Journal of Adolescent Health 48 (2011) 100 –102
www.jahonline.org Adolescent health brief
HIV-Infected Adolescents: Relationship Between Atazanavir Plasma Levels and Bilirubin Concentrations Ana P. Nso, M.D., Ph.D.a,*, Beatriz Larru, M.D., Ph.D.b, Jose M. BellÔn, Ph.D.b, Maria JosÊ Mellado, M.D., Ph.D.c, Jose T. Ramos, M.D., Ph.D.d, Maria Isabel GonzÂlez, M.D., Ph.D.e, Maria Luisa Navarro, M.D., Ph.D.f, Maria A´ngeles MuÒoz-FernÂndez, M.D., Ph.D.b,g, and Maria Isabel de JosÊ, M.D., Ph.D.a a
Servicio de Pediatrìa, Hospital Infantil La Paz, Madrid, Spain Laboratorio de Inmuno-Biologìa Molecular, Hospital General Universitario “Gregorio Maraðòn”, Madrid, Spain Servicio de Pediatrìa-Infecciosas, Hospital Universitario “Carlos III”, Madrid, Spain d Servicio de Pediatrìa-Infecciosas, Hospital de Getafe, Madrid, Spain e Servicio de Pediatrìa-Infecciosas, Hospital Universitario “Doce de Octubre”, Madrid, Spain f Servicio de Pediatrìa-Infecciosas, Hospital General Universitario “Gregorio Maraðòn”, Madrid, Spain g Unidad Asociada de Retrovirologìa Humana, HGUGM-CSIC, Madrid, Spain b c
Article history: Received November 11, 2009; Accepted May 13, 2010 Keywords: Atazanavir; Children; HIV; Therapeutic drug monitoring
A B S T R A C T
The use of atazanavir (ATV) in adolescents infected with human immunodeficiency virus was analyzed in this study. ATV morning plasma concentrations were determined during regular visits to the outpatient department. Results showed that bilirubin levels were higher among patients with higher ATV plasma concentrations (p ⫽ .018). Monitoring plasma levels of ATV could avoid toxicity in these patients. 䉷 2011 Society for Adolescent Health and Medicine. All rights reserved.
Morbidity and mortality of patients infected with human immunodeficiency virus (HIV) have improved dramatically since the introduction of highly active antiretroviral therapy [1]. However, 20%–50% of them still present with viral failure [2]. Atazanavir (ATV) is a protease inhibitor widely used for the treatment of adults infected with HIV [3], but with limited use in treatment of adolescents. Its major associated secondary effect is reversible elevation of bilirubin [4]. The aim of this study was to analyze the use of ATV in a cohort of adolescents. Methods This study has been performed as part of the protocol for measuring antiretroviral concentrations which was carried out
* Address correspondence to: Ana P. Nso, M.D., Ph.D., Servicio de PediatrÎa, Hospital de Torrevieja, Ctra Torrevieja-San Miguel CV 95, Partida la CeÒuela, Torrevieja, Spain. E-mail address:
[email protected] (A.P. Nso).
at five hospitals in Madrid, Spain, between the years 2006 and 2008. Institutional approval for the study was granted by the Research Ethics Committee. Written informed consent was obtained before enrollment. Subjects eligible for the study included adolescents with documented vertical HIV-1 infection and a treatment regimen including ATV. Children known to have renal, hepatic, or intestinal disease and patients receiving concomitant drugs known to have pharmacokinetic interactions with antiretroviral drugs were excluded from this study. ATV plasma concentrations were determined during regular visits to the outpatient department by using a validated UV-high performance liquid chromatography assay [5]. Results were compared with that expected from adult patients on the basis of time taken between intake and sampling. Total bilirubin was measured contemporaneously and a bilirubin increase of ⬎2 mg/dL was considered as a safety cut-off. Quantitative data were compared using 2 test. Quantitative data association was analyzed with Mann–Whitney U test. Spearman’s correlation was used to estimate the association between ATV concentration and serum bilirubin.
1054-139X/$ - see front matter 䉷 2011 Society for Adolescent Health and Medicine. All rights reserved. doi:10.1016/j.jadohealth.2010.05.009
A.P. Nso et al. / Journal of Adolescent Health 48 (2011) 100 –102
101
Table 1 Baseline characteristics of patients receiving a combination including atazanavir
Weight (kg) Gender Age (years) Tanner stage CDC status Treatment compliance CD4% CD8% Log10VL ARV regimen
Patient 1
Patient 2
Patient 3
Patient 4
Patient 5
47 F 18 5 B Intermediate
50.5 F 15.3 4 B Intermediate
52.5 F 15.4 5 B Good
50 F 13.1 3 C Good
48.5 F 12.4 3 C Good
29.5 44.3 1.70 ATV/RTNFFTC
21.5 41.9 1.70 ATV/RABCddI
30 34 3.75 ATV/RFTCTNF
37 35 1.70 ATV/RABCEFV
21 25 5.89 ATV/R3TCABCEFV
F ⫽ female; CDC ⫽ Centers for Disease Control and Prevention; Log10VL ⫽ viral load logarithm; ARV ⫽ antiretroviral; ATV/R ⫽ atazanavir ⫹ ritonavir; TNF ⫽ tenofovir; FTC ⫽ emtricitabine; ABC ⫽ abacavir; ddI ⫽ didanosine; EFV ⫽ efavirenz; 3TC ⫽ lamivudine.
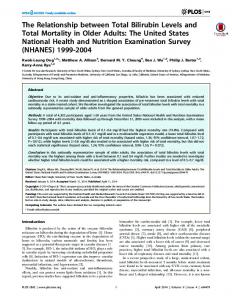
Results Of the 129 patients in the cohort, five received ATV containing highly active antiretroviral therapy and were included in this study. All the participants were female adolescents with previous treatment failure and receiving a night dose of 300 mg ATV and 100 mg ritonavir. The median age was 15.5 years (range, 12.4 –18 years), and the demographic characteristics are summarized in Table 1. A total of 16 samples were collected during follow-up, at a mean time of 12.5 hours after previous dose intake (standard deviation [SD] ⫽ .5 hours). As expected, all the tested samples had ATV concentrations that were more than the recommended ATV 24-hour concentration of 150 ng/mL. The mean concentration of ATV in adolescents was 1,474.06 ng/mL, slightly lower than the 2,000 ng/mL obtained in adults 12–13 hours after intake of the same dose [6]. There was considerable inter-individual variability in plasma concentrations having a broad range of values and a large coefficient of variation (82.4%). None of the patients presented with ATV-resistance mutations. Mean bilirubin level was significantly higher among patients with ATV-containing regimen (2 mg/dL) as compared with those without ATV treatment (.47 mg/dL) (p ⫽ .001). Among adolescents treated with ATV, mean total bilirubin was 1.5 mg/dL (SD ⫽ .9 mg/dL) in patients with ATV plasma level ⬍2,000 ng/mL. In contrast, patients with ATV plasma concentrations ⬎2,000 ng/mL had significantly higher bilirubin levels, with a mean of 3.1 mg/dL (SD ⫽ 1.0 mg/dL). Differences were statistically significant (p ⫽ .018). Serum bilirubin concentrations correlated significantly with higher ATV concentrations (Spearman’s r ⫽ .72, p ⫽ .006). This correlation is represented in Fig. 1. The severity of jaundice was mild among patients with hyperbilirubinemia and none of them required treatment discontinuation because of this secondary effect.
women. Nevertheless, previous studies [7] have demonstrated that gender does not influence ATV plasma concentration levels. ATV is administered once daily, usually at night, as determination of ATV trough concentration generates technical difficulties and morning monitoring of this drug is easier in clinical practice. In the present study, samples were obtained between 12 and 13 hours after administration of the night dose. To interpret our results, area under the curve records in adults was used to predict trough concentrations [8]. The analysis of the model used confirms that predictions are both precise and unbiased. Therefore, using a 12-hour threshold could be useful for the monitoring of ATV toxicity in patients receiving ATV at night, with the inherent limitations of using adult studies for adolescent population. A strong correlation between high ATV levels and hyperbilirubinemia has been shown in this study because of the competitive inhibition of the UDP-glycuronyltransferase (UGT1A1) enzyme by ATV [9]. Patients did not need a change in their treatment regimen as a result of this outcome, probably because jaundice is a mild and reversible effect that does not affect therapy regimen modification in multitreated patients. However, jaundice might be an uncomfortable secondary effect, especially for the population mentioned earlier. Physical appearance influ-
Discussion ATV is a relatively recent protease inhibitor. The present study was designed to provide more data on the use of ATV in adolescents infected with HIV. In this study, all participants were aged ⬎12 years received their third or superior line of treatment because of multiple previous failures. This illustrates the fact that ATV is used in adolescents as a rescue drug. Remarkably, all our patients were
Figure 1. Correlation between bilirubin (total and unconjugated) serum levels and atazanavir plasma concentrations. rs ⫽ Spearman’s r.
102
A.P. Nso et al. / Journal of Adolescent Health 48 (2011) 100 –102
ences a major part of the self-esteem of an adolescent and a symptom-like jaundice can lead to body dissatisfaction and social adjustment problems because of visible physical differences. ATV plasma level can decrease when it is administered simultaneously with other drugs. Therefore, it is frequently boosted with ritonavir. However, this boosting is related to an increase in its toxicity, especially hyperbilirubinemia [10]. Further analyses are required to evaluate the risks and benefits of a simplification switch from ritonavir-boosted ATV to ATV-alone so as to decrease toxicity. Adequacy of the adult dose for adolescents has not yet been established. The preliminary findings of this study show that adolescents with regimens including ATV present higher bilirubin levels more frequently as compared with the other patients. Therefore, plasma measurements of ATV levels could be useful in monitoring ATV toxicity, for selected patients with elevated unconjugated bilirubin or jaundice. Acknowledgments This work has been supported by grants from the (FIPSE); (FIS); (). A.P. Nso and B. Larru contributed to this study with protocol development, collecting and recording data, and writing the manuscript. The analytic framework was done by J. M. BellÔn. Patient screening was performed by M. J. Mellado, J. T. Ramos, M. I. GonzÂlez, M. L. Navarro,. M. I. de JosÊ contributed to the study with patient screening and writing of the manuscript. M. . MuÒoz-FernÂndez supervised design and execution of the study. All authors read and approved the final manuscript.
References [1] de Martino M, Tovo PA, Balducci M, et al. Reduction in mortality with availability of antiretroviral therapy for children with perinatal HIV-1 infection. Italian Register for HIV Infection in Children and the Italian National AIDS Registry. JAMA 2000;284:190 –7. [2] Ribera E, Lopez-Cortes LF, Soriano V, et al. Therapeutic drug monitoring and the inhibitory quotient of antiretroviral drugs: Can they be applied to the current situation? Enferm Infecc Microbiol Clin 2005;23:55– 67. [3] Macassa E, Delaugerre C, Teglas JP, et al. Change to a once-daily combination including boosted atazanavir in HIV-1-infected children. Pediatr Infect Dis J 2006;25:809 –14. [4] Smith DE, Jeganathan S, Ray J. Atazanavir plasma concentrations vary significantly between patients and correlate with increased serum bilirubin concentrations. HIV Clin Trials 2006;7:34 – 8. [5] Sarasa-Nacenta M, Lopez-Pua Y, Mallolas J, et al. Simultaneous determination of the HIV-protease inhibitors indinavir, amprenavir, ritonavir, saquinavir and nelfinavir in human plasma by reversed-phase high-performance liquid chromatography. J Chromatogr B Biomed Sci Appl 2001;757:325–32. [6] Burger DM, Agarwala S, Child M, et al. Effect of rifampin on steady-state pharmacokinetics of atazanavir with ritonavir in healthy volunteers. Antimicrob Agents Chemother 2006;50:3336 – 42. [7] von Hentig N, Babacan E, Lennemann T, et al. The steady-state pharmacokinetics of atazanavir/ritonavir in HIV-1-infected adult outpatients is not affected by gender-related co-factors. J Antimicrob Chemother 2008;62: 579 – 82. [8] Dickinson L, Boffito M, Back D, et al. Population pharmacokinetics of ritonavirboosted atazanavir in HIV-infected patients and healthy volunteers. J Antimicrob Chemother 2009;63:1233– 43. [9] Zhang D, Chando TJ, Everett DW, et al. In vitro inhibition of UDP glucuronosyltransferases by atazanavir and other HIV protease inhibitors and the relationship of this property to in vivo bilirubin glucuronidation. Drug Metab Dispos 2005;33:1729 –39. [10] Molto J, Santos JR, Valle M, et al. Monitoring atazanavir concentrations with boosted or unboosted regimens in HIV-infected patients in routine clinical practice. Ther Drug Monit 2007;29:648 –51.