Editor. A 57-year-old man was transferred to our institution for a sus- pected pyoderma gangrenosum (PG) of the right leg. History dated back to a month prior to ...
JEADV
LETTER TO THE EDITOR
Pyoderma gangrenosum with extensive pulmonary involvement Editor A 57-year-old man was transferred to our institution for a suspected pyoderma gangrenosum (PG) of the right leg. History dated back to a month prior to his transfer, when the patient presented to an outside hospital. There, he was found to have an inflammatory nodule on the right leg, with central necrosis and ulceration, and an associated fever of 40°C. Laboratory testing revealed anaemia (haemoglobin: 8.6 g/dL), thrombocytopenia (platelets: 71 000/mm3) with myelocytosis and an elevated CRP (150 mg/L). The patient was diagnosed with necrotizing fasciitis; treatment with broad-spectrum antibiotics was initiated, rapidly followed by surgical debridement. However, the patient’s state worsened post-operatively, with extension of the lesion, development of Proteus mirabilis pneumonia and severe neutropenia (granulocytes: 150/mm3). Given this worsening condition, a dermatologist was consulted and a skin biopsy was performed (Fig. 1a and b), diagnosing pyoderma gangrenosum. Concomitantly, the diagnosis of a myelodysplastic syndrome with acute myelofibrosis was made on a bone marrow biopsy. Intravenous (IV) prednisone was started and the patient was transferred to our institution. At the time of admission, there was an extensive right leg surgical wound (Fig. 2a) and the patient was still febrile (38.5°C). Intravenous antibiotics covering P. mirabilis (ceftazidime, vancomycin and ciprofloxacin) and IV prednisone 1 mg/kg had already been started and were continued.
Two weeks after admission, and after an initial overall improvement, fever recurred alongside with pulmonary (cough, dyspnoea and hypoxemia) and cutaneous symptoms (development of pathergy around an intra-arterial catheter) (Fig. 2b). The patient was transferred to the intensive care unit, where a CT scanner revealed diffuse bilateral alveolar opacities (Fig. 2c). Bronchoalveolar lavage (after a 48-h antibiotic window) diagnosed neutrophilic alveolitis (35%) without bacteria on direct examination and culture. The diagnosis of corticosteroid-resistant PG with pulmonary involvement was made. Consequently, the patient received three pulses of 1 g methylprednisolone, followed by anti-TNF alpha (infliximab 5 mg/kg) infusions at week 0, 2 and 6. Pulmonary and cutaneous symptoms resolved within 48 h. A repeat CT scan showed resolution of the radiological findings (Fig. 2d) at week 4. Subsequently, 5-Azacytidine was initiated for his (a)
(c)
(d)
(b)
(a)
250 µm
50 µm
Figure 1 (a and b) show pathological analysis of skin biopsy at 509 and 4009 magnification, respectively, hematein–eosin–safran staining. There is intense neutrophilic infiltration with intradermal abscess formation and dermal necrosis. Scale bar showing 250 and 50 lm respectively.
JEADV 2016
(b)
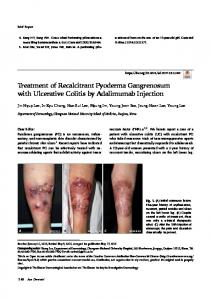
Figure 2 (a) shows patient’s right leg upon arrival in our ward. There were moderate signs of PG activity with surrelevated necrotic border. (b) shows pathergy sign with typical PG lesion around an intra-arterial catheter. (c) shows axial slide of thoracic CT scanner on admission in intensive care unit. There is bilateral asymmetric alveolar infiltrate. (d) shows control thoracic CT scanner 4 weeks after the first methylprednisolone pulse with regression of the alveolar infiltrate bilaterally.
© 2016 European Academy of Dermatology and Venereology
Letter to the Editor
2
myelodysplastic syndrome that was considered to be the underlying instigator of his pyoderma gangrenosum. Unfortunately, the patient died of a multiresistant Stenotrophomonas infection 1 month after beginning infliximab. PG is a rare skin disease characterized by skin ulceration and necrosis, with a heavy neutrophilic infiltrate on skin biopsy without concurrent infection.1 In about half of the cases, PG is associated with either malignancy (haematological or solid), inflammatory disease (e.g. rheumatoid arthritis) or medications.2,3 Neutrophilic extra-cutaneous (lung, intestine, cornea, spleen, etc) involvement is rare. Pulmonary involvement is the most common,4 although there are only few reported cases. We describe here a case of PG with a life-threatening pulmonary involvement that was resistant to initial IV corticosteroids. Knowledge of this complication must lead to its early recognition and rapid increase of immunosuppression to control the neutrophilic disease. In this case, pulmonary PG was suspected because of pulmonary symptoms associated with cutaneous signs of PG activity (pathergy). Differential diagnoses such as infections, cancer and granulomatosis with polyangiitis4 were ruled out in our case. Treatment options consist of systemic corticosteroid, but corticosteroid-resistant or corticosteroid-dependent disease can support the addition of immunosuppressive drugs. Cyclosporine5 and anti-TNF alpha infliximab6 have the most evidence of efficacy. We chose infliximab based on our patient’s critical state that required a drug with a rapid onset of action. Efficacy of this immunosuppressive regimen on the clinical, biological and
JEADV 2016
radiological signs of PG confirmed our diagnosis. Unfortunately, the patient died a few weeks later of a severe infection. We thank Dr Jihanne Abou-Rahal for text review; Dr Francßois Goussot, the pathologist and Dr Pascal Schmoor and Dr Pascal Toussaint for their initial clinical management. M. Scherlinger, S. Guillet, M.-S. Doutre, M. Beylot-Barry, A. Pham-Ledard* Dermatology Department, CHU de Bordeaux, Bordeaux, France *Correspondence: A. Pham-Ledard. E-mail: anne.pham-ledard@ chu-bordeaux.fr
References 1 Brooklyn T, Dunnill G, Probert C. Diagnosis and treatment of pyoderma gangrenosum. BMJ 2006; 333: 181–184. 2 Braswell SF, Kostopoulos TC, Ortega-Loayza AG. Pathophysiology of pyoderma gangrenosum (PG): an updated review. J Am Acad Dermatol 2015; 73: 691–698. 3 Gaspar C, Leyral C, Orlandini V et al. Lethal pulmonary involvement of neutrophilic dermatosis following erythropoietin therapy. Ann Dermatol V�en�er�eol 2008; 135: 384–388. 4 Gade M, Studstrup F, Andersen AK, Hilberg O, Fogh C, Bendstrup E. Pulmonary manifestations of pyoderma gangrenosum: 2 cases and a review of the literature. Respir Med 2015; 109: 443–450. 5 Ormerod AD, Thomas KS, Craig FE et al. Comparison of the two most commonly used treatments for pyoderma gangrenosum: results of the STOP GAP randomised controlled trial. BMJ 2015; 350: h2958–h2958. 6 Brooklyn TN, Dunnill MGS, Shetty A et al. Infliximab for the treatment of pyoderma gangrenosum: a randomised, double blind, placebo controlled trial. Gut 2006; 55: 505–509. DOI: 10.1111/jdv.13976
© 2016 European Academy of Dermatology and Venereology