2005, 26(1):44 – 62
ecules. These peripheral and local changes could be the result of the direct action of progesterone on peripheral and uNK cells through nongenomic pathways or indirect effects on NK cells through support of a Th2 cytokine environment. It is known that proliferative responses of PBMC to recall antigens such as influenza A and tetanus as well as to alloantigens are significantly decreased in healthy women in early pregnancy compared with the nonpregnant state (159). These changes occur in an immune environment characterized by decreased levels of Th1 cytokines. Progesterone has been shown to enhance Th2 cytokine production by Th1-producing T cell clones (160) and enhance differentiation of T cells into the Th2 pathway (44). In addition, it has been shown to block Th1 immunity to trophoblast by PBMC of women with RPL in vitro (139). The high progesterone state in pregnancy likely favors a Th2 environment in the periphery as well as in the maternal-fetal interface, which suppresses some aspects of NK activity and alters NK cytokine production toward a Th2 phenotype. In RPL, increases in NK cell numbers and activity in peripheral blood are associated with possibly increased numbers of CD56dimCD16⫹ cells in the endometrium. The apparent role of uNK cells in RPL pathogenesis in the human may at first seem contradictory to the important function of uNK cells in vascular remodeling during pregnancy in the mouse and the potential involvement of uNK cells in healthy human pregnancy outlined above. However, there are several possible explanations for this observation. First, the uNK cells involved in the pathogenesis of RPL may be a different cell population than the normal uNK cells present during a successful pregnancy, as a result of a Th1/Th2 cytokine imbalance in the periphery. In RPL, there is a failure to downregulate immune responses to recall antigens and alloantigens (159), perhaps as a result of a predominance of Th1 cytokines in the peripheral blood. What the initial insult is that favors the establishment of a Th1 milieu, however, remains to be determined. It is possible that there is decreased sensitivity to the immunosuppressive effects of progesterone on peripheral lymphocytes due to polymorphisms in progesterone cell targets. However, once this Th1 environment is established, it could directly result in the observed increased peripheral NK cell numbers and function via the actions of Th1 cytokines IL-2 and IFN-␥. Alternatively, there could be decreased sensitivity to progesterone at the level of the NK cells, leading to increased NK cell numbers and activity. Subsequently, peripheral NK cells could infiltrate the uterus and result in increased numbers of CD56dimCD16⫹ cells in the endometrium (see Section IV.B.). It is therefore possible, that the uNK cells that normally reside in the endometrium and encourage the development of a healthy pregnancy are not involved in the pathogenesis of RPL, but rather, peripheral NK cells that are normally not present in substantial numbers in the uterus may be the culprits. Another possibility is that NK cell cytokine expression is important for one stage of placental development (e.g., during the initial placental development associated with implantation) and not for another. High numbers of NK cells and/or activity later in pregnancy may be detrimental. Alternatively, the subtypes of uNK cells in RPL or their functionality could be different, translating to aberrant behavior
Dosiou and Giudice • NK Cells in Pregnancy and RPL
and miscarriage. It is also possible that there is Th1/Th2 imbalance locally, in the endometrium. In fact, implantation sites of unexplained RPL patients with normal chromosomal content have been recently shown to have decreased numbers of Th2 cells (161). Defective production of IL-4 and LIF by decidual T cells from patients with unexplained RPL has also been documented (162). Production of both IL-4 and LIF is up-regulated by progesterone (162); a defect in regulation of that pathway may account for some cases of unexplained RPL. Dysregulation of other participants of the local endometrial immune milieu involving uNK has been investigated. Progesterone receptor polymorphisms have been investigated in women with unexplained RPL, and no association was found for the specific PROGINS polymorphism of the PR gene (163). Decreased amounts of glycodelin production have been reported in uterine flushings of women with unexplained RPL (164); furthermore, levels were lower in women who went on to miscarry than those who were able to have a live birth (164). Elevated levels of IL-13 and IL-15 with an increased IL-13/IL-15 ratio (165) and decreased IL-1 and IL-6 expression (166) have been observed in midsecretory endometrium of women with unexplained RPL compared with controls, suggesting abnormal regulation of these cytokines in RPL. Finally, studies of gene expression in placentae from patients with unexplained RPL have been performed and are comprehensively reviewed in a recent publication (167). In one of these studies, chorionic villi specimens of patients with unexplained RPL (wk 6 – 8 of gestation) were found to have decreased expression of angiogenesis-related genes and increased expression of apoptosisrelated genes compared with specimens from fertile patients with elective terminations of pregnancy (168). In a second study, subtractive hybridization analysis of chorionic villi from patients with unexplained RPL compared with fertile women (wk 6 – 8 of gestation) has identified eight genes that are more abundantly expressed in normals: glycodelin, mucin 1, matrix metalloproteinase-2, fibronectin, hCG, hemoglobin-␥ globulin, and two unidentified genes (169). Finally, immunohistochemical analysis has shown diminished expression of VEGF, VEGF receptors, and tyrosine kinase with Ig and epidermal growth factor homology domains (Tie) receptors in placental and decidual tissues from women with unexplained RPL compared with women undergoing elective pregnancy terminations (170). One criticism of all of the above studies is that the RPL samples were derived from miscarriages, which raises the question whether the observed changes in gene expression are the cause or result of the miscarriages. Nevertheless, the function of the genes identified could yield insight into the pathogenesis of RPL. D. NK cells and current RPL therapies
Given the poor understanding of the precise mechanisms underlying unexplained RPL, therapy so far has been empirical and not evidence-based. Treatment modalities for RPL include aspirin, heparin, progesterone, hCG, prednisone, leukocyte immunization, and iv Ig (3, 171, 172). Some of these therapies, namely leukocyte immunization and iv Ig, have been pursued as different approaches of immuno-
Dosiou and Giudice • NK Cells in Pregnancy and RPL
modulation to down-regulate the maternal immune response to the embryo. Only treatment with aspirin and heparin in women with antiphospholipid syndrome has shown documented efficacy in well-conducted, prospective, randomized trials (3). Treatment of women with hereditary thrombophilia with lowmolecular weight heparin has had some success (173, 174); however, prospective randomized controlled trials (RCTs) are still needed. Progesterone treatment early in pregnancy in women with RPL has been examined in a metaanalysis of four small controlled trials, which suggested a beneficial effect (175). Preliminary results from Brigham and Women’s Hospital (Boston, MA) have shown that women with Th1 immunity to trophoblast are treated effectively with 100 mg twice a day of progesterone vaginal suppositories beginning 3 d after ovulation (171). However, randomized clinical trials on the use of progesterone in RPL have not been performed, and such trials will be difficult to conduct in the United States because of the practice of commonly treating patients with unexplained RPL with supplemental progesterone vaginal suppositories. Prednisone and hCG have been studied in RCTs and have been found to be ineffective (176 –178). With regard to paternal leukocyte immunization in RPL, there have been five published RCTs, only one of which showed a beneficial effect (172). In the latter study, methods of randomization were not well defined, and data analysis was somewhat unconventional (179). Furthermore, a metaanalysis using individual patient data showed no benefit of leukocyte immunization (180). Similarly, there have been six RCTs of iv Ig treatment of unexplained RPL; four showed no benefit, and two showed a benefit. These studies were reviewed in a metaanalysis of individual patient data that revealed no statistically significant benefit for iv Ig in unexplained RPL (181). Finally, a recent RCT from Denmark confirmed no benefit in an intention-to-treat analysis (182). Therefore, there is no solid evidence supporting the use of either paternal leukocyte immunization or iv Ig in the treatment of unexplained RPL. It is interesting that two of the most commonly used therapeutics in RPL affect NK cell function. Heparin, in addition to its anticoagulant effects, is known to suppress NK cell cytotoxicity (183, 184) and antagonize IFN-␥ action by inhibiting its binding to the cell surface (185, 186). The second therapy, progesterone, can inhibit Th1 cytokine release and reduce embryotoxicity by trophoblast-activated PBMC cultures from women with RPL (139). A recent study of women with unexplained infertility has shown that ovarian stimulation with gonadotropins and progesterone results in a decrease in Th1 CD4⫹ cells, NK cells, and NK cell activity (187). Such treatment also results in a decrease in the levels of plasma IFN-␥ and IL-2 and an increase in TGF-1 (187). Whether these changes translate into higher numbers of successful pregnancies, however, remains to be determined through RCTs. Thus, currently, treatment for unexplained RPL remains empiric. Prospective randomized trials for use of heparin or progesterone in women with unexplained RPL are still needed to document efficacy of these modalities in this patient population. Certainly, from a theoretical standpoint,
Endocrine Reviews, February 2005, 26(1):44 – 62 57
they would be rational therapeutic tools, given their immunomodulatory effects. Understanding the exact mechanism of NK cell involvement in the pathogenesis of unexplained RPL will hopefully identify more targets for the development of new and effective therapies.
V. Eye to the Future
In summary, peripheral NK cells and uNK cells comprise distinct cell populations, in terms of phenotype and function. Available evidence suggests hormonal regulation of both populations, but predominantly of the uNK population, through an intricate endometrial cytokine and hormonal network (Fig. 1 and Table 3). Through direct or indirect effects of progesterone, uNK cells likely provide appropriate cytokine support and local immunomodulation, and peripheral NK cells down-regulate their activity in a normal pregnancy. In RPL, creation of a Th1 cytokine environment in the periphery may lead to NK cell activation and proliferation, which could result in migration of cytotoxic NK cells into the uterus and cause miscarriage. Alternatively, the local endometrial immune milieu may be disrupted at a variety of levels, causing defects in homing of the proper NK population to the uterus, local production of cytokines and hormones such as IL-15 and prolactin, or impairment of more downstream events such as production of immunoregulatory factors by uNK cells. Disruption at any of these levels may alter the ability of the uNK population to perform its normal functions and result in an unsuccessful pregnancy. Additional studies are needed to identify which, if any, of the above mechanisms is responsible for the changes observed in NK cells in RPL and to validate whether hormonal dysregulation of the immune response, at any level, is responsible for these effects. Genetic analysis of the uNK population in women with a history of unexplained RPL compared with fertile controls could provide insight into mechanisms underlying RPL and potentially identify candidate genes. Investigation of polymorphisms in hormonal and cytokine receptor genes may provide additional important information. As we develop a more comprehensive understanding of the hormonal modulation of the endometrial immune environment, we shall be better positioned to develop novel, specific, and effective therapeutics for patients with unexplained RPL.
Acknowledgments We thank Dr. Joseph Hill for his valuable comments on the manuscript. Address all correspondence and requests for reprints to: Linda C. Giudice, M.D., Ph.D., Department of Gynecology and Obstetrics, Stanford University Medical Center, Stanford, California 94305. E-mail:
[email protected] This work was supported by National Institutes of Health (NIH) Grant T-32 (to C.D.), the Endocrine Fellows Foundation (to C.D.), the Fannie E. Rippel Foundation Fellowship (to C.D.), and NIH Cooperative Program on Trophoblast-Maternal Tissue Interactions (U-01-HD-42298; to L.C.G.).
58
Endocrine Reviews, February 2005, 26(1):44 – 62
Dosiou and Giudice • NK Cells in Pregnancy and RPL
References 1. Stirrat GM 1990 Recurrent miscarriage. Lancet 336:673– 675 2. Clifford K, Rai R, Watson H, Regan L 1994 An informative protocol for the investigation of recurrent miscarriage: preliminary experience of 500 consecutive cases. Hum Reprod 9:1328 –1332 3. Lee RM, Silver RM 2000 Recurrent pregnancy loss: summary and clinical recommendations. Semin Reprod Med 18:433– 440 4. Kutteh WH 1999 Recurrent pregnancy loss: an update. Curr Opin Obstet Gynecol 11:435– 439 5. Stray-Pedersen B, Stray-Pedersen S 1984 Etiologic factors and subsequent reproductive performance in 195 couples with a prior history of habitual abortion. Am J Obstet Gynecol 148:140 –146 6. Robertson MJ, Ritz J 1990 Biology and clinical relevance of human natural killer cells. Blood 76:2421–2438 7. Nagler A, Lanier LL, Cwirla S, Phillips JH 1989 Comparative studies of human FcRIII-positive and negative natural killer cells. J Immunol 143:3183–3191 8. Cooper MA, Fehniger TA, Caligiuri MA 2001 The biology of human natural killer-cell subsets. Trends Immunol 22:633– 640 9. Lanier LL 2001 On guard–activating NK cell receptors. Nat Immunol 2:23–27 10. Biassoni R, Cantoni C, Marras D, Giron-Michel J, Falco M, Moretta L, Dimasi N 2003 Human natural killer cell receptors: insights into their molecular function and structure. J Cell Mol Med 7:376 – 387 11. King A, Allan DS, Bowen M, Powis SJ, Joseph S, Verma S, Hiby SE, McMichael AJ, Loke YW, Braud VM 2000 HLA-E is expressed on trophoblast and interacts with CD94/NKG2 receptors on decidual NK cells. Eur J Immunol 30:1623–1631 12. Northern AL, Rutter SM, Peterson CM 1994 Cyclic changes in the concentrations of peripheral blood immune cells during the normal menstrual cycle. Proc Soc Exp Biol Med 207:81– 88 13. Yovel G, Shakhar K, Ben-Eliyahu S 2001 The effects of sex, menstrual cycle, and oral contraceptives on the number and activity of natural killer cells. Gynecol Oncol 81:254 –262 14. Souza SS, Castro FA, Mendonca HC, Palma PV, Morais FR, Ferriani RA, Voltarelli JC 2001 Influence of menstrual cycle on NK activity. J Reprod Immunol 50:151–159 15. Beer AE, Kwak JY, Ruiz JE 1996 Immunophenotypic profiles of peripheral blood lymphocytes in women with recurrent pregnancy losses and in infertile women with multiple failed in vitro fertilization cycles. Am J Reprod Immunol 35:376 –382 16. Gregory CD, Lee H, Rees GB, Scott IV, Shah LP, Golding PR 1985 Natural killer cells in normal pregnancy: analysis using monoclonal antibodies and single-cell cytotoxicity assays. Clin Exp Immunol 62:121–127 17. Gregory CD, Lee H, Scott IV, Golding PR 1987 Phenotypic heterogeneity and recycling capacity of natural killer cells in normal human pregnancy. J Reprod Immunol 11:135–145 18. Ponte M, Cantoni C, Biassoni R, Tradori-Cappai A, Bentivoglio G, Vitale C, Bertone S, Moretta A, Moretta L, Mingari MC 1999 Inhibitory receptors sensing HLA-G1 molecules in pregnancy: decidua-associated natural killer cells express LIR-1 and CD94/ NKG2A and acquire p49, an HLA-G1-specific receptor. Proc Natl Acad Sci USA 96:5674 –5679 19. Seaman WE, Blackman MA, Gindhart TD, Roubinian JR, Loeb JM, Talal N 1978 -Estradiol reduces natural killer cells in mice. J Immunol 121:2193–2198 20. Seaman WE, Merigan TC, Talal N 1979 Natural killing in estrogentreated mice responds poorly to poly I.C despite normal stimulation of circulating interferon. J Immunol 123:2903–2905 21. Hanna N, Schneider M 1983 Enhancement of tumor metastasis and suppression of natural killer cell activity by -estradiol treatment. J Immunol 130:974 –980 22. Fernandes-Carlos T, Riondel J, Glise D, Guiraud P, Favier A 1997 Modulation of natural killer cell functional activity in athymic mice by -carotene, oestrone and their association. Anticancer Res 17: 2523–2527 23. Gauchez AS, Riondel J, Fernandes-Carlos T, Jacrot M, Guiraud P, Coudray C, Calop J, Favier A 1996 Effect of oestrone on the natural killer (NK) cell activity, antioxidant status and tumour
24.
25.
26. 27. 28. 29. 30.
31. 32.
33. 34. 35. 36. 37. 38. 39. 40. 41.
42. 43.
44. 45.
growth in athymic mice xenografted with human tumours. Anticancer Res 16:853– 859 Curran EM, Berghaus LJ, Vernetti NJ, Saporita AJ, Lubahn DB, Estes DM 2001 Natural killer cells express estrogen receptor-␣ and estrogen receptor- and can respond to estrogen via a non-estrogen receptor-␣-mediated pathway. Cell Immunol 214:12–20 Screpanti I, Santoni A, Gulino A, Herberman RB, Frati L 1987 Estrogen and antiestrogen modulation of the levels of mouse natural killer activity and large granular lymphocytes. Cell Immunol 106:191–202 Sorachi K, Kumagai S, Sugita M, Yodoi J, Imura H 1993 Enhancing effect of 17 -estradiol on human NK cell activity. Immunol Lett 36:31–35 Baral E, Nagy E, Berczi I 1995 Modulation of natural killer cellmediated cytotoxicity by tamoxifen and estradiol. Cancer 75:591– 599 Uksila J 1985 Human NK cell activity is not inhibited by pregnancy and cord serum factors and female steroid hormones in vitro. J Reprod Immunol 7:111–120 Siiteri PK, Febres F, Clemens LE, Chang RJ, Gondos B, Stites D 1977 Progesterone and maintenance of pregnancy: is progesterone nature’s immunosuppressant? Ann NY Acad Sci 286:384 –397 Szekeres-Bartho J, Hadnagy J, Pacsa AS 1985 The suppressive effect of progesterone on lymphocyte cytotoxicity: unique progesterone sensitivity of pregnancy lymphocytes. J Reprod Immunol 7:121–128 Sulke AN, Jones DB, Wood PJ 1985 Hormonal modulation of human natural killer cell activity in vitro. J Reprod Immunol 7:105– 110 Inoue T, Kanzaki H, Imai K, Narukawa S, Katsuragawa H, Watanabe H, Hirano T, Mori T 1996 Progesterone stimulates the induction of human endometrial CD56⫹ lymphocytes in an in vitro culture system. J Clin Endocrinol Metab 81:1502–1507 Van Voorhis BJ, Anderson DJ, Hill JA 1989 The effects of RU 486 on immune function and steroid-induced immunosuppression in vitro. J Clin Endocrinol Metab 69:1195–1199 Hansen KA, Opsahl MS, Nieman LK, Baker Jr JR, Klein TA 1992 Natural killer cell activity from pregnant subjects is modulated by RU 486. Am J Obstet Gynecol 166:87–90 Stites DP, Siiteri PK 1983 Steroids as immunosuppressants in pregnancy. Immunol Rev 75:117–138 Gerli R, Rambotti P, Nicoletti I, Orlandi S, Migliorati G, Riccardi C 1986 Reduced number of natural killer cells in patients with pathological hyperprolactinemia. Clin Exp Immunol 64:399 – 406 Matera L, Ciccarelli E, Cesano A, Veglia F, Miola C, Camanni F 1989 Natural killer activity in hyperprolactinemic patients. Immunopharmacology 18:143–146 Matera L, Cesano A, Bellone G, Oberholtzer E 1992 Modulatory effect of prolactin on the resting and mitogen-induced activity of T, B, and NK lymphocytes. Brain Behav Immun 6:409 – 417 Chambers WH, Amoscato AA, Smith MS, Kenniston TW, Herberman RB, Appasamy PM 1995 Prolactin receptor expression by rat NK cells. Nat Immun 14:145–156 Matera L, Muccioli G, Cesano A, Bellussi G, Genazzani E 1988 Prolactin receptors on large granular lymphocytes: dual regulation by cyclosporin A. Brain Behav Immun 2:1–10 Horseman ND, Zhao W, Montecino-Rodriguez E, Tanaka M, Nakashima K, Engle SJ, Smith F, Markoff E, Dorshkind K 1997 Defective mammopoiesis, but normal hematopoiesis, in mice with a targeted disruption of the prolactin gene. EMBO J 16:6926 – 6935 Bouchard B, Ormandy CJ, Di Santo JP, Kelly PA 1999 Immune system development and function in prolactin receptor-deficient mice. J Immunol 163:576 –582 Ehring GR, Kerschbaum HH, Eder C, Neben AL, Fanger CM, Khoury RM, Negulescu PA, Cahalan MD 1998 A nongenomic mechanism for progesterone-mediated immunosuppression: inhibition of K⫹ channels, Ca2⫹ signaling, and gene expression in T lymphocytes. J Exp Med 188:1593–1602 Miyaura H, Iwata M 2002 Direct and indirect inhibition of Th1 development by progesterone and glucocorticoids. J Immunol 168: 1087–1094 Henderson TA, Saunders PT, Moffett-King A, Groome NP,
Dosiou and Giudice • NK Cells in Pregnancy and RPL
46.
47. 48. 49. 50. 51.
52. 53. 54.
55.
56.
57.
58. 59. 60.
61.
62. 63. 64.
65. 66. 67.
Critchley HO 2003 Steroid receptor expression in uterine natural killer cells. J Clin Endocrinol Metab 88:440 – 449 Zhu Y, Rice CD, Pang Y, Pace M, Thomas P 2003 Cloning, expression, and characterization of a membrane progestin receptor and evidence it is an intermediary in meiotic maturation of fish oocytes. Proc Natl Acad Sci USA 100:2231–2236 Murphy KM, Reiner SL 2002 The lineage decisions of helper T cells. Nat Rev Immunol 2:933–944 Abbas AK, Murphy KM, Sher A 1996 Functional diversity of helper T lymphocytes. Nature 383:787–793 O’Garra A 1998 Cytokines induce the development of functionally heterogeneous T helper cell subsets. Immunity 8:275–283 Paganin C, Matteucci C, Cenzuales S, Mantovani A, Allavena P 1994 IL-4 inhibits binding and cytotoxicity of NK cells to vascular endothelium. Cytokine 6:135–140 Seo N, Tokura Y, Furukawa F, Takigawa M 1998 Down-regulation of tumoricidal NK and NK T cell activities by MHC Kb molecules expressed on Th2-type ␥␦ T and ␣ T cells coinfiltrating in early B16 melanoma lesions. J Immunol 161:4138 – 4145 Deniz G, Akdis M, Aktas E, Blaser K, Akdis CA 2002 Human NK1 and NK2 subsets determined by purification of IFN-␥-secreting and IFN-␥-nonsecreting NK cells. Eur J Immunol 32:879 – 884 Loza MJ, Peters SP, Zangrilli JG, Perussia B 2002 Distinction between IL-13⫹ and IFN-␥⫹ natural killer cells and regulation of their pool size by IL-4. Eur J Immunol 32:413– 423 Szekeres-Bartho J, Barakonyi A, Polgar B, Par G, Faust Z, Palkovics T, Szereday L 1999 The role of ␥/␦ T cells in progesteronemediated immunomodulation during pregnancy: a review. Am J Reprod Immunol 42:44 – 48 Szekeres-Bartho J, Par G, Dombay G, Smart YC, Volgyi Z 1997 The antiabortive effect of progesterone-induced blocking factor in mice is manifested by modulating NK activity. Cell Immunol 177: 194 –199 Polgar B, Kispal G, Lachmann M, Paar G, Nagy E, Csere P, Miko E, Szereday L, Varga P, Szekeres-Bartho J 2003 Molecular cloning and immunologic characterization of a novel cDNA coding for progesterone-induced blocking factor. J Immunol 171:5956 –5963 Maret A, Coudert JD, Garidou L, Foucras G, Gourdy P, Krust A, Dupont S, Chambon P, Druet P, Bayard F, Guery JC 2003 Estradiol enhances primary antigen-specific CD4 T cell responses and Th1 development in vivo. Essential role of estrogen receptor ␣ expression in hematopoietic cells. Eur J Immunol 33:512–521 Fox HS, Bond BL, Parslow TG 1991 Estrogen regulates the IFN-␥ promoter. J Immunol 146:4362– 4367 Cuturi MC, Anegon I, Sherman F, Loudon R, Clark SC, Perussia B, Trinchieri G 1989 Production of hematopoietic colony-stimulating factors by human natural killer cells. J Exp Med 169:569 –583 Naume B, Johnsen AC, Espevik T, Sundan A 1993 Gene expression and secretion of cytokines and cytokine receptors from highly purified CD56⫹ natural killer cells stimulated with interleukin-2, interleukin-7 and interleukin-12. Eur J Immunol 23:1831–1838 Biassoni R, Ferrini S, Prigione I, Pelak VS, Sekaly RP, Long EO 1991 Activated CD3-CD16⫹ natural killer cells express a subset of the lymphokine genes induced in activated ␣  ⫹ and ␥ ␦ ⫹ T cells. Scand J Immunol 33:247–252 Bulmer JN, Morrison L, Longfellow M, Ritson A, Pace D 1991 Granulated lymphocytes in human endometrium: histochemical and immunohistochemical studies. Hum Reprod 6:791–798 Saito S 2000 Cytokine network at the feto-maternal interface. J Reprod Immunol 47:87–103 King A, Balendran N, Wooding P, Carter NP, Loke YW 1991 CD3-leukocytes present in the human uterus during early placentation: phenotypic and morphologic characterization of the CD56⫹⫹ population. Dev Immunol 1:169 –190 King A, Loke YW 1991 On the nature and function of human uterine granular lymphocytes. Immunol Today 12:432– 435 Moffett-King A 2002 Natural killer cells and pregnancy. Nat Rev Immunol 2:656 – 663 Koopman LA, Kopcow HD, Rybalov B, Boyson JE, Orange JS, Schatz F, Masch R, Lockwood CJ, Schachter AD, Park PJ, Strominger JL 2003 Human decidual natural killer cells are a unique NK cell subset with immunomodulatory potential. J Exp Med 198:1201–1212
Endocrine Reviews, February 2005, 26(1):44 – 62 59 68. Kodama T, Hara T, Okamoto E, Kusunoki Y, Ohama K 1998 Characteristic changes of large granular lymphocytes that strongly express CD56 in endometrium during the menstrual cycle and early pregnancy. Hum Reprod 13:1036 –1043 69. Chantakru S, Miller C, Roach LE, Kuziel WA, Maeda N, Wang WC, Evans SS, Croy BA 2002 Contributions from self-renewal and trafficking to the uterine NK cell population of early pregnancy. J Immunol 168:22–28 70. Lydon JP, DeMayo FJ, Funk CR, Mani SK, Hughes AR, Montgomery Jr CA, Shyamala G, Conneely OM, O’Malley BW 1995 Mice lacking progesterone receptor exhibit pleiotropic reproductive abnormalities. Genes Dev 9:2266 –2278 71. Tibbetts TA, Conneely OM, O’Malley BW 1999 Progesterone via its receptor antagonizes the pro-inflammatory activity of estrogen in the mouse uterus. Biol Reprod 60:1158 –1165 72. Yao MW, Lim H, Schust DJ, Choe SE, Farago A, Ding Y, Michaud S, Church GM, Maas RL 2003 Gene expression profiling reveals progesterone-mediated cell cycle and immunoregulatory roles of hoxa-10 in the preimplantation uterus. Mol Endocrinol 17:610 – 627 73. Kitaya K, Yasuda J, Nakayama T, Fushiki S, Honjo H 2003 Effect of female sex steroids on human endometrial CD16(neg) CD56(bright) natural killer cells. Fertil Steril 79:730 –734 74. Stewart JA, Bulmer JN, Murdoch AP 1998 Endometrial leucocytes: expression of steroid hormone receptors. J Clin Pathol 51:121–126 75. King A, Gardner L, Loke YW 1996 Evaluation of oestrogen and progesterone receptor expression in uterine mucosal lymphocytes. Hum Reprod 11:1079 –1082 76. Borzychowski AM, Chantakru S, Minhas K, Paffaro VA, Yamada AT, He H, Korach KS, Croy BA 2003 Functional analysis of murine uterine natural killer cells genetically devoid of oestrogen receptors. Placenta 24:403– 411 77. Seppala M, Taylor RN, Koistinen H, Koistinen R, Milgrom E 2002 Glycodelin: a major lipocalin protein of the reproductive axis with diverse actions in cell recognition and differentiation. Endocr Rev 23:401– 430 78. Kao LC, Tulac S, Lobo S, Imani B, Yang JP, Germeyer A, Osteen K, Taylor RN, Lessey BA, Giudice LC 2002 Global gene profiling in human endometrium during the window of implantation. Endocrinology 143:2119 –2138 79. Choe YS, Shim C, Choi D, Lee CS, Lee KK, Kim K 1997 Expression of galectin-1 mRNA in the mouse uterus is under the control of ovarian steroids during blastocyst implantation. Mol Reprod Dev 48:261–266 80. Lim KJ, Odukoya OA, Ajjan RA, Li TC, Weetman AP, Cooke ID 1998 Profile of cytokine mRNA expression in peri-implantation human endometrium. Mol Hum Reprod 4:77– 81 81. Lin H, Mosmann TR, Guilbert L, Tuntipopipat S, Wegmann TG 1993 Synthesis of T helper 2-type cytokines at the maternal-fetal interface. J Immunol 151:4562– 4573 82. Kitaya K, Nakayama T, Okubo T, Kuroboshi H, Fushiki S, Honjo H 2003 Expression of macrophage inflammatory protein-1 in human endometrium: its role in endometrial recruitment of natural killer cells. J Clin Endocrinol Metab 88:1809 –1814 83. Red-Horse K, Drake PM, Gunn MD, Fisher SJ 2001 Chemokine ligand and receptor expression in the pregnant uterus: reciprocal patterns in complementary cell subsets suggest functional roles. Am J Pathol 159:2199 –2213 84. Ancelin M, Buteau-Lozano H, Meduri G, Osborne-Pellegrin M, Sordello S, Plouet J, Perrot-Applanat M 2002 A dynamic shift of VEGF isoforms with a transient and selective progesterone-induced expression of VEGF189 regulates angiogenesis and vascular permeability in human uterus. Proc Natl Acad Sci USA 99:6023– 6028 85. Popovici RM, Kao LC, Giudice LC 2000 Discovery of new inducible genes in in vitro decidualized human endometrial stromal cells using microarray technology. Endocrinology 141:3510 –3513 86. Chantakru S, Wang WC, van den Heuvel M, Bashar S, Simpson A, Chen Q, Croy BA, Evans SS 2003 Coordinate regulation of lymphocyte-endothelial interactions by pregnancy-associated hormones. J Immunol 171:4011– 4019 87. Okada S, Okada H, Sanezumi M, Nakajima T, Yasuda K, Kanzaki H 2000 Expression of interleukin-15 in human endometrium and decidua. Mol Hum Reprod 6:75– 80
60
Endocrine Reviews, February 2005, 26(1):44 – 62
88. Okada H, Nakajima T, Sanezumi M, Ikuta A, Yasuda K, Kanzaki H 2000 Progesterone enhances interleukin-15 production in human endometrial stromal cells in vitro. J Clin Endocrinol Metab 85: 4765– 4770 89. Verma S, Hiby SE, Loke YW, King A 2000 Human decidual natural killer cells express the receptor for and respond to the cytokine interleukin 15. Biol Reprod 62:959 –968 90. Wu WX, Brooks J, Glasier AF, McNeilly AS 1995 The relationship between decidualization and prolactin mRNA and production at different stages of human pregnancy. J Mol Endocrinol 14:255–261 91. Jones RL, Critchley HO, Brooks J, Jabbour HN, McNeilly AS 1998 Localization and temporal expression of prolactin receptor in human endometrium. J Clin Endocrinol Metab 83:258 –262 92. Gubbay O, Critchley HO, Bowen JM, King A, Jabbour HN 2002 Prolactin induces ERK phosphorylation in epithelial and CD56(⫹) natural killer cells of the human endometrium. J Clin Endocrinol Metab 87:2329 –2335 93. Jabbour HN, Critchley HO, Yu-Lee LY, Boddy SC 1999 Localization of interferon regulatory factor-1 (IRF-1) in nonpregnant human endometrium: expression of IRF-1 is up-regulated by prolactin during the secretory phase of the menstrual cycle. J Clin Endocrinol Metab 84:4260 – 4265 94. Ohteki T, Yoshida H, Matsuyama T, Duncan GS, Mak TW, Ohashi PS 1998 The transcription factor interferon regulatory factor 1 (IRF-1) is important during the maturation of natural killer 1.1⫹ T cell receptor-␣/⫹ (NK1⫹ T) cells, natural killer cells, and intestinal intraepithelial T cells. J Exp Med 187:967–972 95. Ogasawara K, Hida S, Azimi N, Tagaya Y, Sato T, YokochiFukuda T, Waldmann TA, Taniguchi T, Taki S 1998 Requirement for IRF-1 in the microenvironment supporting development of natural killer cells. Nature 391:700 –703 96. Ashkar AA, Black GP, Wei Q, He H, Liang L, Head JR, Croy BA 2003 Assessment of requirements for IL-15 and IFN regulatory factors in uterine NK cell differentiation and function during pregnancy. J Immunol 171:2937–2944 97. Lechleitner S, Gille J, Johnson DR, Petzelbauer P 1998 Interferon enhances tumor necrosis factor-induced vascular cell adhesion molecule 1 (CD106) expression in human endothelial cells by an interferon-related factor 1-dependent pathway. J Exp Med 187: 2023–2030 98. Muller H, Liu B, Croy BA, Head JR, Hunt JS, Dai G, Soares MJ 1999 Uterine natural killer cells are targets for a trophoblast cellspecific cytokine, prolactin-like protein A. Endocrinology 140:2711–2720 99. Ferry BL, Starkey PM, Sargent IL, Watt GM, Jackson M, Redman CW 1990 Cell populations in the human early pregnancy decidua: natural killer activity and response to interleukin-2 of CD56-positive large granular lymphocytes. Immunology 70:446 – 452 100. King A, Birkby C, Loke YW 1989 Early human decidual cells exhibit NK activity against the K562 cell line but not against first trimester trophoblast. Cell Immunol 118:337–344 101. King A, Loke YW 1990 Human trophoblast and JEG choriocarcinoma cells are sensitive to lysis by IL-2-stimulated decidual NK cells. Cell Immunol 129:435– 448 102. Jokhi PP, King A, Sharkey AM, Smith SK, Loke YW 1994 Screening for cytokine messenger ribonucleic acids in purified human decidual lymphocyte populations by the reverse-transcriptase polymerase chain reaction. J Immunol 153:4427– 4435 103. Saito S, Nishikawa K, Morii T, Enomoto M, Narita N, Motoyoshi K, Ichijo M 1993 Cytokine production by CD16-CD56bright natural killer cells in the human early pregnancy decidua. Int Immunol 5:559 –563 104. King A 2000 Uterine leukocytes and decidualization. Hum Reprod Update 6:28 –36 105. Trundley A, Moffett A 2004 Human uterine leukocytes and pregnancy. Tissue Antigens 63:1–12 106. Guimond MJ, Luross JA, Wang B, Terhorst C, Danial S, Croy BA 1997 Absence of natural killer cells during murine pregnancy is associated with reproductive compromise in TgE26 mice. Biol Reprod 56:169 –179 107. de Fougerolles AR, Baines MG 1987 Modulation of the natural killer cell activity in pregnant mice alters the spontaneous abortion rate. J Reprod Immunol 11:147–153
Dosiou and Giudice • NK Cells in Pregnancy and RPL 108. Greenwood JD, Minhas K, di Santo JP, Makita M, Kiso Y, Croy BA 2000 Ultrastructural studies of implantation sites from mice deficient in uterine natural killer cells. Placenta 21:693–702 109. Guimond MJ, Wang B, Croy BA 1998 Engraftment of bone marrow from severe combined immunodeficient (SCID) mice reverses the reproductive deficits in natural killer cell-deficient tg ⑀ 26 mice. J Exp Med 187:217–223 110. Croy BA, He H, Esadeg S, Wei Q, McCartney D, Zhang J, Borzychowski A, Ashkar AA, Black GP, Evans SS, Chantakru S, van den Heuvel M, Paffaro Jr VA, Yamada AT 2003 Uterine natural killer cells: insights into their cellular and molecular biology from mouse modelling. Reproduction 126:149 –160 111. Barber EM, Pollard JW 2003 The uterine NK cell population requires IL-15 but these cells are not required for pregnancy nor the resolution of a Listeria monocytogenes infection. J Immunol 171: 37– 46 112. Ashkar AA, Croy BA 2001 Functions of uterine natural killer cells are mediated by interferon ␥ production during murine pregnancy. Semin Immunol 13:235–241 113. Zhang JH, He H, Borzychowski AM, Takeda K, Akria S, Croy BA 2003 Analysis of cytokine regulators inducing interferon production by mouse uterine natural killer cells. Biol Reprod 69:404 – 411 114. Jokhi PP, King A, Jubinsky PT, Loke YW 1994 Demonstration of the low affinity ␣ subunit of the granulocyte-macrophage colonystimulating factor receptor (GM-CSF-R ␣) on human trophoblast and uterine cells. J Reprod Immunol 26:147–164 115. Jokhi PP, Chumbley G, King A, Gardner L, Loke YW 1993 Expression of the colony stimulating factor-1 receptor (c-fms product) by cells at the human uteroplacental interface. Lab Invest 68:308 – 320 116. Yelavarthi KK, Hunt JS 1993 Analysis of p60 and p80 tumor necrosis factor-␣ receptor messenger RNA and protein in human placentas. Am J Pathol 143:1131–1141 117. Peyman JA, Hammond GL 1992 Localization of IFN-␥ receptor in first trimester placenta to trophoblasts but lack of stimulation of HLA-DRA, -DRB, or invariant chain mRNA expression by IFN-␥. J Immunol 149:2675–2680 118. Loke YW, King A, Gardner L, Carter NP 1992 Evidence for the expression of granulocyte-macrophage colony-stimulating factor receptors by human first trimester extravillous trophoblast and its response to this cytokine. J Reprod Immunol 22:33– 45 119. Drake BL, Head JR 1994 GM-CSF and CSF-1 stimulate DNA synthesis but not cell proliferation in short-term cultures of mid-gestation murine trophoblast. J Reprod Immunol 26:41–56 120. Saito S, Saito M, Enomoto M, Ito A, Motoyoshi K, Nakagawa T, Ichijo M 1993 Human macrophage colony-stimulating factor induces the differentiation of trophoblast. Growth Factors 9:11–19 121. Athanassakis I, Bleackley RC, Paetkau V, Guilbert L, Barr PJ, Wegmann TG 1987 The immunostimulatory effect of T cells and T cell lymphokines on murine fetally derived placental cells. J Immunol 138:37– 44 122. Berkowitz RS, Hill JA, Kurtz CB, Anderson DJ 1988 Effects of products of activated leukocytes (lymphokines and monokines) on the growth of malignant trophoblast cells in vitro. Am J Obstet Gynecol 158:199 –203 123. Hunt JS, Soares MJ, Lei MG, Smith RN, Wheaton D, Atherton RA, Morrison DC 1989 Products of lipopolysaccharide-activated macrophages (tumor necrosis factor-␣, transforming growth factor-) but not lipopolysaccharide modify DNA synthesis by rat trophoblast cells exhibiting the 80-kDa lipopolysaccharide-binding protein. J Immunol 143:1606 –1613 124. Graham CH, Lysiak JJ, McCrae KR, Lala PK 1992 Localization of transforming growth factor- at the human fetal-maternal interface: role in trophoblast growth and differentiation. Biol Reprod 46:561–572 125. Stewart CL, Kaspar P, Brunet LJ, Bhatt H, Gadi I, Kontgen F, Abbondanzo SJ 1992 Blastocyst implantation depends on maternal expression of leukaemia inhibitory factor. Nature 359:76 –79 126. King A, Loke YW 1993 Effect of IFN-␥ and IFN-␣ on killing of human trophoblast by decidual LAK cells. J Reprod Immunol 23: 51– 62 127. Rabinovich GA, Baum LG, Tinari N, Paganelli R, Natoli C, Liu FT, Iacobelli S 2002 Galectins and their ligands: amplifiers, silenc-
Dosiou and Giudice • NK Cells in Pregnancy and RPL
128. 129.
130. 131. 132.
133. 134. 135. 136.
137.
138.
139.
140.
141.
142. 143.
144. 145. 146.
ers or tuners of the inflammatory response? Trends Immunol 23: 313–320 Logdberg L, Wester L 2000 Immunocalins: a lipocalin subfamily that modulates immune and inflammatory responses. Biochim Biophys Acta 1482:284 –297 Rachmilewitz J, Borovsky Z, Riely GJ, Miller R, Tykocinski ML 2003 Negative regulation of T cell activation by placental protein 14 is mediated by the tyrosine phosphatase receptor CD45. J Biol Chem 278:14059 –14065 Ritson A, Bulmer JN 1989 Isolation and functional studies of granulated lymphocytes in first trimester human decidua. Clin Exp Immunol 77:263–268 Manaseki S, Searle RF 1989 Natural killer (NK) cell activity of first trimester human decidua. Cell Immunol 121:166 –173 Croy BA, Chapeau C 1990 Evaluation of the pregnancy immunotrophism hypothesis by assessment of the reproductive performance of young adult mice of genotype scid/scid.bg/bg. J Reprod Fertil 88:231–239 Stallmach T, Ehrenstein T, Isenmann S, Muller C, Hengartner H, Kagi D 1995 The role of perforin-expression by granular metrial gland cells in pregnancy. Eur J Immunol 25:3342–3348 Yamada H, Polgar K, Hill JA 1994 Cell-mediated immunity to trophoblast antigens in women with recurrent spontaneous abortion. Am J Obstet Gynecol 170:1339 –1344 Hill JA, Polgar K, Anderson DJ 1995 T-helper 1-type immunity to trophoblast in women with recurrent spontaneous abortion. JAMA 273:1933–1936 Kwak-Kim JY, Chung-Bang HS, Ng SC, Ntrivalas EI, Mangubat CP, Beaman KD, Beer AE, Gilman-Sachs A 2003 Increased T helper 1 cytokine responses by circulating T cells are present in women with recurrent pregnancy losses and in infertile women with multiple implantation failures after IVF. Hum Reprod 18: 767–773 Raghupathy R, Makhseed M, Azizieh F, Omu A, Gupta M, Farhat R 2000 Cytokine production by maternal lymphocytes during normal human pregnancy and in unexplained recurrent spontaneous abortion. Hum Reprod 15:713–718 Raghupathy R, Makhseed M, Azizieh F, Hassan N, Al-Azemi M, Al-Shamali E 1999 Maternal Th1- and Th2-type reactivity to placental antigens in normal human pregnancy and unexplained recurrent spontaneous abortions. Cell Immunol 196:122–130 Choi BC, Polgar K, Xiao L, Hill JA 2000 Progesterone inhibits in-vitro embryotoxic Th1 cytokine production to trophoblast in women with recurrent pregnancy loss. Hum Reprod 15(Suppl 1): 46 –59 Polgar K, Hill JA 2002 Identification of the white blood cell populations responsible for Th1 immunity to trophoblast and the timing of the response in women with recurrent pregnancy loss. Gynecol Obstet Invest 53:59 – 64 Emmer PM, Nelen WL, Steegers EA, Hendriks JC, Veerhoek M, Joosten I 2000 Peripheral natural killer cytotoxicity and CD56(pos)CD16(pos) cells increase during early pregnancy in women with a history of recurrent spontaneous abortion. Hum Reprod 15:1163–1169 Aoki K, Kajiura S, Matsumoto Y, Ogasawara M, Okada S, Yagami Y, Gleicher N 1995 Preconceptional natural-killer-cell activity as a predictor of miscarriage. Lancet 345:1340 –1342 Ntrivalas EI, Kwak-Kim JY, Gilman-Sachs A, Chung-Bang H, Ng SC, Beaman KD, Mantouvalos HP, Beer AE 2001 Status of peripheral blood natural killer cells in women with recurrent spontaneous abortions and infertility of unknown aetiology. Hum Reprod 16:855– 861 Souza SS, Ferriani RA, Santos CM, Voltarelli JC 2002 Immunological evaluation of patients with recurrent abortion. J Reprod Immunol 56:111–121 Coulam CB, Goodman C, Roussev RG, Thomason EJ, Beaman KD 1995 Systemic CD56⫹ cells can predict pregnancy outcome. Am J Reprod Immunol 33:40 – 46 Kwak JY, Beaman KD, Gilman-Sachs A, Ruiz JE, Schewitz D, Beer AE 1995 Up-regulated expression of CD56⫹, CD56⫹/CD16⫹, and CD19⫹ cells in peripheral blood lymphocytes in pregnant women with recurrent pregnancy losses. Am J Reprod Immunol 34:93–99
Endocrine Reviews, February 2005, 26(1):44 – 62 61 147. Morikawa M, Yamada H, Kato EH, Shimada S, Ebina Y, Yamada T, Sagawa T, Kobashi G, Fujimoto S 2001 NK cell activity and subsets in women with a history of spontaneous abortion. Cause, number of abortions, and subsequent pregnancy outcome. Gynecol Obstet Invest 52:163–167 148. Yamada H, Kato EH, Kobashi G, Ebina Y, Shimada S, Morikawa M, Sakuragi N, Fujimoto S 2001 High NK cell activity in early pregnancy correlates with subsequent abortion with normal chromosomes in women with recurrent abortion. Am J Reprod Immunol 46:132–136 149. Gilman-Sachs A, DuChateau BK, Aslakson CJ, Wohlgemuth GP, Kwak JY, Beer AE, Beaman KD 1999 Natural killer (NK) cell subsets and NK cell cytotoxicity in women with histories of recurrent spontaneous abortions. Am J Reprod Immunol 41:99 –105 150. Nielsen HB, Secher NH, Christensen NJ, Pedersen BK 1996 Lymphocytes and NK cell activity during repeated bouts of maximal exercise. Am J Physiol 271:R222–R227 151. Terao K, Suzuki J, Ohkura S 2002 Circadian rhythm in circulating CD16-positive natural killer (NK) cells in macaque monkeys, implication of plasma cortisol levels. Primates 43:329 –338 152. Lachapelle MH, Miron P, Hemmings R, Roy DC 1996 Endometrial T, B, and NK cells in patients with recurrent spontaneous abortion. Altered profile and pregnancy outcome. J Immunol 156:4027– 4034 153. Shimada S, Kato EH, Morikawa M, Iwabuchi K, Nishida R, Kishi R, Onoe K, Minakami H, Yamada H 2004 No difference in natural killer or natural killer T-cell population, but aberrant T-helper cell population in the endometrium of women with repeated miscarriage. Hum Reprod 19:1018 –1024 154. Clifford K, Flanagan AM, Regan L 1999 Endometrial CD56⫹ natural killer cells in women with recurrent miscarriage: a histomorphometric study. Hum Reprod 14:2727–2730 155. Quenby S, Bates M, Doig T, Brewster J, Lewis-Jones DI, Johnson PM, Vince G 1999 Pre-implantation endometrial leukocytes in women with recurrent miscarriage. Hum Reprod 14:2386 –2391 156. Michimata T, Ogasawara MS, Tsuda H, Suzumori K, Aoki K, Sakai M, Fujimura M, Nagata K, Nakamura M, Saito S 2002 Distributions of endometrial NK cells, B cells, T cells, and Th2/Tc2 cells fail to predict pregnancy outcome following recurrent abortion. Am J Reprod Immunol 47:196 –202 157. Emmer PM, Steegers EA, Kerstens HM, Bulten J, Nelen WL, Boer K, Joosten I 2002 Altered phenotype of HLA-G expressing trophoblast and decidual natural killer cells in pathological pregnancies. Hum Reprod 17:1072–1080 158. Drake PM, Gunn MD, Charo IF, Tsou CL, Zhou Y, Huang L, Fisher SJ 2001 Human placental cytotrophoblasts attract monocytes and CD56(bright) natural killer cells via the actions of monocyte inflammatory protein 1␣. J Exp Med 193:1199 –1212 159. Bermas BL, Hill JA 1997 Proliferative responses to recall antigens are associated with pregnancy outcome in women with a history of recurrent spontaneous abortion. J Clin Invest 100:1330 –1334 160. Piccinni MP, Giudizi MG, Biagiotti R, Beloni L, Giannarini L, Sampognaro S, Parronchi P, Manetti R, Annunziato F, Livi C, Romagnani S, Maggi E 1995 Progesterone favors the development of human T helper cells producing Th2-type cytokines and promotes both IL-4 production and membrane CD30 expression in established Th1 cell clones. J Immunol 155:128 –133 161. Michimata T, Sakai M, Miyazaki S, Ogasawara MS, Suzumori K, Aoki K, Nagata K, Saito S 2003 Decrease of T-helper 2 and Tcytotoxic 2 cells at implantation sites occurs in unexplained recurrent spontaneous abortion with normal chromosomal content. Hum Reprod 18:1523–1528 162. Piccinni MP, Beloni L, Livi C, Maggi E, Scarselli G, Romagnani S 1998 Defective production of both leukemia inhibitory factor and type 2 T-helper cytokines by decidual T cells in unexplained recurrent abortions. Nat Med 4:1020 –1024 163. Kurz C, Tempfer CB, Boecskoer S, Unfried G, Nagele F, Hefler LA 2001 The PROGINS progesterone receptor gene polymorphism and idiopathic recurrent miscarriage. J Soc Gynecol Investig 8:295– 298 164. Dalton CF, Laird SM, Estdale SE, Saravelos HG, Li TC 1998 Endometrial protein PP14 and CA-125 in recurrent miscarriage patients; correlation with pregnancy outcome. Hum Reprod 13: 3197–3202
62
Endocrine Reviews, February 2005, 26(1):44 – 62
165. Chegini N, Ma C, Roberts M, Williams RS, Ripps BA 2002 Differential expression of interleukins (IL) IL-13 and IL-15 throughout the menstrual cycle in endometrium of normal fertile women and women with recurrent spontaneous abortion. J Reprod Immunol 56:93–110 166. von Wolff M, Thaler CJ, Strowitzki T, Broome J, Stolz W, Tabibzadeh S 2000 Regulated expression of cytokines in human endometrium throughout the menstrual cycle: dysregulation in habitual abortion. Mol Hum Reprod 6:627– 634 167. Baek KH 2004 Aberrant gene expression associated with recurrent pregnancy loss. Mol Hum Reprod 10:291–297 168. Choi HK, Choi BC, Lee SH, Kim JW, Cha KY, Baek KH 2003 Expression of angiogenesis- and apoptosis-related genes in chorionic villi derived from recurrent pregnancy loss patients. Mol Reprod Dev 66:24 –31 169. Baek KH, Choi BC, Lee JH, Choi HK, Lee SH, Kim JW, Hill JA, Chung HM, Ko JJ, Cha KY 2002 Comparison of gene expression at the feto-maternal interface between normal and recurrent pregnancy loss patients. Reprod Fertil Dev 14:235–240 170. Vuorela P, Carpen O, Tulppala M, Halmesmaki E 2000 VEGF, its receptors and the tie receptors in recurrent miscarriage. Mol Hum Reprod 6:276 –282 171. Hill JA 1999 Recurrent pregnancy loss. In: Creasy RK, Resnik R, eds. Maternal-fetal medicine. 4th ed. Philadelphia: W.B. Saunders Company; 423– 443 172. Rai R, Regan L 2002 The endometrium in recurrent miscarriage. In: Glasser SR, Aplin JD, Giudice LC, Tabibzadeh S, eds. The endometrium. New York: Taylor, Francis; 546 –555 173. Brenner B, Hoffman R, Blumenfeld Z, Weiner Z, Younis JS 2000 Gestational outcome in thrombophilic women with recurrent pregnancy loss treated by enoxaparin. Thromb Haemost 83:693– 697 174. Carp H, Dolitzky M, Inbal A 2003 Thromboprophylaxis improves the live birth rate in women with consecutive recurrent miscarriages and hereditary thrombophilia. J Thromb Haemost 1:433– 438 175. Daya S 1989 Efficacy of progesterone support for pregnancy in women with recurrent miscarriage. A meta-analysis of controlled trials. Br J Obstet Gynaecol 96:275–280 176. Harrison RF 1992 Human chorionic gonadotrophin (hCG) in the management of recurrent abortion; results of a multi-centre placebo-controlled study. Eur J Obstet Gynecol Reprod Biol 47:175–179
Dosiou and Giudice • NK Cells in Pregnancy and RPL 177. Quenby S, Farquharson RG 1994 Human chorionic gonadotropin supplementation in recurring pregnancy loss: a controlled trial. Fertil Steril 62:708 –710 178. Laskin CA, Bombardier C, Hannah ME, Mandel FP, Ritchie JW, Farewell V, Farine D, Spitzer K, Fielding L, Soloninka CA, Yeung M 1997 Prednisone and aspirin in women with autoantibodies and unexplained recurrent fetal loss. N Engl J Med 337:148 –153 179. Mowbray JF, Gibbings C, Liddell H, Reginald PW, Underwood JL, Beard RW 1985 Controlled trial of treatment of recurrent spontaneous abortion by immunisation with paternal cells. Lancet 1:941–943 180. Jeng GT, Scott JR, Burmeister LF 1995 A comparison of metaanalytic results using literature vs individual patient data. Paternal cell immunization for recurrent miscarriage. JAMA 274:830 – 836 181. Daya S, Gunby J, Porter F, Scott J, Clark DA 1999 Critical analysis of intravenous immunoglobulin therapy for recurrent miscarriage. Hum Reprod Update 5:475– 482 182. Christiansen OB, Pedersen B, Rosgaard A, Husth M 2002 A randomized, double-blind, placebo-controlled trial of intravenous immunoglobulin in the prevention of recurrent miscarriage: evidence for a therapeutic effect in women with secondary recurrent miscarriage. Hum Reprod 17:809 – 816 183. Yamamoto H, Fuyama S, Arai S, Sendo F 1985 Inhibition of mouse natural killer cytotoxicity by heparin. Cell Immunol 96:409 – 417 184. Johann S, Zoller C, Haas S, Blumel G, Lipp M, Forster R 1995 Sulfated polysaccharide anticoagulants suppress natural killer cell activity in vitro. Thromb Haemost 74:998 –1002 185. Fritchley SJ, Kirby JA, Ali S 2000 The antagonism of interferon-␥ (IFN-␥) by heparin: examination of the blockade of class II MHC antigen and heat shock protein-70 expression. Clin Exp Immunol 120:247–252 186. Douglas MS, Rix DA, Dark JH, Talbot D, Kirby JA 1997 Examination of the mechanism by which heparin antagonizes activation of a model endothelium by interferon-␥ (IFN-␥). Clin Exp Immunol 107:578 –584 187. Fornari MC, Sarto A, Berardi VE, Martinez MA, Rocha MG, Pasqualini S, Diez RA 2002 Effect of ovaric hyper-stimulation on blood lymphocyte subpopulations, cytokines, leptin and nitrite among patients with unexplained infertility. Am J Reprod Immunol 48:394 – 403
Endocrine Reviews is published bimonthly by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving the endocrine community.