tween familial adenomatous polyposis (FAP) and PTC. Moreover, some authors postulate the existence of familial PTC as a distinct entity. Evidence for this is ...
0021-972X/97/$03.00/0 Journal of Clinical Endocrinology and Metabolism Copyright © 1997 by The Endocrine Society
Vol. 82, No. 2 Printed in U.S.A.
Two Families with an Autosomal Dominant Inheritance Pattern for Papillary Carcinoma of the Thyroid J. R. BURGESS, A. DUFFIELD, S. J WILKINSON, R. WARE, T. M. GREENAWAY, J. PERCIVAL, AND L. HOFFMAN Department of Diabetes and Endocrine Services (J.R.B., A.D., T.M.G., L.H.) Royal Hobart Hospital, Department of Nuclear Medicine (R. W.), Royal Hobart Hospital; General Practitioner (J.P.); Department of Surgery (S.J.W.), University of Tasmania, Hobart, Tasmania ABSTRACT Background: Papillary carcinoma of the thyroid (PTC) is the most prevalent malignancy of the thyroid gland. Although the majority of lesions are sporadic tumors, an established relationship exists between familial adenomatous polyposis (FAP) and PTC. Moreover, some authors postulate the existence of familial PTC as a distinct entity. Evidence for this is limited, however, there being few well characterized descriptions of pedigrees with high prevalence of PTC. Aims: The objective of the present study was to examine an apparent heritable predisposition to PTC occurring in two Tasmanian families in which PTC occurs commonly.
Methods: Pedigree charts were constructed for both families and the medical records of the members reviewed. Results: In Pedigree I, 7 of 25 members had PTC (6 of these had coexisting multinodular goiter (MNG), and 11 others had MNG. In Pedigree II, identical male twins and their daughters had PTC. Conclusions: In both families there is evidence of autosomal dominant inheritance of PTC. The association of PTC with MNG suggests a possible role for MNG in tumor pathogenesis in hereditary PTC. The majority of the patients were diagnosed with PTC before commencement of prospective screening, indicating clinically relevant disease in the families described. (J Clin Endocrinol Metab 82: 345–348, 1997)
P
Patients and Methods
APILLARY CARCINOMA of the thyroid (PTC) is detectable in approximately 9% of the general population at autopsy (1, 2). Antemortem, an annual incidence rate for thyroid carcinoma between 0.9 –5.2 per 100,000 of population has been reported, PTC accounting for over 85% of the lesions (3). Studies assessing the prevalence of familial forms of PTC indicate that 3.5– 6.2% of patients with PTC have one or more first degree relatives with thyroid carcinoma (4 – 6). An association is known to exist between familial adenomatous polyposis (FAP) and PTC (3, 7, 8); however, a number of reports identify clearly families in which PTC occurs as a distinct entity, unrelated to FAP (4 – 6, 9, 10). The majority of such kindreds, however, contain fewer than 4 family members affected by PTC. It is possible that environmental factors or random association may explain the occurrence of PTC in a proportion of these families. Some authors have postulated an autosomal dominant basis for familial PTC; however, the exact mode of inheritance remains obscure (4, 5, 9). Stoffer et al.(4) noted an increased occurrence of nonmalignant thyroid disease in some families with PTC, but the relationship between benign thyroid disease and the subsequent development of malignant papillary lesions was unclear. We report two unrelated Tasmanian kindred in which PTC occurs commonly.
The details of two unrelated families attending a consultant endocrinologist for management of PTC were obtained. Where available, the results of isotope imaging and thyroid histopathology of tissue from fine needle aspiration (FNA) or surgery have been reviewed. A firm diagnosis of PTC was made in those patients having characteristic histopathology. The diagnosis of PTC was considered probable in two deceased individuals in whom pathological confirmation was not available to corroborate an historical diagnosis. In these cases, the history of thyroid surgery and a diagnosis of PTC was provided by a medical practitioner.
Results Pedigree I
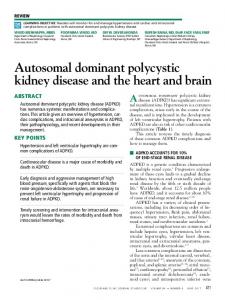
A 62-yr-old female presented with a hoarse voice. A multinodular goiter (MNG) had been noted 2 yr previously. On examination, left vocal cord paralysis and a hard, left sided neck mass were detected. Neck exploration demonstrated locally invasive papillary carcinoma of the thyroid. The patient was treated with total thyroidectomy and 6000 MBq of radio iodine. No evidence of abnormal 131I uptake was noted on post-ablative whole body scans. Abnormal areas of thallium uptake in the neck and chest were noted, becoming less prominent on consecutive scans. She remains well. Three of the patient’s six children presented with MNG in the ensuing six months (Patients M, N, and P, Fig. 1) and underwent surgical resection. Surgical management was undertaken because of mild compressive symptoms, a low thyrotropin level (indicating unsuitability for thyroxine suppression), and patient anxiety. One patient had FNA of the thyroid preoperatively that was nondiagnostic. PTC was detected during pathological examination in all cases, one microscopic, one 10 mm in diameter, and the other multifocal PTC. On screening, one of the patient’s six children (Patient
Received August 12, 1996. Revision received November 12, 1996. Accepted November 19, 1996. Address correspondence and requests for reprints to: L. Hoffman, M.D., F.R.A.C.P., Consultant Endocrinologist, Department of Diabetes and Endocrine Services, Royal Hobart Hospital, GPO Box 1061L, Tasmania, Australia 7001.
345
346
BURGESS ET AL.
JCE & M • 1997 Vol 82 • No 2
thyroidectomy, ablative radio iodine, and thyroxine suppression. The 22-yr-old daughter of the other twin (Patient L) had a MNG on screening, and a sclerosing papillary microcarcinoma was found on resection. There has been no evidence of recurrence in any of these family members. The family tree for Pedigree II is also summarized in Fig. 1. The characteristics of surgically treated thyroid disease from both pedigrees are summarized in Table 1. Discussion
FIG. 1. Pedigree chart for two kindreds with papillary thyroid carcinoma.
O) had a solitary nodule confirmed as PTC on excision. Screening other family members yielded two further relatives with MNG who had multifocal PTC (Patients U and W). Patient U had neoplasia suggested on preoperative FNA. Other relatives with abnormal thyroid glands on screening are shown in Fig. 1. The family history revealed two additional relatives who had probable thyroid carcinoma (patients B and D). Both had thyroidectomies in their 50’s (before 1950) and were reported by relatives and medical practitioners to have thyroid cancer; however, histological confirmation was not possible. There was no family history of colonic malignancy or intestinal polyposis and no history of radiation exposure. Pedigree II
A 49-yr-old male presented with a 3-week history of leftsided neck swelling. Examination revealed a 1.5 cm mass palpable in the left lobe of the thyroid gland. The patient’s family history was unremarkable for thyroid or bowel malignancy, and there was no history of radiation exposure. Following ultrasound and isotope imaging (Fig. 1), the patient underwent hemithyroidectomy, and histopathological examination revealed papillary carcinoma. Total thyroidectomy was subsequently performed, and the patient received a 6000 MBq dose of radio iodine. Follow-up studies to 3 yr have not demonstrated disease recurrence. One year subsequent to presentation of the index case, the patient’s monozygotic twin brother presented with a neck mass, assessment of which also revealed PTC, metastatic to a cervical lymph node. In 1995, the 23-yr-old daughter (Patient K) of the index case presented with a right sided thyroid mass, subsequently proven to be an invasive 12 mm PTC. She was treated by total
In this report we describe two kindred with a high prevalence of PTC. In both families, history and physical examination consistent with FAP or Cowden’s syndrome was absent. In Pedigree I, 18 of 25 members had either PTC, multinodular goiter, or both. Although Pedigree II is less extensive, the development of PTC in monozygotic twins (within one year of each other) and in 2 of their offspring suggests an underlying genetic predisposition to thyroid neoplasia. The fact that both parents and a grandparent of the twins lived to an advanced age without evidence of thyroid cancer suggests the possibility of a de novo mutation occurring early in the twins embryogenesis. Although a family history of thyroid cancer has been reported in up to 6.2% of patients presenting with PTC, the pedigrees in these reports are small, and a clear inheritance pattern is absent. Pedigree I represents one of the largest kindred with non-FAP familial PTC described thus far. The kindred exhibits an autosomal dominant pattern of PTC occurrence and a strong association with multinodular goiter. Historically, Tasmania is recognized as having a high prevalence of endemic goiter secondary to iodine deficiency (11). However, the prevalence of goiter in this population had fallen to less than 10% by 1975, following the introduction of public health measures that have rendered the community iodine replete (12). Thus, on the basis of this prevalence data the proportion of family members in Pedigree I with MNG is high. An association may exist between iodine deficiency, multinodular goiter, and thyroid malignancy. However such an association is weak at best: a recent study detected PTC in only 2.2% of patients undergoing thyroidectomy for MNG (13). If a link between iodine deficiency and thyroid neoplasia does exist, it is unlikely to explain our observations, as the prevalence of follicular, rather than papillary, neoplasia is increased in this circumstance (3). It is possible that in this kindred MNG is a heritable condition, acting as a precursor to malignant disease. Existing evidence supports this contention, as thyroid malignancy is thought to be a multistep process. Furthermore, common genetic factors have been implicated in the pathogenesis of both MNG and PTC (9). Among several possible oncogenes, the PTC/RET oncogene is a model a and putative candidate for the development of PTC in the families we describe (14, 15). Activating rearrangements of this oncogene have been identified in tissue from MNG and PTC, while they are typically absent in other neoplasms. Transgenic mice carrying the RET/PTC oncogene develop bilateral thyroid carcinoma with cellular features comparable to human PTC (15). Mutations of the RET proto-oncogene predispose to the development of multiple
FAMILIAL PAPILLARY CANCER OF THE THYROID
347
TABLE 1. Thyroid gland characteristics in patients treated by thyroidectomy Age
Ultrasonographic characteristics
I (G)
Patient (code)
43
I (K)
62
I (L)
34
I (M)
35
Enlarged gland, heterogenous, consistent with MNG Enlarged nodular gland, consistent with MNG 3 3 2.2 cm solitary solid nodule, left lobe enlarged Multiple solid and cystic nodules, consistent with MNG
I (N) I (O) I (P)
24 42 39
Enlarged gland, 4 nodules Solid nodule Consistent with MNG
I I I I
(T) (T1) (T2) (U)
58 29 26 54
I (V) I (W) I (Z) II (G)
32 23 27 51
MNG MNG 2 thyroid nodules, largest 2 cm 2 thyroid nodules; left lobes; atypical cells on FNA 2 nodules left lobe Multiple nodules, 2–5 mm MNG Right lobe enlarged and homogenous, left enlarged; MNG, largest nodule 2 cm
II (H)
49
II (K)
23
II (L)
22
Enlarged gland; nodular left lobe containing a 20 mm solid nodule Normal sized gland containing a 10 mm and 2 mm nodule Lesions in upper left lobe and heterogeneous texture lower pole right lobe
Characteristics on isotope imaging
large MNG, no dominant nodule cold nodule in otherwise normal gland MNG; overall uptake increased; dominant nodule with cold areas MNG; overall uptake increased; no dominant cold nodule
large cold area left lobe; generalized patchy uptake patchy tracer uptake consistent with MNG
Thyroid histopathology
MNG with lymphocytic thyroiditis. No evidence of malignancy follicular variant of PTC occurring in a MNG MNG with benign dominant nodule sclerosing PTC occurring in a MNG Multifocal PTC PTC sclerosing PTC occurring in a MNG; background of lymphocytic thyroiditis early MNG MNG MNG with lymphocytic thyroiditis early MNG with multifocal PTC containing follicular variants early MNG MNG, multifocal PTC in left lobe MNG well differentiated PTC metastatic to cervical lymph node; solitary follicular adenoma in thyroid gland PTC containing follicular elements
solitary cold nodule
PTC containing follicular elements
normal sized gland, areas of marked decrease in uptake
sclerosing papillary microcarcinoma
endocrine neoplasia type II and the associated medullary thyroid carcinoma (16). Tissue samples from several patients will be analyzed for activating RET mutations. Incomplete penetrance of familial PTC may explain both the obligatory carrier status of patient C in Pedigree I and nonexpression of clinically overt thyroid disease. The influence of secondary modifying factors, such as gender, may explain this observation as in pedigree I, where six of seven patients with PTC are female. This observation is similar to that of Lote et al.(9), who described a female predilection for PTC in a Norwegian family. Both families included individuals with multifocal PTC occurring at a young age, consistent with other reports of familial PTC (17). All patients to date appear to be cured, except for a small focus of thallium uptake in patient I(K), however the follow-up time is less than 4 yr. The optimal strategy for investigation and management of kindred with PTC is unclear. Exclusion of occult FAP would seem prudent, however in the absence of a family history of bowel malignancy, or characteristic physical stigmata of Gardner’s syndrome, routine colonic assessment would seem unwarranted. The possible high risk of PTC developing in an underlying MNG, and the limited value of ultrasonography, isotope scanning, and FNA in excluding malignancy in this setting, argue strongly for thyroidectomy in family members of Pedigrees I and II who have evidence of MNG. The screening strategy recommended for these families is annual thyroid ultrasonography and neck palpation by an
experienced examiner. Patients with evidence of goiter may then be counselled regarding the potential risk of malignancy and offered the option of early thyroidectomy. Conclusions
The kindred described herein support the existence of an autosomal dominant inheritance pattern for papillary carcinoma of the thyroid, separate from the established association with familial adenomatous polyposis. Although the molecular mechanisms and pathogenesis of PTC in the families we describe are unknown, a strong association with multinodular goiter, and possibly with female gender, is evident. The optimal screening and management protocol for asymptomatic family members is unclear. However, regular and lifelong screening is advisable. Early consideration of total thyroidectomy should be given for patients with evidence of multinodular goiter. Acknowledgments The authors gratefully acknowledge the details of medical and surgical management provided by Mr. D. Merry and other medical practitioners caring for members of the kindred described herein.
References 1. Chong PY. 1994 Thyroid carcinomas in Singapore autopsies. Pathology. 26:20 –22.
348
BURGESS ET AL.
2. Furmanchuk AW, Roussak N, Ruchti C. 1993 Occult thyroid carcinomas in the region of Minsk, Belarus. An autopsy study of 215 patients. Histopathology. 23:319 –325. 3. Farid NR, Shi Y, Zou M. 1994 Molecular basis of thyroid cancer. Endocr Rev. 15:202–32. 4. Stoffer SS, Van Dyke DL, Vaden Bach J, Szpunar W, Weiss L. 1986 Familial papillary carcinoma of the thyroid. Am J Med Genet. 25:775–782. 5. Hrafnkelsson J, Tulinius H, Jonasson JG, Olafsdottir G, Sigvaldason H. 1989 Papillary thyroid carcinoma in Iceland: a study of the occurrence of families and the coexistence of other primary tumors. Acta Oncol. 28:785–788. 6. Kwok CG, McDougall IR. 1995 Familial differentiated carcinoma of the thyroid: report of five pairs of siblings. Thyroid. 5:395–397. 7. Camiel MR, Mule JE, Alexander LI, Beninghoff DL. 1968 Association of thyroid carcinoma with Gardner’s syndrome in siblings. N Engl J Med. 278:1056 –1058. 8. Case records of the Massachusetts General Hospital (Case. 50 - 1982). 1982 N Engl J Med. 307:1566 –1573. 9. Lote K, Andersen K, Nordal E, Brennhovd IO. 1980 Familial occurrence of papillary thyroid carcinoma. Cancer. 46:1291–1297.
JCE & M • 1997 Vol 82 • No 2
10. Gorson D. 1992 Familial papillary carcinoma of the thyroid. Thyroid. 2:131–132. 11. Clements FW, Gibson HB, Howeler-Coy JF. 1970 Goitre prophylaxis by addition of potassium iodate to bread. Experience in Tasmania. Lancet. 1:489 – 492. 12. Tasmanian Thyroid Advisory Committee. 1981 Study in disease surveillance, 1950 –1979. Med J Aust. 2:234 –238. 13. Mathai V, Idikula J, Fenn AS, Nair A. 1994 Do long-standing nodular goitres result in malignancies? Aust N Z J Surg. 64:180 –182. 14. Grieco M, Santoro M, Berlingieri MT, et al. 1988 Molecular cloning of PTC, a new oncogene found activated in human thyroid papillary carcinomas and their lymph node metastasis. Ann NY Acad Sci. 551:380 –381. 15. Jhiang SM, Sagartz JE, Tong Q., et al. 1996 Targeted expression of the RET/ PTC 1 oncogene induces papillary thyroid carcinoma. Endocrinology. 137:375–378. 16. Mulligan LM, Ponder BAJ. 1995 Genetic basis of endocrine disease: multiple endocrine neoplasia type 2. J Clin Endocrinol Metab. 80:1989 –1995. 17. Grossman RF, Shih-Hsin Tu, Quan-Yang Duh, et al. 1995 Familial nonmedullary thyroid cancer. Arch Surg. 130:892– 899.