171
Work 24 (2005) 171–182 IOS Press
The implementation of motor learning principles in designing prevention programs at work Tal Jarus∗ and Navah Z. Ratzon Department of Occupational Therapy, Tel Aviv University, Ramat Aviv, Tel Aviv 69978, Israel Tel.: +972 3 6409104; Fax: +972 3 6409933; E-mail:
[email protected]
Received 1 September 2003 Accepted 12 November 2003
Abstract. Occupational therapy practitioners offer services to workers in the workplace to prevent musculoskeletal disorders (MSDs), to help the injured worker restore function, and to recover capacities needed to return to the job. Despite the existence of some evidence about the efficacy of prevention programs, there is uncertainty and even disagreement among health professionals, about the outcome of prevention programs for people with MSDs. It is proposed that principles of motor learning can assist the therapist in structuring prevention programs to facilitate the workers learning of correct movement patterns. This paper discusses basic concepts of motor learning emphasizing characteristics of the learner, the type of task, the structure of practice and application to prevention programs at work settings. We present a four-stage model for prevention programs based on principles of both motor learning and ergonomics. This model coincides with the broad perspective suggested in current occupational therapy models which focuses on the person, the environment, the occupation and their effects on occupational performance.
1. Introduction Occupational therapists work with persons, groups, and organizations focusing on the performance of the occupations (e.g., self care, work, leisure) of life [43]. A focus on work as one category of occupation has been integral to the profession of occupational therapy since it was conceived. Providing opportunities for the development and refinement of work skills and behaviors is central to occupational therapy practice [51]. The challenge for the occupational therapist is to help the client attain and maintain a worker role. In the work place, one must learn how to activate one’s body in a proper way in order to prevent musculoskeletal disorders (MSDs). In cases where there is already an injury, a worker must relearn voluntary control over injured muscles in order to perform the work. Occupational ∗ Corresponding
author.
therapy practitioners of the 1990’s find themselves involved in addressing the work-related needs not only of clients, but also of industries and insurance companies. Injury-prevention programs and worker education are receiving greater emphasis. A major concern of occupational therapy is the identification of context characteristics that facilitate performance and encourage the development of skills [47]. For occupational therapy, where the client must learn or relearn motor skills and perform them efficiently later in different contexts, the acquisition conditions that produce optimal retention and transfer of the learned skills should be emphasized [33]. We propose that clients will achieve maximal progress in the workplace when intervention is guided by principles of motor learning. ‘Motor learning’ refers to a set of internal processes associated with practice or experience leading to relatively permanent changes in motor behavior [65,66]. This paper will present basic concepts in motor learning and will discuss the application of these concepts
1051-9815/05/$17.00 2005 – IOS Press and the authors. All rights reserved
172
T. Jarus and N.Z. Ratzon / Motor learning and preventing MSD at workstations
in the work environment. Back injury or cumulative trauma disorders of the hand and wrist account for millions of days lost from work and lost of productivity as well as workers’ compensation claims [69]. Americans make nearly 70 million visits to physicians’ offices each year seeking treatment for MSD’s. In 1999 alone, nearly 1 million US workers took time off because of work-related MSDs [79]. Low back pain (LBP) is the most common MSD and throughout western society and has increased dramatically during the last years [15, 52,54,55,80]. Therefore, this paper will focus on MSD prevention programs at work.
2. Prevention programs at work Prevention programs can be divided into primary and secondary prevention programs [21,22,36]. Primary prevention focuses on reducing the incidence of new episodes of injury. Primery prevention programs aim to assist the worker by increasing his or her resistance to musculoskeletal injury (proper lifting techniques, material handling, behavior modification) or to improve the work by reducing the physical demands, usually through the ergonomic redesign of tasks and work spaces [20]. Secondary prevention programs are designed primarily to reduce disability or work absenteeism for people who already have a problem; the programs are categorized as work place-based interventions and health system interventions [21]. Work place prevention programs include an active physician or therapist at work who is involved with instructing workers immediately after a musculoskelatal injury and modifying duties at work. In the secondary prevention programs of the health system, health care givers who diagnose and treat workers are required mainly to minimize pain and disability, and structure rehabilitation programs. Prevention programs vary from place to place, yet, most back injury prevention programs include (1) back belts, (2) exercise/flexibility training, (3) back schools, and (4) educational classes. These programs may include combinations of education in: back pain/injury prevention, wearing the belt, fitness body mechanics, lifting ergonomics, and structure and function of spine; demonstration and practice of body mechanism and basic exercises; training in injury prevention methods; ergonomic improvements; pain control relaxation; and supervised practice sessions with individual feedback [37].
2.1. The efficacy of prevention programs Despite the existence of some evidence about the efficacy of prevention programs, there is uncertainty and even disagreement among health professional about the outcome of intervention programs for people with MSD [6,11]. Most programs for exercise/flexibility training and back schools were found to have positive effects [37] whereas, evidence supporting the use of back braces and back belt programs and education programs in industry is conflicting [40,46,53,62]. Carlton [9] found that there was no carryover of the information learned regarding proper body mechanics to the actual work site. Furthermore, Frank et al. [21] reported that in some places where secondary prevention program was offered at the workplace, the workers perceived these programs as pressure for premature return to work. Indeed, very few interventions have produced a clear reduction in the incidence of musculoskeletal injuries when evaluated by rigorous scientific criteria [17,20]. Moreover, despite intervention attempts, the overall trend for work related injuries has been relatively stable over the past several decades [16], or on the rise as claimed by some [15,52,54,55,80]. Minimal progress in reduction may be due to lack of etiologic understanding, lack of appropriate intervention selection, or lack of appropriate intervention implementation. Turner [78], argues that when researching prevention programs, the length of time of follow up is critical. She claims that workers who attended back school programs do show significantly fewer sick-leave days during their initial pain episode than those in a placebo treatment. However, there were no differences between back school, physiotherapy, and placebo groups on measures of pain, function or recurrence of pain during follow up a year later. Her findings concur with other researchers who found that prevention programs were less effective during follow-up [5,31,41]. From the above discussion it is apparent that primary and secondary work prevention programs are limited in their effectiveness. In an attempt to rectify this situation it is proposed that principles of motor learning can assist the therapist in structuring prevention programs, in order to facilitate workers learning of correct movement patterns. 2.2. Motor learning Motor learning refers to a set of internal processes associated with practice or experience leading to rela-
T. Jarus and N.Z. Ratzon / Motor learning and preventing MSD at workstations
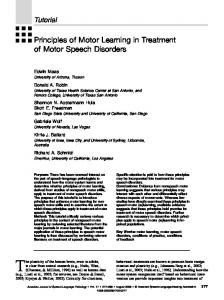
tively permanent changes in motor behavior [65]. The motor learning process involves three main phases, acquisition, retention, and transfer. For example, a worker learning to lift a box correctly (acquisition pahse) should be able to perform this task a week later (retention phase) and to transfer this learning and correctly lift different items at the workplace (transfer phase). The acquisition phase may indicate performance, while the retention and transfer phases may indicate learning [48,63,66]. As occupational therapists, we meet our clients for a limited period of time. Our main focus is not necessarily how the person performs the task in treatment, but rather how the person will perform in the future in his or her natural environment – at home or at work [33]. As mentioned earlier, some evidence shows that outcome of current intervention programs do not demonstrate good retention, as indicated by longer follow-up studies [5,31,41], nor good transfer of training to the work site [9]. Research in the area of motor learning that focuses on the understanding of acquisition and practice of motor skills, investigates how different factors influence the process of movement acquisition. Research of prevention of MSDs in work settings focuses on how different factors influence placing and maintaining workers in an occupational environment. Interestingly enough, the factors of both areas parallel those mentioned as critical concepts in most occupation models presented in the last decade in occupational therapy literature. The Person-Environment-Occupation (PEO) model [12–14,42], includes three major constructs: The person, which in motor learning literature is referred to as the learner and in work settings as the worker; occupation, which is referred to as the task, in both motor learning and ergonomics; and the environment, parallels to the structure of practice in the motor learning literature and analysis of work site in ergonomics (see Fig. 1). Motor learning studies investigating characteristics of the learner ask questions such as, are there people who learn movements faster than others? Can we identify those people and characterize them? Does intelligence influence motor learning? What is the relation between the age of the learner and motor learning? Within the domain of motor learning, studies also explore factors relating to type of task. Typical questions include: do we have to use different teaching methods in order to teach different categories of tasks? How does the complexity level of the task affect motor learning? Finally, studies questioning issues related to the structure of practice may ask for example, how much
Person Learner Worker
OP ML
173
Environment Structure of Practice analysis of work site
Occupation Task Work OP – occupational performance ML – motor learning
Fig. 1. Incorporating the PEO model with motor learning and ergonomic concepts.
feedback to give to the learner during practice? How accurate should the feedback be? Is the length of practice time important? How does context of practice affect motor learning? For the purpose of this paper we will elaborate on a few topics of the above issues that are relevant to prevention programs at work. 2.3. Characteristics of the learner 2.3.1. Age Many studies investigated the processes related to the effects of age on motor performance in individuals past puberty or in the upper age categories. One generalization is that, past the age of about 25 years, a progressive decline occurs in just about every measurable aspect of motor behavior [74]. For example, a systematic reduction in reaction time (RT) and movement time (MT) occurs through the developmental years up to about age 19, followed by a period of relatively stable capability through age 30 and a systematic slowing in both these variables as age increases further [23,64,74]. This trend is typical of many other variables that could be studied, such as strength, speed, postural control, perceptual skills, and anticipation [59,61,74,75,81,86]. In tasks for which both accuracy and speed are required, the overall score will often negatively affected with increasing age because speed decreases even though accuracy is either increased or held constant [66]. Studies showed that some of this slowing down need not be related to any slowing in the central nervous system, but rather is related to the fact that older people appear to be more “cautious” than younger people [84]. The highest incidence rate for accidents at work leading to an absence of more than three days is recorded among
174
T. Jarus and N.Z. Ratzon / Motor learning and preventing MSD at workstations
workers under the age of 26 (5830 per 100,000), either because they are in high-risk jobs or because their actions or lack of experience place them at high risk. Although beyond this age the incidence rate of accidents declines, the seriousness of accidents increases, rising from 3.6 accidents per 100,000 among those aged under 26, to 8.9 per 100,000 among the 46–65 age group [19]. This evidence from the work place might indicate that younger workers are faster and more reckless, thus are more inclined to be involved in accidents, albeit less severe ones. On the other hand, it seems that due to the slowing down with age and difficulties in stability, there are more falling, dropping, and “missing” accidents for elderly workers, which lead to fatal results. When planning prevention programs at work depending on the age of the person, instructions on whether to pay attention to the speed or the accuracy while performing tasks should differ. In addition, workers might need practice on different aspects of the task depending on their age. For example, it is recommanded to emphasize techniques that compensate for decrease in strength in older workers, like more short breaks, incorporating technical equipment (such as lifts, pullies), or to emphasize practicing timing in tasks where the timing is not determined by the person. 2.3.2. Trait anxiety Trait anxiety is a stable measure of the individual’s general tendency toward worry or anxiety [66]; it does not fluctuate very much from moment to moment or from task to task.Yerkes and Dodson [91] suggested that with increased arousal, performance increases to an optimal point and then decreases with further increases in arousal. This well known inverted-U principle, now termed “Zones of optimal functioning” [28,67], was supported by research evidence (e.g. [38,50,83]). In addition, each person has a range of individual optimal arousal which results in optimal function and improved performance [28]. Such support was also found at the work place [58]. Alternative views suggested that the relationship between anxiety and performance is much more complex than the relationship suggested by the inverted-U principle (for e.g. [1,28–30]) and requires further empirical examination [66]. Given the fact that high and low trait-anxious people respond with different amounts of arousal to identical stress situations, it has been found that these altered levels of arousal lead different people to perform diversely in similar situations. If a given level of arousal is optimal for a specific motor task, an individual who is high trait-anxious will reach that level with less ex-
• State anxiety • Instructions
• Trait anxiety
(mo tivating techniques)
Structure of Practice
Learner ML
Task
• Complexity • Novelty ML - motor learning
Fig. 2. Factors relating to anxiety that affect motor learning.
ternal motivation than will an individual who is classified as low trait-anxious. Thus, there is a risk of overmotivating the high trait-anxious individual or undermotivating the low trait-anxious individual [8]. Individuals high in trait anxiety tend to perform better than individuals with normally low arousal levels on very simple tasks. On the other hand, these high-anxious individuals tend to do worse on complex tasks, especially if novel responses are required. Additionally, it was found that there is a marked inferiority of high-anxious people early in the practice sequence as compared to the low-anxious people, but this difference dissipated with continued practic [67]. Therefore instructors in prevention programs should probably use motivating techniques very carefully in early practice, especially if the tasks are dangerous or the learners are high in trait anxiety, because motivation techniques will further elevate levels of anxiety (see Fig. 2). The type of task interacts with level of arousal thereby effecting performance. A task that requires fine motor control (such as delicate welding tasks, brain surgery) or contains important decision-making (as in fire fighters or piloting an airplane), will benefit from a lower level of arousal [82]. On the other hand, for gross-motor tasks (as lumberjacking), or tasks that are not cognitively complex (lifting heavy weights) a higher level of arousal is probably needed for maximum performance. Tasks that have high force requirements, relatively stereotyped response patterns, and high levels of practice appear to be least affected by stress. Finally, the situation in which the person performs can effect his/her anxiety level. Environmental factors that may increase arousal, include noise, heat, and humidity. In
T. Jarus and N.Z. Ratzon / Motor learning and preventing MSD at workstations
these situations, stimulus variety and intensity should also be noted. At the work setting there are certain psychosocial conditions that can affect the level of arousal. For example, numerous studies have shown that if people work at monotonous, boring tasks for long periods of time, their performance deteriorates in direct proportion to the time spent on the task [26]. If individuals must monitor a radarscope or watch for defective parts on an assembly line, their chances of making correct responses decline in proportion to the time spent on the job. Indeed, in the typical workplace, documented psychological stressors include workers complaints about monotonous work, time pressure, high workload, lack of peer support, and poor supervisor-employee relationship [27]. Whether the worker is being observed by others, perceives that the demands of the task is above her/his capability, or perceive the situation to be threatening, anxiety levels will increase. Psychological stressors are frequently associated with psychosomatic complaints, health indicators, and with musculoskeletal problems [32]. Bonzani et al. [7] have shown that psychological stress results in a psychological state which, along with the current employment status, are the most important factors in prolonging disability among workers with MSD. When applying these factors to prevention programs, the instructor must consider the task, the work situation, and the trait anxiety level of the worker. Accordingly, the instructor should either increase or decrease the level of arousal. There are reliable and valid questionnairs therapists can use to measure trait and state anxiety, for example, the State Trait Anxiety Inventory ([STAI] 73). Yet, controlling and manipulating arousal levels is more an intuitive art form than a science. 2.4. Type of task A motor skill is defined as an integration of voluntary serial movements of the limb or body towards a specific goal directed action. One acquires a vast range of motor skills over time, some due to spontaneous action and some due to intentional effort [76]. Skill acquisition is task-dependent [24], where the structure of the task determines the demands placed upon the performer. Although motor skills are very difficult to categorize because they are so diverse [71], it is useful to describe them on somewhat independent continuums in order to understand these requirements and the processes underlying skill acquisition. There are few ways to classify motor skills, along a number of dimen-
175
sions, such as considering environmental predictability (open versus closed skills) [25,60], according to task organization and complexity (continuous, discrete, and serial skills), or the relative importance of motor and cognitive elements [66,67]. An open task is a task where the timing of the task is determined by the environment, while in a closed task the timing is determined by the performer [25,60]. For example, typing minutes of a meeting from a dictatape, where the timing of the typing is not controlled by the typist is an open task. The demand of such a task with regards to timing is different from a closed task, such as typing from a written report. This will affect the learning processes of these two tasks, because acquiring an open task involves the diversification of movement patterns over practice [25]. The range of movements generated must fit the variable environmental conditions (i.e., the variable speed of the discussion the typist has to follow) for the performer to be successful (i.e. typing the minutes). Automaticity is not possible. Practice with diversified movement patterns is recommended. In contrast, in the closed task, due to stable environmental conditions, the performer works on appropriately limiting movement patterns and the performance becomes more habitual or automatic. Extended practice under stable environmental conditions is recommanded. Other dimensions of the type of task that effect learning processes includes task complexity and task organization. Task complexity refers to how many parts or components are in the task. The more parts, the more complex the task is, for example, a floor exercise routine (highly complex) vs. lifting a patient (low complex). Task organization refers to how the components of a task are interrelated. The more the parts are intimately related to one another, the higher the degree of organization. As will be discussed in the next section, the type of practice suggested is greatly dependent on the type of task. Therefore, when considering prevention program planning , these concepts would translate into practical recommendations for the therapist on how to structure the prevention program.
3. Structure of practice 3.1. Similarity between context of practice and retention The amount of transfer and retention of a skill depends upon the similarity between the two tasks and/or
176
T. Jarus and N.Z. Ratzon / Motor learning and preventing MSD at workstations
contexts in which the task is performed. The higher the similarity between the component parts of the skills or two performance situations, the greater the amount of positive transfer [67,68]. Thus we would expect that the amount of transfer between using an electrical screwdriver with a specific screw, to using it with different size and shape of screws would be greater than the transfer between the screwdriver task and an assembly task. We would likewise expect that practice conditions which emphasize performance situations similar to those that are required in a work place would lead to a higher degree of transfer. Practicing an assembly task in a quiet, cool and dry place should lead to a low degree of transfer to completing this assembly task in a noisy, hot, humid factory, because the skills required to be successful in these two performance situations have very few components in common. Practicing a motor skill can be done in its entirety, i.e. whole practice, or of its component parts, i.e. part practice [85]. Predictions about the facilitating effect of part and whole practice conditions on the learning of a motor skill can be made rather confidently when the organization and complexity characteristics of the skill to be learned are taken into consideration [10,66, 71]. A skill that is relatively high in complexity (many components) and relatively low in organization (components are relatively independent) will benefit from part practice. Using this structure maximum transfer can be expected [56]. For example, the task of a supermarket worker includes bringing products from the warehouse to the main store, putting products on the shelves, organizing the new product on the shelf, placing the ordered products on the front of the shelf, placing non usable products of the trolley, and bringing them to the warehouse. This task include many steps (relatively high in complexity), yet the integration of the component parts of the task is low in demand (low in organization). It is possible to complete these steps in a different chronological manner, for example; fill several trolleys from the warehouse and continue with the above progression, or place the older products in the front of the shelf and then organize the new products in the back. In such a task, during prevention programs for reducing risk for MSDs, the worker can practice proper handling of each component separately. On the other hand, whole practice increase in effectiveness in a skill that is relatively low in complexity but high in organization. For example, tasks that lend themselves to the whole method are those in which timing and speed are critical in order not to destroy the total movement pattern and where the whole task might
be destroyed if isolated parts of the total task were practiced. To illustrate this consider a food-industry worker who has to complete a series of tasks, such as preparing the dough, baking and packing. Although each of these few tasks is simple (relatively low in complexity), yet the timing between each task is crucial (high in organization). Therefore, this worker has to practice the different components together because timing and coordination between those components is crucial. Being able to perform each of those components separately in a correct and safe position, does not predict the ability to perform them correctly once they are combined. Indeed certain adjustments cannot be practiced and learned when individuals practice the parts in isolation. This is especially true for tasks in which parts of it are simultaneous. Many tasks at the work place require that one part of the body has to be coordinated with another, such as two-handed simultaneous movements. Practicing the movements of one hand in isolation will not enable the worker to practice on the coordination between the two hands. 3.2. Distribution of practice Should learners continually practice on a skill with only a few brief rest periods, or should they practice for short periods of time with more frequent and prolonged intervals of rest? This scheduling can be considered within a short time frame, as within one meeting of an hour, or scheduling may be considered long term, as within a week or months of training. For example, Baddeley and Longman [2] found that postal workers learned a typing task used on a mail-sorting machine quickly when taught one hour/one session a day (for 60 days) than a group taught in two hours/two sessions a day (for 15 days). A practice schedule that requires continual practice with short and/or infrequent rest intervals between trials, is called massed practice. When rest intervals are longer and/or more frequent between trials or between a set of trials, this is called distributed practice [66,67]. Lack of conclusive evidence with regards to distribution of practice preclude the formulation of fixed guidelines for prevention programs. Nonetheless it seems from those studies that massing appears to be detrimental to performance (while practicing) and usually detrimental to learning motor skills, when compared to distributed practice [44]. Furthermore, massed practice may produce physical fatigue which by itself is considered a risk factor for MSDs. A few conclusions can be drawn. For tasks where there are elements of phys-
T. Jarus and N.Z. Ratzon / Motor learning and preventing MSD at workstations
ical risk and effort, massed practice can be a problem. Therefore, distributed practice is preferable when the energy demands of the task are high, the task is complex, the length of the task performance is great, the task is not meaningful, and motivation of the learner is low. Schmidt and Lee [66] stated that many tasks used in the industry entail more opportunity for injury if errors are made. Thus, when designing practice in prevention programs in which factors such as fatigue could put the worker at risk due to type of task or previous injury, caution is needed and it is suggested to assure that sufficient rest is provided between practice attempts. The therapist should analyze and match the energy demands of tasks and fitness levels of workers in order to tailor practice conditions with sufficient rest periods. Unfortunately the therapist is often limited by financial and logistical constraints. A majority of prevention programs are financed by the employer and it is therefore clear that from an administrative point of view the goal is to plan as short a program as possible [57]. The limited succes of some prevention programs may be due to insufficient practice. Therefore, even though distributed practice requires a longer period of time to complete, it would be preferable because it results in a better learning effect. On the other hand, massed practice requires less time but results in a reduced learning effect and increases the risk for injury. 3.3. Focus of attention One of the goals of the instructor is to help the learner direct his or her focus of attention to the most relevant and useful source of information. When performing motor tasks one can focus the attention on the task or object, or on the movement itself. An example would be focusing on the box while picking it up as compared to focusing on specific body segments (e.g., legs and back). Recent studies in motor learning that looked at ‘focus of attention’ found that focusing one’s attention externally (i.e., on the object or the effect of the action) as compared to internally (i.e., your movement or the action itself) enhances motor learning and performance [72,88–90]. For example, using a ski-simulator task, instructing participants to focus on the force they exerted on the wheels of the platform was more effective than focusing their attention on the feet that exerted the force, even though the wheels were located directly under the feet [88]. These results are demonstrated consistently with a variety of tasks such as a balance task (stabilometer), golf, and tennis. This seems to
177
complement findings from occupational therapy literature that investigated the effects of “purposefulness”. It is suggested that performing purposeful activity enhances motor performance and learning because it directs attention of the performer externally [35]. Applying these findings seems to suggest that when instructing the worker in the prevention programs, we should direct the workers’ attention to external cues, rather than on their own movement. This is actually contradicting current methods used in prevention programs, where the worker is encouraged to think about his or her movements, focusing on the structure and function of the spine, pain control, relaxation and more [37]. Alternatively instructions should include directing the worker to concentrate on the distance, the height and the weight of the box rather than on the body mechanism and the amount of force needed. It is also possible to practice near a wall and instruct the worker to focus on the force they exerted on the wall rather than focusing their attention on the posture of the back. 3.4. Schedule of practice In most prevention programs the goal is to teach more than a single skill because typically most workers have to perform varied tasks at the work site. Nursing, for example, is considered a profession with high risk for MSDs [39,77] because of its multiple exertion tasks. A nurse has to transfer clients from different places (bed to chair, chair to bathtub, bed to bed, etc), to turn clients over in bed, to carry different objects, and more. It is therefore asked, how to sequence the practice of a number of tasks within a session in order to maximize learning. Battig [4] coined the term contextual interference, which is conceptualized as the effect that contextual variables have on processing demands during practice, and their subsequent effects on memory and transfer of skills. One of Battig’s predictions [3] was concerned with practice order when acquiring few tasks. Contextual interference was operationalized as changes (high contextual interference, random presentation) or repetitions (low contextual interference, blocked presentation) of practice conditions over trials during acquisition. For example, a nurse has to learn to correctly pick up people of different weights and body size from different heights, in a random order. A blocked practice will include picking up the same weight for few trials in a consecutive order, and only then practicing a new weight. A random order, which will be more beneficial than the blocked order, will present the different weights in an unpredictable random order. Battig [3]
178
T. Jarus and N.Z. Ratzon / Motor learning and preventing MSD at workstations Table 1 The four-stages model
Stage The first stage, ground setting The second stage, basic intervention The third stage, progressive intervention The fourth stage, follow up
Nature Assessment of the setting, the worker and the task Group practice to acquire basic safety rules and correct body mechanism based on principles of motor learning Individual practice to upgrade motor skills of specific worker for specific work-station. Individual assessment as a follow up; if there is a need, go back to the second stage
predicted that high contextual interference conditions would hinder acquisition performance, but facilitate retention and transfer when compared to low contextual interference conditions (see Magill and Hall [49] for a review). These predictions have been supported for a variety of motor tasks, including aiming, rapid ballistic movements, timing, and tracking (e.g. [18,22,34,45,70, 87,92]). Although there is a debate in the literature whether the benefit of random practice is true for all types of tasks [49] and for learners with different skill levels [67], in general, there is vast support for the idea that random unpredictable practice is more beneficial for learning as compared to blocked predictable practice, especially with adults. Going back to the example of the nurse who learns to transfer correctly people from bed to chair, rather than practicing on picking up each weight from a sepcific hight separately, it is recommended to practice picking up different weights from different hights in a random order. Therefore, it seems that in planning prevention programs where the worker has to learn few tasks, presenting them in a random order will promote problem solving and therefore be more beneficial.
4. Discussion With so many variables to consider, one can not formulate one ideal prevention model for all work settings. Developing instruction methods for prevention programs at work should be specific to the work place, the worker and the task. Nevertheless, beyond the different work settings we would like to present a fourstage model prevention program which will utilize the principles and knowledge presented above (see Table 1 for depiction of the model). These stages are presented assuming that because some efficiency is needed, most prevention programs are held in groups rather than individually.
Time frame Short Intense/condense Continuous Periodical/short
4.1. Stage I, ground setting Stage I requires on site task analysis as well as examination of the work environment and a relevant assessment of the worker. This stage is essential for building a proper prevention program matched to the worker, the type of task the worker is meant to do, and the workstation in which he or she performs. During the first stage the therapist is summarizing the work setting, personal information and mapping the potential groups. In this stage the following type of questions will be asked: Is the task performed in a noisy, hot, humid work place or does the worker perform it in a quiet, cool place? Is the worker young or old, is he stressed in nature or relaxed? Is he a skillful person or is he new on the job? All these questions could affect the process of acquiring the skills needed in order to perform the task with minimal damage. 4.2. Stage II, basic intervention In stage II, individuals will acquire their work tasks. They will acquire correct body mechanisms in order to work in a safe manner, based on the first stage where the setting, the worker and the task were evaluated. This stage will be conducted in a group format, where mutual basic safty rules will be taught. The prevention program at this stage will be modified by principles of motor learning to insure that the worker will be able to retain and transfer the task to the work setting and will go along with ergonomic principles used to prevent level of exertion and to protect workers. For example, non-repetitive order of practice (random order) is recommended by both motor learning and ergonomic priniciples. Furthermore, both motor learning theory and ergonomic principles concur that performing high energy task require adequate rest, thereofore practice with many rest breaks (distributed practice) is preferred. Ideally, this stage will occur when the worker is first being introduced to his or her work place, thereby pre-
T. Jarus and N.Z. Ratzon / Motor learning and preventing MSD at workstations
venting the development of bad habits. Yet, in reality many times stage II occuring at times when no introduction and group practice is available, i.e. the worker arrives to the work station after the group parctice was completed. In such cases, it is recommended that professional personel like an occupational therapist will escort the new worker through this stage, on an individual basis before moving to the third stage. In such a case, stage II will be an individual stage where primary basic intervention is held until the new worker will be placed in the suitable progressive intervention stage. 4.3. Stage III, progressive intervention Stage III is an on going individualized program in which individuals are placed according to the results of the evaluation that was done at the first stage and their performance in the second stage of the prevention program. This stage will enable us to apply skills acquired in the second stage and to further upgrade the motor skills needed for doing the work safely. At this stage a customized program will be designed to fit the specific worker and the specific work-station. For example, the older worker will be directed to pay attention to the speed, emphasize practicing timing in tasks where the timing is not determined by the person. Furthermore, practice techniques that compensate for decrease in strength, such as more short breaks or incorporating technical equipment (such as lifts, pullies), and practice postural control will be reinforced. The younger worker will be directed to focus on reducing pace, rising accuracy, training avoidance of dangerouse spots that are known as risk factors for accidents. Another example can be the level of arousal (based on valid and reliable questionnaires). The trait anxiety level of the worker together with the type of task and the work situation can determine the instructions given. Accordingly, the instructor should either increase or decrease the level of arousal with motivational techniques (incentives, rewards, and sanctions), structuring the environment (control of sensory intensity and variety, amount of noise, temperature), cognitive strategies (distract the performer from arousal-inducing content), relaxation techniques (kinesthetic awareness of tension in muscles, visualization), or biofeedback (self-regulate processes that control arousal states). Supervision will be carried on a gradually reduced frequency, in the work site. If possible, the workers will be placed in small groups according to the different tasks and worker characteristics. For example, it is possible to divide the workers into those who mostly
179
perform simple tasks and those who mostely perform complex tasks. Further division can be based on age, or years of experience with the task. As mentioned in the previous stage, while this stage is working as an on going intervention, for new workers this program will act as a primary prevention program whereas for others as a secondary prevention program. 4.4. Stage IV, follow up In the IV stage, the efficacy of the prevention program will be evaluated in terms of the worker’s retention and transfer performance. On site and long term follow up are recommended for this stage. A proficiency perspective is frequently used to analyze motor skills and can be used to examine the success of a prevention program. Specifically, analyzing the features that distinguish the higher-skilled performers from lower-skilled ones. It is advantageous to examine the degree of goal achievement by the worker, the energy expended in task performance as well as a timed indicator of task completion. Moreover, follow up should include monitoring of general well being of the worker, worker satisfaction, and specifically complaints about MSD’s. Based upon these results, a decision can be made about whether or not there is a need to go back to the second stage of the intervention, and when to perform the follow up stage again. To summarize, this paper attempted to implement some principles taken from motor learning theory and apply them to the design of prevention programs at work. We propose that the combination of motor learning and ergonomic principles has to be studied in order to base the notion that such combination might contribute to a more effective prevention program. Analyzing both the characteristics of the task involved and the learner, and accordingly plan the structure of practice would be beneficial for improved long term effects. This certainly coincides with the broad perspective suggested in current occupational therapy models viewing the person, the environment and the occupation and their effect on occupational performance. Research with multidimensional attitude is needed to examine the effectiveness of each factor of the guidelines presented above.
References [1]
M.J. Apter, Reversal theory and personality: A review, Journal of Research in Personality 18 (1984), 265–288.
180 [2]
[3]
[4]
[5]
[6]
[7]
[8]
[9]
[10]
[11]
[12]
[13]
[14]
[15]
[16]
[17]
[18]
[19] [20]
T. Jarus and N.Z. Ratzon / Motor learning and preventing MSD at workstations A.D. Baddeley and D.J.A. Longman, The influence of length and frequency of training session on the rate of learning to type, Ergonomics 21 (1978), 627–635. W.F. Battig, Facilitation and interference, in: Acquisition of skill, E.A. Bilodeau, ed., N.Y. Academic Press, 1966, pp. 215– 244. W.F. Battig, The flexibility of human memory, in: Levels of processing in human memory, L.S. Cermak and F.I.M. Craik, eds, Hillsdale, NJ: Erlbaum, 1979, pp. 23–44. D.M. Berwick, S. Budman and M. Feldstein, No clinical effect of back schools in an HMO. A randomized prospective trial, Spine 14(3) (1989), 338–344. P.C. Bohr, Office ergonomics education: A comparison of traditional and participatory Methods, Work 19(2) (2002), 185– 191. P.J. Bonzani, L. Millender, B. Keelan and M.G. Mangieri, Factors prolonging disability in work-related cumulative trauma disorders, Journal of Hand Surgery 22(1) (1997), 30–34. M.G. Calvo, Effort, aversive representation and performance in test anxiety, Personality and Individual Differences 6 (1985), 563–571. R.S. Carlton, The effects of body mechanics instruction on work performance, American Journal of Occupational Therapy 41(1) (1987), 16–20. C.J. Chamberlin and T.D. Lee, Arranging practice conditions and designing instruction, in: Handbook on research in sport psychology, R.N. Singer, M. Murphey and L.K. Tennant, eds, New York: McMillan, 1992. D.C. Cherkin, R.A. Deyo, J.H. Street, M. Hunt and W. Barlow, Pitfalls of patient education-limited success of a program for back pain in primary care, Spine 21(3) (1996), 345–355. C. Christiansen, Occupational therapy: Intervention for life performance, in: Occupational therapy: Overcoming human performance deficits, C. Christiansen and C. Baum, eds, Thorofare, New Jersey: Slack, 1991, pp. 4–43. C. Christiansen and C. Baum, Occupational therapy: Overcoming human performance deficits, Thorofare, NJ: Slack, 1991, pp. 4–43. C. Christiansen and C. Baum, Occupational therapy: Enhancing function and well-being, (2nd ed.), Thorofare, NJ: SLACK Incorporated, 1997. D.I. Clemmer, D.L. Mohr and D.J. Mercer, Low-back injuries in a heavy industry. I. Worker and workplace factors, Spine 16 (1991), 824–830. T.K. Courtney, A. Burdorf, G.S. Sorock and R.F. Herrick, Methodological challenges to the study of occupational injury – an international epidemiology workshop, American Journal of Industrial Medicine 32 (1997), 103–105. L.M. Daltroy, M.D. Iverson, M.G. Larson, R. Lew, E. Wright, J. Ryan, C. Zwerling, A.H. Fossel and M.H. Kiang, A controlled trial of an education program to prevent low back injuries, New England Journal of Medicine 337(5) (1997), 322– 328. P. Del Rey, E. Wughalter and M. Whitehurst, The effects of contextual interference on females with varied experience in open sport skills, Research Quarterly for Exercise and Sport 53 (1982), 108–115. European communities, 1995–2002, Available: http://europa.eu.int/geninfo/copyright en.htm. J.W. Frank, M.S. Kerr, A.S. Brooker, S.E. DeMaio, A. Maetzel, H.S. Shannon, T.J. Sullivan, R.W. Norman and P.R. Wells, Disability resulting from occupational low back pain. Part I: What do we know about primary prevention? A review of
[21]
[22]
[23]
[24] [25]
[26]
[27]
[28]
[29]
[30]
[31]
[32]
[33]
[34]
[35]
[36]
[37]
the scientific evidence on prevention before disability begins, Spine 21(24) (1996), 2908–2917. J.W. Frank, A.S. Brooker, S.E. DeMaio, M.S. Kerr, A. Maetzel, H.S. Shannon, T.J. Sullivan, R.W. Norman and P.R. Wells, Disability resulting from occupational low back pain. Part II: What do we know about secondary prevention? A review of the scientific evidence on prevention after disability begins, Spine 21(24) (1996), 2918–2929. K.E. French, J.E. Rink and P.H. Werner, Effects of contextual interference of three volleyball skills, Perceptual and Motor Skills 71 (1990), 179–186. J.L. Fozard, M. Vercruyssen, S.L. Reynolds, P.A. Hancock and R.E. Quilter, Age differences and changes in reaction time: The Baltimore longitudinal study of aging, Journal of Gerontology: Psychological sciences 49 (1994), 179–189. A.M. Gentile, A working model of Skill acquisition with aplication of teaching, Quest Monograph 17 (1972), 3–23. A.M. Gentile, Skill acquisition: Action, movement, and neuromotor processes, in: Movement science: Foundations for physical therapy in rehabilitation, J.H. Carr, R.B. Shepherd, J. Gordon and J.M. Held, eds, Maryland: Aspen, 1987, pp. 93– 154. M. Gillberg and T. Akerstedt, Sleep loss and performance: no safe duration of a monotonous task, Physiology & Behavior 64 (1998), 599–604. T.R. Hales and P.B. Bernard, Epidemiology of work-related musculoskeletal disorders, Orthopedic Clinic of North America 27 (1996), 679–709. Review. Y.L. Hanin, A study of anxiety in sports, in: Sport pschology: An analysis of athlete behavior, W.F Stroub, ed., Ithaca, NY: Mouvement, 1980, pp. 236–249. Y.L. Hanin, Interpersonal and intragroup anxiety in sports, in: Anxiety in Sports: an international perspective, revising D. Hackfort and C.D. Spielberger, eds, New York: Hemisphere, 1989, pp. 19–28. L. Hardy, A catastrophe model of performance in sports, in: Stress and performance in sport, J.G. Jones and L. Hardy, eds, Chichester: Wiley, 1990, pp. 81–131. K. Harkapaa, G. Mellin, A. Jarvikoski and H. Hurri, A controlled study on the outcome of inpatient and outpatient treatment of low back pain. Part III. Long-term follow-up of pain, disability, and compliance, Scandinavian Journal of Rehabilitation Medicine 22 (1990), 181–188. I.L. Houtman, P.M. Bongers, P.G. Smulders and M.A. Kompier, Psychosocial stressors at work and musculoskeletal problems, Scandinavian Journal of Work Environmental Health 20 (1994), 139–145. T. Jarus, Motor learning and occupational therapy: Organization of practice, American Journal of Occupational Therapy 48 (1994), 810–816. T. Jarus, E.H. Wughalter and J.G. Gianutsos, Effects of contextual interference and conditions of movement task on acquisition, retention, and transfer of motor skills by women, Perceptual and Motor Skills 84 (1997), 179–193. T. Jarus, T.D. Lee and L. Wishart, Enhancing performance through meaningful exercise: A motor learning and control perspective, Paper presanted at the meeting of the American Assossiation of Occupational Therapy, Miami, FL, July, 2002. T. Jones and S. Kumar, Physical ergonomics in low-back pain prevention, Journal of Occupational Rehabilitation 11(4) (2001), 309–319. Review. B.E. Karas and K.M. Conrad, Back injury prevention interventions in the workplace: an integrative review, AAOHN J 44(4) (1996), 189–196. Review.
T. Jarus and N.Z. Ratzon / Motor learning and preventing MSD at workstations [38]
[39]
[40]
[41]
[42]
[43] [44]
[45]
[46]
[47]
[48] [49]
[50]
[51]
[52]
[53]
[54]
[55] [56]
P. Klavora, An attempt to derive Inverted-U curves based on the relationship between anxiety and athletic performance, in: Psychology of motor behavior and sports, D.M. Landers and R.W. Christina, eds, Champaign, IL: Human Kinetics, 1977, pp. 369–377. S. Koda, A. Hisashige, T. Ogawa, N. Kurumatani, M. Dejima, T. Miyakita, R. Kodera, H. Hamada, S. Nakagiri and H. Aoyama, An epidemiological study on low back pain and occupational risk factors among clinical nurses, Sangyo Igaku 33 (1991), 410–422. A. Lahad, A.D. Malter, A.O. Berg and R.A. Deyo, The effectiveness of four interventions for the prevention of low back pain, JAMA 26;272(16) (1994), 1286–1291. G.J. Lankhorst, R.J. Van de Stadt, T.W. Vogelaar, J.K. Van der Korst and A. J. Prevo, The effect of the Swedish Back School in chronic idiopathic low back pain. A prospective controlled study, Scandinavian Journal of Rehabilitation Medicine 15(3) (1983), 141–145. M. Law, B. Cooper, S. Strong, D. Stewart, P. Rigby and L. Letts, The person-environment-occupation model: A transactive approach to occupational performance, Canadian Journal of Occupational Therapy 63 (1996), 9–23. M. Law, C. Baum and W. Dunn, Measuring occupational performance, Thorofare, NJ: Slack Incorporate, 2001. T.D. Lee and E.D. Genovese, Distribution of practice in motor skill acquisition: Learning and performance effects reconsidered, Research Quarterly for Exercise and Sport 59 (1988), 277–287. T.D. Lee and R.A. Magill, The locus of contextual interference in motor- skill acquisition, Journal of Experimental Psychology, Learning, Memory and Cognition 9 (1983), 730–746. S.A. Levender, S.H. Chen, Y.C. Li and G.B.J. Andersson, Pulling on slippery versus non-slippery surfaces: Can a lifting belt help? Proceeding of the Human Factors and Ergonomics Society 40th Annual Meeting, 1996. H. Ma, C.A. Trombly and C. Robinson-Podolski, The effect of context on skill acquisition and transfer, American Journal of Occupational therapy 53 (1999), 138–144. R.A. Magill, Motor learning: Concepts and applications, (3rd ed.), Dubuque, IA: Wm. C. Brown, 1989. R.A. Magill and K.G. Hall, A review of the contextual interference effect in motor skill acquisition, Human Movement Science 9 (1990), 241–289. R. Martens and D.M. Landers, Motor performance under stress: A test of the inverted- U hypothesis, Journal of Personality and Social Psychology 16 (1970), 29–37. L. Matheson, Development of a measure of perceived functional ability, Journal of Occupational Rehabilitation 3(1) (1993), 15–30. H.S. Miedema, A.M. Chorus, C.W. Wevers and S. van-derLinden, Chronicity of back pain problems during working life, Spine 23(18) (1998), 2001–2009. L. Mitchell, F.H. Lawler, D. Bowen, W. Mote, P. Asundi and J. Purswell, Effectiveness and cost-effectiveness of employerissued back belts in areas of high risk for back injury, Journal of Occupational Medicine 36(1) (1994), 90–94. A.L. Nachemson, Instability of the lumbar spine. Pathology, treatment, and clinical evaluation, Neurosurgery Clinics of North America 2(4) (1991), 785–790. Review. A.L. Nachemson, Newest knowledge of low back pain. A critical look, Clinics Orthopedics 279 (1992), 8–20. Review. J. Naylor and G. Briggs, Effects of task complexity and task organization on the relative efficiency of part and whole train-
[57] [58] [59]
[60] [61]
[62]
[63] [64] [65] [66]
[67]
[68]
[69]
[70]
[71] [72]
[73]
[74] [75]
[76] [77]
181
ing methods, Journal of Experimental Psychology 65 (1963), 217–244. G.B. Orr, Ergonomics programs for health care organizations, Occupational Medicine 12 (1997), 687–700. F. Pheasant, Ergonomics, work and health, Aspen Pub. Inc. Gaithersburg, Maryland, 1991, pp. 144–147. P.S. Pohl, C.J. Winstein and B.E. Fisher, The locus of agerelated movement slowing: sensory processing in continues goal-directed aiming, Journal of Gerontology: Psychological Sciences 51 (1996), 94–102. E.C. Poulton, On prediction in skilled movements, Psychological Bulletin 54 (1957), 467–478. J. Pratt, A.L. Chasteen and R.A. Abrams, Rapid aimed limb movements: Age differences and practice effects in components sub-movements, Psychology and Aging 9 (1994), 325– 334. C.R. Raddell, J.J. Congleton, R.D. Huchingson and J.F. Montgomery, An evaluation of a weightlifting belt and back injury prevention training class for airline baggage handlers, Applied Ergonomics 23(5) (1992), 319–329. G.H. Sage, Motor learning and control: A new neuropsychological approach, Dubuque, Iowa: Wm. C. Brown, 1984. T.A. Salthouse, A theory of cognitive aging, Amsterdam: Elsevier, 1985. R.A. Schmidt, Motor control and learning: A behavioral emphasis, (2nd Ed.), Champaign, IL: Human Kinetics, 1988. R.A. Schmidt and T.D. Lee, Motor control and learning: A behavioral emphasis, (3rd Ed), Champaign, IL: Human Kinetics, 1999. R.A. Schmidt and C.A. Wrisberg, Motor Learning and Performance: A problem-based learning approach, (2nd ed.), Champaign, IL: Human Kinetics, 2000. R.A. Schmidt and D.E. Young, Transfer in motor control in motor skill learning, in: Transfer of learning, S.M. Cormier and J.D. Hagman, eds, Orlando, FL: Academic Press, 1987, pp. 47–79. R.J. Schwartz, L. Benson and L.M. Jacobs, The prevalence of occupational injuries in EMTs in New England, Prehospital Disaster Medicine 8(1) (1993), 45–50. J.B. Shea and R.L. Morgan, Contextual interference effects on the acquisition, retention, and transfer of a motor skill, Journal of Experimental Psychology: Human Learning and Memory 5 (1979), 179–187. C.H. Shea, W.L. Shebilske and S. Worchel, Motor learning and control, Englewood Cliffs, NJ: Prentice Hall, 1993. C.H. Shea and G. Wulf, Enhancing motor learning through external-focus instruction and feedback, Human Movement Science 18 (1999), 553–571. C.D. Spielberger, anxiety as an emotional state, in: Anxiety: current trends in theory and research, C.D. Spielberger, ed., NY: Academic Press, 1966. W.W. Spirduso, Physical dimensions of aging, Champaign, IL: Human Kinetics, 1995. N. Teasdale, C. Bard, J. LaRue and M. Fleury, on the cognitive penetrability of posture control, Experimental Aging Research 19 (1993), 1–13. J.F. Travers, Learning analysis and applications, (3ed ed.), New York: David McDay, 1970. A.M. Trinkoff, J.A. Lipscomb, J. Geiger-Brown, C.L. Storr and B.A. Brady, Perceived physical demands and reported musculoskeletal problems in registered nurses, American Journal of Preventive Medicine 24(3) (2003), 270–275.
182 [78]
[79]
[80] [81]
[82]
[83]
[84] [85] [86]
T. Jarus and N.Z. Ratzon / Motor learning and preventing MSD at workstations J.A. Turner, Educational and behavioral interventions for back pain in primary care, Spine 15;21(24) (1996), 2851–2857, discussion 2858–2859. Review. U.S. Department of Health and Human Services, The Research Council- the principal operating arm of the National Academy of Sciences and the National Academy of Engineering, 1991. G. Waddell, Biopsychosocial analysis of low back pain, Ballieres Clinical Rheum 6 (1992), 523–527. M.G. Wade, R. Lindquist, J.R. Taylor and D. Treat-Jacobson, Optical flow, spatial orientation, and the control of posture in the elderly, Journal of Gerontology: Psychological Sciences 50B (1995), 51–58. R.S. Weinberg and V.V. Hunt, The interrelationships between anxiety, motor performance and electromyography, Journal of Motor Behavior 8 (1976), 219–224. R.S. Weinberg and J. Ragan, Motor performance under three levels of trait anxiety and stress, Journal of Motor Behavior 10 (1978), 169–176. A.T. Welford, Psychomotor performance, Annual Review of Gerontology and geriatrics 4 (1984), 237–273. D.C. Wightmam and G. Lintern, Part- task training for tracking and manual control, Human Factors 27 (1985), 267–283. M.H. Woollacott and D.L. Manchester, Anticipatory postural
[87]
[88]
[89]
[90]
[91]
[92]
adjustments in older adults: Are changes in response characteristics due to changes in strategy? Journal of Gerontology: Psychological Sciences 48 (1993), 64–70. C.A. Wrisberg and Z. Liu, The effects of contextual interference variety on the practice, retention, and transfer of an applied motor skill, Research Quarterly for Exercise and Sport 62 (1991), 406–412. G. Wulf, M. Hob and W. Prinz, Instruction for motor learning: differential effects of internal versus external focus of attention, Journal of Motor Behavior 30 (1998), 169–179. G. Wulf, B. Lauterbach and T. Toole, The learning advantage of an external focus of attention in golf, Research Quarterly for Exercise and Sport 70(2) (1999), 120–126. G. Wulf, N.H. McNevin, T. Fuchs, F. Ritter and T. Toole, Intentional focus in complex skill learning, Research Quarterly for Exercise and Sport 71(3) (2000), 229–239. R.M. Yerkes and J.D. Dodson, The relation of strength of stimulus to rapidity of habit- formation, Journal of Comparative Neurology and Psychology 18 (1908), 459–482. D.E. Young, M.J. Cohen and W.S. Husak, Contextual interference and motor skill acquisition: On the processes that influence retention, Human Movement Science 12 (1993), 577– 600.