Downloaded from http://pmj.bmj.com/ on July 9, 2015 - Published by group.bmj.com
PGMJ Online First, published on June 29, 2015 as 10.1136/postgradmedj-2014-133161 Review
Pancreatic cancer: current understanding of molecular and genetic aetiologies Tamara M H Gall,1 Harpreet Wasan,2 Long R Jiao1 1
HPB Surgical Unit, Department of Surgery & Cancer, Imperial College, Hammersmith Hospital, London, UK 2 Department of Oncology, Imperial College, London, UK Correspondence to Professor Long R Jiao, HPB Surgical Unit, Department of Surgery & Cancer, Imperial College, Hammersmith Hospital Campus, Du Cane Road, London W12 0HS, UK;
[email protected] Received 3 December 2014 Revised 18 May 2015 Accepted 11 June 2015
ABSTRACT Pancreatic ductal adenocarcinoma (PDAC) is one of the few cancers where prognosis has not improved over the past few decades. However, there have been several advances in our understanding of the disease leading to earlier detection and targeted therapeutic treatment. It is now understood that specific somatic and germline mutations lead to the development of the disease, and the risk factors associated with this are clearer. Further, several precursor lesions have been identified which, with early detection and surveillance, allows treatment before the development of carcinoma. PDAC can now be diagnosed with a high sensitivity and specificity following advances in radiology, and treatment can be commenced at an earlier stage of the disease. With continued research we are hopeful that the next decade will see an improved survival rate for all patients with pancreatic cancer.
INTRODUCTION Pancreatic cancer is a devastating and aggressive disease with an extremely poor prognosis despite radiological, surgical and oncological advances. The majority of cancers (80%) are exocrine, arising from the ductal cells, and are termed pancreatic ductal adenocarcinomas (PDAC). Although evidence suggests that PDAC is a slowly developing disease with at least 18 years between the initiating mutations and the potential for metastatic spread,1 by the time of diagnosis it is considered an invasive and progressive disease which is highly resistant to chemotherapeutic agents. Our understanding of its tumour biology continues to improve rapidly but, despite this, 5-year survival remains at around just 5%. Surgical resection is the only potentially curative treatment, but this is only possible in 25% of patients at initial diagnosis. Those with advanced disease who are treated oncologically without surgery have a median survival of 6 months.2 Even those with a curative R0 resection (ie, a complete resection with no microscopic residual tumour) only have a median survival of 28.7 months.3 This review discusses the epidemiology, risk factors, screening, precursor lesions and diagnosis of PDAC.
(0.31). Although it only accounts for 3% of new cancer cases, mortality is closely related to incidence and it is the fourth leading cause of cancer death among both men and women. Cancer Research UK shows that age-standardised rates are higher in men (10.4–11.1 per 100 000 population) than in women (8.5–9.0 per 100 000) and in people of white and black ethnicity than in those of Asian ethnicity. The overall incidence has remained fairly constant for decades, with a slight increase in women perhaps relating to a change in smoking rates.
RISK FACTORS Pancreatic cancer can be divided into sporadic and familial cancer. There are four main genes affected in sporadic cancer: KRAS (95% of tumours); CDKN2A ( p16) (90%); p53 (75%); and SMAD4 (55%).5 6 Multiple genetic and epigenetic mutations interlinked with environmental factors will lead to the development of PDAC. As with many cancers, the major risk factor is age, with the majority of cases occurring after the age of 60 years and very few before 40. Some other identified risk factors include smoking, chronic pancreatitis (CP), diabetes, obesity, other medical conditions, diet and ABO blood type. Familial pancreatic cancer is seen in patients with first-degree relatives also affected and in younger patients. In these cases of familial aggregation of PDAC, the PRSS1, SPINK1, CDKN2A, STK11, ATM, BRCA1, BRCA2, PALB2, APC and mismatch repair genes may be involved.
Sporadic pancreatic cancer Smoking Currently, tobacco use is the single most important risk factor for pancreatic diseases, accountable for a quarter of cases. Results from a meta-analysis of 82 studies suggest that smoking causes a 75% increase in the risk of pancreatic cancer with a higher risk in those who smoke more per day and for a longer duration.7 Analysing 51 population-based studies with nearly 3 million participants, ‘ever smokers’ have a relative risk (RR) of developing PDAC of 1.60 compared to ‘never smokers’.8
Chronic pancreatitis (CP) EPIDEMIOLOGY
To cite: Gall TMH, Wasan H, Jiao LR. Postgrad Med J Published Online First: [ please include Day Month Year] doi:10.1136/ postgradmedj-2014-133161
The GLOBOCAN project, led by the International Agency for Research on Cancer and the World Health Organization,4 found that worldwide there are over 300 000 new cases of PDAC diagnosed each year. The cumulative risk of developing the disease before the age of 75 years is 0.47 for every 100 children born, and is higher in more developed regions (0.85) than in less developed regions
Mice with mutant K-ras expression show pancreatitis in the early stages and cerulein injections (a cholecystokinin analogue which hyperstimulates the pancreas inducing pancreatitis) accelerate the progression to advanced cancer in these mice.9 The correlation is also seen in humans, with a recent 15-year cohort study of nearly 12 000 patients with CP finding an increased risk for pancreatic cancer compared with controls, with an adjusted HR of
Gall TMH, et al. Postgrad Med J 2015;0:1–7. doi:10.1136/postgradmedj-2014-133161
Copyright Article author (or their employer) 2015. Produced by BMJ Publishing Group Ltd under licence.
1
Downloaded from http://pmj.bmj.com/ on July 9, 2015 - Published by group.bmj.com
Review 6.9 (95% CI 5.6 to 8.6).10 The risk is more pronounced in the first 2–4 years after the diagnosis of CP10 11 and also in those with tropical pancreatitis.12
Diabetes It has long been recognised that type 2 diabetes may increase the risk of developing PDAC; it is seen to be both a cause and a consequence of cancer. There does not seem to be the same relationship for patients with type 1 diabetes,13 although the majority of studies have not distinguished between the two types. A meta-analysis of over 9000 patients with pancreatic cancer found an 80% greater risk of pancreatic cancer in those with type 2 diabetes.14 However, the RR of developing cancer appears to be increased in those with a shorter duration of disease, suggesting some of the effect may be due to an early manifestation of the tumour, although there does remain some evidence for a causal relationship between diabetes and pancreatic cancer as a 50% increased risk still exists for those with a >10-year history of diabetes.15
Obesity There is increasing evidence suggesting that adiposity may increase the risk of developing pancreatic cancer. Two large meta-analyses analysing 3.5 million people with 8062 cases of PDAC16 and 5 million people with 9504 cases of PDAC17 have been conducted within the last decade. The RR of developing PDAC per unit increase in body mass index (BMI) was 1.12 (95% CI 1.06 to 1.17) per 5-unit increase in the first study and 1.10 (95% CI 1.07 to 1.14) per 5-unit increase in the second study. A dose-response effect is seen with the highest risk in those with a BMI >30.
ABO blood type There is some evidence to suggest that ABO blood type may affect the risk of pancreatic cancer. In a Chinese population an increased risk of cancer was seen in those with blood group A (OR 1.60) compared with blood group O. A meta-analysis of worldwide studies found that there is also an increased risk with blood groups B (OR 1.38) and AB (OR 1.52) compared with group O.28 It is possible that there are ABO-related differences in inflammation and cytokine production, but these theories are not well supported.
Familial pancreatic cancer Around 5–10% of cases of pancreatic cancer are seen to show familial clustering, with an increased risk of pancreatic cancer in individuals with a first-degree relative affected.29 The incidence of pancreatic cancer is estimated to rise from 9 per 100 000 per year in patients with no family history of PDAC to 288 per 100 000 per year in those with three or more first-degree relatives with pancreatic cancer.30 A number of germline mutations have been identified in these familial cases of pancreatic cancer and are summarised in table 1.
PRSS1 and SPINK1 Hereditary pancreatitis increases the risk of developing PDAC. The highly penetrant autosomal dominant disorder, which usually manifests by the age of 30,31 is associated with mutations in PRSS1, which results in recurrent attacks of acute pancreatitis leading to CP and its increased cancer risk. The lifetime risk of PDAC in these patients is 35-fold by 70–75 years of age.32 The autosomal recessive form of hereditary pancreatitis develops due to SPINK1 mutations.33
Other medical conditions There are some suggestions that other pathologies increase the risk of pancreatic cancer. For example, patients with pancreatic cancer are more likely to be Helicobacter pylori positive (OR 2.78).18 Patients with inflammatory bowel disease (IBD)—both Crohn’s disease and ulcerative colitis—have an increased lifetime risk of pancreatic cancer (OR 11.22).19 This risk is further increased in patients with IBD with associated primary sclerosing cholangitis.19 Furthermore, patients who have hepatitis B have an increased risk of pancreatic cancer (OR 1.50)20 and hepatitis C virus may also cause an increased risk (HR 1.6)21 although the association is less clear. Finally, there may be a link between periodontal disease and pancreatic cancer.22
Diet A meta-analysis of 11 prospective studies analysed red and processed meat consumption in 2 307 787 participants with 6643 cases of pancreatic cancer. The RR of pancreatic cancer for a 50 g/day increase in processed meat consumption (about one serving) was 1.19 (95% CI 1.04 to 1.36), resulting in a 19% increased risk.23 There is no increased risk with red meat consumption. Other case–control studies have suggested a diet high in protein and unsaturated fatty acids is associated with a decreased risk of pancreatic cancer, in a dose-dependent fashion.24 There is further limited evidence to suggest a decreased risk of cancer with consumption of fruit and vegetables and whole grains, while a possible increased risk exists with the consumption of sugar-sweetened soft drinks.25 Finally, conflicting evidence is found regarding vitamin D, with some supporting a reduced risk of cancer26 and others a higher risk27 with high levels of vitamin D. 2
Table 1 Summary of germline mutations leading to familial pancreatic cancer Gene with germline mutation PRSS1
SPINK1
CDKN2A
Familial disorder
Effect
Recurrent acute pancreatitis (autosomal dominant)31 Hereditary pancreatits (autosomal recessive)33
Chronic pancreatits and thus increased risk of PC32 Chronic pancreatits and thus increased risk of PC33 20% increased risk of PC by age 7534 26% increased risk of PC35 Linked to increased risk of PC36 No association37 and RR 2.3 for development of PC.38 Differing reports 3.5-fold increased risk of PC39 Mutation seen in 1–3% of families with hereditary PC40 Fourfold increased risk of PC41 3.7% risk of PC41
ATM
FAMMM syndrome (autosomal dominant)34 Peutz–Jeghers (autosomal dominant) Ataxia-telangiectasia
BRCA1
80% risk of breast cancer
BRCA2
80% risk of breast cancer
PALB2
80% risk of breast cancer
APC
FAP
Mismatch repair genes
HNPCC
STK11
FAMMM, familial atypical mole and multiple melanoma; FAP, familial adenomatous polyposis; HNPCC, hereditary non-polyposis colorectal cancer; PC, pancreatic cancer; RR, relative risk.
Gall TMH, et al. Postgrad Med J 2015;0:1–7. doi:10.1136/postgradmedj-2014-133161
Downloaded from http://pmj.bmj.com/ on July 9, 2015 - Published by group.bmj.com
Review CDKN2A
PRECURSOR LESIONS
Another autosomal dominant disorder which has a 20% increased risk of pancreatic cancer by the age of 75, as well as a 60–90% risk of melanoma, is familial atypical mole and multiple melanoma (FAMMM) syndrome. These patients have abnormalities in CDKN2A ( p16).34
There are three types of precursor lesions in PDAC that follow a multistep progression from neoplasia showing mild dysplasia to invasive cancer. They are: pancreatic intraepithelial neoplasia (PanIN); intraductal papillary mucinous neoplasm (IPMN); and mucinous cystic neoplasm (MCN). Some of these lesions may be detected on imaging, often incidentally, and either resected or kept under surveillance to prevent the development of, or to allow early detection of, invasive carcinoma.
STK11 (LKB1) and ATM
Germline mutations in STK11 are associated with Peutz–Jeghers syndrome, an autosomal dominant condition resulting in early-onset, large, multiple small intestinal and colonic polyps with an increased cancer risk at these sites.42 These patients also have a 26% increased risk of pancreatic cancer.35 Mutations in the gene ATM result in the disease ataxia-telangiectasia which results in an increased rate of neoplasia, particularly haematological malignancies.43 These mutations have also been linked to pancreatic cancer.36
BRCA1, BRCA2 and PALB2
People with mutations in BRCA1 and BRCA2 carry an 80% lifetime risk for the development of breast cancer44 and germline mutations in PALB2 are also associated with hereditary breast cancer.45 Those with a BRCA2 mutation also have a 3.5-fold increased risk of pancreatic cancer,39 and this mutation is the most common recognisable cause of familial pancreatic cancer. The risk of pancreatic cancer in BRCA1 mutation carriers is less clear, with some reporting a RR of 2.338 while others have found no association.37 Genome sequencing of pancreatic cancer identified PALB2 as a mutation in 1–3% of pancreatic cancer families,40 and carriers have a 5.9-fold increased risk of pancreatic cancer.46
APC and mismatch repair genes
Mutations of the APC gene are well known to result in familial adenomatous polyposis (FAP), and those in a number of mismatch repair genes predispose to hereditary non-polyposis colon cancer (HNPCC). As well as a 100% and 80% risk of developing colon cancer, respectively, these patients also have a risk of developing extraintestinal cancers. Patients with HNPCC have a 3.7% increased risk of pancreatic cancer while those with FAP may have a fourfold increased risk.41
SCREENING Considering that an earlier diagnosis of pancreatic cancer increases the likelihood of resectable disease,1 there has been interest in screening for pancreatic cancer among the high-risk groups discussed above. The International Cancer of the Pancreas Screening Society (CAPS) recently developed and published consortium statements regarding the management of patients at risk of familial pancreatic cancer.47 There was agreement that there was a role for screening with endoscopic ultrasonography (EUS) and/or magnetic resonance cholangiopancreatography (MRCP) of the pancreas in patients with first-degree relatives from a pancreatic cancer family (ie, a family member with PDAC with at least two affected firstdegree relatives) and patients with Peutz–Jeghers syndrome, HNPCC, BRCA2 mutations or CDKN2A mutations with at least one first-degree relative affected. However, age and screening intervals were not agreed upon and, further, consensus was not reached on which abnormalities should lead to surgical resection. There is currently no screening programme for PDAC. Gall TMH, et al. Postgrad Med J 2015;0:1–7. doi:10.1136/postgradmedj-2014-133161
PanIN PanINs are microscopic proliferative epithelial lesions in the smallcalibre pancreatic ducts and ductules.48 They are the most common precursor lesion recognised in pancreatic cancer. A four-tier classification system was established in 201049 that grades the histopathological findings from PanIN-1 to PanIN-3 lesions with increasingly severe dysplasia to invasive carcinoma. Telomere shortening50 and mutations in Kirsten rat sarcoma (KRAS), thought to be the driver mutation for PDAC, p16/CDKN2A, p53, SMAD4 and BRCA2 genes have all been identified in PanIN lesions.51 Unfortunately, PanINs are not detectable by radiological imaging and thus early detection with preventive and curative resection prior to the development of carcinoma is not yet possible.
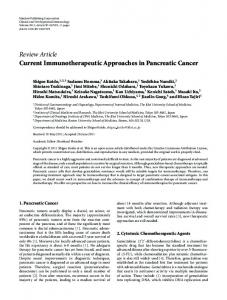
IPMN IPMNs are cystic lesions arising in the main duct or branch duct epithelium of the pancreas characterised by papillary proliferation and mucin production. They are classified according to their malignant transformation from those with low-grade dysplasia to those with invasive carcinoma (I-IPMC). They are also divided into three types based on anatomical location: main duct IPMN (MD-IPMN); branch duct IPMN (BD-IPMN); and mixed type IPMN (mixed IPMN) where both main and branch ducts are involved. Genetic changes in the genes known to be involved in PDAC have been demonstrated in IPMNs—namely, alterations in KRAS, p16/CDKN2A, p53 and SMAD4. IPMNs can be detected with radiological imaging of the pancreas. Analysis of cyst fluid carcinoembryonic antigen (CEA), taken at EUS, can further differentiate between cystic lesions. A CEA >192 ng/mL can detect mucin-producing cysts (IPMNs and MCNs) with 80% accuracy.52 The international consensus guidelines for the management of IPMNs, revised in 2012,53 recommends separate management strategies for those with MD-IPMN/mixed IPMN and those with BD-IPMN. The risk of progression to cancer for MD-IPMN is 36– 90%54 55 and surgical resection is thus advised. For BD-IPMNs the risk of developing an invasive carcinoma has been reported to be as low as 6%56 and therefore annual surveillance of these lesions with MRCP is recommended. Resection of BD-IPMNs is indicated when there are ‘worrying features’ including cyst size >3 cm, a non-enhancing mural nodule, thickened cyst wall and/or an abrupt change in the calibre of the main pancreatic duct (figure 1).
MCN These are mucin-producing cystic lesions of the pancreas characterised by the presence of ovarian type stroma. They are almost always solitary and of incidental finding in young people, located in the body or tail of the pancreas. MCNs are identified on the imaging modalities discussed above and also have a high CEA in the cyst fluid. However, they can be distinguished from IPMNs based on a lack of communication with the main pancreatic duct.57 3.9–30% of MCNs will progress to an invasive cancer, usually PDAC,58 59 and thus surgical resection is recommended. 3
Downloaded from http://pmj.bmj.com/ on July 9, 2015 - Published by group.bmj.com
Review symptoms reported include loss of taste, skin changes and psychological disturbances, namely depression.62
Investigations: laboratory tests
Figure 1 CT scan slice showing a side branch intraductal papillary mucinous neoplasm with mural thrombus.
DIAGNOSIS Presenting symptoms Around 65% of PDAC lesions are seen in the head of the pancreas (HOP), with 15% in the body and tail and the remainder diffusely involving the gland.60 Symptoms tend to manifest once the tumour has invaded surrounding tissues or metastasised to other organs so most people already have advanced disease at diagnosis.29 The most common presenting symptoms reported are: abdominal pain, usually in the upper abdomen which may radiate to the back, experienced by 80% of patients;61 obstructive jaundice reported in 16–85% of those with HOP tumours;62 and weight loss in up to 79%. Courvoisier’s sign, defined as the presence of a non-tender palpable gallbladder and painless jaundice, implies a diagnosis of pancreatic or biliary malignancy rather than gallstones. Diabetes or impaired glucose tolerance can also occur due to damage to the pancreatic parenchyma. Furthermore, obstruction of the pancreatic duct by the tumour may lead to acute pancreatitis. Another sign of PDAC is Trousseau’s syndrome which is characterised by deep or superficial venous thrombosis, hypercoagulability and migratory thrombophlebitis. This syndrome is not exclusive to PDAC and is seen also with lung malignancies and gliomas. Rarer
Table 2 TNM staging of pancreatic cancer according to the American Joint Committee on Cancer (AJCC) TNM staging system TNM stage T-stage Tis T1 T2 T3 T4 N-stage N0 N1 M-stage M0 M1
Description
Carcinoma in situ Tumour 2 cm and limited to pancreas Tumour extends beyond pancreas but no involvement of coeliac axis or SMA Tumour involves the coeliac axis or SMA Regional lymph nodes not involved Regional lymph nodes involved No distant metastases Distant metastases present
M, metastases; N, nodes; SMA, superior mesenteric artery; T, tumour.
4
Where there is a suspicion for pancreatic cancer, further investigations must be urgently undertaken. This involves blood tests including tumour markers and radiological imaging. Routine blood tests are fairly non-specific but may reveal anaemia, hyperglycaemia or raised liver function tests, either as an obstructive picture from the primary tumour obstructing the common bile duct or secondary to liver metastases. In the clinical setting of pancreatic cancer, the most commonly used and validated tumour marker is carbohydrate antigen 19-9 (CA 19-9). CA 19-9 is expressed on the surface of cancer cells as a glycolipid and as an O-linked glycoprotein; 5–10% of the population are unable to synthesise it leading to false negative results.63 Further limitations include a considerable number of false positive results due to its elevation in other malignancies such as colorectal, liver, breast and lung cancers, as well as in benign diseases including, importantly, hyperbilirubinaemia and pancreatitis as well as in liver cirrhosis and lung disorders.64 CA 19-9 also lacks sensitivity for early pancreatic cancers,