J Neurophysiol 114: 411– 418, 2015. First published April 15, 2015; doi:10.1152/jn.00065.2015.
Quantifying feedforward control: a linear scaling model for fingertip forces and object weight Ying Lu,1 Seda Bilaloglu,2 Viswanath Aluru,2 and Preeti Raghavan2,3 1
Center for the Promotion of Research Involving Innovative Statistical Methodology, Steinhardt School of Culture, Education and Human Development, New York University; New York, New York; 2Department of Rehabilitation Medicine, New York University School of Medicine, New York, New York; and 3Department of Physical Therapy, Steinhardt School of Culture, Education and Human Development, New York University, New York, New York Submitted 30 January 2015; accepted in final form 9 April 2015
Lu Y, Bilaloglu S, Aluru V, Raghavan P. Quantifying feedforward control: a linear scaling model for fingertip forces and object weight. J Neurophysiol 114: 411– 418, 2015. First published April 15, 2015; doi:10.1152/jn.00065.2015.—The ability to predict the optimal fingertip forces according to object properties before the object is lifted is known as feedforward control, and it is thought to occur due to the formation of internal representations of the object’s properties. The control of fingertip forces to objects of different weights has been studied extensively by using a custom-made grip device instrumented with force sensors. Feedforward control is measured by the rate of change of the vertical (load) force before the object is lifted. However, the precise relationship between the rate of change of load force and object weight and how it varies across healthy individuals in a population is not clearly understood. Using sets of 10 different weights, we have shown that there is a log-linear relationship between the fingertip load force rates and weight among neurologically intact individuals. We found that after one practice lift, as the weight increased, the peak load force rate (PLFR) increased by a fixed percentage, and this proportionality was common among the healthy subjects. However, at any given weight, the level of PLFR varied across individuals and was related to the efficiency of the muscles involved in lifting the object, in this case the wrist and finger extensor muscles. These results quantify feedforward control during grasp and lift among healthy individuals and provide new benchmarks to interpret data from neurologically impaired populations as well as a means to assess the effect of interventions on restoration of feedforward control and its relationship to muscular control. sensorimotor adaptation; feedforward and feedback control; motor control and learning; precision grasp; electromyography
such as picking up a cup of coffee: to lift the cup smoothly off the table, one must be able to exert the right amount of lifting force that just exceeds the weight of the cup, and do so in a manner that leads to neither a jerky movement, causing the coffee to spill (due to an overestimation of the force) nor a hesitant lift (due to an underestimation of the force). We tend to estimate the approximate force first by recalling similar actions from memory. Should there be an overestimation or underestimation on the first lift, the error between the estimated force and the needed force is used to reestimate the force on the second lift. The ability to predict the optimal force on subsequent attempts is called feedforward control and is thought to occur due to the formation of an internal
CONSIDER AN EVERYDAY TASK
Address for reprint requests and other correspondence: P. Raghavan, Dept. of Rehabilitation Medicine, Rusk Institute of Rehabilitation Medicine, NYU Langone Ambulatory Care Center, 240 E. 38th St., 17th Floor, New York, NY 10016 (e-mail:
[email protected]). www.jn.org
representation of the object’s properties, in this case the objects’ weight, in the central nervous system (Davidson and Wolpert 2004; Gordon et al. 1993; Johansson and Westling 1988a). Feedforward control implies that two critical processes are occurring: 1) the error between the estimated force and the needed force is accurately detected, and 2) the error information is used to update or adapt the motor response on a subsequent attempt to execute the task optimally (Blakemore et al. 1998; Drake and Palmer 2000; Kawato and Wolpert 1998; Shadmehr et al. 2010; Wolpert et al. 1995; Wolpert and Miall 1996). The development of feedforward control is important because it leads to rapid reduction in error and faster relearning on subsequent attempts (Huang et al. 2011; Krakauer and Mazzoni 2011) and suggests that the motor system is capable of learning. Studies from several laboratories, including ours, have shown that feedforward control of grasping forces is impaired after injury to the central nervous system, for example, after stroke despite reasonable practice with the affected hand (Hermsdorfer et al. 2003; Nowak et al. 2003; Raghavan et al. 2006, 2010), suggesting that patients may be unable to effectively sense the error with their affected hand and/or integrate it with motor output, and that their motor systems are therefore unable to learn to execute tasks optimally. Skilled hand function requires that we constantly adapt our motor responses according to the properties of the objects we encounter, such as their weight, texture, or shape. However, an impairment in feedforward control prevents such adaptation, perhaps explaining why even patients who recover the ability to grasp after stroke often cannot perform simple functional tasks, such as picking up a cup of coffee with their affected hand (Lai et al. 2002). To effectively treat impairments in feedforward control, one must first be able to quantify the deficit precisely. The feedforward control of fingertip forces during manipulation of objects of up to three different weights has been studied extensively by using a custom-made grip device instrumented with three-dimensional force sensors (Johansson 1998). Feedforward control is measured by the slope or the rate of change of the vertical (load) force (referred to as load force rate hereafter) before the object is lifted off the table. At the moment of lift, the load force must exceed the weight of the object. However, before lift, the load force rate reflects how well the lifting forces are planned. For example, in healthy individuals, it has been found that after just one or two practice lifts, the rate of change of load force is faster for a heavier object than for a lighter object (Flanagan et al. 2001; Johansson and Westling 1988a). Furthermore, the appropriate load force
0022-3077/15 Copyright © 2015 the American Physiological Society
411
412
A SCALING MODEL FOR MOTOR ADAPTATION
rates can be accurately recalled 24 h later, suggesting that the association between the weight and the force rates are held in memory and used for feedforward control in the future (Flanagan et al. 2001; Gordon et al. 1993). What is not clearly understood is the precise relationship between the load force rate and object weight and how it varies across healthy individuals in a population. Determining an exact quantitative relationship would allow researchers and clinicians to directly evaluate whether individuals have developed optimal feedforward control by comparing the changes in load force rate when lifting objects of different weights with model predictions. If the functional form of the relationship between load force rate and weight for healthy subjects is known, it also could be used as a benchmark to quantify the type and extent of impairment in feedforward control in individuals with injury to the nervous system and to determine which interventions effectively improve the deficits. For example, if the function is of the form of a linear or log-linear relationship and the slope of the model is common across healthy subjects, then the evaluation of feedforward control may be simplified by asking individuals to lift just one pair of weights, rather than an entire set of weights. This simplification is important for patients with impairment because it can be challenging for them to lift many different weights repeatedly. We can then compare whether the difference in the load force rate across the two weights is consistent with what the slope of the model would predict. This also allows for more complex multifactor designs to test the efficacy of various treatment regimens to restore feedforward control without excessive amounts of repetition that may produce fatigue and confound the results. The scaling model hypothesis. In this study, we used a random sample of healthy subjects to model the relationship between the peak rate of change of load force (PLFR) and weight over a range of weights encountered in everyday life. We determined whether a linear function (PLFR ⫽ a ⫹ ⵜweight) or a log-linear function (log PLFR ⫽ a ⫹ ⵜweight) best describes the relationship, because both functions can be used to model the phenomenon that PLFR scales up when weight increases. The linear model posits that PLFR increases by a fixed amount (ⵜ) per unit increase in weight, whereas the log-linear function models a fixed proportional increase in PLFR per unit increase in weight. Furthermore, we tested whether a common relationship exists across individuals given the functional form. Specifically, we posit three hypotheses regarding common relationships across individuals in a healthy population: hypothesis 1) for each unit weight increase, there is a common scaling factor ⵜ and a common intercept a across healthy individuals in a population; hypothesis 2) there is one common scaling factor ⵜ across the healthy population; however, the intercept a may vary by individual (common ⵜ, different a); and hypothesis 3) both the scaling factor and the intercept differ across individuals (different ⵜ and different a). Furthermore, we sought to model the relationship between the activity of arm and hand muscles involved in grasping and lifting and feedforward control as measured by the peak rate of change of load force.
board, and informed consent was obtained from all subjects according to the Declaration of Helsinki. Apparatus. A custom-made grip device that measures the fingertip grip and load forces using 6-df force-torque sensors (ATI, Apex, NC) at a sampling rate of 400 Hz was used in this study (Fig. 1A). The weight of the object could be varied by changing the mass in its core. The device was placed on a custom-made plate with electronic switches in it to detect the timing of object liftoff. Bipolar surface electrodes (DE 2.1; Delsys) were placed over eight muscles [abductor pollicis brevis (APB), extensor digitorum communis (EDC), extensor carpi radialis longus (ECRL), first dorsal interroseous (FDI), flexor digitorum superficialis (FDS), flexor carpi ulnaris (FCU), lower trapezius (LT), and upper trapezius (UT)] on the dominant arm to record muscle activity. Electromyographic (EMG) signals were preamplified and sampled at 2,000 Hz. The force and EMG data were captured synchronously using Spike2 (Cambridge Electronic Design, Cambridge, UK). Experimental task. Subjects grasped the grip device with precision grip and lifted it with their dominant (right) hand at their preferred speed upon hearing an auditory cue. They were provided 7 s to complete each trial, but on average all subjects completed the task within 5 s. Subjects were instructed to lift the object by extending their wrist as shown in Fig. 1B. A strap was placed loosely over the forearm to remind subjects not to move the forearm. Subjects lifted 10 different weights, ranging from 250 to 700 g at 50-g intervals, and each weight was lifted 7 times consecutively. To avoid an order effect, the weights were presented randomly. Each new weight was unknown to the subject. Data processing. Force and EMG data were imported to and processed with MATLAB (The MathWorks, Natick, MA). Both grip and load forces were measured, but for the purpose of this study the computations pertain to load forces only, because it has been shown that when the friction at the grip surface is constant, feedforward control to object weight depends on the load forces (Raghavan et al. 2006). Object liftoff was determined from the plate signals. The force data were smoothed by using a moving average filter with a window of ⫾12.5 ms. Load forces at the thumb and index finger sensors were summed. The load force rate was derived from the summed load forces using a ⫾5-point numerical differentiation (i.e., calculated with a ⫾12.5-ms window). The peak force rate was defined as the highest point in the force rate profile that was followed by a subsequent drop of at least 50% between the onset of load force (⬎0.1 N) and liftoff (i.e., the loading phase; Fig. 1C). The EMG data were filtered with a 5- to 500-Hz bandpass filter and a 60-Hz notch filter, and the root mean square of EMG activity during the loading phase was calculated. The EMG activity was normalized to the maximum voluntary contraction of each muscle for each subject. Statistical analysis. The statistical analyses were conducted using RStudio (version 0.98). Package nlme was used to fit linear growth curve models (Fitzmaurice et al. 2011; Pinheiro and Bates 2000) to test the relationship between peak load force rate and the weight of the object. To determine whether a linear or log-linear model best characterizes the data, we considered both a linear growth curve model and a log-linear growth curve model of the following general forms: Linear growth curve model: PLFRijt ⫽ ai ⫹ ⵜiW j ⫹ ijt Log-linear growth curve model: logPLFRijt ⫽ ai ⫹ ⵜiW j ⫹ ijt
METHODS
Subjects. Ten neurologically intact subjects with dominant right hand (mean age 26.5 ⫾ 6.42 yr, 5 men and 5 women) participated in the study. Subject recruitment and data collection took place at the Motor Recovery Research Laboratory at New York University School of Medicine. The protocols were approved by the institutional review
where PLFRijt denotes the recorded PLFR value (and the logarithmic transform of the PLFR value in the log-linear model) for the i-th subject lifting the j-th weight at the t-th trial, Wj is the j-th weight that a subject lifts (Wj ⫽ 250, 300, 350, . . . , 700 g), and ijt is the corresponding residual term. Here, i ⫽ 1, . . . , 10 subjects; j ⫽
J Neurophysiol • doi:10.1152/jn.00065.2015 • www.jn.org
A SCALING MODEL FOR MOTOR ADAPTATION
B
A
C 30
Load Force Onset
Lift-off
Light LF Light LFR Heavy LF Heavy LFR
10
25
8 20 6 15 4 10 2
Load Force Rate (Newtons/sec)
12
Load Force (Newtons)
413
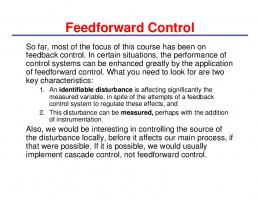
Fig. 1. A: instrumented grip device with 3-df force-torque sensors to measure the horizontal grip and the vertical load forces (a), a compartment for an exchangeable mass to change object weight (b), and a lift sensor (c). B: depiction of the grasp-and-lift task using wrist extension. C: representative data from 1 subject showing the load forces (LF; solid lines) and peak load force rates (LFR; dashed lines) on the 7th trial for lifting an object of light weight (250 g; gray lines) or heavy weight (500 g; black lines). The single vertical line indicates the onset of load force (ⱖ0.1 N); the trials were synchronized at this point. The double vertical line indicates the time of object liftoff for each of the 2 trials depicted. Loading phase refers to the time during which vertical forces are being exerted but the object has not yet been lifted.
5
0
Loading Phase -2 1.4
1.5
1.6
1.7
1.8
1.9
2
2.1
2.2
0 2.3
Time (sec)
1, . . . , 10 weights, and t ⫽ 2, . . . , 7 trials; the first trial was discarded (see RESULTS). ai and ⵜi are the subject-specific intercept and slope terms in the linear part of each model (right-hand side of the equation) and are by default treated as random effects with normal distributions ai ⬃ N(ua, 2 2a) and ⵜi ⬃ N(uⵜ, ⵜ ). Note that when the variance term 2a equals 0, the varying intercept model reduces to common intercept. Similarly, 2 when ⵜ equals 0, the varying slope reduces to common slope. We further tested three alternative hypotheses to determine the specific form of the right-hand side of the equations regarding common relationships across individuals in a healthy population. For hypothesis 1, there is one common scaling factor or slope across the healthy population. In addition, at any given weight, the level of PLFR is the same across the population. In other words, there is no variance in the intercept ai and slope ⵜi across individuals (common intercept a and slope ⵜ). Linear model A1: PLFRijt ⫽ a ⫹ ⵜ W j ⫹ ijt Log-linear model B1: logPLFRijt ⫽ a ⫹ ⵜ W j ⫹ ijt For hypothesis 2, there is one common scaling factor or slope across the healthy population. However, the level of PLFR varies by individual. In other words, there is variability in the intercept ai but not in slope ⵜi across individuals (common slope ⵜ, different intercept a). Linear model A2: PLFRijt ⫽ ai ⫹ ⵜ W j ⫹ ijt
Log-linear model B2: logPLFRijt ⫽ ai ⫹ ⵜ W j ⫹ ijt For hypothesis 3, both the scaling factor or slope and intercept differ by individual, and the variance in both the intercept ai and slope ⵜi is greater than 0 (different slope ⵜ and different intercept a). Linear model A3: PLFRijt ⫽ ai ⫹ ⵜiW j ⫹ ijt Log-linear model B3: logPLFRijt ⫽ ai ⫹ ⵜiW j ⫹ ijt Goodness-of-fit statistics such as log-likelihood and log-likelihood ratio statistics were used to compare the models. For nested models, such as the linear growth models A1, A2, and A3, we can construct log-likelihood ratio tests (LR test) to determine whether the model with more complexity fits the data better than a simpler model at the cost of the extra parameter(s). However, in the linear models the dependent variable PLFR is assumed to be normally distributed, whereas in the log-linear models log PLFR is assumed to be normally distributed; therefore, we cannot directly compare the goodness-of-fit statistics on the basis of likelihood. We therefore performed additional residual diagnosis to check the extent to which each model satisfies the distributional assumption. The goodness-of-fit comparison (Table 1) and residual diagnosis suggest that the log-linear model B2 best characterized the relationship between PLFR and object weight (see RESULTS). We then ex-
J Neurophysiol • doi:10.1152/jn.00065.2015 • www.jn.org
414
A SCALING MODEL FOR MOTOR ADAPTATION
Table 1. Goodness-of-fit comparison of the models Model
Log-Likelihood
AIC
BIC
df
A1 A2 A3 B1 B2 B3
⫺2,444.99 ⫺2,191.19 ⫺2,188.72 ⫺211.63 33.01 34.67
4,895.98 4,392.37 4,389.45 429.26 ⫺34.03 ⫺57.33
4,909.18 4,414.34 4,415.81 442.45 ⫺34.06 ⫺30.97
4 5 6 4 5 6
Comparison
Likelihood Ratio
P Value
A2 vs. A1 A3 vs. A2
507.61 4.93
⬍0.001 0.0265
B2 vs. B1 B3 vs. B2
489.26 3.30
⬍0.001 0.069
%Variance Explained 18.76 66.37 67.98 26.15 69.94 71.03
AIC, Akaike information criterion; BIC, Bayesian information criterion; df, degrees of freedom.
panded model B2 to further model the relationship between muscle activation and PLFR as follows: logPLFRijt ⫽ ai ⫹ ⵜ W j ⫹ 1 logAPBijt ⫹ 2 logECRLijt ⫹ 3 logEDCijt ⫹ 4 logFCUijt ⫹ 5 logFDIijt ⫹ 6 logFDSijt ⫹ 7 logLTijt ⫹ 8 logUTijt ⫹ ijt We used the logarithm of the normalized muscle activity as predictors in this model because it leads to more natural interpretations. For example, a unit change in log ECRL is equivalent to an increase in ECRL by e times (where e is the natural number) based on the simple logarithm calculation (1 ⫹ log ECRL) ⫽ log (e·ECRL). The coefficient of muscle activation, , is interpreted as the change in log PLFR associated with a unit increase in log ECRL, implying that a fixed percentage increase (e ⫺ 1) ⫻ 100% in muscle activation will lead to (e ⫺ 1) ⫻ 100% change in PLFR. In this sense  can be viewed as a muscle efficiency index, because it allows us to compare the effect of muscle activation on PLFR directly. The greater the value of , the greater the change in PLFR produced by the muscle. As in other regression models, the significance of the muscle efficiency index was assessed using the P value of the coefficients . RESULTS
Figure 2 plots the raw data for each subject. In each panel, PLFR is plotted against the different weights, ranging from 250 to 700 g. For each weight, there are seven data points corresponding to the seven trials. In general, three features are noted: 1) there is a consistent and positive relationship between PLFR and weight; 2) the trend line for each subject is at a different level; and 3) the slopes of the trend lines appear to be different: subjects with a higher level of PLFR also tend to have a steeper slope. We also note that the intertrial variability can be high for some subjects.
In the experiment, the weight of the object was unknown to the subjects on the first trial. Therefore, we do not expect them to have developed accurate feedforward control of fingertip forces according to the object’s weight before lifting it. From the second trial onward, we expect that the healthy subjects would have utilized the information from the prior lift(s) to show evidence of feedforward control manifested as a better correspondence between object weight and PLFR. Figure 3 plots the linear correlation coefficients between weight and PLFR for each trial averaged across all subjects. We can see that the linear correlation for the first trial is much lower than that for the second trial. From the second trial on, the correlation between PLFR and weight improves and there is little change with additional practice, suggesting that one practice lift is sufficient to develop feedforward control in healthy subjects. After removing the data for the first trial, we plotted the average PLFR over trials 2–7 for each subject at the different weights (Fig. 4A). Shown is a set of linear trend lines with different slopes, and the trend lines also appear to be located at different levels (different intercepts). This suggests that the data may be modeled using linear growth curve models with varying intercepts and varying slopes. On the other hand, we also note that subjects who have higher levels of PLFR tend to have steeper slopes, which suggests that the PLFR may increase proportionally to an individual’s baseline PLFR level as the weight increases. To model proportional change, we can fit log-linear growth curve models to the data. Figure 4B plots the average log PLFR over trials 2–7 for each subject, showing a set of parallel trend lines suggesting a simpler relationship described by a common slope and varying intercept. To rigorously determine the best model to fit the data, we fit nested linear and log-linear growth curve models to the data
Fig. 2. Peak load force rate (PLFR) for the associated weights for all the trials (n ⫽ 7) and all subjects. Each data point represents 1 trial. Data for each subject (S1–S10) are plotted in a separate panel. A trend line (with confidence band) between PLFR and weight is fitted for each subject.
J Neurophysiol • doi:10.1152/jn.00065.2015 • www.jn.org
A SCALING MODEL FOR MOTOR ADAPTATION
415
Table 2. Derived expected %change in PLFR for various weightpair differences using results from log-linear model B2 95% Confidence Intervals
Difference in Weight Pairs, g
Expected % Change in PLFR
Lower bound
Upper bound
1 50 100 150 200 250
0.0014 0.0739 0.1533 0.2386 0.3302 0.4285
0.0012 0.0632 0.1303 0.2017 0.2776 0.3583
0.0016 0.0848 0.1768 0.2766 0.3849 0.5023
PLFR, peak load force rate.
Fig. 3. Linear correlation coefficient between log PLFR and object weight at each trial, averaged over the subjects.
and compared the goodness-of-fit statistics (see Table 1). As shown in the series of LR tests, we can see that among the three linear growth curve models, model A2 performs better than model A1 (LR ⫽ 507.61, P ⬍ 0.001), and model A3 performs better than model A2 (LR ⫽ 4.93, P ⫽ 0.0265). This indicates that model A3, with varying intercept and varying slope, performs significantly better than models A2 and A1. On the other hand, among the three log-linear growth curve models, model B2 performs significantly better than model B1 (LR ⫽ 489.26, P ⬍ 0.001), but the more complex model B3 does not significantly improve the model fit (LR ⫽ 3.30, P ⫽ 0.065). Therefore, model B2 is preferred among the three log-linear models. Although we cannot directly compare model A3 and model B2 because of different distributional assumptions made under these two models, we performed additional residual diagnosis tests to check whether each model satisfied the distributional assumption. A comparison of the quantile-quantile plots of the standardized residuals against a standard normal variable for linear
growth curve models and log-linear growth curve models (not shown) suggested that the distributional assumption is better respected for the log-linear model. Furthermore, we used the percentage of the variance explained as an additional indicator to compare the models. We found that 67.98% of the variance was explained with linear model A3 when 6 parameters were used (df ⫽ 6), whereas 69.94% of the variance was explained with log-linear model B2 when one fewer parameter was used (df ⫽ 5). The log-linear model B2 is the model of choice, because it respects the distributional assumption better and explains greater variability in the data with fewer parameters than the linear model A3. Under the log-linear model, the coefficient ⵜ can be translated as a proportional change in PLFR as weight increases. As shown in the simple derivation below, the slope ⵜ can also be interpreted in terms of percent change in PLFR resulting from a weight change. For a unit increase in weight, we expect that the PLFR will change proportionally by [exp (ⵜ) ⫺ 1] ⫻ 100%: log PLFR ⫽ a ⫹ ⵜ W ⵜ ⫽ log PLFRW⫹1 ⫺ log PLFRW exp共 ⵜ 兲 ⫽ PLFRW⫹1 ⁄ PLFRW Table 2 reports the derived proportional scaling factors based on log-linear model B2 and provides an empirical guide on how PLFR changes with weight after practice among
Fig. 4. Average PLFR for trials 2–7 at each corresponding object weight (A) and the average log PLFR for trials 2–7 at each corresponding object weight (B). Each line represents a subject. J Neurophysiol • doi:10.1152/jn.00065.2015 • www.jn.org
416
A SCALING MODEL FOR MOTOR ADAPTATION
change in muscle activation leads to a large change in PLFR, i.e., greater muscle efficiency. We found that only activity in the extensor muscles of the wrist (ECRL) and fingers (EDC) and the intrinsic finger flexor (FDI) used to grip the object were significantly related to the change in PLFR (Fig. 6A). To further understand the relationship between extensor activation and the PLFR at a subject level, we modeled the effect of the wrist and fingers extensors (both muscles extend the wrist) as a random coefficient to accommodate individual variability in muscle efficiency. The model showed a high correlation between the level of PLFR and extensor efficiency (r ⫽ 0.98, P ⬍ 0.001). This suggests that individuals that recruit the extensor muscles more efficiently show higher PLFR levels (faster rate of change of load force; Fig. 6B). DISCUSSION
Fig. 5. Predicted relationship between PLFR and object weight. The solid line represents the average relationship between PLFR and weight, and each of the dashed lines represents the relationship between PLFR and weight for a pseudo subject randomly drawn from the fitted distribution.
healthy subjects within a range of weights commonly encountered in daily activities (200 –700 g). The model reports a 0.14% change in PLFR per gram of weight increase: [exp (0.14) ⫺ 1] ⫻ 100%. Put in a more realistic context, this model predicts that the PLFR value will increase by 7.4% {[exp (0.14 ⫻ 50) ⫺ 1] ⫻ 100% (95%CI 6.32– 8.48%)} when the weight of the object increases by 50 g, by 15.33% {[exp (0.14 ⫻ 100) ⫺ 1] ⫻ 100% (95%CI 13.03–17.68%)} when the weight of the object increases by 100 g, and so on. Although the PLFR scales proportionally with weight, model B2 also reveals substantial individual variability in the overall level of PLFR. Figure 5 demonstrates the predicted relationship between PLFR and weight for 100 hypothetical subjects. The solid line indicates a subject with mean level of PLFR in the population. To understand the relationship of muscle activity to PLFR, we expanded model B2 to include the normalized activity of eight muscles involved in the task. Muscle activity was also transformed to the logarithm scale so that the slope coefficients for muscles could be interpreted as percent contribution of specific muscles to percent change in PLFR. A large and positive coefficient of muscle activation suggests that a unit
Optimal hand function requires the hand to sense object properties, such as its weight, and manipulate the object accordingly. In this article, we have established a scaling model for the relationship between fingertip peak load force rates and object weight. We found that after one practice lift, the PLFR, a measure of feedforward control of fingertip forces, scales proportionally to weight, and importantly, the proportionality is common among healthy subjects. Moreover, the baseline level of PLFR varied across individuals and was related to the efficiency of the muscles involved in lifting the object, in this case the muscles that extend the wrist. These results quantify feedforward control during grasp and lift among healthy individuals and provide new benchmarks for assessing the effect of interventions on feedforward control in impaired populations, such as in patients with stroke, cerebral palsy, multiple sclerosis, and other forms of brain injury. Proportional scaling of rate of change of load force to object weight. Johansson and colleagues initiated the examination of fingertip force coordination during object manipulation [see Johansson (1998) for review]. Their results have been used to study sensorimotor integration in healthy individuals, and their model has been found to be sensitive in detecting impairment in fine motor control in various patient populations (Fellows et al. 1998; Gibbs et al. 2008; Gordon et al. 1997, 1999; Schwarz et al. 2001). It has been shown that the rate of change of load force before lifting an object is faster for a heavier weight than for a lighter weight in healthy individuals after one to three trials, resulting in a higher PLFR for a heavy object compared
Fig. 6. A: the regression coefficient  of the log normalized activity of the muscles in the extended log-linear model B2 represents muscle efficiency. APB, abductor pollicis brevis; ECRL, extensor carpi radialis longus; EDC, extensor digitorum communis; FCU, flexor carpi ulnaris; FDS, flexor digitorum superficialis; LT, lower trapezius; UT, upper trapezius. *P ⬍ 0.05; ***P ⬍ 0.001. B: the efficiency of the extensor muscles (ECRL and EDC) were highly correlated with the level of log PLFR for each subject. Each data point represents a subject. The extensor efficiency is the predicted random coefficient for each subject, and the level of log PLFR is the predicted log PLFR at a weight of 450 g for each subject.
J Neurophysiol • doi:10.1152/jn.00065.2015 • www.jn.org
A SCALING MODEL FOR MOTOR ADAPTATION
with a lighter object (Johansson and Westling 1988b). However, a clear difference in PLFR values between light and heavy objects was not seen in a population of patients with stroke despite several practice trials suggesting a lack of feedforward control poststroke (Raghavan et al. 2006). However, the degree of impairment of feedforward control and the reason for the impairment have been difficult to quantify. In this context, the scaling model that we have developed using healthy individuals can serve as a benchmark to more effectively quantify the extent of the impairment in feedforward control in various populations, to conduct experiments to understand the reason for impairment in feedforward control, and to assess improvement in feedforward control with specific interventions. For example, a patient with stroke may be instructed to lift two objects of different weights over multiple trials. Using the scaling model, we can ask: 1) Do the patients scale their peak load force rate proportionally to the weight of the object? 2) After how many trials can we see the scaling effect, if any? 3) What feedback strategies can assist with the scaling of the fingertip load forces to object weight? 4) Is the effect stable within and between sessions? 5) What changes in muscle activity correlate with the improvement in scaling? Answers to these questions will help delineate the extent of impairment and the type of treatment that would help restore feedforward control of fingertip forces, which is necessary for adapting hand function to perform activities of daily living, such as lifting objects of various weights. Relationship of muscle activity to feedforward control. Muscle recruitment patterns are crucial for understanding the formation of weight-related internal representations underlying feedforward control of fingertip forces. Perceived heaviness can inform muscular output (Aniss et al. 1988; Flanagan and Bandomir 2000; Gandevia and Kilbreath 1990). This is thought to occur via corollary discharge signals originating within the central nervous system (Gandevia 1996). However, perceived magnitude of force has been shown to vary as a function of the muscle group generating the force (Jones 2003). EMG patterns have been shown to correlate with feedforward control to object weight during grasping and lifting in healthy individuals (Johansson and Westling 1988a). Furthermore, a change in the spatial tuning patterns of EMG activity has been shown to correlate with motor learning in healthy subjects (Thoroughman and Shadmehr 1999). This change is thought to reflect the formation of an internal representation of the learned behavior. Our results concur with these previous findings in that of the eight muscles from which we recorded, the muscles engaged in lifting the object (primarily the extensors of the wrist) were the only ones whose activity was related to the PLFR before the object was lifted, across the different weights. In addition, our results show that the efficiency of muscle recruitment was related to the level of PLFR, implying that individuals who use their extensors more efficiently are likely to show higher PLFR levels for a given object weight. Furthermore, the relationship between muscle activity patterns and feedforward control suggests how changes to the internal representation of the movement in the brain influence the descending command for translation to behavior via the temporal and spatial control of neuromuscular activity during grasping. Therefore, applying our scaling model to individuals with abnormal EMG activity, such as that following a stroke, could be especially valuable in
417
understanding how restoration of feedforward control can improve motor execution. Conclusion. This study provides a theoretical model that quantifies how fingertip lifting forces scale proportionally to weight in healthy controls. This model provides a benchmark to interpret data from other populations in whom feedforward control of fingertip forces may be impaired, as well as a means to assess improvement in feedforward control and its relationship to muscular control. ACKNOWLEDGMENTS We thank Peter Thai, David Rhee, and Qiang Lin for assistance with data collection. GRANTS This work was supported by National Institute of Child Health and Human Development Grants K23HD049472 and R01HD071978 (to P. Raghavan). DISCLOSURES No conflicts of interest, financial or otherwise, are declared by the authors. AUTHOR CONTRIBUTIONS Y.L. and P.R. conception and design of research; Y.L. and S.B. analyzed data; Y.L., S.B., V.A., and P.R. interpreted results of experiments; Y.L., S.B., and P.R. prepared figures; Y.L., S.B., V.A., and P.R. drafted manuscript; Y.L., S.B., V.A., and P.R. edited and revised manuscript; Y.L., S.B., V.A., and P.R. approved final version of manuscript; S.B. performed experiments. REFERENCES Aniss AM, Gandevia SC, Milne RJ. Changes in perceived heaviness and motor commands produced by cutaneous reflexes in man. J Physiol 397: 113–126, 1988. Blakemore SJ, Goodbody SJ, Wolpert DM. Predicting the consequences of our own actions: the role of sensorimotor context estimation. J Neurosci 18: 7511–7518, 1998. Davidson PR, Wolpert DM. Internal models underlying grasp can be additively combined. Exp Brain Res 155: 334 –340, 2004. Drake C, Palmer C. Skill acquisition in music performance: relations between planning and temporal control. Cognition 74: 1–32, 2000. Fellows SJ, Noth J, Schwarz M. Precision grip and Parkinson’s disease. Brain 121: 1771–1784, 1998. Fitzmaurice G, Laird N, Ware J. Applied Longitudinal Analysis. Hoboken, NJ: John Wiley and Sons, 2011. Flanagan JR, Bandomir CA. Coming to grips with weight perception: effects of grasp configuration on perceived heaviness. Percept Psychophys 62: 1204 –1219, 2000. Flanagan JR, King S, Wolpert DM, Johansson RS. Sensorimotor prediction and memory in object manipulation. Can J Exp Psychol 55: 87–95, 2001. Gandevia SC. Kinesthesia: roles for afferent signals and motor commands. In: Handbook of Physiology. Exercise: Regulation and Integration of Multiple Systems. Bethesda, MD: Am Physiol Soc, 1996, sect. 12, p. 128 –172. Gandevia SC, Kilbreath SL. Accuracy of weight estimation for weights lifted by proximal and distal muscles of the human upper limb. J Physiol 423: 299 –310, 1990. Gibbs A, Pearse EJ, Sheehan JA, Meleady KT, Jayasinha H, Jones N. Estimating and projecting subacute care demand: findings from a review of international methods. Aust Health Rev 32: 778 –785, 2008. Gordon AM, Charles J, Duff SV. Fingertip forces during object manipulation in children with hemiplegic cerebral palsy. II: bilateral coordination. Dev Med Child Neurol 41: 176 –185, 1999. Gordon AM, Ingvarsson PE, Forssberg H. Anticipatory control of manipulative forces in Parkinson’s disease. Exp Neurol 145: 477– 488, 1997. Gordon AM, Westling G, Cole KJ, Johansson RS. Memory representations underlying motor commands used during manipulation of common and novel objects. J Neurophysiol 69: 1789 –1796, 1993.
J Neurophysiol • doi:10.1152/jn.00065.2015 • www.jn.org
418
A SCALING MODEL FOR MOTOR ADAPTATION
Hermsdorfer J, Hagl E, Nowak DA, Marquardt C. Grip force control during object manipulation in cerebral stroke. Clin Neurophysiol 114: 915–929, 2003. Huang VS, Haith A, Mazzoni P, Krakauer JW. Rethinking motor learning and savings in adaptation paradigms: model-free memory for successful actions combines with internal models. Neuron 70: 787– 801, 2011. Johansson RS. Sensory input and control of grip. Novartis Found Symp 218: 45–59, 1998. Johansson RS, Westling G. Coordinated isometric muscle commands adequately and erroneously programmed for the weight during lifting task with precision grip. Exp Brain Res 71: 59 –71, 1988a. Johansson RS, Westling G. Programmed and triggered actions to rapid load changes during precision grip. Exp Brain Res 71: 72– 86, 1988b. Jones LA. Perceptual constancy and the perceived magnitude of muscle forces. Exp Brain Res 151: 197–203, 2003. Kawato M, Wolpert D. Internal models for motor control. Novartis Found Symp 218: 291–304, 1998. Krakauer JW, Mazzoni P. Human sensorimotor learning: adaptation, skill, and beyond. Curr Opin Neurobiol 21: 636 – 644, 2011. Lai SM, Studenski S, Duncan PW, Perera S. Persisting consequences of stroke measured by the Stroke Impact Scale. Stroke 33: 1840 –1844, 2002.
Nowak DA, Hermsdorfer J, Topka H. Deficits of predictive grip force control during object manipulation in acute stroke. J Neurol 250: 850 – 860, 2003. Pinheiro JC, Bates DM. Mixed-Effects Models in S and S-PLUS. New York: Springer, 2000. Raghavan P, Krakauer JW, Gordon AM. Impaired anticipatory control of fingertip forces in patients with a pure motor or sensorimotor lacunar syndrome. Brain 129: 1415–1425, 2006. Raghavan P, Santello M, Gordon AM, Krakauer JW. Compensatory motor control after stroke: an alternative joint strategy for object-dependent shaping of hand posture. J Neurophysiol 103: 3034 –3043, 2010. Schwarz M, Fellows SJ, Schaffrath C, Noth J. Deficits in sensorimotor control during precise hand movements in Huntington’s disease. Clin Neurophysiol 112: 95–106, 2001. Shadmehr R, Smith MA, Krakauer JW. Error correction, sensory prediction, and adaptation in motor control. Annu Rev Neurosci 33: 89 –108, 2010. Thoroughman KA, Shadmehr R. Electromyographic correlates of learning an internal model of reaching movements. J Neurosci 19: 8573– 8588, 1999. Wolpert DM, Ghahramani Z, Jordan MI. An internal model for sensorimotor integration. Science 269: 1880 –1882, 1995. Wolpert DM, Miall RC. Forward models for physiological motor control. Neural Netw 9: 1265–1279, 1996.
J Neurophysiol • doi:10.1152/jn.00065.2015 • www.jn.org