Ncuropsychology 1998, Vol. 12, No. 1,134-145
Copyright 1998 by the American Psychological Association, Inc. 0894-4105/98/$3.00
Visual-Motor Integration Functioning in Children With Tourette Syndrome Robert T. Schultz, Alice S. Carter, Marshall Gladstone, Lawrence Scahill, James E Leckman, Bradley S. Peterson, Heping Zhang, Donald J. Cohen, and David Pauls Yale University A neuropsychological model of visual-motor integration skill was proposed and tested in 50 children with Tourette syndrome (TS) and 23 unaffected control children matched for age. Children with TS performed significantly worse than control children on the Beery Visual-Motor Integration (VMI) Test. Consistent with the proposed model, visuoperceptual and fine-motor coordination subprocesses were significant predictors of VMI scores. However, the subprocesses did not fully account for the diagnostic group difference on the VMI. These results suggest that the integration of visual inputs and organized motor output is a specific area of neuropsychological weakness among individuals with TS.
Tourette syndrome (TS) is a neuropsychiatric disorder of childhood onset characterized by multiple motor and one or more vocal tics that wax and wane in severity across time. Tourette syndrome and chronic tics are familial and heritable, with segregation analyses suggesting major gene transmission (e.g., Eapen, Pauls, & Robertson, 1993; Hasstedt, Leppert, Filloux, van de Wetering, & McMahon, 1995; Pauls & Leckman, 1986; Walkup et al., 1996). Although motor and phonic tics constitute the core elements of the diagnostic criteria for TS, individuals with the condition frequently have a wide array of difficulties, including problems with attention, disinhibition, and obsessive-compulsive symptoms (Cohen, Detlor, Shaywitz, & Leckman, 1982; Comings & Comings, 1985; Robertson, Trimble, & Lees, 1988). Neuropsychological studies of TS have focused on an array of functions, with the most consistently observed difficulties occurring on tests of visual-graphic and motor ability. The ability to copy designs accurately has been investigated in 10 prior studies (see Table 1). Nine of the 10 studies reported in the literature found visual-motor integration deficits (relative to other domains of functioning). For
example, Brookshire and colleagues (Brookshire, Butler, Ewing-Cobbs, & Fletcher, 1994) found that visual-motor integration scores in children and adolescents with TS were approximately 0.75 SDs below the normative mean. Six studies employed the Bender--Gestalt Test, whereas another used a highly similar measure, the Beery Visual-Motor Integration (VMI) Test. These measures demand little in the way of executive function. A more complex design, the Rey-Osterreith Complex Figure (Rey), was investigated in three prior studies. In addition to requiring the integration of visuoperceptual and fine-motor skills, the Rey requires executive function organization. Given its executive function component, it is of interest that the only study that failed to find significant impairment in TS employed the Rey. Although this literature provides consistent evidence for a relative deficit in visual-motor integration skill in TS, methodological shortcomings limit firm conclusions. Most studies to date have employed fairly small sample sizes (i.e., less than 20 participants). More important, 8 of the 10 studies failed to use a control group of any type and instead relied on normative data. Normative data are problematic because many measures are poorly normed with respect to sample size at each age interval and adequate representation of participants by region, ethnicity, socioeconomic status, and general intelligence. Moreover, normative data are usually collected only for a single test, whereas neuropsychological studies of patients typically entail an extensive battery of measures. With a long battery, fatigue and fluctuations in motivation will affect performance, especiaily in children, thus increasing the chance of spurious findings when comparisons are made to normative data. Only 1 of the 10 studies in the literature tested for comorbid attention deficit hyperactivity disorder (ADHD). This is significant because half or more of all clinic-referred cases of TS also have comorbid ADHD (Robertson et al., 1988; Walkup, Scahill, & Riddle, 1995), and children with TS and ADHD may have a different profile of cognitive abilities and worse social adjustment than children with TS alone (Dykens et al., 1990; Stokes, Bawden, Camfield,
Robert T. Schultz, Marshall Gladstone, Lawrence Scahill, and Bradley S. Peterson, Child Study Center, Yale University; Alice S. Carter and David Pauls, Child Study Center and Department of Psychology, Yale University; James E Leckman, Child Study Center and Department of Pediatrics, Yale University; Heping Zhang, Department of Epidemiology and Public Health, Yale University; Donald J. Cohen, Child Study Center and Departments of Pediatrics and Psychology, Yale University. This work was supported in part by National Institute of Mental Health Grant P01 MH49351 and the National Tourette Syndrome Association. This work would not have been possible without the help of Margot Anderson, John Hart, and Abbe Skolsky. Correspondence concerning this article should be addressed to Robert T. Schultz, Child Study Center, P.O. Box 207900, Yale University, New Haven, Connecticut 06520. Electronic mail may be sent via Internet to
[email protected]. 134
VISUAL-MOTOR INTEGRATION IN TS
135
Table 1 Visual-Motor Integration Skill
Study Lucas et al. (1967) Shapiro et al. (1974) Shapiro et al. (1978) Hagin et al. (1982) Sutherland et al. (1982) Incagnoli & Kane (1982) Ferrari et al. (1984) Randolph et al. (1993) Brookshire et al. (1994) Harris et al. (1995)
Comorbid ADHD?
Sample 15 TS 30 TS 50 TS 50 psychiatric outpatients 10 TS 32 TS 31 NC 13 TS 10 TS 12 TS 31 TS 20 non-TS siblings 10 TS - ADHD 32 TS + ADHD
Not evaluated Not evaluated Not evaluated Not evaluated Not evaluated Not evaluated Not evaluated Yes (n = 8) Not evaluated 5 "overactive" No Yes
Age (years) +- SD
11-18 22 children 28 adults 10 14.7 14.2 11.8 --- 1.1 10.8 (7-14) 10.5 (8- 16) 11.4 +--2.8 11.4 + 2.9 11.6 (8-14) 11.2 (7-14)
Test
Deficit/Group difference
Bender-Gestalt Bender-Gestalt Bender-Gestalt
Yes Yes Yes
Bender-Gestalt Rey-Osterreith
Yes Yes
Bender-Gestalt Bender--Gestsalt Rey-Osterreith VMI
Yes Yes No Yes
Rey-Osterreith Rey-Osterreith
No Yes
For studies not employing a control group, deficit was indicated if more than 20% of the sample scored at least 1.5 SD below the mean. ADHD = attention deficit hyperactivity disorder; TS = Tourette syndrome; NC = normal controls; VMI = Beery Visual-Motor Integration Test.
Note.
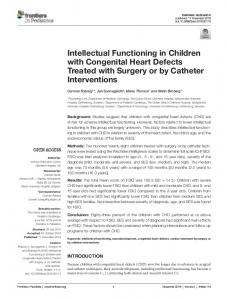
Backman, & Dooley, 1991). Moreover, children with ADHD alone show deficits in visual-motor integration and motor coordination compared to unaffected controls (Campbell & Werry, 1986; Frost, Moffitt, & McGee, 1989), indicating that it might be the ADHD component and not TS per se that is responsible for observed deficits in drawing ability. In addition, previous studies have not examined the influence of depressive symptoms on visual-motor integration, even though depression is believed to have a deleterious effect on nonverbal functions. Tests of visual-motor integration are compound measures, calling upon visual-perceptual ability and fine-motor coordination, in addition to the integration of visualperceptual analyses into motor programs for successful performance (see Figure 1). Deficient visual-motor integration could be a function of suboptimal capacity in one or both of these component processes. An important issue, therefore, is whether individuals with TS have difficulty in these more rudimentary component processes that could explain their visual-motor integration performance, or whether the deficit is specific to the integration of visual and motor processes. In addition to separate visual and finemotor processes, performance on tests of visual-motor integration also requires intact sustained attention and motor impulse control. Vigilance and motor inhibition are the two pillars of attentional ability (Barkley, 1990). Effortful maintenance of attention is a prerequisite for adequate performance on any test. Motor inhibition can be distinguished
Visual ~ineMotorCoordination)
~
(SustainedAttelation)
~ Motorlnhibition)
Component processes contributing to visual-motor integration skill.
Figure 1.
from fine-motor coordination during a copying task in that the latter refers to the continuous coordination of the small-muscle groups employed during a skilled pencil movement, whereas motor inhibition refers to both the cessation of activity when appropriate and the delayed onset of activity so as to allow for planning of the motor sequence. Thus, at least four separate subprocesses may contribute to visual-motor integration ability: visual-perceptual processes, fine-motor coordination, sustained attention, and inhibitory motor processes. Although motor, attention, and visuoperceptual skills have been examined in several prior studies of TS, analyses have not focused on their relationship to visual-motor integration ability. Table 2 presents results from all studies that employed tests of motor speed (i.e., Finger Tapping) and motor coordination (i.e., the Grooved or Purdue Pegboard). Each of the six studies produced evidence suggestive of motor skill difficulties, although some questions about laterality remain. Pegboard tests involve visually guided movement and are dependent on adequate somatosensory ability, but they are primarily measures of relatively complex motor sequencing and dexterity, requiring fine manipulation by the fingers and quick, accurate, and coordinated arm and shoulder movements. Simple motor speed without visual-perceptual or somatosensory demands, as indexed by the Finger Tapping test, appears unimpaired in samples of subjects with TS (Bomstein, 1990; Bornstein, 1991; Bornstein, Baker, Bazylewich & Douglass, 1991; Randolph, Hyde, Gold, Goldberg, & Weinberger, 1993), suggesting that deficits in elementary motor skill cannot explain the deficits on the pegboard tests. Thus, the relative motor deficits in TS seem to be at a level "downstream" from simple motor speed, involving more complex coordination of movements in space. Moreover, the suggestion is that motor coordination may account for a significant portion of visual-motor integration variance, but this has been untested until now.
136
SCHULTZ ET AL.
Table 2 Fine-Motor Skill Study
Sample
Comorbid ADI-ID?
Age (years) + SD
Hagin et al. (1982) Bomstein (1990)
10 TS 100 TS
Not evaluated Not evaluated
10 12.3 - 3.3
Bornstein et al. (1991)
28 TS
No
11.4 - 3.9
Bornstein (1991)
36 TS 15 NC 12 TS + ADHD
Not evaluated Yes (n = 8)
32.5 + 11.4 31.1 --+ 9.9 10.5 (8-16)
31 TS 20 non-TS sibling 82 TSc
Not evaluated 5 "overactive" Yes (n = 36)
11.4 __-2.8 11.4 -+ 2.9 11.7 - 2.7
Randolph et al. (1993) Brookshire et al. (1994) Yeates & Bornstein (1994)
Test
Deficit/Group difference
Purdue Pegboard Grooved Pegboard Finger Tapping Grooved Pegboard Finger Tapping Grooved Pegboard Finger Tapping Purdue Pegboard Finger Tapping Grooved Pegboard
Yes Yes No Yes--Nondominant Yes--Dominant Yes--Dominant No Yesa Noa Trendb
Grooved Pegboard Finger Tapping
No TS + ADHD versus TS - ADHD differences
Note. For studies not employing a control group, deficit was indicated if more than 20% of the sample scored at least 1.5 SD below the mean. ADHD = attention deficit hyperactivity disorder; TS = Tourette syndrome; NC = normal controls. K)n the basis of our comparison of reported scores to normative data. It is not clear whether a substantial minority (i.e., 20%) scored at least 1.5 SD below the mean on the Finger Tapping test. bThechildren with TS scored 0.504).67 SD below the normative mean for the two conditions, but comparison to siblings without TS resulted in a statistical trend. The possibility of subsyndromal manifestations of the disorder in genetically related family members compromises the interpretabilityof this latter finding. CAsubset of the 100 children studied by Bornstein (1990). The literature on possible visuoperceptual deficits in TS is less clear (see Table 3), in part because the measures employed differ between studies and in part because few studies have selected instruments that are highly specific to this domain of functioning. The early literature tended to
focus on relative deficits in Wechsler Performance IQ (PIQ) compared with Verbal IQ (VIQ). Although Shapiro, Shapiro, Bruun, and Sweet (1978) and Sutherland, Kolb, Schoel, Whishaw, and Davies (1982) found significant PIQ deficits, Incagnoli and Kane (1981), Golden (1984), Ferrari, Mat-
Table 3 Visuoperceptual Ability Study
Sample
Shapiro et al. (1978)
50 TS 50 psychiatric outpatients Incagnoli & Kane (1982) 13 TS Sutherland et al. (1982) 32 TS 31 NC
Comorbid ADHD? Not evaluated
22 children VIQ > PIQ 28 adults
Not evaluated Not evaluated
11.8 - 1.1 14.7 14.2
Golden (1984) Ferrari et al. (1984)
9 TS 10 TS
Not evaluated Not evaluated
Dykens et al. (1990)
19 TS + ADHD 11 TS - ADHD
Yes No
Bornstein et al. (1991) Bomstein (1991)
28 TS 36 TS 15 NC 12 TS
No Not evaluated
Randolph et al. (1993) Lanser et al. (1993) Brookshire et al. (1994)
Age (years) +- SD
Test
VIQ > PIQ PIQ Mooney Closure R/L Differentiation Semmes 13-20 VIQ > PIQ 10.8 (7-14) Motor-Free Visual Perception Test VIQ > PIQ 10.5 (7-14) PIQ
11.4 - 3.9 VIQ > PIQ or PIQ > VIQ 32.5 ___ 11.4 PIQ 31.1 --_ 9.9 Yes (n = 8) 10.5 (8-16) Facial Recognition Block Design 16 TS No 10.4 (7-14) VIQ > PIQ 31 TS Not evaluated 11.4 --- 2.8 Judgment of Line Orientation 20 non-TS siblings 5 "overactive" 11.4 -+ 2.9
Deficit/Group difference Yes No a Yesb No No No No Yes Noc TS - ADHD Impaired relative to TS + ADHD Yesd No~ Yesf No No No (compared to sibling control)
Note. For studies not employing a control group, deficit was indicated if more than 20% of the sample scored at least 1.5 SD below the mean. ADHD = attention deficit hyperactivity disorder; TS = Tourette syndrome; VIQ = Verbal IQ; PIQ = Performance IQ; NC = normal controls; R/L = fight/left. aFour of the 13 participants had a VIQ-PIQ discrepancy of at least 15 points, bFor participants 9 years or older. CFiveof the 10 participants had a VIQ-PIQ discrepancy of at least 15 points, dFive of 28 participants had VIQ at least 12 points greater than PIQ, and 5 had the opposite, eVIQ-PIQ differences not reported, but PIQ not significantly lower than control group, tSignificantly impaired compared with less severely affected co-twin.
VISUAL-MOTOR INTEGRATION IN TS thews, and Barabas (1984), and Lanser and colleagues (Lanser, Van Santen, Jennekens-Schinkel, & Roos, 1993) did not. Dykens and colleagues (Dykens et al., 1990) found significantly lower PIQ among children with TS - A D H D as compared with TS + ADHD. Bornstein et al. (1991), on the other hand, reported greater V I Q - P I Q discrepancies in TS, regardless o f the direction. Other measures with a visuoperceptual or visuospatial component have also provided mixed results (see Table 3). The primary goal o f this study was to address the methodological shortcomings of prior work and provide a clear test o f the hypothesis that children with TS exhibit relative deficits in visual-motor integration skill as compared with a sample of age-matched, unaffected control children. Moreover, we tested the hypothesis that performance on tests o f visual-motor integration can be predicted by the four component processes (fine-motor coordination, visuoperceptual ability, motor inhibition, and sustained attention) in our model (Figure 1) and that relative deficits in v i s u a l - m o t o r integration skill can be explained by weakness in one or more component processes. A second goal of the study was to assess the role that A D H D and depressive symptoms play in visual-motor integration performance by subdividing the TS group into children with and without comorbid A D H D and by statistical control for scores on the Childhood Depression Inventory. These analyses are critical tests o f the specificity o f v i s u a l - m o t o r integration weakness in TS. Method
Participants Children with a clinical diagnosis of TS were recruited for participation from the TS specialty clinic of the Yale University Child Study Center, New Haven, Connecticut. Before entry into the study, the children's parents were interviewed and clinical records reviewed to exclude children with a history of neurological illness, loss of consciousness, or comorbid diagnoses of pervasive developmental disorder, psychosis, or mental retardation. Control children of the same age were recruited through newspaper advertisements and announcements within the university and at local area schools; they were paid $50 for their participation. Control-participant exclusion criteria included a lifetime diagnosis of any psychiatric or neurologic disorder, including head injury with loss of consciousness.
Diagnostic Process To confirm the diagnostic status of the unaffected controls and the children with a putative diagnosis of TS, we gathered multiple parent-, chiM-, teacher-, and clinician-completed ratings including the Vineland Adaptive Behavior Scales--Survey edition (Sparrow, Balla, & Cicchetti, 1984), Child Behavior Checklist (Achenbach, 1991), ADHD Rating Scale (DuPaul, 1991), Conners Parent and Teachers ADHD Rating Scales (Conners, 1989), Yale Global Tic Severity Scale (Leckman et al., 1989), Children's Yale-Brown Obsessive--Compulsive Scale (Riddle et al., 1992), Leyton Obsessional Inventory (Flament et al., 1988), Revised Children's Manifest Anxiety Scale (Reynolds & Richmond, 1987), Childhood Depression Inventory (Kovacs, 1985), review of clinical records, and a semistructured developmental history interview with a
137
parent that included screening questions for psychiatric disorders based on the Schedule for Affective Disorders and Schizophrenia for School-Age Children (Orvaschel & Puig-Antich, 1987). Principal and comorbid Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev.; DSM-III-R; American Psychiatric Association, 1987) diagnoses were then formally established with a best-estimate diagnostic procedure (Leckman, Sholomskas, Thompson, Belanger, & Weissman, 1982), which entailed two experienced clinicians (Lawrence Scahill and James E Leckman) reviewing all available information and independently judging the presence or absence of the following diagnoses: TS, chronic motor tics, chronic vocal tics, obsessive-compulsive disorder (OCD), obsessivecompulsive personality disorder, ADHD, oppositional defiant disorder, conduct disorder, and other major psychiatric disorders. In addition, each clinician counted the number of DSM-III-R ADHD diagnostic criteria that the child satisfied. Kappa statistics were computed on the three major diagnoses of interest: TS, OCD, and ADHD (.84, 1.0, and .66, respectively). Subsequently, disagreements involving the principal and secondary diagnoses, or both, were resolved by a joint review of the records by the two clinicians. The consensus diagnostic process resulted in 12 patients being dropped from the study for one of the following reasons: a failure to have a diagnosis of TS (e.g., chronic motor tics; n - - 5 ) ; the presence of Pervasive Developmental Disorder Not Otherwise Specified (PDD NOS; n = 2); IQ less than 75 (n = 1); current major depression (n = 1); history of psychosis (n = 1); syncopal induced seizures (n = 1); or insulin-dependent diabetes (n = 1), which has been associated with neuropsychological deficits. Three control children were dropped after participation in the study because of IQ less than 75 (n = 1), a significant discrepancy between their IQ and Achievement test scores suggesting the presence of a learning disability (n = 1), and significant obsessivecompulsive symptoms (n = 1). The final sample consisted of 50 children (35 boys and 15 girls) with TS between the ages of 8.1 and 14.3 years (10.8 --- 1.5). These children were compared with 23 unaffected control children (11 boys and 12 girls) between the ages of 8.2 and 13.7 years (10.8 -+ 1.8). Table 4 provides the means and standard deviations for the characteristics of the TS and control samples. There were no significant differences in age or handedness between the two groups, although there was a trend (p < .10) for more boys than girls in the TS group compared with the control group. However, gender did not affect any neuropsychological measure; there were no significant main or interaction effects of gender on any of the dependent variables. There was a trend (p < .10) for Vocabulary scores to be lower among the TS children. Children with TS scored significantly higher on the Childhood Depression Inventory compared with the unaffected controls, t(1, 69) = 3.01, p < .01. Thirty-four (68%) of the children with TS also met criteria for ADHD (26 boys and 8 girls), and 6 (12%) had comorbid OCD (3 boys and 3 girls). Comparisons among the controls, TS + ADHD, and TS - ADHD of the characteristics presented in Table 4 revealed no significant group differences in age or handedness, but there was a trend for differences in the distribution by sex, and a main effect for Vocabulary scores, F(2, 72) = 3.69, p < .05. However, none of the posthoc Scheff6 F tests of subgroup differences on Vocabulary were significant. In addition to possible comorbid OCD and ADHD, 27 of the 50 children with TS had at least one other diagnosis, 15 had at least two, 7 had at least three, and 4 had four additional diagnoses. The number of primary (i.e., TS, OCD, ADHD) and secondary diagnoses was summed to create a crude index of overall psychopathology, with the mean score of the TS sample equal to 3.04 _+ 1.34. After removing the ADHD and TS diagnoses from the count, the TS + ADHD and TS - ADHD groups were not significantly
138
SCHULTZ ET AL. Table 4
Sample Characteristics and Psychiatric Symptoms
Characteristic or symptom Sample characteristics Age (years) Men/Women Handedness (fight/left) KBIT vocabulary Psychiatric symptoms CDI YGTSS motor YGTSS phonic CYBOCS obsessions CYBOCS compulsions
TS --- ADHD (n = 50)
M
SD
10.8 1.5 35/15 40/10 106.7 9.0 9.9 12.8 9.3 1.0 1.1
8.1 3.5 5.2 3.0 2.2
TS + ADHD (n = 34)
M
SD
11.0 1.6 26/8 28/6 104.9 8.3 11.0 13.0 10.5 0.2 1.1
8.6 3.3 3.2 0.9 2.5
TS - ADHD (n = 16)
M
SD
10.4
1.4 9/7 12/4 110.6 9.2 8.2 12.5 6.7 2.3 1.1
7.1 4.1 7.6 4.5 1.7
Unaffected controls (n = 23)
M
SD
10.8 1.7 11/12 21/2 111.0 10.9 4.4
4.1 -----
Note.
Vocabulary scores are reported as standard scores; all other measures are reported as raw scores. Data are presented as group means with standard deviations except for numbers of men and women and numbers of right- and left-handed participants. Dashes indicate that unaffected controls were not assessed with the YGTSS and CYBOCS. TS = Tourette syndrome; ADHD = attention deficit hyperactivity disorder; KBIT = Kaufman Brief Intelligence Test; CDI = Childhood Depression Inventory; YGTSS = Yale Global Tic Severity Scale; CYBOCS = Children's Yale-Brown Obsessive-Compulsive Scale. different in terms of number of additional diagnoses (1.47 --- 1.11 vs. 1.13 --- 1.36).
Neuropsychological A s s e s s m e n t After informed consent, all children were administered a comprehensive neuropsychological test battery in a uniform order, across two testing sessions, each averaging about 2 hr in duration. The battery included the Kaufman Brief Intelligence Test (KBIT; Kaufman & Kanfman, 1990), composed of a Vocabulary and a Matrices subtest. The KBIT provides a reliable estimate of general intelligence that correlates greater than .80 with Full-Scale IQ scores derived from the Wechsler Intelligence Scale for Children-Revised (WlSC-R; Kaufman & Kaufman, 1990; Naugle, Chelune, & Tucker, 1993). Handedness was assessed clinically using the laterality scale of the Halstead-Reitan Battery (Reitan & Davison, 1974). Visual-motor integration was assessed with the B e e r y Buktenica Visual-Motor Integration Test (VMI; Beery, 1989) and the Rey--Osterreith Complex Figure (Osterreith, 1944; Rey, 1941), using the Taylor (1959) scoring system. The component processes depicted in Figure 1 were measured as follows: Visuoperceptual skill was assessed with two measures, the Block Design (BD) subtest of the W I S C - R and the Matrices subtest of the KBIT. Because each of these subtests load on general intelligence (g), g was controlled by having Vocabulary as a covariate in all analyses of visual-perceptual skill. Fine-motor coordination was measured with the Purdue Pegboard (Tiffen, 1968). Dominant, nondominant, and bimanual conditions were administered sequentially, with a single repetition of this sequence. The average of the two trials was taken. In addition, the number of times pegs were dropped and the number of times the child "broke set" by taking more than one pin from the well was recorded to assess whether these might influence total score. Children with TS were able to suppress tic activity during each of the timed trials of the Purdue Pegboard, and in no case did tic activity appear to directly interfere with neuropsychological test performance. Motor inhibition and sustained attention were assessed with a computer-administered continuous performance test (CPT; Loong, 1991). The CPT consisted of two conditions, each 5 min in duration. The first required the child to
press the keyboard space bar whenever the target letter X appeared on the monitor and to not respond to any other letter. During the 5 min, 100 target stimuli were randomly presented. The second condition required the child to press the space bar whenever the X followed the letter A (the AX condition). Fifty such occurrences were randomly presented during the 5 min. The number of commissions (responses to nontarget letters) constituted the measure of motor inhibition; the number of omissions (i.e., failures to detect the target) served as the measure of sustained attention.
Medication Status Accurate records on medication status for the date of testing were available for 46 of the 50 participants with TS. Twenty-seven (59%) were taking medications for treatment of their TS, OCD, or ADHD, whereas 19 (41%) were not. Two children were taking two different medications (neuroleptic and methylphenidate or clomipramine), and one child was taking three medications (neuroleptic, clomipramine, and benzotropine). The number of children taking specific medications was as follows: clonidine, 13; neuroleptic, 9 (4 taking haloperidol and 5 taking pimozide); clomipramine, 4; desipramine, 3; benzotropine, 1; and methylphenidate, 1. An analysis of variance assessed whether neuropsychological performance differed by medication status (none, clonidine, neuroleptic, or other). No significant differences emerged with the exception of nondominant hand performance on the Purdue Pegboard, F(3, 45) = 3.17, p < .05. Unfortunately, this analysis cannot disentangle cause and effect, because the reasons why a medication is prescribed or effective may in part be a function of the child's profile of neuropsychological strengths and weaknesses. Moreover, psychomotor retardation with neuroleptics is typical only after initiation of these agents or after a dosage increase, and with time there is habituation and disappearance of these unwanted side effects (Cassens, Inglis, Appelbaum, & Gutheil, 1990; King, 1990). None of the children on a neuroleptic in this study had begun the medication or had a change in dosage in the 8 weeks before testing, suggesting that these agents were not causing problems in psychomotor functioning. Moreover, analyses presented in the Results section are not changed when the 9 children on neuroleptics are excluded. This is consistent with prior studies of medication effects
VISUAL-MOTOR INTEGRATION IN TS on neuropsychological performance in TS (e.g., Bomstein & Yang, 1991).
Data Analyses The data analytic plan entailed first testing the hypothesized relationship between visual-motor integration and the four putative component processes using correlational analyses. Next, TS versus control differences in neuropsychological performance were assessed with stepwise discriminant function analyses. These analyses tested the hypothesis that visual-motor integration skill differed between participants with TS and controls, independent of performance on the component processes in the model. Subsequent analyses employed multivariate analyses of covariance (MANCOVAs), discriminant function analyses, and correlations to assess individual component processes in our neuropsychological model of visual-motor integration, the subgroupings of TS with and without comorbid ADHD, and the relationship between psychiatric symptoms and neuropsychological performance. There is a large general factor of intelligence in neuropsychological batteries, which, if not removed, would otherwise inflate correlations between putative tests of isolable functions (Matarazzo, 1990). Therefore, in all analyses, Vocabulary, as a proxy for g, was first removed from each variable by covariation, so the specificity of the relationships could be measured without the ubiquitous influence of general intelligence (Vocabulary has the highest g loading of any individual intelligence subtest; Brody, 1992). Moreover, this covariation was necessary because of a trend for higher Vocabulary scores among the controls as compared with the participants with TS. Results
Component Process Correlations With Visual-Motor Integration Correlational analyses tested the relationship between each component process and the supraordinate domain of visual-motor integration skill. Separate correlational analyses within the TS and control groups revealed highly similar patterns; hence, the results employing the total sample are reported. The two measures of visual-motor integration used in this study, the Rey and the VMI, were significantly correlated (removing Vocabulary, partial r = .48, p < .0001), suggesting that they tap a common performance dimension. Our model (Figure 1) predicted that each of the four component processes would correlate with the VMI and the Rey. Partial correlations were significant between Matrices and the VMI (r = .33, p < .05), and BD and the VMI (r = .53, p < .0001), supporting the association between visual-perceptual skill and visual-motor integration. BD was also significantly correlated with the Rey (partial r = .47, p < .0001), but Matrices was not (partial r = .19, ns). Next, the relationship between motor coordination and visual-motor integration skill was assessed. Significant partial correlations were observed for dominant, nondominant, and bimanual performance on the Purdue Pegboard and the VMI (partial rs = .25, .27, and .29, respectively, all ps < .05). However, partial correlations between the Purdue Pegboard and the Rey were not significant. Thus, both motor and visual-perceptual reasoning were more strongly associated with the VMI than with the Rey. Neither motor control nor sustained attention measures correlated significantly
139
with the visual-motor integration measures, after controlling for general intelligence. In a multiple regression, BD (controlling for Vocabulary) was the only significant predictor of visual-motor integration skill, even though in the absence of BD, the Purdue Pegboard also had shown a relationship to visual-motor integration skill.
Discriminant Function Analyses Stepwise discriminant function analyses were used to test the hypothesis that children with TS could be differentiated from the unaffected control children on the basis of their neuropsychological performance on measures of visualmotor integration and the proposed component processes (controlling for Vocabulary scores). Table 5 presents the mean scores ( _ SD) for each of the measures in the model by diagnostic group. In addition, because the semipartiai correlation between the Childhood Depression Inventory raw scores and the VMI (controlling for Vocabulary) was negative ( r - - . 2 4 , p < .05), the Childhood Depression Inventory was also included in the model. The overall model was significant, Wilks's lambda = 0.74, F(2, 63) = 11.29, p < .0001. However, only the VMI, F(1, 63) = 11.54, p < .005, and the number of commission errors on the AX condition of the CPT, F(1, 63) = 8.15, p < .01, contributed significantly to the prediction. These two variables enabled correct classification of 82% of the unaffected control participants and 80% of children with TS. The Rey was not a significant contributor to the model. In fact, the univariate analysis controlling for g found only a statistical trend (p < .10) for worse performance on the Rey by children with TS compared with control participants.
Analyses of Component Processes Next we examined whether each of the measures of the component processes were related to TS. Although the discriminant function analysis showed that only the VMI and motor inhibition were significant predictors, their inclusion in that model precluded an understanding of group differences on lower level processes with which they share variance. To test for possible group differences in performance on individual measures of visuoperceptual processing, fine-motor control, vigilance, and motor inhibition, a series of MANCOVAs was conducted, with Vocabulary included as a covariate. These analyses allow for greater comparability between this and other studies but do not supplant the discriminant function analyses. MANCOVA testing for group difference in the visuoperceptual ability tests (BD and Matrices) was significant, Wilks's lambda = .873, F(2, 68) = 4.96, p < .01. Subsequent analyses of covariance showed that children with TS performed significantly lower on Matrices, F(1, 69) = 8.74, p < .001, with a trend for differences on BD, F(1, 69) = 3.29, p < .10. Within the fine-motor domain, a repeatedmeasures MANCOVA, with the dominant, nondominant, and bimanual conditions of the Purdue Pegboard as the dependent measures, was significant, Wilks's lambda = 0.872, F(3, 69) = 3.36, p < .05, with a significant main
140
SCHULTZ ET AL. Table 5
Visual-Motor Integration and Component Process Scores by Diagnostic Group TS --- ADHD (n = 50) Test Visual-motor integration VMI Rey-Osterreith Copy Visual-perceptual skill KBIT Matrices Block Design Fine-Motor skill Purdue dominant Purdue nondominant Purdue bimanual Motor inhibition CPT X commissions CPT AX commissions Sustained attention CPT X omissions CPT AX omissions
TS + ADHD (n = 34)
TS - ADHD (n = 16)
Unaffected controls (n = 23)
M
SD
M
SD
M
SD
M
SD
90.9 24.6
12.7 4.5
90.4 24.9
13.9 4.6
92.0 24.5
9.9 4.3
105.3 26.9
12.4 3.8
110.7 11.14
11.8 3.04
111.1 11.09
11.9 3.13
109.8 11.30
11.9 3.0
122.2 12.96
14.5 3.17
13.47 12.28 10.49
1.97 1.39 1.98
13.44 12.29 10.35
2.20 1.60 2.19
13.53 12.25 10.78
1.41 0.86 1.46
14.74 13.35 11.72
1.80 1.72 1.70
6.86 10.28
5.33 7.88
7.43 10.23
6.2 7.86
5.64 10.40
2.44 8.18
3.32 4.32
3.00 3.75
3.98 3.57
3.11 2.78
4.13 3.48
2.98 2.61
3.64 3.73
3.48 3.20
2.42 2.77
3.73 2.18
Note. The Rey, Purdue Pegboard, and CPT are reported in raw scores; VMI, Matrices, and Block Design are reported in standard scores. All scores are group means with standard deviations. TS = Tourette syndrome; ADHD = attention deficit hyperactivity disorder; VMI = Beery Visual-Motor Integration Test; KBIT = Kaufman Brief Intelligence Test; CPT = continuous performance test. effect for diagnostic group, F(1, 71) = 10.02, p < .005. There were, however, no significant condition or Condition × Group interactions, suggesting no laterality or bimanual effects. Univariate analyses of covariance revealed that the TS group scored significantly lower on all three conditions of the Purdue Pegboard, F(1, 71) = 6.24, p < .05; F(1, 71) -8.54, p < .005; and F(1, 71) -- 6.73, p < .05, respectively. The two groups did not differ on the number o f pegs dropped (ps > .60 for each condition) or the number of losses o f set, that is, picking up two pegs at once (ps > .30), suggesting that the poorer performance of the TS participants was due to fine-motor control and speed, not to gross errors of coordination or violating the rules of the task. There were no significant differences on the C g r measures of vigilance (omission errors). However, the TS group exhibited more difficulty with motor inhibition, because they committed significantly more errors of commission in both the X condition, F(1, 57) = 4.67, p < .05, and the AX condition, F(1, 61) = 9.69,p < .005.
TS Subgroup Analyses Stepwise discriminant function analysis was used to evaluate whether neuropsychological measures could differentiate TS + A D H D from TS - ADHD. W h e n controlling for Vocabulary, none o f the measures differentiated these two groups. There were no differences between the two TS subgroups on Matrices, BD, the three Purdue Pegboard conditions, the Childhood Depression Inventory, or any CPT measure. However, when Vocabulary standard scores were entered into the model (without first residualizing the other variables), the model was significant, Wilks's lambda = 0.91, F(1, 48) = 4.90, p < .05. Children with TS + A D H D scored significantly lower on Vocabulary than did those with
TS - ADHD, F(1, 70) = 4.09, p < .05, and Vocabulary scores correctly classified 74% of the children with TS + A D H D and 63% o f the children with TS - ADHD. Symptom severity of TS and OCD at the time o f testing was assessed using the Yale Global Tic Severity Scale and Children's Yale-Brown Obsessive-Compulsive Scale, respectively (see Table 4). Compared with the TS + A D H D group, the TS - A D H D group had a significantly greater total obsessions score, t(1, 30) = 2.06, p < .05. On the other hand, the TS + A D H D group had a significantly greater total phonic tic score, t(1, 33) = 2.09, p < .05. No group differences were found for motor tics, compulsions, Childhood Depression Inventory, or the total score. Correlational analyses within the TS group with each of these variables and the cognitive measures suggested few significant relationships. Total phonic tic score correlated negatively with Spelling (r = - . 4 1 , p < .05) and positively with CPT X omissions (r = .42, p < .05). On the Children's Yale-Brown Obsessive-Compulsive Scale, the total compulsions score was negatively correlated with BD (r = - . 3 6 , p < .05). Number of DSM-III-R A D H D symptom criteria correlated negatively with Reading (r = - . 3 5 , p < .05) and Spelling (r = - . 4 1 , p < .01) scores from the Kaufman Test of Educational A c h i e v e m e n t - - B r i e f form (Kaufman & Kaufman, 1985). Our index o f general psychopathology, created by summing the number of DSM-III-R diagnoses, was negatively correlated with the V M I (r = - . 3 4 , p < .05). Given the number o f multiple comparisons, these correlations should be interpreted with caution. Discussion Consistent with prior studies, we obtained significant differences between children with TS and unaffected con-
VISUAL-MOTOR INTEGRATION IN TS trois on measures of visual-motor integration. Children with TS scored approximately 1 SD below the controls on the VMI. The TS group also performed significantly lower on copying the Rey, a more complex design that demands executive organization, although the effect size was smaller (about 0.5 SD) and reduced to a trend when covarying the influence of general intelligence. Thus, deficits in visualmotor integration skill among children with TS may be less pronounced on tests with more of an executive-functioning component. This is in agreement with the extant literature (Table 1) because the only negative finding to date with respect to visual-motor integration is with a comparison employing the Rey. Moreover, the VMI, which is a purer measure of visual-motor integration skill than the Rey, was the best predictor of TS group membership in our discriminant function analyses and was more highly correlated with the component processes in our model (Figure 1). We obtained partial validation of our neuropsychological model of visual-motor integration skill. Even after controlling for general intelligence, visual-perceptual skill (BD and Matrices) and fine-motor coordination (Purdue Pegboard) were significantly correlated with visual-motor integration. However, we did not find significant correlations between visual-motor integration and either sustained attention (CPT omissions) or motor inhibition (CPT commissions). Thus, two of the four constructs in our model were shown to share variance with visual-motor integration independent of g. Before concluding that sustained attention and motor inhibition are not essential component processes of visual-motor integration, further study is warranted using additional or different measures of these constructs to test the proposed relationships. Recent advances in CPTs provide more sensitive measures of vigilance and motor inhibition (e.g., the Conners CPT; Conners, 1994). A principle aim of the study was to test whether observed relative deficits in visual-motor integration might be secondary to problems among one or more of the component processes. The literature on fine-motor coordination difficulties in TS is nearly as compelling as that of visual-motor integration, but there have been no studies of the impact of fine-motor coordination deficits on drawing ability. In agreement with previous studies, TS children performed about 0.75 SD below that of controls on the Purdue Pegboard. However, when the VMI was entered into the discriminant function analysis, the Purdue Pegboard no longer contributed unique variance to distinguish the groups, suggesting that its predictive power was absorbed by its functional overlap with the VMI. Although we employed the Purdue Pegboard as a test of motor coordination, indisputably there is a visual component to the test. Indeed, it is difficult to conceive of meaningful tests of motor coordination that do not involve either direct visualization or visual imagery (e.g., a motor test when blindfolded might still engage visual mapping and imagery of the physical environment). Comparisons of motor skill among the congenitally blind with and without TS might adjudicate the issue, but such samples would be difficult to ascertain. The literature on potential visuoperceptual deficits in TS
141
is smaller, less coherent, and less persuasive, largely because the measures employed have not been highly specific to this domain of functioning. Our measures (Matrices and BD) are open to that same criticism, because performance on these tests is multidetermined, with a clear loading on g. Nevertheless, children with TS were found to have a relative weakness on both BD and Matrices (covarying Vocabulary as a proxy for g). This finding, however, is complicated by the fact that the children with TS scored above the general population mean on both BD and Matrices, whereas the unaffected controls scored well above the mean on these measures (but not on Vocabulary), suggesting that the samples may not be representative. When entered into the discriminant function analyses with the VMI, however, neither of the visual-perceptual measures were additive independent predictors of diagnosis. Thus, children with TS scored lower on the VMI compared with the controls even when controlling for visual-perceptual skill (BD and Matrices). Although continuous performance measures of sustained attention and motor inhibition did not correlate with visualmotor integration as predicted, motor inhibition was the other significant variable in the discriminant function analysis. The children with TS were much more impulsive than the controls, and their motor disinhibition as measured with a CPT was independent of visual-motor integration deficits. Stepwise discriminant function analyses showed that, in combination, visual-motor integration skill and inhibitory control were able to accurately classify 82% of the unaffected controls and 80% of the children with TS. Surprisingly, the CPT measurement of impulsivity was not predictive of comorbid ADHD among the children with TS, suggesting that either our CPT was insensitive or that ADHD in the context of TS is qualitatively different from ADHD alone. We also examined the possible impact of comorbid ADHD on visuomotor integration skill, a potential confound that had not previously been addressed in the literature. The TS + ADHD and TS - ADHD participants were equally impaired on the VMI, further suggesting that the relative deficit in visual-motor integration among children with T S is independent of disorders of attention and impulse control. Other investigators have noted that the majority of patients with TS perform within normal limits on tests of neuropsychological functioning ( ± 1.5 SD from the mean), with only a subsample showing clinically meaningful impairments (Randolph et al., 1993). For example, Bornstein (1990) showed that approximately 20% of his sample of 100 children with TS showed impairment on a summary index of neuropsychological functioning, with impairments in sensory and motor functioning being the most common. Our data are in agreement with this assessment, because only a fraction of the participants with TS scored well below the normative mean on the visual-motor and fine-motor measures. For example, 32% of the children with TS scored at least 1 SD below the mean on the VMI, while 78% scored below the mean. Thus, the entire distribution of scores appears to be shifted slightly downward toward more impaired performance on select neuropsychological measures. The shift is small enough that the majority of children
142
SCHULTZ ET AL.
with TS functioned within normal limits, broadly defined, although not so small as to be easily ignored, especially when one considers the fact that Full-Scale IQ in this sample was somewhat above the general population mean. The neural basis for deficient visual-motor integration skill in TS is uncertain. Although the parallels to developmental disorders such as TS may be imprecise, considerable knowledge about systems subserving visual-motor integration and its component processes has been gleaned from lesions in adulthood. Both right- and left-hemisphere processes have been implicated in drawing ability, but the contributions of each to good performance is probably different. Right-hemisphere damage typically results in drawings with sufficiently accurate detail but distorted spatial relations among the elements and a failure to capture the gestalt, while left-hemisphere lesions more often result in drawings that are slowly executed, oversimplified, lacking detail, but spatially intact (Gainotti & Tiacci, 1970; Marshall et al., 1994; McFie & Zangwill, 1960; Warrington, James, & Kinsbourne, 1966). The drawing dysfunction among right-hemisphere-damaged patients appears to be a result of a primary impairment in perception as it guides the movement of the hand in space (e.g., Kirk & Kertesz, 1989; Warfington & James, 1967). Interpretation of left-brain mechanisms in drawing disturbance is more difficult and in many cases is attributable to low-level errors of motor execution secondary to dominant-hand hemiparesis (Carlesimo, Fadda, & Caltagirone, 1993; Gainotti, 1985; Kirk & Kertesz, 1989). However, ideomotor dyspraxia (i.e., deficits in selecting and sequencing movement elements) and ideational dyspraxia (deficits in the conceptual organization and planning of movement) can also cause the simplification of drawing seen in left-hemisphere constructional dyspraxics (Kirk & Kertesz, 1989; Piercy, Hfcaen, & Ajuriacurra, 1960; Warrington & James, 1967). Although both hemispheres may contribute to visual-motor integration, a more important role for the fight is suggested by the greater frequency of drawing difficulties with right-hemisphere lesions (Damasit, 1985), especially when patients with global cognitive deficits are excluded (Villa, Gainotti, & De Bonis, 1986). Lesions to the parietal cortex in humans produce impaired visual perception, particularly when the injury is in the right hemisphere (for a complete review, see Andersen, 1987). The integration of motor movements with visuoperception is conducted with body-centered representations of space (as opposed to retinotopic) within the posterior parietal cortex (Andersen & Zipser, 1988). Single-cell recording studies in nonhuman primates and functional neuroimaging studies in humans indicate that the posterior parietal cortex codes for the position of body parts relative to one another and to the external world and participates in planned movements in external space (Andersen, 1987; Bonda, Petrides, Frey, & Evans, 1995). These processes are essential for accurate drawing. Posterior parietal lobule lesions result in reaching errors and deficits in fine-motor coordination with visual guidance (Andersen, 1987; Hyvarinen, 1982). Moreover, a small region within the posterior parietal cortex, the lateral intraparietal area, appears to be specialized for the visualmotor integration of saccadic eye movements, allowing
location of targets in space and planning for subsequent movements (Andersen, Brotchie, & Mazzoni, 1992). Superior aspects of the right parietal lobe also subserve somatosensory processes (Mountcastle, Lynch, Georgopoulos, Sakata, & Acufia, 1975), which allow for feedback about the placement of the pencil on the fingertips and real-time adjustments for fine-motor control during drawing. Although considerable evidence documents the role of the nondominant parietal lobe in somatosensory and visuospatial processes contributing to visual-motor integration, it is also clear that drawing is a complex ability involving multiple brain regions. The integration of visuoperceptual, somatosensory, and motor components in drawing is probablymediated by bidirectional exchange of information between parietal and motor areas of the frontal cortex (Quintana & Fuster, 1993), with a substantial integrative contribution from subcortical circuits (e.g., Alexander, Delong, & Strick, 1986). Indeed, visuomotor integration deficits may arise from frontal and subcortical lesions, in addition to parietal lobe lesions. Marshall and colleagues (Marshall et al., 1994) studied drawing dysfunction in 37 patients with fight-hemisphere stroke, with lesions distributed between subcorfical, anterior, and posterior cortical locations. When both drawing and visuoperceptual function was disturbed, lesions always involved the temproparietaloccipital junction. When visual-spatial functions were intact, but drawings were unrecognizable, lesion location more often was subcortical, with a point of lesion overlap across participants in the anterior limb of the internal capsule and the lateral head of the fight caudate nucleus. Thus, the basal ganglia may have a specific role in the synthesizing motor programming and perceptual inputs. This is consistent with other reports of constructional apraxia after subcortical lesions in the nondominant hemisphere (e.g., Agostini, Collette, Orlando, & Tredici, 1983). The role of the basal ganglia in drawing disturbance is particularly intriguing because neuroimaging, neuropathological, and phenomenological studies implicate the basal ganglia and functionally related cortical and thalamic structures in the pathobiology of TS (Anderson et al., 1992; Balthazar, 1956; Hyde et al., 1995; Peterson et al., 1993; Singer, Hahn, & Moran, 1991; Singer et al., 1993). A specific role for the right caudate in the pathobiology is suggested by a magnetic resonance imaging study of 10 pairs of monozygotic twins concordant for tics (Hyde et al., 1995). The size of the right caudate nucleus was significantly reduced in the more severely affected twin. Abnormalities of the right caudate, therefore, could have a primary role in both the tic behavior and the impaired visual-motor integration skills seen in TS. However, our data suggest that the pathobiology is probably bilateral because we found that dominant and nondominant hand were equally impaired on the Purdue Pegboard. Interestingly, family studies support an etiologic link between TS and one form of OCD (Pauls, Raymond, Stevenson, & Leckman, 1991; Pauls, Towbin, Leckman, Zahner, & Cohen, 1986), and OCD also involves relative deficits in visual-motor integration (Behar et al., 1984; Boone, Ananth, Philpott, Kaur, & Djenderedjian, 1991;
VISUAL-MOTOR INTEGRATION IN TS Hollander et al., 1993), visuoperceptual ability (Aronowitz et al., 1994), and visual-spatial reasoning (Head, Bolton, & Hymas, 1989; Savage et al., 1996). Moreover, neuroimaging findings also implicate the caudate nuclei in the pathobiology of OCD (Baxter et al., 1992; Luxenberg et al., 1988; Robinson et al., 1995), suggesting that the visuoperceptual and visuomotor integration deficits in TS and OCD may arise from a common abnormality in the basal ganglia, and more specifically in the caudate nuclei and their associated cortical-striatal networks. This is feasible because the caudate serves an integrative function, receiving input from motor areas of the frontal lobe (e.g., frontal eye fields, lateral orbital, supplementary motor and premotor areas) and visuoperceptual areas of the parietal lobe (Alexander et al., 1986). The caudate is well situated to function as a control process for the integration of motor and perceptual processing streams important to visual-motor integration. In summary, our data are in complete agreement with the extant literature on relative deficits in visual-motor integration among children with TS. Moreover, we found no evidence to suggest that comorbid ADHD or depressive symptomatology could account for the observed group differences. The consistency with which drawing difficulties have been observed across all studies in the literature suggests that this domain of functioning should be routinely assessed for all referrals with TS. In our experience, the manner in which the child's difficulty with visual-motor integration is typically manifested is in his or her penmanship. Frequently these children struggle with legible handwriting and in many cases it is a significant impediment in school. This study also provides partial support for a component process model of visual-motor integration. Scores on the VMI were significantly correlated with tests of visuoperceptual and fine-motor coordination. Moreover, three putative component processes, fine-motor skill, visuoperceptual ability, and response inhibition, were also significant areas of weakness for children with TS, irrespective of their ADHD status. However, none of the measures used for assessing these three component processes could fully account for the deficits in visual-motor integration. Therefore, the integration of sensory and motor processes appears to be a fundamental consequence of TS, perhaps arising from abnormalities in the caudate nuclei. We advocate the use of a component process approach to disentangle dimensions of visual-motor integration. Future studies should consider using motor-free tests of visuoperceptual and visuospatial functioning, simple and complex motor tasks with a limited role for visuoperceptual analyses, and more extensive measures of motor inhibition and vigilance.
References Achenbach, T. M. (1991). Manual for the Child Behavior Checklist and Revised Child Behavior Profile. Burlington: University of Vermont, Department of Psychology. Agostini, E., Collette, A., Orlando, G., & Tredici, G. (1983). Apraxia in deep cerebral lesion. Journal of Neurology, Neurosurgery and Psychiatry, 46, 804-808.
143
Alexander, G. E., Delong, M. R., & Strick, E L. (1986). Parallel organization of functionally segregated circuits linking basal ganglia and cortex. Annual Review of Neuroscience, 9, 357-381. American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disorders (3rd ed., rev.). Washington, DC: Author. Andersen, R. A. (1987). Inferior parietal lobule function in spatial perception and visuomotor integration. In E Plum, V. B. Mountcastle, & S. R. Geiger (Eds.), The handbook of physiology: Section 1: The nervous system. Vol. 5. Higher functions of the brain (pp. 483-518). Bethesda, MD: American Physiological Society. Andersen, R. A., Brotchie, E R., & Mazzoni, R (1992). Evidence for the lateral intraparietal area as the parietal eye field. Current Opinion in Neurobiology, 2, 840-846. Andersen, R. A., & Zipser, D. (1988). The role of the posterior parietal cortex in coordinate transformations for visual-motor integration. Canadian Journal of Physiological Pharmacology, 66, 488-501. Anderson, G., Pollak, E., Chatterjee, D., Leckman, J., Riddle, M., & Cohen, D. (1992). Postmortem analyses of brain monoamines and amino acids in Tourette's syndrome: A preliminary study of subcortical regions. Archives of General Psychiatry, 49, 584586. Aronowitz, B. R., Hollander, E., DeCaria, C., Cohen, L., Saoud, J. B., Stein, D., Liebowitz, M. R., & Rosen, W. G. (1994). Neuropsychology of obsessive-compulsive disorder: Preliminary findings. Neuropsychiatry, Neuropsychology and Behavioral Neurology, 7, 81-86. Balthazar, K. (1956). Uber das anatomishe substrat der generalisierten tic-krenkeit (maladie des tics, Gilles de la Tourette): Entwicklungshemmung des corpus striatum. Archives of Psychiatry Nervenkr, 195, 531-549. Barkley, R. A. (1990). Attention deficit hyperactivity disorder: A handbook for diagnosis and treatment. New York: Guilford Press. Baxter, L. R., Schwartz, J. M., Bergman, K. S., Szuba, M. P., Guze, B. H., Mazziotta, J. C., Alazraki, A., Selin, C. E., Ferng, H., Munford, P., & Phelps, M. E. (1992). Caudate glucose metabolic rate changes with both drug and behavior therapy for obsessivecompulsive disorder. Archives of General Psychiatry, 49, 681689. Beery, K. E. (1989). Developmental test of visual-motor integration: Administration, scoring and teaching manual. Cleveland, OH: Modern Curriculum Press. Behar, D., Rapoport, J. L., Berg, C. J., Denckla, M. B., Mann, L., Cox, C., Fedio, P., Zahn, T., & Wolfman, M. G. (1984). Computerized tomography and neuropsychological test measures in children with obsessive--compulsive disorder. American Journal of Psychiatry, 141, 363-369. Bonda, E., Petrides, M., Frey, S., & Evans, A. (1995). Neural correlates of mental transformations of the body-in-space. Proceedings of the National Academy of Sciences, USA, 92, 11180-11184. Boone, K. B., Ananth, J., Philpott, L., Kaur, A., & Djenderedjian, A. (1991). Neuropsychological characteristics of nondepressed adults with obsessive--compulsive disorder. Neuropsychiatry, Neuropsychology, & Behavioral Neurology, 4, 96-109. Bornstein, R. A. (1990). Neuropsychological performance in children with Tourette syndrome. Psychiatric Research, 33, 73-81. Bornstein, R. A. (1991). Neuropsychological performance in adults with Tourette syndrome. Psychiatric Research, 37, 229-236.
144
SCHULTZ ET AL.
Bornstein, R. A., Baker, G. B., Bazylewich, T., & Douglass, A. B. (1991). Tourette syndrome and neuropsychological performance. Acta Psychiatry Scandanavia, 84, 212-216. Bornstein, R. A., & Yang, V. (1991). Neuropsychological performance in medicated and unmedicated patients with Tourette's disorder. American Journal of Psychiatry, 148, 468--47 t. Brody, N. (1992). Intelligence. New York: Academic Press. Brookshire, B. L., Butler, I. J., Ewing-Cobbs, L., & Fletcher, J. M. (1994). Neuropsychological characteristics of children with Tourette syndrome: Evidence for a nonverbal learning disability? Journal of Clinical and Experimental Neuropsychology, 16, 289-302. Campbell, S. B., & Werry, J. S. (1986). Attention deficit disorder (hyperactivity). In H. C. Quay & J. S. Werry (Eds.), Psychopathological disorders of childhood (3rd ed., pp. 111-155). New York: Wiley. Carlesimo, G. A., Fadda, L., & Caltagirone, C. (1993). Basic mechanisms of constructional apraxia in unilateral braindamaged patients: Role of visuoperceptual and executive disorders. Journal of Clinical and Experimental Neuropsychology, 15, 342-358. Cassens, G., Inglis, A. K., Appelbaum, E S., & Gutheil, T. G. (1990). Neuroleptics: Effects on neuropsychological function in chronic schizophrenic patients. Schizophrenia Bulletin, 16, 477-499. Cohen, D. J., Detlor, J., Shaywitz, B. A., & Leckman, J. E (1982). Interaction of biological and psychological factors in the natural history of Tourette syndrome: A paradigm for childhood neuropsychiatric disorders. In A. J. Friedhoff & T. N. Chase (Eds.), Advances in neurology (pp. 31-40). New York: Raven Press. Comings, D. E., & Comings, B. G. (1985). Tourette syndrome: Clinical and psychological aspects of 250 cases. American Journal of Human Genetics, 35, 435-450. Conners, C. K. (1989). Conners' rating scales manual. North Tonawanda, NY: Multi-Health Systems. Conners, C. K. (1994). The Conners Continuous Performance Test (CPT) (Version 3.0) [Computer software]. North Tonawanda, NY: Multi-Health Systems. Damasio, A. R. (1985). Disorders of complex visual processing: Agnosias, achromatopsia, Balint's syndrome, and related difficulties of orientation and construction. In M. M. Mesulam (Ed.), Principles of behavioral neurology (pp. 259-288). Philadelphia: Davis. DuPaul, G. J. (1991). Parent and teacher ratings of ADHD symptoms: Psychometric properties in a community based sample. Journal of Clinical Child Psychology, 20, 245-253. Dykens, E., Leckman, J., Riddle, M., Hardin, M., Schwartz, S., & Cohen, D. (1990). Intellectual, academic, and adaptive functioning of Tourette syndrome children with and without attention deficit disorder. Journal of Abnormal Psychology, 18, 607-615. Eapen, N., Pauls, D. L., & Robertson, M. M. (1993). Evidence for autosomal dominant transmission in Gilles de la Tourette syndrome: United Kingdom Cohort Study. British Journal of Psychiatry, 162, 593-596. Ferrari, M., Matthews, W. S., & Barabas, G. (1984). Children with Tourette syndrome: Results of psychological tests given prior to drug treatment. Developmental Behavioral Pediatrics, 5, 116-119. Flament, M. E, Whitaker, A., Rapoport, J. L., Davies, M., Zarenba-Berg, C., Kalikow, K., Sceery, W., & Shaffer, D. (1988). Obsessive compulsive disorder in adolescence: An epidemiological study. Journal of the American Academy of Child and Adolescent Psychiatry, 6, 764-771. Frost, L. A., Moffitt, T. E., & McGee, R. (1989). Neuropsychological correlates of psychopathology in an unselected cohort of young adolescents. Journal of Abnormal Psychology, 98, 307313.
Gainotti, G. (1985). Constructional apraxia. In E J. Vinken, G. W. Bruyn, & H. L. Klawans (Eds.), Handbook of clinical neurology (pp. 491-505). Amsterdam: Elsevier Science. Gainotfi, G., & Tmcci, C. (1970). Patterns of drawing disability in right and left hemispheric patients. Neuropsychologia, 8, 379-384. Golden, G. S. (1984). Psychologic and neuropsychologic aspects of Tourette's syndrome. Neurologic Clinics, 2, 91-102. Hagin, R. A., Beecher, R., Pagano, G., & Kreeger, H. (1982). Effects of Tourette syndrome on learning. Advances in neurology: Vol. 35. Gilles de la Tourette syndrome (pp. 323-329). New York: Raven. Harris, E. L., Schuerholz, L., Singer, H. S., Reader, M. J., Brown, J. E., Cox, C., Mohr, J., Chase, G. A., & Denkla, M. B. (1995). Executive function in children with Tourette syndrome and/or attention deficit hyperactivity disorder. Journal of the International Neuropsychological Society, 1, 511-516. Hasstedt, S. J., Leppert, M., Filloux, E, van de Wetering, B. J., & McMahon, W. M. (1995). Intermediate inheritance of Tourette syndrome, assuming assortative mating. American Journal of Human Genetics, 57, 682-689. Head, D., Bolton, D., & Hymas, N. (1989). Deficit in cognitive shifting ability with obsessive--compulsive disorder. Biological Psychiatry, 25, 929-937. Hollander, E., Cohen, L., Richards, M., Mullen, L., DeCaria, C., & Stem, Y. (1993). A pilot study of the neuropsychology of obsessive-compulsive disorder and Parkinson's disease: Basal ganglia disorders. Journal of Neuropsychiatry and Clinical Neurosciences, 5, 104-107. Hyde, T., Stacey, M., Coppola, R., Handel, S., Rickler, K., & Weinberger, D. (1995). Cerebral morphometric abnormalities in Tourette's syndrome: A quantitative MRI study of monozygotic twins. Neurology, 45, 1176--1182. Hyv/irinen, J. (1982). The parietal cortex of monkey and man. Berlin, Germany: Springer-Verlag. Incagnoli, T., & Kane, R. L. (1981). Neuropsychological functioning in Gilles de la Tourrette's syndrome. Journal of Clinical Neuropsychology, 3, 167-171. Kaufman, A. S., & Kaufman, N. L. (1985). Kaufman Test of EducationaI Achievement: Briefform manual. Circle Pines, MN: American Guidance Service. Kaufman, A. S., & Kaufman, N. L. (1990). Kaufman Brief Intelligence Test. Circle Pines, MN: American Guidance Service. King, D. J. (1990). The effect of neuroleptics on cognitive and psychomotor function. British Journal of Psychiatry, 157, 799811. Kirk, A., & Kertesz, A. (1989). Hemispheric contributions to drawing. Neuropsychologia, 27, 881-886. Kovacs, M. (1985). The Children's Depression Inventory (CDI). Psychopharmacology, 21, 995-1000. Lanser, J. B. K., Van Santen, W. H. C., Jennekens-Schinkel, A., & Roos, R. A. C. (1993). Tourette's syndrome and right hemisphere dysfunction. British Journal of Psychiatry, 163, 116-118. Leckman, J. E, Riddle, M. A., Hardin, M. T., Oft, S. I., Swartz, K. L., Stevenson, J., & Cohen, D. J. (1989). The Yale Global Tic Severity Scale: Initial testing of a clinician-rated scale of tic severity. Journal of the American Academy of Child and Adolescent Psychiatry, 28, 566-573. Leckman, J. E, Sholomskas, D., Thompson, W. D., Belanger, A., & Weissman, M. M. (1982). Best estimate of lifetime of psychiatric diagnosis. Archives of General Psychiatry, 39, 879-883. Loong, J. W. K. (1991). The Continuous Performance Test. San Luis Obispo, CA: Wang Neuropsychological Laboratory. Lucas, A. R., Kauffman, E E., & Morris, E. M. (1967). Gilles de la Tourette disease: A clinical study of fifteen cases. Journal of the American Academy of Child Psychiatry, 6, 700-722.
VISUAI~MOTOR INTEGRATION IN TS Luxenberg, J., Swedo, S., Flament, M., Friedland, R., Rapoport, J., & Rapoport, S. (1988). Neuroanatomical abnormalities in obsessive-compulsive disorder detected with quantitative X-ray computed tomography. American Journal of Psychiatry, 145, 1089-1093. Marshall, R. S., Lazar, R. M., Binder, J. R., Desmond, D. W., Drucker, E M., & Mohr, J. E (1994). Interhemispheric localization of drawing dysfunction. Neuropsychologia, 32, 493-501. Matarazzo, J. D. (1990). Psychological assessment versus psychological testing. American Psychologist, 45, 999-1017. McFie, J., & Zangwill, O. L. (1960). Visual-constructive disabilities associated with lesions of the left cerebral hemisphere. Brain, 83, 243-260. Mountcastle, V. B., Lynch, J. C., Georgopoulos, A., Sakata, H., & Acufia, C. (1975). Posterior parietal association cortex of the monkey: Command function for operations within exterpersonal space. Journal of Neurophysiology, 38, 871-908. Naugle, R. I., Chelune, G. J., Tucker, G. (1993). Validity of the Kaufman Brief Intelligence Test. Psychological Assessment, 5, 182-186. Orvascbel, H., & Puig-Antich, J. (1987). Schedule for Affective Disorders and Schizophrenia for School-Age Children (K-SADS) (4th ed.). (Available from Helen Orvaschel, Western Psychiatric Institute and Clinic, 3811 O'Hara St., Pittsburgh, PA 15213) Osterreith, P. A. (1944). Le test de copie d'une figure complexe Archives de Psychologie, 30, 206-356. Pauls, D. L., & Leckrnan, J. E (1986). The inheritance of Gilles de la Tourette's syndrome and associated behaviors: Evidence for autosomal dominant transmission. New England Journal of Medicine, 315, 993-997. Pauls, D. L., Raymond, C. L., Stevenson, J. M., & Leckman, J. E (1991). A family study of Gilles de la Tourette syndrome. American Journal of Human Genetics, 48, 154-163. Pauls, D. L., Towbin, K. E., Leckman, J. F., Zahner, G. E. P., & Cohen, D. J. (1986). Gilles de la Tourette's syndrome and obsessive-compulsive disorder: Evidence supporting a genetic relationship. Archives of General Psychiatry, 43, 1180-1182. Peterson, B., Riddle, M., Cohen, D., Katz, L., Smith, J., Hardin, M., & Leckman, J. E (1993). Reduced basal ganglia volumes in Tourette's syndrome using 3-D reconstruction techniques from magnetic resonance images. Neurology, 43, 941-949. Piercy, M., Hrcaen, H., & Ajuriacurra, J. (1960). Constructional apraxia associated with unilateral cerebral lesions. Left and right side cases compared. Brain, 83, 225-242. Quintana, J., & Fuster, J. M. (1993). Spatial and temporal factors in the role of prefrontal and parietal cortex in visuomotor integration. Cerebral Cortex, 3, 122-132. Randolph, C., Hyde, T. M., Gold, J. M., Goldberg, T. E., & Weinberger, D. R. (1993). Tourette's syndrome in monozygotic twins. Neurology, 50, 725-728. Reitan, R. M., & Davison, L. A. (1974). Clinical neuropsychology: Current status and applications. Washington, DC: Winston. Rey, A. (1941). L'examen psychologique dans les cas d'encephalopathie traumatique. Archives de Psychologie, 28, 286-340. Reynolds, C. R., & Richmond, B. (1987). Revised Children's Manifest Anxiety Scale (RCMAS) manual. Los Angeles: Western Psychological Services. Riddle, M. A., Scahill, L., King, R. A., Hardin, M., Anderson, G., Ort, S. I., Smith, C., Leckman, J. E, & Cohen, D. J. (1992). Double-blind, crossover trial of fluoxetine and placebo in children and adolescents with obsessive--compulsive disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 31, 1062-1069.
145
Robertson, M. M., Trimble, M. R., & Lees, A. (1988). The psychopathology of the Gilles de la Tourette: A phenomenological analysis. British Journal of Psychiatry, 152, 383-390. Robinson, D., Wu, H., Munne, R. A., Ashtari, M., Alvir, J. M. J., Lemer, G., Koreen, A., Cole, K., & Bogerts, B. (1995). Reduced caudate nucleus volume in obsessive-compulsive disorder. Archives of General Psychiatry, 52, 393-398. Savage, C. R., Keuthen, N. J., Jenike, M. A., Brown, H. D., Baer, L., Kendrick, A. D., Miguel, E. C., Ranch, S. L., & Albert, M. S. (1996). Recall and recognition memory in obsessive-compulsive disorder. Journal of Neuropsychiatry and Clinical Neuroscience, 8, 99-103. Shapiro, A. K., Shapiro, E. S., Bruun, R. D., & Sweet, R. D. (1978). GiUes de la Tourette syndrome. New York: Raven Press. Shapiro, E., Shapiro, A. K., & Clarkin, J. (1974). Clinical psychological testing in Tourette's syndrome. Journal of Personality Assessment, 38 (5), 464-478. Singer, H., Hahn, I. H., & Moran, T. (1991). Abnormal dopamine uptake sites in postmortem striatum from patients with Tourette's syndrome. Annals of Neurology, 30, 558-562. Singer, H., Reiss, A., Brown, J., Aylward, E., Shih, B., Chee, E., Harris, E., Reader, M., Chase, G., Bryan, N., & Denclda, M. (1993). Volumetric MRI changes in basal ganglia of children with Tourette's syndrome. Neurology, 43, 950-956. Sparrow, S. S., Balla, D. A., & Cicchetti, D. V. (1984). Vineland Adaptive Behavior Scales. Circle Pines, MN: American Guidance Clinic. Stokes, A., Bawden, H. N., Camfield, E R., Backman, J. E., & Dooley, J. M. (1991). Peer problems in Tourette's disorder. Pediatrics, 87, 936-942. Suthedand, R. J., Kolb, B., Schoel, W. M., Whishaw, I. Q., & Davies, D. (1982). Neuropsychological assessment of children and adults with Tourette syndrome: A comparison with learning disabilities and schizophrenia. In A. J. Friedhoff & T. N. Chase (Eds.), Advances in neurology: Vol. 35. Gilles de la Tourette syndrome (pp. 311-321). New York: Raven. Taylor, E. M. (1959). The appraisal of children with cerebral deficits. Cambridge, MA: Harvard University Press. Tiffen, J. (1968). Purdue Pegboard Test. Chicago: Scientific Research Associates. Villa, G., Gainotti, G., & De Bonis, C. (1986). Constructive disabilities in focal brain-damaged patients: Influence of the hemispheric side, locus of lesion and coexistent mental deterioration. Neuropsychologia, 24, 497-510. Walkup, J. T., LaBuda, M. C., Singer, H. S., Brown, J., Riddle, M. A., & Hurko, O. (1996). Family study and segregation analysis of Tourette syndrome: Evidence for a mixed model of inheritance. American Journal of Human Genetics, 59, 684-693. Walkup, J. T., Scahill, L. D., & Riddle, M. A. (1995). Disruptive behavior, hyperactivity, and learning disabilities in children with Tourette's syndrome. In W. J. Weiner & A. E. Lang (Vol. Eds.), Advances in neurology: Vol. 65. Behavioral neurology of movement disorders (pp. 259-272). New York: Raven. Warrington, E. K., & James, M. (1967). Disorders of visual perception in patients with localized cerebral lesions. Neuropsychologia, 5, 253-266. Warrington, E. K., James, M., & Kinsbourne, M. (1966). Drawing disability in relation to laterality of cerebral lesion. Brain, 89, 53-82. Yeates, K. O., & Bornstein, R. A. (1994). Attention deficit disorder and neuropsychological functioning in children with Tourette's syndrome. Neuropsychology, 8, 65-74. Received March 18, 1996 Revision received April 25, 1997 Accepted June 4, 1997 •