The incidence of cesarean hysterectomy, uterine scar dehiscence, placenta placenta previa, placenta accreta and bladder injury was similar in two groups.
ORIGINAL ARTICLE HIGHER ORDER MULTIPLE REPEAT CESAREAN SECTIONS: MATERNAL AND FETAL OUTCOME Tariq Y. Khashoggi, ABOG From the Department of Obstetrics and Gynecology, King Saud University College of Medicine, King Khalid University Hospital, Riyadh, Saudi Arabia.
Correspondence to: Dr. T. Khashoggi P.O. Box 2925 Riyadh 11461 Saudi Arabia
Accepted for publication May 2003
D
Background: Multiple repeat cesarean delivery is common in many parts of Saudi Arabia. We conducted a retrospective analysis of patient records to determine the major and minor complications as well as the neonatal outcome associated with multiple repeat cesarean sections. Methods: We analyzed relationships between the number of cesarean sections and various demographic and clinical variables in 150 patients undergoing 4 to 8 cesarean sections (mean 6.0) compared with a control group of 140 patients undergoing 2 to 3 cesarean sections (mean 2.5) during the period from 1996 to 2000 at the Security Forces Hospital, Riyadh, Kingdom of Saudi Arabia. Results: Both the gestation age of the mother and birth weight of the baby were lower in the study group compared with the control group (mean gestation age 36 weeks in the study group compared with 37 weeks in the control group (P=0.001), and mean birth weight 2.9 kg for infants in the study group compared with 3.1 kg in the control group (P=0.01). The total duration of the operation was longer in the study group (63 minutes on average) compared with the control (45 minutes on average) (P=0.001). There were 80 cases of severe adhesion encountered during surgery in the study group compared with 40 cases in the control group (P=0.001). There was no difference in the Apgar score of the baby and the neonatal admission rate in the two groups. The incidence of cesarean hysterectomy, uterine scar dehiscence, placenta placenta previa, placenta accreta and bladder injury was similar in two groups. The incidence of post partum pyrexia, wound infection, urinary tract infection, and blood transfusion was also comparable in the two groups. Conclusion: No specific additional risk is associated with higher order (four to eight) repeat cesarean sections that is not normally encountered with lower order (two to three) repeat cesarean sections. Keywords: Multiple repeat cesarean section, uterine rupture, operative complication, placenta previa, placenta accreta
uring the past two decades, the rate of cesarean delivery in the developed world has been steadily increasing. Currently the United Kingdom has a cesarean section rate of 21%1 and of the 4 million births that occur each year in the United States approximately 25% are by cesarean delivery 2. However, in the developing countries, cesarean section as a mode of delivery is still considered a last option and the cesarean section rate has not shown a parallel expansion3. The factors contributing to high cesarean delivery rate in the developed countries include the management of breech presentation, routine use of electronic fetal monitoring, previous cesarean section scar, and the fear of litigation. Overall, previous cesarean delivery is the leading obstetrics indication for cesarean delivery (39%) in many obstetric units followed by dystocia (28%), fetal distress (14%), breech presentation (9%) and others (10%).4,5 The most unacceptable complication of repeat caesarean section is a risk of scar rupture during pregnancy, second
www.kfshrc.edu.sa/annals
Ann Saudi Med 2003;23(5):278-282
only to death after three or more cesarean sections,6 with increased risk of maternal and fetal mortality.7 For this reason, it is a common practice in the developed world to offer sterilization to women after the third cesarean section. Women are given the chance of a fourth cesarean section in exceptional circumstances only. However, in countries where large families are encouraged by social and cultural factors, any attempt to limit the cesarean section to two or three is likely to be rejected. Although modern obstetric practice has made repeat cesarean sections a feasible option, little is known about the risk involved in multiple cesarean sections, especially when the number exceeds four. The number of patients in the few publications dealing with patients undergoing four or more multiple cesarean sections has been too small for statistical analysis purposes.8-10 Individual case histories of women having several cesarean sections (up to 13) have also been reported.11 The aim of the present study was to determine the outcome and associated risks for the mother and fetus during the fourth or subsequent repeat cesarean section.
Annals of Saudi Medicine • 2003 September-October, Volume 23 • 278
Khashoggi Higher Order Multiple Repeat Cesarean Sections
Methods The study was a retrospective analysis of patient records that included 150 pregnant women who had undergone three or more previous cesarean sections managed by the Department of Obstetrics and Gynecology, Security Forces Hospital, Riyadh, Saudi Arabia between January 1996– December 2000 (inclusive). It is the policy of the department to perform elective cesarean section on patients who have had two or more previous cesarean deliveries. This is normally carried out between 37-38 weeks gestation unless there is another indication to deliver them early. Two patients had previous seven cesarean sections, 10 patients had previous six, 20 patients had previous five, 40 had previous four and 78 patients had previous three cesarean sections. Elective cesarean section was the planned method of delivery in the study group. Fourteen patients had cesarean section before the scheduled time, six due to the onset of labor (within two hours of the start of labor), three due to abruptio placenta, two due to severe pre eclampsia, and three due to leaking liquor. A control group was formed by selecting the next woman delivered by cesarean section, who had previous one to two cesarean sections, after each of the 150 women in the study group. Ten women were excluded from the analysis because of missing data. Twenty women in the control group had previous one cesarean section and 120 women had previous two cesarean sections. The case records of the study and control groups were analyzed for age, parity, height and weight of patient, the length of gestation, the mode of operation whether elective or non elective and type of anesthesia used. Details of operative and post operative course, including duration of operation, fall in hemoglobin, hospital stay, severity of adhesion, visceral injuries, and incidence of other unforeseen surgical procedures such as cesarean hysterectomy and admission to surgical intensive care unit (SICU) were also taken. Perinatal outcome of the newborn including incidence of intrauterine growth retardation, multiple pregnancy, birth weight, Apgar score, and incidence of admission to the neonatal intensive care unit (NICU) was also recorded. The operation was performed by a senior obstetrician or well-trained assistant doctor. Either Pfannenstiel or midline incision was used and standard lower segment transverse incision was made in the lower segment. Chi-squared test was used to analyse discrete variable and Mann-Whitney U- test for analyzing continuous variables Results Maternal age and parity was higher in the study group (Table 1). Gestation at cesarean section was less in the study group. Less patients in the study group had regional anesthesia due to anticipation of more operative complication. The birth weight of babies in the control group was significantly greater (Table 2). The mean birth weight
in the study group was 2.9 kg compared 3.1 kg in the control group. There was no significant difference in the rest of the parameters in the two groups. There were no maternal deaths (Table 3). In the study group uterine scar fenestration (incomplete uterine rupture) was seen in six patients (one patient was in labor), and four patients had complete uterine rupture (two during labor and two before labor). There were four patients in the control group with uterine scar dehiscence, three with incomplete dehiscence (one patient was in labor) and one with complete dehiscence (during labor). The duration of the operation was 63 minutes in the study group compared with 45 minutes in the control group. The difference was statistically significant. However this difference did not affect the Apgar score. There was no significant difference in the blood loss or the amount of blood transfused in the two groups. Blood loss of more than one litre occurred in two patients in the study group and seven patients in the control group. Also there was no difference in the level of decrease of hemoglobin from the pre-operative to post-operative value in the two groups. There were 80 patients in the study group who had dense adhesion noted during the operation compared with 40 patients in the control group. The difference was statistically significant. Three patients in the study group and one patient in the control group ended up in hysterectomy. The patient requiring hysterectomy in the control group had atonic post partum hemorrhage losing more than a liter of blood in the first two hours. Prophylactic antibiotic was given to 100 patients in the study group and 103 patients in the control group. The length of hospital stay was 4.5 days in the study group and 4 days in the control group. This was statistically significant. There was no significant difference in the rest of the parameters between the two groups. Intensive postoperative care was needed in four patients in each group. In the study group, one patient had severe pre-eclampsia and the other three had cesarean hysterectomy and massive post partum hemorrhage to require admission into intensive care unit. The four patients who needed intensive post-operative care in the control group was due to massive blood loss during surgery. No clinically evident thrombo-emboli complication or any mechanical or paralytic ileus was noted. There was no difference in the incidence of wound infection, bladder injury, urinary tract infection or chest infection. The incidence of post operative pyrexia (unknown cause) a temperature of >37.5oC lasting for more than 48 hours, was not different in the two groups. There were two cases of bladder injury in the study group and one patient had bladder injury in the control group. All were repaired successfully. The two cases in the study group underwent emergency hysterectomy due to placenta previa and placenta accreta.
279 • Annals of Saudi Medicine • 2003 September-October, Volume 23
www.kfshrc.edu.sa/annals
Khashoggi Higher Order Multiple Repeat Cesarean Sections
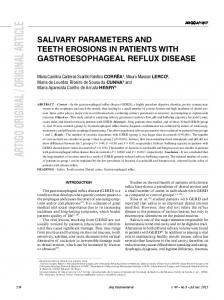
TABLE 1. Demographic and clinical features of the study and control groups.
Variable Maternal age (years) Parity Height (cms) Weight (kg) Gestational age (weeks)
Study group Controls (n=150) (n=140) (mean ± SD) (mean ± SD)
P-value
34 ± 4.4
33 ± 4.2
0.0490
6 ± 1.5 153 ± 7.1
4 ± 2.0 154 ± 6.1
0.001 0.17
72 ± 12.1
72 ± 13.5
0.07
36 ± 1.7
37 ± 1.5
0.00001
n(%) n(%) Mode of operation Elective 120 (85.7) 0.6866 126 (84) Non-elective 24 (14.3) 0.6866 24 (16) Anesthesia Spinal/epidural 9(6)/1(0.7) 10(7.1)/10(7.1) 0.7058/0.0052 General 0.0196 120 (85.7) 141 (94) Cesarean section 22 (15.7) 0.1291 34 (22.7) and tubal ligation
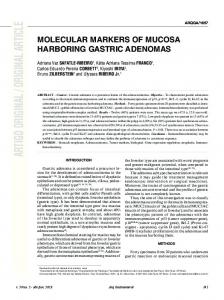
TABLE 2. Perinatal features in the two groups.
Variable Birth weight (kg) Apgar score 1 min 5 min
Below 10th percentile Preterm (1000 cc) Adhesion (severe) Placenta praevia Placenta accreta Cesarean hysterectomy Bladder injury Wound infection UTI Chest infection Temperature >37.5ºC (unknown cause, repeated findings) Blood transfusion Dehiscense of scar at operation Complete Incomplete SICU admission
Study Group (n=150) (mean ± SD) 63 ± 30.5 9.8 ± 10.9 4.5 ± 1.5 n (%)
Control (n=140) (mean ± SD)
P-value
45 ± 19.5 11.5 ± 12.5
0.0000* 0.2173
4 ± 1.0 n (%)
0.0010*
12 (8) 80 (53.3) 8 (5.3) 3 (2)
7 (5) 40 (28.6) 5 (3.6) 2 (1.4)
0.2986 0.0000* 0.4818 0.6922
3 (2) 2 (1.3) 1 (0.7) 2 (1.3) 2 (1.3)
1 (0.7) 1 (0.7) 2 (1.4) 3 (2.1) 2 (1.4)
0.3338 0.6062 0.5614 0.6001 0.9413
11 (7.3)
5 (3.6)
0.1628
22 (14.6)
15 (10.7)
0.3170
10 (6.7) 4 (2.7) 6 (4) 4 (2.7)
4 (2.8) 1 (0.7) 3 (2.1) 4 (2.9)
0.1158 0.1833 0.3446 0.9180
during dissection of the abdominal wall and separation of the bladder from the lower segment. This increased the average operating time (63 minutes) as compared to 45 minutes in the control group. However, this difficulty was of minor clinical importance as the Apgar score of the newborn and maternal recovery were good, and primary healing of the wound and the urinary bladder were uncomplicated. High attachment of the bladder on the abdominal wall is frequent in these patients and should be taken into consideration when opening the peritoneum, or a midline incision of the abdominal cavity considered as an alternative. There were no cases of bowel injury in the present study as uterointestinal adhesions are not common after cesarean section. Others have also reported similar findings.11 There were also no cases of thromboembolism in the study. The most common indication for an emergency hysterectomy in obstetrics is massive hemorrhage often due to placenta accreta or fresh uterine rupture and post operative morbidity is 35-60% in these patients.17,18 In our study, emergency hysterectomy was performed on patients who
had placenta accreta, placenta previa or complete uterine rupture. There was no major morbidity noted in patients who underwent hysterectomy. The incidence of placenta previa and placenta accreta amongst the study and control groups, was similar. Others have reported an increased risk of placenta previa and placenta accreta with multiple caesarean sections.19 Apart from the major morbidity discussed above, the most common morbidity after caesarean section includes endometritis, urinary tract infection, wound infection, need for blood transfusion, post op pyrexia and chest infection. Incidence of such complications was comparable in the two groups. The finding of significantly smaller birth weight babies in the study group may be due to the influence of maternal age, parity and gestation period. However, it is also possible that the scarred uterus as a result of multiple cesarean sections, is a contributing factor. Whatever the cause, a smallish baby is advantageous to the mother as it will prevent the over distension of uterus with its consequences. Women who have a vaginal delivery after a cesarean section, face three times the risk of uterine rupture than those who have a second cesarean section. 14,15,20 Cases of successful trial of vaginal delivery in patients with up to three previous cesarean sections have been reported. 21 However, at present the success and risk of trials of labor in women with several previous cesarean sections are not properly evaluated. Most obstetricians do not attempt trial of labor after three or more previous cesarean sections especially if the woman did not have previous vaginal delivery. The present finding of impaired lower segment healing would discourage attempting vaginal delivery in such patients even though the original indication for a cesarean section was no longer relevant. The advantages of vaginal birth as compared to cesarean delivery are numerous. However obstetric care of subsequent pregnancy and delivery whether abdominal or vaginal is still complicated and risky. Not all women who opt for a trial of labor after previous cesarean delivery have a safe, uncomplicated vaginal birth and instead require repeat cesarean delivery. In addition most of the major complications such as uterine rupture, need of hysterectomy and other operative complications occur in group of women who failed in their attempt at vaginal birth after a previous cesarean delivery than those who had elective repeat cesarean section.22,23,24 As it is difficult to precisely calculate the risk to the mother and the fetus of trial labor versus cesarean section after previous abdominal delivery, many obstetricians continue to perform repeat cesarean section. It is probable that with an increase in the rate of cesarean sections, multiple repeat cesarean sections will become more common. Our results clearly demonstrate that with appropriate prenatal care, adequate pre-operative
281 • Annals of Saudi Medicine • 2003 September-October, Volume 23
www.kfshrc.edu.sa/annals
Khashoggi Higher Order Multiple Repeat Cesarean Sections
preparation, maintenance of meticulous surgical techniques and careful post-operative follow-up as many as four to eight cesarean sections are as safe as two or three such procedures.
References 1. Dobson R. National Sentinel cesarean section audit report. BMJ. 2001; 323:951. 2. McMahon MJ. Vaginal birth after cesarean. Clin Obstet Gynecol. 1998; 41:369-381. 3. Rohra S, Bacchus MJ. A review of cesarean section performed at the Georgeton Hospital Guyana. W Ind Med J. 1983; 32:91-96 4. Porreco RP, Thorp JA. The cesarean birth epidemic: Trends, causes and solutions. Am J Obstet Gynecol.1996; 175:369-374. 5. Shiono P, Fielden J, Mcnelis D, Rhoads G, Pearse W. Recent trends in cesarean birth and trial of labor rates in the United States. JAMA. 1987; 257:494-497. 6. Tamale-Sali EG, Iskander MN. Is there a risk of lower segment scar rupture in pregnancy after multiple cesarean section? J Obstet Gynecol. 1992; 12:19-21. 7. Leung AS, Leung EK, Paul RH. Uterine rupture after previous cesarean delivery: maternal and fetal consequences. Am J Obstet Gynecol. 1993;169:945-950. 8. Kaplan B, Rabinerson D, Harel L, Neri A, & Chayen B. Multiple repeat cesarean sections - Brief communication. Intl Fed of Gynecol & Obstet. 1996; 55:173-174. 9. Soltan MH, Al Nuaim L, Khashoggi T, Chowdhury N, Kangave D, Adelusi B. Sequelae of repeat cesarean sections. Int J Gynecol Obstet. 1996; 52:127-132. 10. Kirkinen P. Multiple cesarean sections: outcomes and complications. Brit J Obstet Gynaecol. 1988; 95:778-782. 11. Piver M & Johnston P. The safety of multiple cesarean section. Obstet Gynecol. 1969; 34:690-694.
www.kfshrc.edu.sa/annals
12. Heritage CK, Cunningham M. Association of elective repeat cesarean delivery and persistent pulmonary hypertension in the newborn. Am J Obstet Gynecol. 1985; 152:627-629. 13. Report on confidential inquiries into maternal deaths in UK 19851987 (1991). HMSO. London. 14. Ojo V A, Adetoro O O, Okwerekwu F E O. Characteristics of maternal death following cesarean section in a developing country. Int J Gynecol Obstet. 1988; 27:171-176. 15. Pettiti D. Maternal mortality and morbidity in cesarean section. Clin Obstet Gynecol. 1985; 28:763-769. 16. Flamm BL, Goings JR, Liu Y & Wolde-Tsadik G. Elective repeat cesarean delivery vs trial of labor: A prospective multicenter study. Obstet Gynaecol. 1994; 83(6):927-928. 17. Plauche W. Cesarean hysterectomy: indications, techniques and complications. Clin Obstet Gynecol. 1986; 29:318-328. 18. Sturdee D & Rushton I. Cesarean and postpartum hysterectomy 1968-1983. Br J Obstet Gynaecol. 1986; 93:270-274. 19. Rageth JC, Juzi C, Grossenbacher H. Delivery after previous cesarean: a risk evaluation. Obstet Gynecol. 1999; 93:332-337. 20. Gregory KD, Korst LM, Cane P, Platt LD, Kahn K. Vaginal birth after cesarean and uterine rupture rates in California . Obstet Gynecol. 1999; 94:985-989. 21. Rosen MG, Dickenson JC, Westhoff CL. Vaginal birth after cesarean: A meta-analysis of morbidity and mortality. Obstet Gynecol. 1991; 77:465-470. 22. McMahon MJ, Luther ER, Bowes WA Jr., Olsham AF. Comparison of a trial of labor with an elective second cesarean section. N Engl J Med. 1996; 335:689-695. 23. Granovsky-Grisaru S, Shaya M, Diamnant YZ. The management of labor in women with more than one uterine scar: Is a repeat cesarean section really the only “safe” option?. J Perinat Med. 1994; 22:13-17. 24. Lyndon-Rochelle, Holt VL, Easterling TR, Martin DP. Risk of uterine rupture during labor among women with a prior cesarean delivery. N Eng J Med. 2001; No.1, 345: 3-8.
Annals of Saudi Medicine • 2003 September-October, Volume 23 • 282