Sociology of Health & Illness Vol. 28 No. 7 2006 ISSN 0141–9889, pp. 927–950 doi: 10.1111/j.1467-9566.2006.00513.x Lorelei O General riginal Jones Article practitioners and Judith and Green shifting discourses of professionalism Blackwell Oxford, Sociology SHIL © 0141-9889 7 28 Blackwell UK Publishing ofPublishing Health &Ltd Illness Ltd/Editorial Board 2006
Shifting discourses of professionalism: a case study of general practitioners in the United Kingdom Lorelei Jones1 and Judith Green2 1
National Collaborating Centre for Women and Children’s Health, Royal College of Obstetrics and Gynaecology 2 Health Services Research Unit, London School of Hygiene and Tropical Medicine
Abstract
This paper addresses shifting constructions of professional identity in the context of debates about reflexive modernisation and the changing role of professionals in the provision of primary healthcare. Data are drawn from interviews with 20 early-career general practitioners (GPs), who accounted for their orientations towards work in rather different ways from those typically reported in much primary care research. In particular, they reported high job satisfaction and success in achieving what they called ‘nice work’. We argue that these GPs typify a shift in discourses of professionalism, characterised by respondents as the ‘new general practice’, which explicitly rejects many values attributed to ‘traditional’ general practice. Within the ‘new general practice’, professionalism has been de-coupled from some of the paradigmatic traits of traditional rhetorical accounts (such as vocation), and has significantly reframed others. Despite policy concerns that a retreat from ‘vocational’ professionalism will lead to reductions in service quality, we argue that this is not inevitable. The ‘new general practice’ resonates with the social values of reflexive modernisation, and has the potential to enable new, less paternalistic, forms of relationships with clients, although it remains to be seen whether this potential is realised in healthcare delivery.
Keywords: professionalism, reflexive modernisation, primary care, general practitioners, workforce
© 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd. Published by Blackwell Publishing Ltd., 9600 Garsington Road, Oxford OX4 2DQ, UK and 350 Main Street, Malden, MA 02148, USA
928
Lorelei Jones and Judith Green
Introduction Since Freidson’s (1970) classic work, sociological debate about professions has inevitably been concerned with questions of ideology as well as description. In addition to attempting to define the traits that might distinguish ‘professional’ occupational groups (and the strategies by which these traits might be achieved, or threatened), sociologists have also had to address the referent ‘professionalism’ at the level of discourse. In what contexts, and with what effects, are claims to ‘be professional’ made? The two kinds of question are of course intricately connected, in that occupational claims to professional identity on the basis of possession of particular traits can only be credible in the context of normative consensus about what a professional is. Moreover, discussions about issues such as professionalising projects inevitably rely on rhetorical claims made by professional organisations. To describe oneself as ‘professional’ is to make a discursive claim about not only membership of a privileged occupational group (Southerton 2002), but also the possession of such valued attributes as trustworthiness and competence (Elston 2004). In everyday discourse, references to ‘professionalism’ are commonplace as distinguishers of preferred modes of occupational behaviour; claims to moral adequacy and markers of the limits to appropriate relationships with clients. These everyday usages of the term ‘professional’ are not trivial: they constitute part of the cultural backdrop against which current debates about the role and governance of professionals is conducted. In recent years, particularly in the United Kingdom (UK), these debates have focused on appropriate models for the governance of professional organisations (Allsop et al. 2004); the kinds of values that medical professionalism should espouse within a changing healthcare environment (BMA 1994, Rosen and Dewar 2004) and the role of professionals vis a vis the communities of clients they work with (Green 2005). The link between these policy-level debates and the individual accounts of practitioners lies in the role of work in identity formation in contemporary society. The ways in which practitioners derive meaning from, and present, their workplace roles, in relation to other possible workplace roles, is a key element in both their self-identity as ‘a professional’ and the ways in which their professional organisations represent their interests in national policy arena, which in turn feed into debates about governance, values and relations with clients. It is plausible that these individual accounts, part of the reflexive projects of individual practitioners, are increasingly significant in an era in which there is a widespread assumption of the agential possibilities for each of us to define our own working (and professional) identity. The decline in the normative dominance of work roles over identity has been widely debated as part of the reflexive modernisation thesis. This thesis frames the narratives people tell about their lives as being reflexively constructed against either a backdrop of liberation from the normative constraints of © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
General practitioners and shifting discourses of professionalism
929
traditional prescriptive categories of class, gender or occupation in Giddens’ (1991) emancipatory account, or the erosion of the traditional moral anchoring of lifetime workplace identities in Sennett’s (1998) less optimistic one. To a greater or lesser extent, as workers, we face uncertainty about the trajectory of our careers, and the possibility of constructing ‘portfolio’ working lives. Like other professionals, doctors are increasingly less likely to work as ‘traditional’ solo practitioners or in partnerships that might endure over a working life, and more likely to work in complex or novel organisations (Johnson 1995), with the expectation of numerous changes in location and role specification over a career. Their decisions about career planning have taken place in the context of considerable public scrutiny over the constitution of proper modes of professional governance in contemporary societies ever more geared towards public accountability and user involvement. Until recently, these trends have been debated largely in terms of their potential threat to essential elements of professional status, focusing on how far, for instance, external control is likely to erode professional autonomy (McKinlay and Arches 1985, Hunter 1994, Coburn 1993) or how far client input is likely to reduce medical dominance (Williams and Popay 1994). As Lupton (1997) notes, though, to ask questions about whether or not professionalism is under threat in medicine rather misses the point, as ‘doctors still see themselves, and are perceived by the general public, as “professionals”, albeit bearing different meanings and responsibilities from previous notions of professional practice’ (Lupton 1997: 493). She advocates repositioning the debate as one about ‘reprofessionalisation’, in which the complex sets of practices which constitute professional practice can be explored. This paper is a contribution to such a project, in which we explore how early career GPs construct themselves as ‘professional’ in their talk about work and, in doing so, contribute to a new constitution of the normative contours of professionalism in medicine. This group is a particularly interesting one in the light of their centrality to recent shifts in the organisation of primary care in the UK.
Background: changes in primary care in the UK In 1912 the National Health Insurance Scheme required that families register with a general practitioner and this system of patient registration has remained to this day, with 99 per cent of the population currently registered (Audit Commission 2002). This ‘personal list’ has been central to the values of GPs in the UK, with Baker and Pringle (2000: 4) suggesting that ‘the registered list means that there is a long-term relationship and responsibility between doctors and individual patients, and between practices and populations of patients’. Comprehensive, longitudinal care, organised around the personal relationship of a doctor and his or her patients, has long been considered a key attribute of primary care in the UK (see, for instance, Starfield 1994, RCGP 1969). When the National Health Service was created © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
930
Lorelei Jones and Judith Green
in 1948, GPs became ‘independent contractors’. A GP working as an independent contractor is known as a principal. Independent contractor status has remained the dominant model of practice for GPs in the UK, but other, ‘non-principal’ medical employees have also provided primary care services. Non-principals have historically fallen into three main types: locums, retainers and associates. Locums are doctors who cover for periods of absence on a short or long-term basis, for example, for sickness, holidays or maternity leave. The retainer scheme was established to enable doctors, most often women with family commitments, to ‘retain’ their knowledge and skills by working up to four sessions per week. In 2002, the retainer scheme was replaced by the Flexible Careers Scheme. Associates, now known as salaried doctors, are doctors employed by a practice on a salaried basis. The last two decades have seen substantial changes in the general practice workforce and the conditions under which they work. One of the most dramatic is perhaps the decline in dominance of independent contractors as the major providers of general practice services. In 1983, 98 per cent of GPs worked as principals. Currently, 41 per cent of GPs are classified as nonprincipals (DoH 2004). GPs are also more likely to be working part time. In 1983, there were no provisions for principals to work anything other than full time, whereas by 2003, 22 per cent were part time. Finally, the trend towards larger practices has continued, with a rise in the numbers working in or for partnerships of six or more GPs, and a corresponding decline in single-handed and small practices (DoH 2004). These changes in the primary care workforce have happened against a policy backdrop of increasingly active management of primary care, with the traditional independence of the solo practitioner replaced with tighter control and accountability (Lewis 1998, Charles-Jones et al. 2003). Taken together, these are significant changes to the organisation of primary care work in the UK, yet to date little work has been done on their implications. One exception is the analysis of Charles-Jones and colleagues (Charles-Jones et al. 2003) of the effects of the what they call the ‘transformation of general practice’, in particular the redistribution of work in primary care. They argue that there has been a ‘hybridisation’ of primary care work, in which nurses are increasingly taking on tasks once defined as medical, and which has necessitated both GPs and nurses engaging in professionalising strategies to demarcate their professional roles. Doctors have to make claims for special expertise over those areas of work that still require discretion, and thus reconfigure themselves as specialists or consultants to maintain professional dominance. One outcome of this, they suggest, is a shift away from the biographical orientation that traditionally marked off the unique contribution of the GP, towards a more biomedical orientation. We were also interested in whether there were fundamental shifts in the orientations of medical professionals, in the light of sociological theory on the role of work in the formation of identity in late modernity, and the policy debates about the likely implications of changing understandings of © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
General practitioners and shifting discourses of professionalism
931
professionalism for the health service. One study that provided some clues to radical shifts in how professionals understood their careers and identities as doctors in the UK was the BMA cohort study (Jones and Fisher 2006), a 10-year longitudinal study which followed the career paths of 544 doctors who graduated from UK medical schools in 1995. This study identified a number of trends. Although general practice is not attractive to medical graduates initially, it becomes popular in subsequent years because it is perceived as offering a superior work-life balance. Once in general practice, both male and female doctors are choosing to work reduced hours and/or in non-principal posts (Jones and Fisher 2006). The BMA cohort provided a salient sampling frame to select a group of relatively young professionals to explore in more detail the orientations of this increasingly important sector of the healthcare workforce. Data for this paper are drawn from a sample from the BMA cohort invited to take part in an in-depth interview.
Methods A purposive sampling strategy was used to select interviewees who were currently working in general practice from across England, Wales and Scotland in a range of rural and urban locations. In total, 20 GPs (14 women, 6 men) were included in the study, reflecting the gender composition of the total cohort study participants who had become GPs. These GPs all graduated from medical school in 1995, and their ages ranged from 32 to 37. Most (18) were working as non-principals at the time of interview. Interviews, lasting about an hour, were conducted by the first author (LC), mostly at the GP’s home (N = 16) and were audio-taped and transcribed. In all interviews, participants were prompted for reasons for choosing general practice, career histories, descriptions of their work, satisfactions and dissatisfactions with the job and plans for the future. Participants were encouraged to elaborate when they raised other topics. In later interviews, participants were also asked to reflect on questions arising from early analysis, including direct questions on the meaning of professionalism in general practice. Analysis of the transcripts was thematic, but using some of the principles of ‘grounded theory’ (Glaser and Strauss 1967), in that initial interview transcripts were ‘open coded’, with intense line-by-line analysis of the transcript to elucidate initial concepts for exploration and to suggest further sampling. Data analysis and collection were thus undertaken simultaneously. In this paper, we report on our analysis of the ways in which ‘professionalism’ was used as a referent, and how it relates to two particular in-vivo categories which recurred within the transcripts: ‘nice work’ and ‘the new general practice’. Ethical approval was sought and granted by the London School of Hygiene and Tropical Medicine Ethics Committee. All interviewees have been given pseudonyms in this paper. © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
932
Lorelei Jones and Judith Green
Results High job satisfaction In contrast to those from many other recent studies of GPs in the UK, the accounts of these interviewees could be characterised as expressing extremely high job satisfaction. For these young, largely non-principal GPs, work was described positively in general (‘brilliant’, ‘fantastic’ and ‘good fun’ were typical summary descriptions) and their combination of work, family and other interests was often explicitly identified as ‘ideal’. The doctors themselves talked of being ‘very happy’. To a large extent, this satisfaction was the result of having their expectations of their career choices met. These doctors had chosen general practice, often after a start in hospital medicine, because it would be flexible; it would fit in with their life. These choices had been vindicated, in that they had managed to organise their general practice work to suit their own needs. Salaried and locum work meant they could choose the number of sessions they worked each week, without onerous on-call responsibilities. Work choices were presented as agential decisions, through which most had achieved ‘the perfect balance’ between time at work, time with their family and other interests: I think this is ideal . . . I mean it was quite difficult putting it all together really and getting one job and getting the other job, and it was quite a juggling match to fit it all in, and so yes, this is what I’ve wanted to do, exactly the balance. Whether I would do two half-days in general practice or one half-day in whatever, I don’t know, I definitely want to have a day with the children, but obviously as they go to school I might be better off having two afternoons or something, because picking them up in the afternoon is going to be a nightmare. So it’s a flexible, ongoing thing I think. But yes this is what I chose and this is what I wanted to do (Dominic, salaried GP). The advantages are that it’s lifestyle at the moment, and I don’t have any responsibility and I don’t come away with any worries or concerns, I go to work, do a job and come away and I can get on with my personal life. Whereas I’m sure if I was a partner I’d be worrying about lots of things (Margaret, GP locum). These participants described what could be called classic ‘portfolio’ career aspirations, with an expectation that although they would probably stay in general practice, this would offer a range of job experiences, with the possibility of constantly adding to their skills and developing other specialisms: I’ve already done palliative care, endoscopy and emergency care, and would be classed as specialist GP in all those areas . . . and there’s other things I want to do, I’m not going to be just a GP (Andrew, salaried GP). © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
General practitioners and shifting discourses of professionalism
933
This flexibility also led to a confidence that general practice work would continue to offer a career path that could be tailored to changing family circumstances or other preferred activities, rather than acting as a constraint on ‘life’, which was explicitly constituted as those activities external to paid work: I think the other main advantage to locuming for me is the flexibility of holidays, I basically work to fund holidays, that sounds very selfish, but that’s kind of what I do and I think having had years of working in a hospital where you’re dictated to, it’s fantastic . . . the phone goes and they ring up and they say, ‘Can you work Monday?’ and you say ‘yes’, or ‘no, I don’t really like that practice I won’t go there’, or ‘I’ll just do a morning because I want the afternoon to go and see a friend’, or take a long weekend or whatever, so its just wonderful for me to be in control of what I do and not be dictated to anymore (Rebecca, GP locum). I wanted to be around when my children were growing up, I didn’t want to work until seven every evening when they were in bed, so I thought I have to make the decision what makes me happy, and it makes me happy to do my work and to have my social life and have my family separate. And obviously the work is still intellectually challenging . . . Other people think differently about their vocation . . . (Jamie, salaried GP). Market demand for locum and salaried doctors meant that the doctors in the study were in a position to dictate the kind of general practice work they undertook. It meant they could elect to do work that they particularly enjoyed and avoid work that did not interest them. Rebecca’s comment, above, that she would turn down sessions in an undesirable practice, is an indication of a key theme in these accounts: that of the search for ‘nice work’, and the planning that went into ensuring that work was not only in its place within a balance of activities, but was also interesting and enjoyable in its own right. ‘Nice work’ ‘Nice work’ was an emic category, employed by some respondents to describe either their current situations, or the ones they sought. It also usefully summarises the attributes of favoured work for all interviewees in the sample, as there was a broad consensus on what constituted preferred employment characteristics. First, ‘nice work’ enabled you to develop relationships with the patients. Regular locum sessions, such as a maternity locum in which another GP’s list would be covered for six months, were particularly sought for this reason. At the time of the interviews many practices had moved from a system of individual doctor ‘lists’ to a system of ‘open access’ where patients cannot book an appointment in advance and, instead, must ring on the morning of the day they wish to see a doctor. Nonetheless, the doctors interviewed who managed regular sessions were still able to © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
934
Lorelei Jones and Judith Green
develop ‘a following’ of patients who knew what days they worked and would ask for them by name. Second, ‘nice work’ was work done in practices which were friendly, well run and innovative and, for some participants, ideally in rural areas although others were happily working in inner city practices: The one practice, which was a lovely, lovely practice I worked in [county name], we all kind of just seemed to finish at about the same time and there was a room set aside with a kitchen off it and we’d go and make a coffee and you’d sit down and do the repeat prescriptions and all just be sitting there, which was really nice (Philippa, GP Flexible Careers Scheme). It [current practice] is just a nice environment to work in, it’s friendly . . . you’re in and out, chatting to other people (Sophie, GP locum). Third, ‘nice work’ was unhurried with enough time to give to patients and to do other things during the day. Finally, ‘nice work’ was intrinsically interesting work. These participants were not trading less responsibility for more routine, but were consciously seeking work that provided stimulation. Rather than being constrained by the routine nature of much of the primary care workload, which has been commented on in other studies (see, for instance, Horobin and McIntosh 1983), the majority of non-principals in this study maintained intellectual challenges in their working lives by developing a specialist interest. This might involve running a clinic in the surgery or working as a clinical assistant in a hospital department or other setting in addition to general practice sessions. This was facilitated by the flexible nature of their general practice commitments. The special interests being pursued in the interview sample included neurology, accident and emergency, endoscopy, palliative care, sports medicine, family planning, rheumatology, dermatology, occupational health and medico-legal work. The communities within which these GPs were working varied, including rural settings, affluent suburbs, inner city practices, deprived towns and specialist drug and alcohol services. Although there was broad agreement about the preferred type of practice, preferences for particular types of patient varied, with most interviewees expressing satisfaction so long as their case-loads allowed variety and the use of expertise. Creating the ‘polyclinic’ There is a potential moral threat in claiming the self-interested pursuit of ‘nice work’, in that this positions what ‘others’ do as stressful, routine or dirty work. The non-principals in this study were, however, careful to deflect this threat by presenting their choices as not adding to the burden of unrewarding or burdensome work done by the principals in their practices. © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
General practitioners and shifting discourses of professionalism
935
Rather, in these accounts, demanding flexibility and contributing to specialisation in primary care enabled all GPs to pursue the dream of a balanced life and nice work and avoid the constraints of overwhelming practice demands: . . . there are very few full-time partners who are fixed on the practice and then there are lots of salaried doctors that either have families or do other things (Philippa, GP Flexible Careers Scheme). Rather than merely filling the gaps in primary care provision, these interviewees saw themselves as contributing to the emergence of what we call a ‘polyclinic’-type provision, in which all providers specialise to some extent. The accounts of work and practice organisation in these interviews construct an ideal, at least, of a polyclinic facility: multi-professional practices where the doctors, nurses and other healthcare practitioners have special interests and in which patients benefited from a broad range of in-house expertise. In such practices, all staff benefit from reduced hours, with salaried doctors and locums used by the practice as an extra pair of hands to enable this to happen. There were some empirical descriptions of this scenario, where participants referred to a senior partner who had withdrawn from clinical practice altogether to work for the primary care trust (PCT) or to manage the practice. Other respondents reported colleagues involved in research, teaching, medical publishing and broadcasting: Well, here at this practice where I’m working in, they’re sort of quite keen that people pursue other interests other than pure general practice. I work eight sessions a week, which means I get one day off a week and what my colleagues have done, they’ve taken a day or a session out to pursue interests, one partner does diabetes and another is into cardiology, another one’s into rheumatology . . . (Deepak, salaried GP). This echoes the findings of Charles-Jones et al. (2003) on the reconfiguring of the GP as a ‘specialist’ or a consultant in primary care. Rose, a part-time partner, was the only GP to report a system of personal lists, with little specialisation within her practice, and she commented that ‘that’s perceived as a bit old-fashioned now, I think’. Most respondents discussed specialisation enthusiastically. The polyclinic included specialised nursing clinics in areas such as chronic disease management, treatment room provision and well women clinics. Reception staff, too, became an essential element, using a high degree of discretion to triage patients to the most appropriate provider. For some participants, there was some tension between this trend for specialisation within a practice and the desire to remain a generalist: I think, the whole point of general practice is, or the whole attraction is the variety . . . I think this has happened with the triage nursing, or the © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
936
Lorelei Jones and Judith Green
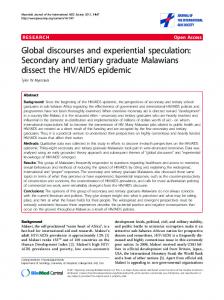
contraceptive nursing, suddenly all the contraception pills are going to the nurse and actually it’s quite nice to see a young person occasionally . . . (Rebecca, GP locum). As Rebecca’s comment suggests, though, the imperative to retain some element of generalisation lies in the intrinsic interest of ‘variety’ rather than any fundamental commitment to the ideal of comprehensive care. Comprehensiveness may be a traditional value of primary care, but it was not a salient one for the GPs in this study. Indeed, comprehensiveness was, for many, associated with the dysfunctions of the traditional primary care model, rather than its advantages, in that GPs might well have been practising in areas outside their expertise. As one example, Charlotte recalled older GPs with whom she had worked, who, she felt, were not up to date on contraceptive advice. She went on to comment: . . . but I don’t know how you do keep up with everything . . . I don’t think patients mind being referred on [to another GP], and I think they get a better quality of care . . . from my point of view it works well, because I’ve never felt 100 per cent confident with that aspect of general practice so it’s nice for me to have a colleague who is good at it (Charlotte, GP locum). So the polyclinic model was presented as not just ensuring an interesting workload for participants, but also a better service for patients. The ‘new general practice’ In framing the kinds of work they liked, and the advantages this had for patients, many participants explicitly contrasted their orientations with what they called the ‘old fashioned GP’ or ‘old-school general practice’. The particular features of favoured general practice work we have discussed so far – its balance with the rest of life, the pursuit of nice work and the maximisation of exposure to interesting work, appropriately referred within the polyclinic – constituted this ‘new’ general practice. This was visible in the contrasts many participants made between their approach and that of an older generation of GPs who epitomised an out-dated model of professionalism. The core values of the ‘new general practice’, summarised in Table 1 overleaf, were fairly stable across the interviews. One element was that, for new GPs, financial remuneration was reported as a less important motivator than quality of life: It’s a very family-oriented practice here, I think the idea is not to earn as much money as you can, it’s to have a good quality of life and provide a good service (Andrew, salaried GP). I think its basically very patient-centred. The guy who’s the senior partner, he’s always ploughed any profits back into the practice, he doesn’t draw a © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
General practitioners and shifting discourses of professionalism
937
Table 1 Contrasts made in interviews between professional characteristics of ‘traditional’ and ‘new’ general practice ‘Traditional’ general practice
‘The new general practice’
Orientation to work
Medicine is a vocation and ‘master status’
Medicine is a job and part of a work-life balance
Core moral values
Commitment Status in community
Quality of work Quality of life
Career structure
Flat career
Portfolio career
Professional relationships
Hierarchical Independent solo practitioner
Democratic Part of professional network
Relationships to clients
Comprehensive, continuous responsibility Paternalistic
Co-ordinator of network of professionals Patient-centred
Workload
Routine Time pressured
Stimulating Controlled
huge salary for himself. I think all the doctors that work there, they’re not sort of money grabbing types, they just want to get job satisfaction and feel like they’re doing a good job and providing a good service really (Helen, GP locum). The choice, however, was clearly not just one of trading off income against ‘nice work’. There was also a cluster of features related to nice work within the polyclinic that typified, for them, the ‘new general practice’. One was a democratic workplace culture, in which equality across the primary care team was valued. Preferred practices were those in which work was shared out fairly between doctors, with an absence of indicators of hierarchy such as titles or separate coffee rooms for different staff. Collaborative workplaces were particularly prized: The reason I like my practice so much is this really fluid sort of communication between doctors, nurses, receptionists, everything’s sort of on a level, everyone’s on first name terms and there aren’t any doors that you can’t knock on (Helen, GP locum). There was no hierarchy . . . we were all equal, they were as equal and professional as we were, and I much prefer that. I don’t like working in an environment where there is the sort of, the top older GP, the newer GPs and then the nurses and then the receptionists . . . (Margaret, GP locum). This democratic orientation also flavoured accounts of relationships with patients, which stressed a patient-centred approach and an orientation to © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
938
Lorelei Jones and Judith Green
shared decision-making. The GPs in this study had been trained under the Vocational Training Scheme, which focuses on communication skills. Several drew on their experience of this training to contrast their ‘patient-centred’ approach to the doctor-patient relationship with the paternalism of their predecessors. Felicity, for instance, refers to her GP trainer, who was nearing retirement when she was a trainee: He was very much of the old school, very formal with his patients, not very good at keeping up to date . . . he wasn’t so good at the chit-chat, so he was quite authoritarian I suppose (Felicity, salaried GP). I think as younger GPs we’ve been very fortunate, in that we’ve had a lot of training in communication skills and I think we’ve been taught to share things with the patient a lot more . . . I think older GPs can be more prescriptive in their style, I think the younger GPs tend to try and share information with the patient and get them involved in decision making . . . (Helen, GP locum). In the extract below, Penny perhaps sums up the differences between how the GPs in this study characterised their work in relation to their images of traditional general practice work in explicitly comparing elements of the ‘old-fashioned general practice’ with what she herself calls ‘the new general practice’: I think very much old-fashioned general practice was your life, you were on call 24-hours a day, your patients knew where you lived, they knocked on your door, they hailed you in the street, they followed you down the road and your life was not your own until you retired, and that has positives and negatives, in that the positives are that you were part of the community, you were part of almost their family if you like, and if you stay in the same area, which most people did, then you would build up relationships that would perhaps mean that if things did go slightly awry you would probably be less likely to get a complaint, because they know that you looked after mum when she died and so from that point of view it’s a slightly protective element, whereas the new general practice I feel very much is, people are doing a job, it’s a job that has a vocational element, but at the end of the day it’s not a life really any more, and I think most people don’t want it to be in actual fact. And I also think that the change has been to a certain extent forced upon us by the demands of the patients, there is no way that the old-fashioned general practitioner could do the equivalent of let’s say a [rural area] doctor’s on-call shift and be rung at 11 o’clock, because someone’s got no Paracetamol, well no sorry, and that didn’t happen, because people were more self reliant perhaps and self sufficient, and they had families around (Penny, GP locum). © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
General practitioners and shifting discourses of professionalism
939
Here Penny, perhaps not surprisingly, undercuts her own account of the advantages of old-fashioned general practice. First, she suggests that the benefits of continuity are primarily in the interests of professionals, given that this might reduce the likelihood of patient complaints and, second, she claims that contemporary patient behaviour no longer enables this kind of commitment. Rhetorically, the ‘old’ way of doing things is constructed as impossible to realise, even if it were desirable: it is simply inappropriate to the modern list of individualised patients, rather than the families and communities catered for by the ‘old-fashioned’ GP. More specifically, though, continuity, like comprehensiveness, is constructed as not only inappropriate, but emphatically ‘unprofessional’ in the context of modern healthcare practice. It is presented as a refuge of traditional GPs with inadequate technical and communication skills. Thus, the decline in continuity, like the decline in comprehensiveness, is constructed as being inherently beneficial for patient care, rather than a loss. In Ahmad’s account of the differences between traditional and new general practice, it is possible to see the discursive work entailed in presenting the new as more professional, despite the superficial loss of the enduring patient-doctor relationship: Older GPs knew their patients and their families and their grandfather . . . now, because the patient-doctor relationship isn’t as good, doctors need to perform better to keep that relationship . . . most patients I see have never met me before, they’re making their own mind up about whether I’m good or not, so doctors are judged more (Ahmad, GP locum). Rejecting vocation Penny’s comment, above, that ‘people are doing a job . . . but at the end of the day it’s not a life any more’ perhaps sums up what these GPs saw as the key difference between them and ‘old-fashioned’ GPs. The doctors interviewed were uncompromising in their dedication to quality of life. They did not feel that medicine ‘was their life’; life itself happened outside the realm of work. Although, as Penny says, medicine might have a ‘vocational element’, it was not in and of itself a vocation, but rather a job performed during demarcated ‘work’ time. Of the 20 GPs interviewed, only one (Elaine) did not make this distinction. Elaine was the only participant to provide the kind of description of a GP that could be seen as unambiguously ‘vocational’: Interviewer: Elaine:
And what about being professional, what does that mean to you? It means never being off duty, always I suppose being a doctor . . . I suppose [medicine is] a respected profession, so respect from the community, that’s about it, yes.
Elaine was also the only participant in this study to claim that there were no differences between older and younger doctors. Even Elaine, though, had © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
940
Lorelei Jones and Judith Green
developed what might be called a portfolio career, involving sessions in sports medicine, and one day a week in a minor injuries unit as well as her salaried GP sessions. The disavowal of vocation as the defining feature of professionalism did not imply rejection of professionalism or pride in clinical competence. Indeed, there was a strong focus on quality in the interview accounts. However, the quality of the services they provided was not reported as deriving from a commitment to continuity or comprehensiveness, or the kind of vocational definition Elaine (above) uses, but from technical competence, continuous learning and communications skills. In answer to direct questions in the later interviews about what a good doctor was, almost all mentioned some aspect of technical competence as core, and many mentioned the obligation to update skills through continuous learning: If someone takes [on] appraisal properly, they become an excellent doctor because they learn ways to find out how to sort things . . . and that promotes learning (Ahmad, GP locum). Someone who listens to patients, who respects the patient, obviously who is clinically competent . . . looks for their own areas of weakness and tries to improve them (Helen, GP locum). Being a professional was discussed in similar terms by most: Interviewer: Rose:
What do you think it means to be a professional? I think it means to have a sense of responsibility for your patients, to keep yourself up to date, in terms of your competence and your knowledge (Rose, part-time partner).
Many also made a direct connection between enjoying work and professionalism. First, the obligation not to ‘burn out’ was essential for maintaining the enthusiasm and energy required for developing good patient-doctor relationships. Second, having work you enjoyed was essential for ensuring that clinical development was not compromised by a declining interest in medicine itself, and a subsequent failure to keep skills and knowledge updated: I think it’s one of those things that if you’re kind of fresh and you’re not frazzled and you’ve got time and you’ve got energy to give to the patients when you’re there, hopefully you can sort them out a bit better and listen to them properly, and I think that’s a trade-off between that and kind of being there all the time, that maybe you’re being a bit short with them and you’ve not got quite so much energy to throw at the problem (Helen, GP locum). © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
General practitioners and shifting discourses of professionalism
941
I think one of the most important things is that a doctor cares and is conscientious . . . in order to care and be conscientious [you have to] be in a situation where you enjoy your work . . . I like to read something in the BMJ, and then the next day I can actually apply what I’ve read . . . (Simon, recent partner). Simon went on to compare himself to older GPs who had no interest in staying up to date, who he described as having ‘lost what being a doctor is all about’. Thus, the rejection of vocational professionalism, and its associated burdens, was constructed as essential to the adoption of appropriate modern professional orientations and the improvements in standards that followed. Direct benefits to patients were also claimed to accrue through the specialist skills of the polyclinic doctor, and the professional networks they developed: I think it increases my experience and if I don’t know what to do with them I can, I’ve got easy access to the dermatology department, so I can ask them, take a picture with my digital camera and then show it to somebody. So hopefully it reduces the need for referral or delays the referral for a bit longer if there’s other things that we can try before referring them. So I suppose in that way it’s perhaps providing a better service for the patients as well (Emily, salaried GP). The rejection of vocationalism – the idea that being a GP was a calling, and a job that defined the rest of your life – was therefore not a rejection of a professional role, but rather a reframing of that professionalism. Central to the ‘new’ professionalism were three traits: positioning yourself as one of a network of professional colleagues; an obligation to be clinically competent and constantly update knowledge, and a commitment to patient-centred and collaborative practice.
Discussion The doctors who participated in this study had successfully found themselves ‘nice work’, which was preferably undertaken in friendly, well-run, innovative practices which allowed then considerable control over hours of work, the combination of work and non-work interests, the combination of general practice and other professional interests and the kind of general practice work undertaken. These GPs may not be typical of the broader workforce, and it is not known whether their orientations reflect those of their cohort, or those of early-career GPs more generally. They are, though, an important group given that they are among the early graduates of the remodelled Vocational Training Scheme (DOH 2002). In a labour market characterised by problems in GP recruitment, and policy initiatives to © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
942
Lorelei Jones and Judith Green
attract more GPs by extending flexible career options, these GPs had secured favourable contracts and, perhaps unsurprisingly, they reported extremely high job satisfaction. In part, this is perhaps also an inevitable result of the agential narratives elicited in the interviews: these GPs stressed their own choices in making their careers, and the explicit ways in which they maximised their own goals in seeking work in an environment in which their skills are in relatively short supply. Having been prompted for a story focusing on active choices, it would, then, be difficult to express dissatisfaction. However, their reported satisfaction marks a notable departure from much research on primary care over the last two decades, which has been characterised by reports of poor morale (Chambers and Campbell 1996, Caplan 1994, Horobin and McIntosh 1983, Sibbald et al. 2003). Poor morale has been attributed to both the routine nature of much general practice work, and to stress deriving from time pressures, reorganisations and the associated administrative burden (see, for instance, Leese and Bosanquet 1996, Hannay et al. 1992). Horobin and McIntosh’s study, which was based on interviews from the late 1970s, typifies perhaps one aspect of dissatisfaction, the burdensome proportion of routine. One GP was quoted as saying: our skills are absolutely wasted . . . frustration and boredom set in. There are those days when you go home and think, ‘Have I got to do this for another 20 years?’ (Horobin and McIntosh 1983: 32). The GPs in this study had managed to avoid many of these potential causes of dissatisfaction. Fewer hours and discretion over the work they did meant that they were less likely to be burdened by the routine or the time pressure of a (particularly urban) practice; a combination of different types of clinical work meant a more interesting case-mix; and a retreat (for most) from the responsibilities of running a practice meant they were less concerned with the effects of restructuring or the implementation of new primary care policy. A legitimate policy concern is that of equity: who will take on the responsibilities of stressful inner-city practices if new entrants to the profession are ruthlessly seeking ‘nice work’, potentially exacerbating the inverse care law? Policies extending flexibility in primary care contracts aim to address equity concerns (DOH 2000) but the effects have been, so far, equivocal (Williams et al. 2001, CMO 2005, Scott et al. 2001). It is encouraging perhaps that many of our interviewees assumed that they would take on more responsibilities as their careers progressed, and indeed two were already partners. Although they also expected that their futures would still entail ‘nice work’, in well-run practices, with team working and colleagues who specialised and were careful to preserve a work life balance, this did not necessarily imply choosing practices in affluent areas: some were working in inner city communities, or in schemes providing services for hard-to-reach clients, such as those with alcohol or drug use problems. © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
General practitioners and shifting discourses of professionalism
943
A few participants, such as Rebecca, quoted above, attributed their decisions to instrumental motivations on wanting to work simply to fund holidays. Significantly, though, most were careful to present themselves not as individuals who wished merely to avoid the well-known stresses of general practice through ‘dropping out’ or making purely self-serving decisions to prioritise their own quality of life over the legitimate demands of a professional life. Rather, their decisions were presented as constituting a ‘new’ professionalism, the contours of which were remarkably stable across the interviews. The pursuit of ‘nice work’ and a good work-life balance was not presented as a retreat from professionalism but, in Lupton’s (1997) phrase, a ‘reprofessionalisation’. In the accounts of these GPs, we can begin to outline the structures of this new professionalism, which entails a rejection of some core values of traditional professionalism and a re-framing of others. The most significant change is perhaps the de-coupling of vocationalism from professionalism. A key attribute in many trait approaches to the professions has been the idea that professionalism embodied a ‘calling’ or ‘vocation’, at least as an ideological claim. Shuval and Bernstein’s (1996) summary of the attributes of vocationalism is pertinent: The concept refers to an all encompassing devotion to work characterised by total personal involvement that focuses on the intrinsic rewards of work, transcends the monetary reward and spills over to invade the professional’s leisure time leaving little space for extra-occupational concerns (1996: 966). Like others, they suggest that, ‘although this notion has served as a basis for a functional mythology, it seems unlikely that in practice it ever characterised more than a small proportion of professionals’ (1996: 966). Whether or not a vocational orientation to work was ever empirically characteristic of medical professionals, what is striking is perhaps the decreasing rhetorical force it has as a normative ideal. In 1994 the BMA surveyed a sample of their membership on the subject of their core values. In one question doctors were asked to indicate which of four statements best accorded with their view of medicine, ranging from ‘Medicine is a vocation, and only those who are prepared to make it their primary commitment should enter the profession’ through to ‘Medicine is a job like any other and doctors have a right to work normal hours and forget about work when they get home’. Whereas 18 per cent of doctors over 55 chose the first statement, fewer than one per cent of doctors under 30 did (HPERU 1995). However, the amount of rhetorical work our participants had to do in claiming a professional orientation whilst disavowing vocation, is perhaps evidence that vocationalism has not completely lost its normative force. Its rejection still has to be discursively reframed as a positive embrace of other values. Echoing debates about the declining role of work in the formation of identity, Shuval and Bernstein © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
944
Lorelei Jones and Judith Green
(1996) suggested that vocation in medicine had been replaced by a plurality of other, non-work-related, commitments that were equally important as sources of identity. The findings from the present study could be read simply as reflecting this trend, with doctors expressing an uncompromising dedication to quality of life, and a retreat from the idea of work as central to identity (‘medicine is not a life anymore’). Indeed, in many ways their pursuit of ‘nice work’ bears striking similarities to Giddens’s (1991) description of ‘pure relationships’. In late modernity, argues Giddens, traditional roles and identities no longer underpin life decisions, which are instead taken reflexively, with individuals having to choose between options. The ‘pure relationship’, freed from the normative expectations of traditional identities, is valued for its own sake, and maintained so long as it promises to satisfy each partners’ expectations. It is also reflexively organised, with each partner consciously reflecting on the status of the relationship and making nuanced judgments about when and how much to commit because, once committed, the obligations of trust and intimacy entail a certain amount of work to sustain. The GPs in this study could be seen as following an imperative to seek ‘pure jobs’, in that there was no expectation that financial or traditional constraints would keep them in a practice for a lifetime, and each job would be maintained so long as it had benefits for each side. They also sought a kind of intimacy and trust within the workplace, with favoured practices being those which were democratically organised, in which colleagues collaborate as a functioning team. We suggest, however, that there is more in these accounts than simply an empirical example of reflexive modernisation or a replacement of vocation by ‘pure jobs’. We also found a carefulness on the part of these GPs to present their work as ‘professional’ in that it was practised in a way which maximised benefits to patients. Indeed, given the changing health-care environment, their orientations to work were presented as better able to meet the needs of patients than ‘traditional’ models of practice. Resistance to a traditional vocational model was constructed as healthy and morally worthy, in that was in the ultimate interests of clients and other colleagues as well as the GPs themselves. Not only have the GPs in our study de-coupled the construct of vocation from the discourse of professionalism, they also rhetorically clustered ‘vocation’ with an orientation to work that becomes constructed as essentially dysfunctional within a modern healthcare context. Vocation was explicitly associated with ‘old-fashioned’ attitudes, which were framed as not only anachronistic, but also potentially damaging in both the paternalism they engendered in relationships with clients and the unhealthy self-sacrifice demanded by continuous access to patients. Old-fashioned vocation entailed a dominance over other areas of life that was inherently problematic, rather than morally worthy. There is a nice contrast here with the views reported of single-handed GPs in London in the 1990s (Green 1996): solo practitioners who had often rejected the ‘modernity’ of the large practice. The single-handed © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
General practitioners and shifting discourses of professionalism
945
GPs self-consciously presented themselves as ‘old fashioned’, and their accounts of motivations, commitment and job satisfaction were rooted in a particular relationship with the local community: one of ongoing immersion, in which the responsibility to provide 24-hour, continuing care was spoken of as a source of pride rather than a burden. For the single-handed GPs, the bedrock of professionalism was the relationship to individual patients over time, often over generations, and to a local community, to which the GP felt he or she belonged. They perhaps embodied vocational professionalism, with its acceptance of the centrality of the work role to social identity. The non-principals in the present study also valued relationships with patients but, for them, these were enhanced not through intimate knowledge derived from comprehensive and continuous care, but through a democratic shared approach to decision-making, willingness to refer within the polyclinic and an obligation to remain enthused by their work. There is, then, evidence here of a significant shift in the meaning of professionalism in primary care in the UK. The majority of GPs in this study were working as non-principals, representing an increasingly significant part of the primary care workforce. For them, professionalism was based primarily on quality, in terms of commitment to professional standards of work, keeping abreast of the latest evidence in their chosen specialties and developing good relationships with colleagues. In short, the primary orientation of the new professional was not to the local community, but to a professional community, which regulated (through professional standards, continuing education and the collaboration of clinical colleagues) what counted as ‘good’ general practice.
Policy implications: is the new professionalism a concern for primary care provision? There has been some concern over the potential implications of this retreat from vocational professionalism towards a more constrained search for the ‘pure job’. Allen (1997), for instance, has suggested that the professional values of young doctors will have implications for continuity of care and service development, and the workforce implications of increasing numbers of GP entrants intending to work part time has been noted (Bowler and Jackson 2002). Richard Cooper, of the Health Policy Institute of Wisconsin, has perhaps been most blunt in his summary of the likely implications: ‘Doctors who focus on a good lifestyle are bad news for patients. An 80 hour week means you are always available’ (Dosani 2003). The pursuit of ‘life balance’ has been, in policy discourse, a problem for providing healthcare. We argue that this pessimistic reading is not necessarily justified, because the claims made by the GPs in this study, even if read as ideological rather than empirical statements about orientations to practice, do suggest a more appropriate professionalism for contemporary society. It may be that © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
946
Lorelei Jones and Judith Green
concern is rooted in a nostalgia about ‘old-fashioned’ general practice that does not really reflect either the reality of vocational professionalism, or the supposed benefits to patient care. Continuity, for instance, has been a central plank of general practice in the UK, with various claims made for its worth: In primary care a ‘personal doctor’ with accumulated knowledge of the patients’ history, values, hopes and fears will provide better care than a similarly qualified doctor who lacks such knowledge; and that the benefits of such continuity will include not only greater satisfaction for the patient but also more efficient consultations, better preventative care and lower costs (Gray et al. 2003: 160). Gray and colleagues (2003), however, in a systematic review of the literature on the effects of continuity of care on patient care, found the results to be equivocal. Prioritising continuity perhaps exaggerates the significance of the GP to individuals’ lives, especially for those young adults who consult infrequently. At times of ill health or death there are a number of people involved – family, friends, the priest or other spiritual leader – all of whom are likely to be more important than the GP to the patient. Multiple health professionals are involved in the process of managing health, yet it is only the GP from whom 24-hour responsibility is deemed essential. Continuity of care is a normative ideology, which plays a role in the governance of proper patient conduct. Within a dominant professional perspective on the doctor-patient relationship that stresses the role of the GP as ever (potentially) present, and the only gateway to other health services, the opportunity for patients to consider alternative perspectives on how they may want to manage their health is limited. Despite claims of its benefits to the patient, it serves particular interests of the doctor, in consolidating a paternalistic clientprovider relationship model that is based on superiority, rather than mutual respect. Taking pride in 24-hour responsibility for patients, and making claims for this as altruistic professionalism, implies perhaps a patronising relationship with clients, rather than the kind of mutually respectful relationships stressed by the ‘new’ GPs. In his discussion of the effects of introducing competition in the public services, Le Grand (2003) draws on the moral contrast of ‘knightly’ and ‘knavish’ behaviour to point to the disincentives to respect inherent in the paternalism of ‘old-fashioned’ professionalism: For although acts of altruism require compassionate interest in the welfare of the beneficiary, this does not imply respect. Indeed, rather the reverse, the altruistic may feel he or she is superior to the beneficiary. Feelings of superiority are hard to reconcile with mutuality of respect. Some knights need to deal with pawns if their knightly impulses are to be properly satisfied (Le Grand 2003: 27). © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
General practitioners and shifting discourses of professionalism
947
The new democracy may well be as functional a mythology as vocation, but it at least suggests the possibility of more mutually respectful relationships. As yet, only speculation about the effects on patient relationship is possible. Charles-Jones and colleagues (Charles-Jones et al. 2003) suggest that the transformation of general practice has a number of implications for patient relationships, in particular the focus on ‘sorting’ patients into categories based on the biomedical rather than psycho-social needs. Increasing specialisation within the clinic, the focus on measurable throughputs and evidencebased treatment, they claim, risk the erosion of the ethical orientation towards individual biographical patients and its replacement by a ‘more efficient, but less personal’ style (Charles-Jones et al. 2003: 89). The GPs in our study, however, still valued personal and continuing relationships with patients, at least in terms of an ideological commitment, but had perhaps rejected the rather paternalistic extension of the clinical gaze into the ‘whole’ patient, 24 hours a day, over a lifetime. It remains to be seen whether the claims of our GPs are merely functional mythology, or are realised in different types of relationships with clients, but there seem no a priori grounds for pessimism. In addition to debate over the implications for patient relationships, there has been a policy concern that the specialty is both failing to recruit sufficient numbers to meet the needs of the service (Lambert et al. 1996), and that the labour supply in general practice will be increasingly affected by the decision of doctors to work part time, often posed as the ‘problem’ of the feminisation of the workforce (Bowler and Jackson 2002, Dosani 2003, MWSAC 1997). One representative of the BMA general practitioners committee went as far as arguing in favour of biasing entry to medical school toward males because ‘You do not get 35–40 years’ service from the females’ (Moore 2002). The irony was not lost on correspondents to the British Medical Journal, one of whom noted that ‘others who may take career breaks are those who are interested in medical politics’ (Walker 2002). We also suggest that feminisation may not be a particularly helpful way to frame this shift. First, the present study has shown that both men and women want to work reduced hours for a variety of reasons. While having more time to spend with small children was a reason given by both men and women, the majority of doctors interviewed for this study did not have children but were nonetheless seeking a better work-life balance. Equally important was a desire to build a satisfying and varied career by combining general practice with other professional interests. Thus, reflexive life planning, rather than ‘feminisation’, may be a more illuminative way of framing the drivers towards part-time work. Rather than implicitly assuming that the rising number of women in the primary care workforce is a problem for policy, this will re-orientate workforce research towards asking how far emerging forms of primary care organisation resonate with the expectations of professional-client relationships in contemporary society. © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
948
Lorelei Jones and Judith Green
Conclusions The main reported motivation for the early career GPs in this study was quality of life, but they also presented themselves as responsible professionals. We have characterised their orientation to general practice as typifying a ‘new professionalism’, a discourse primarily orientated towards the search for ‘nice work’ and ‘pure’ jobs, but in the context of reframing what the referent ‘professionalism’ might mean for medicine. Vocation is no longer a normative trait of positive professional identity, and has been devalued as characterising old-fashioned, over-burdened and dysfunctional approaches to primary care. Instead, new professionalism is demonstrated through a commitment to constantly improve technical quality, as judged by professional peers, rather than with reference to relationships with a community of clients. This paper rejects the argument that this new professional ethic will necessarily impact negatively on patient care. First, the high morale of these ‘new’ GPs will potentially improve the quality of patient care. Second, the more democratic orientation towards both colleagues and patients engenders at least the possibility of new, and more respectful, relationships between professionals and patients. Address for correspondence: Judith Green, Health Services Research Unit, London School of Hygiene and Tropical Medicine, Keppel Street, London WCIE 7HT e-mail:
[email protected].
Acknowledgements This study was funded by BMA, where Lorelei Jones was employed at the time of the fieldwork. We are grateful to Helena Morris for administrative support, and to two anonymous SHI referees for very helpful comments on this paper. Thanks in particular to the GPs who participated, for their generosity with their time.
References Allen, I. (1997) Committed but Critical. London: British Medical Association. Allsop, J., Jones, K., Meerabeau, L., Mulcahy, L. and Price, D. (2004) Regulation of the Health Professions: a Scoping Exercise Carried out on Behalf of CRHP. Leicester: DeMontfort University. Audit Commission (2002) A Focus on General Practice in England. London: Audit Commission. Baker, M. and Pringle, M. (2000) Is there a Future for Independent Contractor Status in UK General Practice? London: Royal College of General Practitioners. Bowler, I. and Jackson, N. (2002) Experiences and career intentions of general practice registrars in Thames Deaneries, British Medical Journal, 324, 464–5. © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
General practitioners and shifting discourses of professionalism
949
British Medical Association (BMA) (1994) Core Values for the Medical Profession in the 21st Century: Survey Report. London: BMA. Caplan, R. (1994) Stress, anxiety, and depression in hospital consultants, general practitioners, and senior health service managers, British Medical Journal, 309, 1261–3. Chambers, R. and Campbell, I. (1996) Anxiety and depression in general practitioners: associations with type of practice, fundholding, gender and other personal characteristics, Family Practice, 13, 170 –3. Charles-Jones, H., Latimer, J. and May, C. (2003) Transforming general practice: the redistribution of medical work in primary care, Sociology of Health and Illness, 25, 71–92. CMO (2005) Report on Research into Recruitment and Retention of GPs in Wales. Office of the CMO. Coburn, D. (1993) State authority, medical dominance, and trends in the regulation of the health professions: the Ontario case, Social Science and Medicine, 37, 129–38. Department of Health (DOH) (2000) The NHS Plan: a Plan for Investment, a Plan for Reform Cm 4818-I. London: Stationery Office. Department of Health (DOH) (2002) The GP Registrar Scheme: Vocational Training for General Medical Practice. London: DOH. Department of Health (DOH) (2004) Statistics for General Medical Practitioners for England: 1993–2003. Bulletin 2004/03. Dosani, S. (2003) Implications of the gender revolution in medicine, British Medical Journal Career Focus, 326, 159. Elston, M.A. (2004) Professions and professionalization. In Gabe, J., Bury, M. and Elston, M.A. (eds) Key Concepts in Medical Sociology. London: Sage. Freidson, E. (1970) Profession of Medicine. A Study of the Sociology of Applied Knowledge. New York: Harper and Row. Giddens, A. (1991) Modernity and Self Identity: Self and Society in the Late Modern Age. Cambridge: Polity Press. Glaser, B. and Strauss, A. (1967) The Discovery of Grounded Theory. Chicago: Aldine. Gray, D., Evans, P., Sweeny, K., Lings, P., Seamark, D., Seamark, C., Dixon, M. and Bradley, N. (2003) Towards a theory of continuity of care, Journal of the Royal Society of Medicine, 96, 160 – 6. Green, J. (1996) Time and space revisited: the creation of community in singlehanded British general practice, Health and Place, 2, 85–94. Green, J. (2005) Professions and community, New Zealand Sociology, 20, 122–41. Hannay, D., Usherwood, T. and Platts, M. (1992) Workload of general practitioners before and after the new contract, British Medical Journal, 304, 615–18. Health Policy and Economic Research Unit (HPERU) (1995) Core Values for the Medical Profession in the 21st Century. Survey Report. London: British Medical Association. Horobin, G. and McIntosh, J. (1983) Time, risk and routine in general practice, Sociology of Health and Illness, 5, 313–31. Hunter, D. (1994) From tribalism to corporatism: the managerial challenge to medical dominance. In Gabe, J., Kelleher, D. and Williams, G. (eds) Challenging Medicine. London: Routledge. Johnson, T. (1995) Governmentality and the institutionalization of expertise. In Johnson, T., Larkin, G. and Saks, M. (eds) Health Professions and the State in Europe. London: Routledge. © 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd
950
Lorelei Jones and Judith Green
Jones, L. and Fisher, T. (2006) Workforce trends in general practice: results from a longitudinal study of doctors’ careers, British Journal of General Practice, 56, 134– 6. Lambert, T., Goldacre, M., Edwards, C. and Parkhouse, J. (1996) Career preferences of doctors who graduated in the United Kingdom, British Medical Journal, 313, 19–24. Leese, B. and Bosanquet, N. (1996) Changes in general practice organisation: survey of general practitioners’ views on the 1990 contract and fundholding, British Journal of General Practice, 46, 95–9. Le Grand, J. (2003) Competition in public services has the moral virtue of encouraging respect for their users, New Statesman, 13 October, 27–29. Lewis, J. (1998) The medical profession and the state: GPs and the GP contract in the 1960s and the 1990s, Social Policy and Administration, 32, 132–50. Lupton, D. (1997) Doctors on the medical profession, Sociology of Health and Illness, 19, 480–97. McKinley, J. and Arches, J. (1985) Towards the proletarianization of physicians, International Journal of Health Services, 15, 161–95. Moore, W. (2002) BMA negotiator calls for more male medical students, British Medical Journal, 324, 754. Medical Workforce Standing Advisory Committee (MWSAC) (1997) Planning the Medical Workforce. Medical Workforce Standing Advisory Committee: Third Report. Rosen, R. and Dewar, S. (2004) On Being a Doctor. Redefining Professionalism for Better Patient Care. London: King’s Fund. Royal College of General Practitioners (RCGP) (1969) The educational needs of the future general practitioner, Journal of the Royal College of General Practice, 18, 358–60. Scott, A., Sullivan, F., Wordsworth, S. and Heaney, D. (2001) Evaluation of Salaried Payment for General Practitioners in Scotland. HERU Discussion Paper 02/01. Sennett, R. (1998) The Corrosion of Character. New York: WW Norton. Shuval, J. and Bernstein, J. (1996) The dynamics of professional commitment: immigrant physicians from the former Soviet Union in Israel, Social Science and Medicine, 42, 7, 965–74. Sibbald, B., Bojke, C. and Gravelle, H. (2003) National survey of job satisfaction and retirement intentions among general practitioners in England, British Medical Journal, 326, 22–6. Southerton, D. (2002) Boundaries of us and them: class mobility and identification in a new town, Sociology, 36, 171–93. Starfield, B. (1994) Is primary care essential? Lancet, 344, 1129–33. Walker, S. (2002) Working women seem to be scapegoats in medicine [letter], British Medical Journal, 324, 1453. Williams, G. and Popay, J. (1994) Lay knowledge and the privilege of experience. In Gabe, J., Kelleher, D. and Williams, G. (eds) Challenging Medicine. London: Routledge. Williams, J., Petchey, R., Gosden, T., Leese, B. and Sibbald, B. (2001) A profile of PMS salaried GP contracts and their effect on recruitment, Family Practice, 18, 283–7.
© 2006 The Authors. Journal compilation © 2006 Foundation for the Sociology of Health & Illness/Blackwell Publishing Ltd