Arthritis & Rheumatism (Arthritis Care & Research) Vol. 47, No. 6, December 15, 2002, pp 645– 650 DOI 10.1002/art.10788 © 2002, American College of Rheumatology
ORIGINAL ARTICLE
Trajectory of Assistive Device Usage and User and Non-User Characteristics: Long-Handled Bath Sponge JOAN C. ROGERS,1 MARGO B. HOLM,1
AND
LYNETTE PERKINS2
Objectives. To examine use of an assistive device, a long-handled bath sponge (LHBS) in patients with rheumatoid arthritis and osteoarthritis to describe use from the time of in-hospital prescription to the 2- and 12-month followups, and to describe the characteristics of those who became device users and non-users. Methods. Patients (n ⴝ 102) who were prescribed a LHBS during hospitalization were followed prospectively. The clinical and psychosocial assessment included disease, physical and psychosocial factors, and disability. Results. The overall usage rate for the LHBS was 86%. When compared with users, non-users had fewer arthritic joints, perceived greater control over their disability and pain, and had less favorable perceptions of the LHBS. Characteristics that did not differentiate non-users from users were sociodemographic variables, disease duration, movement capability, level of disability and pain, and general perceptions of assistive devices. Conclusion. The results support the early identification of patients who are likely to become non-users so that acceptable alternative interventions can be planned. KEY WORDS. Assistive devices; Disability; Rheumatoid arthritis; Osteoarthritis.
INTRODUCTION People with arthritis are at risk for dependence in activities of daily living secondary to pain, stiffness, joint limitations, and muscle weakness (1). Assistive devices are frequently prescribed by rehabilitation professionals to reduce dependence, ease pain, overcome joint limitations, compensate for muscle weakness, and enhance safety. Although assistive device users typically express a high level of satisfaction with assistive devices (2), usage surveys also indicate that a substantial number of assistive devices are abandoned, often shortly after they have been obtained. Little research has been conducted to distinguish patients who become device non-users from those who become device users. These data are needed so that at the point of referral, rehabilitation therapists can appropriately target patients for interventions that either increase Supported in part by a grant from the Arthritis Foundation. 1 Joan C. Rogers, PhD, Margo B. Holm, PhD: University of Pittsburgh, Pennsylvania; 2Lynette Perkins, MS: Centers for Rehabilitative Services, McKeesport, Pennsylvania. Address correspondence to Joan C. Rogers, PhD, Department of Occupational Therapy, School of Health and Rehabilitation Sciences, University of Pittsburgh, 5017 Forbes Tower, Pittsburgh, PA 15260. E-mail:
[email protected]. Submitted for publication March 6, 2001; accepted in revised form February 2, 2002.
their adherence to device prescriptions or support nondevice solutions to disability reduction. Evidence from patients with rheumatic disease suggests that when the usage rate for all prescribed devices is considered, neither age nor sex distinguishes users from non-users. However, when rates for specific devices are examined, the discard rate for bathing, dressing, and toileting aids tends to be higher for men than women (3,4), and older patients tend to make greater use of walking aids than younger patients (4). A relationship between increased disability and increased device use has also been observed (2). The overall purpose of this study was to trace an assistive device frequently prescribed for people with arthritis (5), namely a long-handled bath sponge (LHBS), and to examine device usage. The specific purposes were to describe the trajectory of LHBS usage from in-hospital prescription to 2- and 12-month followup after discharge; and to describe the demographic, disease, impairment, disability and device perception characteristics of LHBS users and non-users at 3 points in time: hospitalization, and 2and 12-month followup.
METHODS Patients. Patients were from the inpatient rheumatology service of St. Margaret Memorial Hospital, Pittsburgh, 645
646 Pennsylvania. Data were collected from 1989 to 1992 in conjunction with a prospective longitudinal study on the use of assistive devices (6). Inclusion criteria were a definitive diagnosis of rheumatoid arthritis (RA) or osteoarthritis (OA) made by a rheumatologist; prescription of an assistive device by an occupational therapist; and, ⱖ18 years of age. Exclusion criteria were surgery for other than joint-related problems; and functional disability not related to RA or OA, for example, disability secondary to stroke or visual loss. The present analysis includes only those patients who received a LHBS. Measures. Measures of disease, impairment, and disability were obtained while patients were hospitalized. A more in-depth description of these instruments has been published previously (7). In addition to RA or OA, disease duration and joint count were the disease measures. Impairment of active movement was assessed on the Keitel Functional Test (KFT) (8). The KFT consists of 24 movements of the lower and upper extremities and spinal column and yields scores ranging from 4 –100, with joint restrictions increasing as the score increases. Pain perception was assessed by visual analog scales, which were added to 7 of the daily living activities assessed on the Health Assessment Questionnaire (HAQ). No pain was indicated by 0 and very severe pain was indicated by 100. Depression was self-rated using the Center for Epidemiologic Studies Depression Scale (CES-D) (9), which consists of 20 statements of depressive symptoms. Scores range from 0 – 60, with higher scores suggestive of depressive impairment. Self-efficacy for controlling function (FSE), pain (PSE), and other arthritis symptoms (OSE) was evaluated on the respective subscales of the Perceived SelfEfficacy Scale for People with Arthritis (SE) (10). Subscale scores range from 10, indicating low certainty, to 100, indicating a high level of certainty. The HAQ (11) was used to measure self-reported disability. HAQ scoring was adapted to use the mean rating rather than the highest item score for each category as suggested by our prior research (12). The value of assistive technology devices (ATD) was assessed on 2 questionnaires specifically devised for this study: the ATD-General (17 items) which assessed perceptions about the use, acceptability, and adequacy of assistive devices in general; and the ATD-Specific (15 items) which assessed perceptions about the LHBS. Content validity of the ATD-General and ATD-Specific was based on the work of Batavia and Hammer (13), who identified factors that consumers viewed as important for evaluating assistive technology. Items on both questionnaires were scored using a 4-point ordinal scale, with 4 indicating strongly agree and 1 indicating strongly disagree. Measures of internal consistency, using Cronbach’s alpha, were 0.87 and 0.78 for the ATD-General and 0.86 and 0.89 for the ATD-Specific, at 2 and 12 months, respectively. For the ATD-General tool, test–retest reliability within 24 hours was established with 22 subjects; ICC (2,1) ⫽ 0.84, P ⬍ 0.001. For the Specific-ATD tool, test–retest reliability within 24 hours was established with 10 subjects; ICC (2,k) ⫽ 0.98, P ⬍ 0.001.
Rogers et al Procedures. During hospitalization, demographic, disease, impairment, and disability data, and the ATD-General were collected. Disease duration was obtained from the medical record and was verified by each patient. Joint count was reported by patients using a checklist of 30 possible tender joint regions, in response to the question, “Has your arthritis affected any of the following joints?” All other self-report measures were administered in a questionnaire format. The ATD-General was administered during hospitalization because the LHBS was not yet available to subjects. The KFT was administered by 1 of 2 licensed occupational therapists trained to interrater reliability of greater than 90%. At 2 and 12 months after hospitalization, usage data about the LHBS prescribed during hospitalization were collected via telephone interview. The ATD-Specific was administered to all subjects at 2 months and was readministered at 12 months to subjects using the LHBS. The ATD-General was readministered at 12 months to subjects who were not using the LHBS. Additionally, the SE and HAQ were readministered at 12 months. The telephone interviews were facilitated by mailing copies of the questions and response options to the patients prior to the telephone call. Data analysis. Device usage was described using a flow chart from prescription to the 2-month and 12-month followups. Chi-square tests were used to assess differences in the proportion of patients with RA versus OA among users and non-users. Demographic differences between device users and non-users were tested using the Z score test of proportions. Independent t-tests were used to test for differences between users and non-users on disease, impairment, disability, and perceptions of assistive device variables, and paired t-tests were used to test for changes in variables collected longitudinally (disability, self-efficacy, and perceptions of assistive devices).
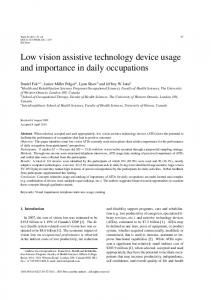
RESULTS Trajectory of assistive device use. As indicated on the flowchart (Figure 1), the majority of the subjects (72 of 102) were using the LHBS at the 2-month followup, and of those not using it at that time (n ⫽ 30), more than half (n ⫽ 16) had used it at one time. Thus, the overall usage rate was 86%. Of the 72 subjects using the LHBS at the 2-month followup, the majority (n ⫽ 52) were also using it at the 12-month followup. Of the 16 subjects who had used the LHBS at some point prior to the 2-month followup but were not using it then, 2 had reinitiated use by the 12month followup. The 13 subjects who never used the LHBS indicated that they had others help them with bathing, did not need the LHBS for bathing, or that the LHBS did not work well for them. Characteristics of device users and non-users. The characteristics of 102 in-hospital LHBS users and nonusers, and the in-hospital measures for those who became device users and non-users at 2 months and 12 months are
Characteristics of Assistive Device Users vs. Non-users
Figure 1. Flow chart of the trajectory of use and non-use of the long-handled bath sponge. *Total differences due to missing data.
presented in Table 1. The total sample (n ⫽ 102) was predominantly Caucasian (93.1%), female (79.4%), and had a mean age of 64.6 years. Approximately half (52%) were married and had at least a high school education (59.7%). A minority (36.3%) lived alone. There were no demographic differences between patients who became device users and those who were non-users. The majority of the sample had RA (60.8%) and were hospitalized for disease exacerbation (50.0%), rather than for surgery (10.8%) (Table 1). There was no significant difference in the proportion of RA surgical and OA surgical patients who became users or non-users at 2 months (users, 2 ⫽ 2.58, 1 df, P ⫽ 0.11; non-users, 2 ⫽ 0.09, 1 df, P ⫽ 0.76), or 12 months (users, 2 ⫽ 1.90, 1 df, P ⫽ 0.16; non-users, 2 ⫽ 0.53, 1 df, P ⫽ 0.47). However, in the nonsurgical patient groups, a significantly greater proportion of the RA patients became both users and non-users of the LHBS than the OA patients at 2 months (users, 2 ⫽ 8.32, 1 df, P ⬍ 0.01; non-users, 2 ⫽ 4.26, 1 df, P ⬍ 0.05) or 12 months (users, 2 ⫽ 5.48, 1 df, P ⬍ 0.05; non-users, 2 ⫽ 7.25, 1 df, P ⬍ 0.01). The mean duration of the arthritis diagnosis was 15.3 years and the mean number of involved joints of 30 possible joints was 17 joints. One patient was lost to attrition at the 12-month followup. At 2 and 12 months, users were distinguished from non-users in having a greater number of arthritic joints. Patients having more than the sample mean number of joints involved (mean ⫽ 17) during hospitalization were more prone to use the LHBS than those who had fewer than the mean number of joints involved. Patients with RA identified a significantly greater number of involved joints (t ⫽ 4.9, 1 df, P ⬍ 0.0001) than those with OA. Significantly greater proportions of patients with greater numbers of involved joints in the upper extremities (Z ⫽ 5.56, P ⬍ 0.05), and the lower extremities (Z ⫽ 5.23, P ⬍ 0.05) were still using the LHBS at the 2-month followup, compared to those not using it. No significant differences were found at 12 months. In terms of impairments, users and non-users were not distinguishable in movement capability, pain, depression, or perceived self-efficacy for other situations (See Table 1, in-hospital impairment variables). However, based on the
647 KFT, significantly greater proportions of patients with overall lower extremity movement restrictions (Z ⫽ 3.87, P ⬍ 0.05), used the LHBS at the 2 month followup, compared with those with few lower extremity restrictions. There were no significant differences at 12 months. The hospital admission self-efficacy for function scores, differentiated between users and non-users at the 2- and 12-month assessments, and the hospital admission selfefficacy for pain score differentiated between them at 12 months. Non-users continued to report significantly greater self-efficacy for function and pain at the 12-month followup. Hence, patients who became non-users tended to perceive that they had better control of their disability and pain than those who became users. Comparison of the in-hospital and 12-month self-efficacy scores for those who were device users and non-users at the 12-month assessment, evidenced no significant change (See Table 1, in-hospital and 12-month followup, impairment variables). Neither the total HAQ disability score nor the HAQ bathing item score distinguished device users from nonusers at either time point (See Table 1 in-hospital, disability variables). Thus, patients who became users did not differ from those who became non-users in overall or bathing-specific disability. However, the HAQ disability (1.30 – 0.85; P ⱕ 0.01) and bathing item (1.27– 0.77; P ⱕ 0.05) scores for non-device users indicated decreased disability between hospitalization and the 12-month testing, unlike the users who evidenced significant functional improvement only on the overall HAQ disability score (1.10 – 0.95; P ⱕ 0.05) (see Table 1, in-hospital and 12-month followup, disability variables). As assessed on the ATD-General, all patients highly endorsed assistive devices as useful; hence, users and non-users did not differ in their overall perceptions of assistive devices (See Table 1, in-hospital, ATD-General). The device perceptions of non-users did not change from hospitalization to 12-month followup (see Table 1, 12 month followup, ATD-General). When asked about the LHBS at the 2-month followup, the perceptions of users were significantly more positive than those of non-users (see Table 2). Specifically, users expressed more positive perceptions of the LHBS regarding ease of use, replacing the device if it were broken, its potential for both increasing and achieving functional independence, and its capability for increasing safety during bathing. User perceptions of the LHBS did not change from the 2- to the 12month assessment (See Table 1, followup: 2 and 12 months, ATD-Specific).
DISCUSSION Independence in bathing is important for maintaining independent living in the community. Ergonomic studies indicate that reaching to bathe the back and feet often challenge the movement capabilities of adults with disabilities (14,15). Thus, it is not surprising that a device that compensates for reductions in reach, a LHBS, was the most frequently prescribed device in our study of adults with RA and OA, and that when prescribed it was generally
648
Rogers et al
Table 1. Device user and non-user characteristics In-Hospital (n ⴝ 102) In-hospital Demographic variables (based on in-hospital measure) Age, years (mean) White, % Female, % Living alone, % Married, % Education level ⬍12 years, % 12 years, % ⬎12 years, % Disease variables (based on in-hospital measure) RA, nonsurgical admission, n (%) RA, surgical admission, n (%) OA, nonsurgical admission, n (%) OA, surgical admission, n (%) Number of years diagnosed, mean Number of joints involved/30, mean Impairment variables (based on in-hospital measure) Keitel Functional Test, mean Pain visual analog scale, mean Self-efficacy pain Self-efficacy function, mean Self-efficacy other, mean CES-D, mean Disability variables (based on in-hospital measure) HAQ—(adapted version), mean HAQ—(adapted version), Bathing Item, mean ATD-General (in-hospital measure) 2 month followup ATD-Specific (LHBS), mean 12 month followup Impairment variables Self-efficacy pain, mean Self-efficacy function, mean Self-efficacy other, mean Disability variables HAQ—(adapted version), mean HAQ—(adapted version), bathing item, mean ATD-General, mean ATD-Specific (LHBS), mean
Users 2 months (n ⴝ 72)
Non-Users 2 months (n ⴝ 30)
Users 12 months (n ⴝ 54)
Non-Users 12 months (n ⴝ 48)
64.6 93.1 79.4 36.3 52.0
63.8 90.3 81.9 36.1 50.0
66.5 100.0 73.3 36.7 56.7
65.0 88.9 79.6 35.2 48.1
64.1 97.9 79.2 37.5 56.3
40.2 33.3 26.4
41.7 33.3 25.0
36.6 33.3 30.0
46.3 33.3 20.5
33.3 33.3 33.4
51 (50.0) 11 (10.8) 21 (20.6) 19 (18.6) 15.3 17.0
37 (51.4)† 6 (8.3)§ 16 (22.2)† 13 (18.1)§ 14.7 18.2
14 (46.7)‡ 5 (16.7)§ 5 (16.7)‡ 6 (20.0)§ 16.7 14.0¶
28 (51.9)‡ 4 (7.4)§ 13 (24.1)‡ 9 (16.7)§ 15.5 19.0
23 (47.9)† 7 (16.7)§ 8 (14.6)† 10 (20.8)§ 15.1 14.8¶
36.5 12.6 55.9 51.6 61.3 15.3
35.6 12.3 55.5 48.8 59.0 14.3
38.7 13.5 57.0 58.4¶ 66.8 17.8
36.43 12.4 52.3 47.1 59.6 14.6
36.6 12.8 60.0¶ 56.7¶ 63.2 16.1
1.10 0.92 3.0
1.20 1.17 3.0
1.10 0.93 3.0
1.20 1.06 3.0
2.8
2.6**
1.14 3.0
54.2 49.8 62.7 0.93 0.70
59.6¶ 61.2¶ 64.3 0.85 0.77 2.8
2.7
* RA ⫽ rheumatoid arthritis; OA ⫽ osteoarthritis; CES-D ⫽ Center for Epidemiologic Studies Depression Scale; HAQ ⫽ Health Assessment Questionnaire; ATD ⫽ assistive technology device; LHBS ⫽ long-handled bath sponge † P ⬍ 0.01 for comparisons between nonsurgical patients with OA versus RA. ‡ P ⬍ 0.05 for comparisons between nonsurgical patients with OA versus RA. § No significant differences among surgical patients with OA versus RA. ¶ P ⬍ 0.05 for comparison group in same time period. ** P ⬍ 0.01 for comparison group in same time period.
used. Our 86% usage rate for the LHBS is consistent with (16) or exceeds (17) that reported in other studies. Nevertheless, of the 29% of our patients who were not using the LHBS at 2 months after it was prescribed, 13% had never used it. The non-users and discarders are of particular interest because their abandonment of the LHBS has implications for device prescription. If potential nonusers can be identified early in the rehabilitative process, their intervention can be focused on improving adherence to device usage or redirected to meeting their functional
needs without devices. Hence, having identified device users and non-users at the 2- and 12-month assessments, we analyzed their disease, impairment, and disability characteristics during hospitalization to ascertain surrogate markers that could be used at the time of device prescription to identify patients likely to become nonusers. Our findings suggest that during hospitalization, patients who had less than 17 joints involved and scored greater than 55.9 and 51.6 in perceived self-efficacy for function and pain, respectively, were more likely to be-
Characteristics of Assistive Device Users vs. Non-users
Table 2. Mean item scores on ATD-specific for longhandled bath sponge users and non-users at 2-month followup* Item 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15.
Easy to use Like appearance Comfortable to use Easy to maintain Hard to store§ Fear of getting hurt when using aid§ Replace aid Recommend to friend Met expectations Helped to bathe independently Increased bathing independence Made bathing easier Made bathing safer Use resulted in needing less help Use resulted in needing more help§
Users 2 months
Non-users 2 months
3.04 3.04 3.07 3.03 2.04 1.96
2.72† 2.95 2.83 3.00 2.11 2.00
2.92 2.97 2.93 2.94
2.47‡ 2.89 2.72 2.61†
2.93
2.61†
3.01 2.94 2.94
2.72 2.56‡ 2.83
2.03
2.00
* Rating scale: 4 ⫽ Strongly agree; 1 ⫽ Strongly disagree. † P ⱕ 0.05. ‡ P ⱕ 0.01. § Item scored in reverse.
come non-users than users. Furthermore, after patients had the opportunity to use the LHBS at home, we ascertained that compared to users, non-users had less favorable perceptions of it. Thus, patients who had less pervasive disease, were moderately confident that they could perform critical functional tasks as well as control their function and pain, and held more negative impressions of the LHBS, were more likely to become non-users. Overall, our findings suggest that disease pervasiveness and psychological factors related to self-efficacy and device perceptions may outweigh sociodemographic, disease duration, movement, pain, depression, and disability factors in portending device acceptance or rejection. Although the role of psychological factors as determinants of device usage has been recognized (18,19), few studies have systematically examined this relationship. Our finding that confidence in one’s ability to perform daily living tasks and to control pain differentiated our non-users from users, although their levels of disability and actual pain did not, supports the salience of psychological factors for fostering device usage. This sense of the self as being in control may have translated into a desire to carry out bathing in a “normal” or “usual” adult manner, with a reduced reliance on the compensatory aid. Further support for the salience of psychological factors in device usage is gleaned from our findings concerning device perceptions. Non-users had less favorable perceptions of the LHBS than users, but both groups had similar and generally favorable perceptions about assistive devices in general. Thus, it was perceptions of the specific device rather than perceptions of devices in general that
649 influenced use. The advantage of the specific device data is understandable not only because device features, such as appearance, ease of use, and comfort, can differ from device to device, but also because device features interact with user characteristics to facilitate functional outcomes, such as task independence and safety. Of critical concern is the fact that several items that differentiated non-users from users involved the rehabilitative goals for which the LHBS was prescribed. Thus, our non-users failed to see the device as a means of enhancing either their independence or safety in bathing. From the dependence perspective, non-users expressed a preference for personal assistance over equipment, although from the independence perspective, they indicated that their functional ability precluded the need for the device. These findings suggest that at the time of device prescription, greater attention should be directed toward educating patients and their caregivers about the rehabilitative purposes of the device while simultaneously appreciating patients’ preferences for resolving problems in daily living functioning through assistive technology, personal assistance, or a combination of equipment and personal assistance. Our data also suggest that over time, patients’ need for a device may change. Although there was an overall improvement in functional status for users and non-users, the reduction of bathing disability was confined to the nonusers. Thus, their abandonment of the bathing aid may be related to the improved function that they experienced in the year following their hospitalization. The discard of assistive devices that are needed temporarily should not be regarded as reflecting an inappropriate device prescription. Among the patient characteristics that are readily available to health professionals during hospitalization that did not differentiate non-users from users were the sociodemographic variables—age, sex, education, marital status, and living arrangements. Our negative findings are consistent with those of other researchers in regard to age (4) and sex (4,17,20), but they conflict with the evidence on living arrangements (18), and education (19). The strongest evidence linking demographic characteristics with device usage comes from population-based studies (21–24). Despite a lack of total agreement, these studies support the following: increased usage with increased age, a difference in usage by device and sex, preferences for help from equipment versus people by sex, and living alone as fostering greater usage. In light of these results and the scarcity of research on demographics and device usage in clinical studies, and because demographic data are available to health professionals when devices are prescribed, further research on demographics and devices is warranted. Our findings should be interpreted in the light of several limitations. First, the study was conducted at only one acute care hospital with data collection taking place before significant managed care penetration. The practice patterns of the referring physicians may be dissimilar to those of other physicians and managed care may now restrict access to the LHBS. Second, we confined our analyses to only one assistive device, albeit one commonly recommended. Once prescribed, the LHBS was immediately available to patients at discharge. Third, our sample was
650 predominately female with disability secondary to RA, and although hospitalized, the overall level of disability was minimal to moderate. Consequently, our findings cannot be generalized to patients seen in other settings, those prescribed other assistive devices, those using other procurement mechanisms, and those with more extensive disability. Despite these limitations, the study represents a significant nascent attempt to identify potential device nonusers so that appropriate rehabilitative interventions can be initiated. Further research is needed to clarify the demographic, personal, and environmental characteristics of assistive device users and nonusers.
ACKNOWLEDGMENTS The authors thank the occupational therapy practitioners at St. Margaret Memorial Hospital, Pittsburgh, PA, for participating in this study, especially Jill Noaker Lucke, OTR/L and Louise L. Stofko, COTA.
Rogers et al
10.
11.
12.
13.
14. 15. 16.
17.
REFERENCES 1. Yelin E, Katz PP. Transitions in health status among community-dwelling elderly people with arthritis: a national, longitudinal study. Arthritis Rheum 1990;33:1205–15. 2. Mann WC, Hurren D, Tomita M. Assistive devices used by home-based elderly persons with arthritis. Am J Occup Ther 1995;49:810 –20. 3. Haworth RJ. Use of aids during the first three months after total hip replacement. Br J Rheumatol 1983;22:29 –35. 4. Haworth RJ, Hopkins J. Use of aids following total hip replacement. Br J Occup Ther 1980;43:398 – 400. 5. Stowe J, Chamberlain MA. Aids for arthritics. Br J Occup Ther 1980;43:80 – 4. 6. Rogers JC, Poole JL, Holm MB, Kwoh CK, Stofko LL. Assistive devices: prescription, patient education, patient perceptions. Arthritis Care Res 1989;2:S11. 7. Holm MB, Rogers JC, Kwoh CK. Predictors of functional disability in patients with rheumatoid arthritis. Arthritis Care Res 1998;11:346 –55. 8. Eberl DR, Fasching V, Rahlfs V, Schleyer I, Wolf R. Repeatability and objectivity of various measurements in rheumatoid arthritis: a comparative study. Arthritis Rheum 1976;10: 1278 – 86. 9. Radloff LS. The CES-D scale: a self-report depression scale for
18. 19.
20. 21.
22.
23.
24.
research in the general population. Appl Psychol Meas 1977; 1:385– 401. Lorig K, Chastain RL, Ung E, Shoor S, Holman HR. Development and evaluation of a scale to measure perceived selfefficacy in people with arthritis. Arthritis Rheum 1989;32:37– 44. Fries JF, Spitz P, Young DY. The dimensions of health outcomes: the Health Assessment Questionnaire, disability, and pain scales. J Rheumatol 1982;9:789 –93. Tomlin GS, Holm MB, Rogers JC, Kwoh CK. Comparison of standard and alternative Health Assessment Questionnaire scoring procedures for documenting outcomes in patients with rheumatoid arthritis. J Rheumatol 1996;23:1524 –30. Batavia AI, Hammer GS. Toward the development of consumer-based criteria for the evaluation of assistive devices. J Rehabil Res Dev 1990;27:425–36. Parker MG, Thorslund M. The use of technical aids among community-based elderly. Am J Occup Ther 1991;45:712– 8. Mitchell J. User requirements and hygienic equipment. Ergonomics 1981;24:871– 88. Seeger MS, Fisher LA. Adaptive equipment used in the rehabilitation of hip arthroplasty patients. Am J Occup Ther 1982; 36:503– 8. Geiger CM. The utilization of assistive devices by patients discharged from an acute rehabilitation setting. Phys Occup Ther Geriatrics 1990;9:3–25. Gitlin LN. Why older people accept or reject assistive technology. Generations 1995;19:41– 66. Rogers JC, Holm MB. Assistive technology device use in patients with rheumatic disease: a literature review. Am J Occup Ther 1992;46:120 –7. Zimmer A, Chappell NL. Mobility restrictions and the use of devices among seniors. J Aging Health 1994;6:185–208. Manton KG, Corder L, Stallard E. Changes in the use of personal assistance and special equipment from 1982 to 1989: results from the 1982 and 1989 NLTCS. Gerontologist 1993; 33:168 –76. Verbrugge LM, Rennert C, Madans JH. The great efficacy of personal and equipment assistance in reducing disability. Am J Public Health 1997;87:384 –92. Edwards NI, Jones DA. Ownership and use of assistive devices amongst older people in the community. Age Ageing 1998;27:463– 8. Norburn JEK, Bernard SL, Konrad TR, Woomert A, DeFriese GH, Kalsbeek WD, et al. Self-care and assistance from others in coping with functional status limitations among a national sample of older adults. J Gerontol B Psychol Sci Soc Sci 1995;50:S101–9.