May 10, 2017 - specific findings, and HLA B51 and A26 were negative. Based on these CD/. Behçet's diseaseâlike findings, we trea- ted the patient with oral ...
Inflamm Bowel Dis � Volume 23, Number 6, June 2017
Letters to the Editor
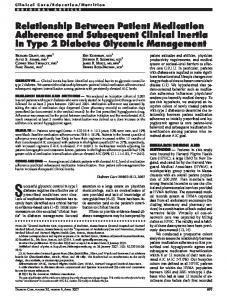
FIGURE 1. Endoscopic and histopathological findings. A longitudinal ulcer in the terminal ileum (A) and round ulcers in the middle esophagus (B) were detected by colonoscopy and esophagogastroduodenoscopy, respectively. Biopsy specimens revealed no specific findings except for inflammatory cellular infiltrates (C).
revealed a longitudinal ulcer in the terminal ileum (Fig. 1A). Esophagogastroduodenoscopy showed round ulcers in the middle esophagus (Fig. 1B). Biopsy specimens revealed no specific findings except for inflammatory cellular infiltrates (Fig. 1C). Stool culture and an examination by an ophthalmologist showed no specific findings, and HLA B51 and A26 were negative. Based on these CD/ Behc¸et’s disease–like findings, we treated the patient with oral prednisolone (40 mg/d). Two months later, no recurrent lesions were seen on colonoscopy, esophagogastroduodenoscopy, or a skin examination except for a longitudinal ulcer scar in the terminal ileum. The risk of paradoxical psoriasis has been reported to be as high as 1.6% to 10.1% in patients with CD treated with tumor necrosis factor-alpha inhibitors,3 which are also used for the treatment of psoriasis. Although the mechanism underlying paradoxical psoriasis has not yet been elucidated, an imbalance of cytokines is suspected to be involved.3 The blockade of IL-17 may also induce an imbalance in the cytokine levels, thereby resulting in the onset of CD or Behc¸et’s disease.
Hisashi Shiga, MD, PhD Sho Fukuda, MD Katsunori Iijima, MD, PhD Department of Gastroenterology and Neurology Akita University Graduate School of Medicine Akita, Japan
REFERENCES 1. Hueber W, Sands BE, Lewitzky S, et al. Secukinumab, a human anti-IL-17A monoclonal antibody, for moderate to severe Crohn’s disease: unexpected results of a randomised, double-blind placebo-controlled trial. Gut. 2012;61:1693–1700. 2. Targan SR, Feagan B, Vermeire S, et al. A randomized, double-blind, placebo-controlled phase 2 study of Brodalumab in patients with moderate-to-severe Crohn’s disease. Am J Gastroenterol. 2016;111: 1599–1607. 3. Fréling E, Baumann C, Cuny JF, et al. Cumulative incidence of, risk factors for, and outcome of dermatological complications of anti-TNF therapy in inflammatory bowel disease: a 14-year experience. Am J Gastroenterol. 2015;110:1186–1196.
Relationship Between Patient Knowledge and Medication Adherence in Inflammatory Bowel Disease To the Editor: Despite advances in pharmacologic and surgical treatment strategies, patients’ understanding and knowledge of their inflammatory bowel disease (IBD) varies widely and has lagged behind such advances despite current gastrointestinal evidence-based guidelines that underscore Statistical analysis reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award number UL1TR001417. The department of M. S. Mulekar and B. Wang received funding from this grant.
The authors have no conflict of interest to disclose. Copyright © 2017 Crohn’s & Colitis Foundation DOI 10.1097/MIB.0000000000001156 Published online 10 May 2017.
the importance of patient education.1 Patients’ understanding of their disease processes correlates with better outcomes in many chronic relapsing and remitting illnesses. The aim of this study was to see whether a correlation exists between patients’ knowledge of inflammatory bowel disease and medication adherence, as perceived by both the patient and the physician. Two hundred one consecutive outpatients at one academic Crohn’s and Colitis Center (University of Miami, Miami, FL) enrolled. All patients completed the validated 24-question Crohn’s and Colitis Knowledge Score (CCKNOW)2 and a 3-question Medication Adherence Questionnaire (MAQ)3 survey (3; maximum adherence) at an office visit waiting to see a provider. Physicians then completed a validated Clinical Rating Scale,4 scored 1 to 7 (maximum adherence), to assess their perception of the patients’ medication adherence after the visit encounter. Two hundred one patients completed the study, 87 men (43.3%) and 114 women (56.7%). Disease type included the following: 122 (60.7%) Crohn’s disease, 68 (33.8%) ulcerative colitis, 11 (5.5%) indeterminate. Mean age was 40.2 6 15.1 years. Mean overall survey scores were as follows: CCKNOW 10.94 6 4.98 of 24, MAQ 2.28 6 0.88 of 3, and Clinical Rating Scale 6.07 6 1.16 of 7. No baseline differences in mean CCKNOW scores were noted between either sex or type of disease. No statistically significant differences were noted in the mean inflammatory bowel disease knowledge of patients as assessed by the overall CCKNOW scores for different levels of medication adherence as assessed by the overall MAQ in total, by individual MAQ questions, or by the Clinical Rating Scale score (Table 1). To conclude, our study results suggest that no association between patients’ disease knowledge and patient or physician perception of medication adherence exists. Regardless, higher knowledge has yet to show significant positive association with key objective clinical www.ibdjournal.org |
Copyright © 2017 Crohn’s & Colitis Foundation. Unauthorized reproduction of this article is prohibited.
E39
Inflamm Bowel Dis � Volume 23, Number 6, June 2017
Letters to the Editor
TABLE 1. Summary of CCKNOW Scores and Medication Adherence Measures Survey
% Response
CCKNOW Score Overall (n ¼ 201) Crohn’s disease (n ¼ 122) Ulcerative colitis (n ¼ 68) Indeterminate (n ¼ 11) MAQ1 No (n ¼ 75) Yes (n ¼ 124) MAQ2 No (n ¼ 37) Yes (n ¼ 163) MAQ3 No (n ¼ 32) Yes (n ¼ 168) Overall MAQ All 3 No (n ¼ 7) One Yes (n ¼ 35) 2 Yes (n ¼ 53) All 3 Yes (n ¼ 104) CRS score 3 (n ¼ 8) 4 (n ¼ 16) 5 (n ¼ 31) 6 (n ¼ 44) 7 (n ¼ 102)
Mean 6 SD 6 6 6 6
60.7 33.8 5.5
10.94 11.23 10.35 10.88
4.98 0.45 0.60 1.76
37.7 62.3
10.35 6 4.68 11.23 6 5.15
18.5 81.5
10.84 6 5.24 10.94 6 4.94
16.0 84.0
10.59 6 5.09 10.98 6 4.98
3.5 17.6 26.6 52.3
8.86 11.34 10.11 11.28
6 6 6 6
4.06 4.90 5.14 4.97
4.0 8.0 15.4 21.9 50.8
10.38 10.56 10.39 12.02 10.74
6 6 6 6 6
1.77 1.25 0.90 0.75 0.49
MAQ scale 0 to 3. CRS scale 0 to 7. No 0, 1, and 2 scores were observed for CRS. Percentages may not add up to 100% because of rounding. CRS, Clinician Rating Scale.
parameters, such as colorectal cancer risk or intestinal inflammation (as measured by fecal calprotectin).5 As greater knowledge of disease seems to positively impact other chronic relapsing and remitting illnesses, research investigating other factors
E40
contributing to optimal medication adherence should be undertaken.
Andrew C. Berry, DO* Kevin Dholaria, MD†
Frank Czul-Gurdian, MD† Erin Forster, MD† Vibhu Chittajallu, BS‡ Erica Graff, BS‡ Danny J. Avalos, MD§ Madhuri S. Mulekar, PhDk Bin Wang, PhDk Amar R. Deshpande, MD† *Department of Medicine University of South Alabama Mobile, Alabama † Division of Gastroenterology Miller School of Medicine University of Miami Miami, Florida ‡ Miller School of Medicine University of Miami Miami, Florida § Division of Gastroenterology Texas Tech University Health Sciences Center El Paso El Paso, Texas k Department of Mathematics and Statistics University of South Alabama Mobile, Alabama
REFERENCES 1. Carter MJ, Lobo AJ, Travis SP, et al. Guidelines for the management of inflammatory bowel disease in adults. Gut. 2004;53(suppl 5):V1–V16. 2. Eaden JA, Abrams K, Mayberry JF. The Crohn’s and Colitis knowledge score: a test for measuring patient knowledge in inflammatory bowel disease. Am J Gastroenterol. 1999;94:3560–3566. 3. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24:67–74. 4. Kemp R, Hayward P, Applewhaite G, et al. Compliance therapy in psychotic patients: randomised controlled trial. BMJ. 1996;312:345–349. 5. Eaden JA, Abrams K, Mayberry JF. Does patient knowledge affect the colorectal cancer risk in ulcerative colitis? Postgrad Med J. 2002;78:615–618.
| www.ibdjournal.org
Copyright © 2017 Crohn’s & Colitis Foundation. Unauthorized reproduction of this article is prohibited.




























![Improving Patient Medication Adherence [PDF]](https://m.moam.info/img/260x300/improving-patient-medication-adherence-pdf_6479d0ee098a9ee37d8b4658.jpg)















![Patient-Reported Medication Adherence Barriers Among Patients with ... [PDF]](https://m.moam.info/img/260x300/patient-reported-medication-adherence-barriers-amo_647d26e8098a9ede188b4586.jpg)
