of the systemic examination showed normal findings. What is the classic sign seen in the photographs? Answer: The Hertoghe sign. Thinning or loss of the outer ...
Pablo Robles*, Jose Julio Jiménez, and Isabel Monedero. Department of Cardiology, Fundación Hospital Alcorcón, Avda Budapest no. 1, 28922 Alcorcón ...
31 Jan 2012 ... The Art of R Programming: A Tour of Statistical. Software Design, by ... I would go
even further and argue that The Art of R programming is a ...
Matsuda M, Shimomura I, Sata M, Arita Y, Nishida M, Maeda N, Kumada M,. Okamoto Y ... Tan KC, Xu A, Chow WS, Lam MC, Ai VH, Tam SC, Lam KS.
Jan 16, 2017 - protein as markers of disease activity in association with up-regulation ... Interstitial granulomatous dermatitis (Ackerman's syndrome).
Clinical Vignette. Interstitial granulomatous dermatitis (Ackerman's syndrome) in SLE presenting with the 'rope sign'. A 50-yr-old man presented with synovitis of ...
Jun 22, 2017 - Annual Intranet & Digital Workplace Summit in San. Francisco, hosted ... and participate with your ne
Classical Conditioning Vignettes. 1. Jane is scared of loud noise. Loud noise makes her heart beat faster and she scream
Jan 13, 2016 - Tricuspid valve endocarditis and septic pulmonary emboli illustrated by ECG-gated multi-slice. CT of the chest. Emmanuel Coche1Ã, Etienne ...
We can save images in other formats by using IJ$saveAs() function of IJ class. We can check whether the given object is
Jun 22, 2017 - highlighted the top 10 key insights to help you communicate what you ... and participate with your new di
Dec 21, 2015 - E-mail address: [email protected]. Forty-eight-year old woman with left-sided mastectomy due to breast cancer received.
Dec 21, 2015 - Veldhuisen DJ. The effect of darbepoetin alfa treatment on clinical out- comes in anemic patients with symptomatic heart failure: a preplanned.
May 13, 2011 - hemichorea-hemiballismus (HCHB) movements on the left side. On admission, the neurological examination revealed no abnor- mal pyramidal ...
Nov 15, 2013 - of serum IgG4. IgG4-related ophthalmic disease was diag- nosed and the patient was prescribed prednisolone at a dose of 40mg/day, with ...
The purpose of the RImageJ Vignette is to show how to get up and ... ImageJ GUI can be launced from R/JGR console by cre
food when. John shakes the food bag. John started to whistle when shaking the bag. One day,. 1. John was whistling at a
The quality of ECG interpretation by GPs was evaluated in several studies. ..... Dubin D. Snelle interpretatie van ECG's. Vierde, geheel herziene druk.
The scientist teaches a crow how to use tools to find food in a puzzle box. Another crow observes the first crow find th
The Government is proposing to introduce a simple time-based charge for the use of the United. Kingdom road network by h
of images are combined or blended, such as image-based rendering, texture projection ... aperture limits light paths equally at the center and edges of frame. Some lens ... spatial variation â which they call âintended vignettingâ â using a l
Vignette: Counting flowers. Note: Use these ... Ask participants to watch and
listen to the vignette. ... always different ways of seeing the same practice or
event.
issues and will most likely increase in use as software for ... (1) nature of a sales practice (does/does ..... Empirical studies of mental accounting by consumers.
General notes / Tips: ⢠Exact problem w/ single answer. ⢠Follow the program exactly. ⢠Be aware of sun exposure p
E-mail: [email protected]. Published as a Rapid ... From the Departments of 1Endocrinology and 2Neurology, Command Hospital, Lucknow, UP, India.
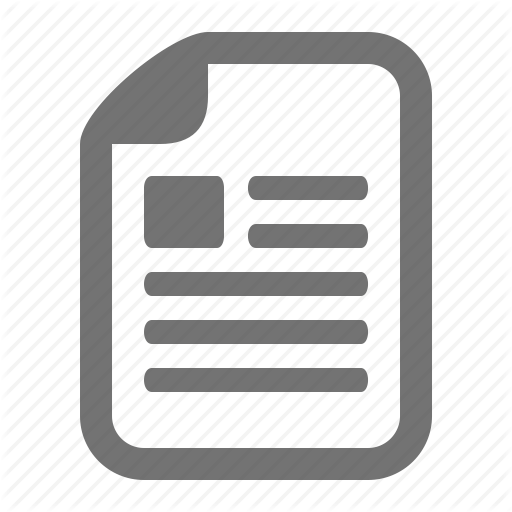
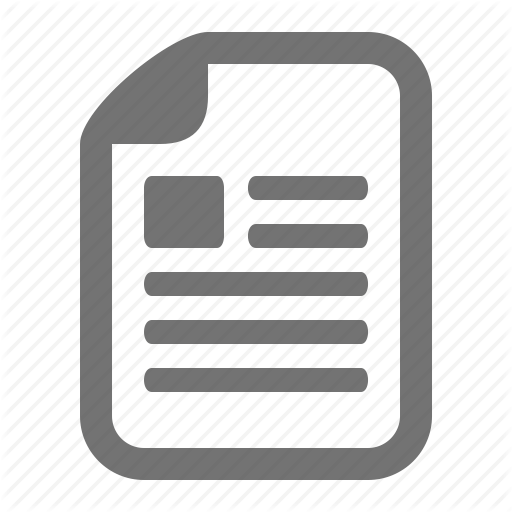
Visual Vignette K. V. S. Hari Kumar, MD, DNB1; Somasekharan Manoj, MD, DM2 From the Departments of 1Endocrinology and 2Neurology, Command Hospital, Lucknow, UP, India Case Presentation: A 30-year-old man presented with progressively worsening weakness of both shoulder girdle muscles associated with wasting for a period of 1 year. The patient had initially noticed muscle aches followed by easy fatigability in using both arms and also difficulty in climbing stairs. There was no history to suggest involvement of the distal muscles of the extremities or pharyngeal, neck, trunk, or ocular muscles. He indicated that he had gained 4 kg during a 1-year period and had periorbital puffiness. Physical examination revealed sinus bradycardia (pulse, 52/min), dry skin, a dull expressionless face with puffy eyelids, and no evidence of goiter (Fig. 1). Neurologic examination disclosed proximal weakness of both shoulders in all movements in association with atrophy of muscles but without evidence of percussion myotonia over the deltoid muscles (Fig. 2). He had grade 4 strength (on a scale of 1 to 5) in both lower limbs proximally in conjunction with normal strength distally. Deep tendon jerks were elicitable with delayed relaxation. The rest of the systemic examination showed normal findings. What is the diagnosis?
Fig. 1
Fig. 2
Answer: Hypothyroidism-associated myopathy. Routine hematologic and biochemical tests showed normal results except for dyslipidemia (total cholesterol, 225 mg/dL; triglycerides, 196 mg/dL; and low-density lipoprotein cholesterol, 156 mg/ dL) and elevated creatine kinase (CK) (180 U/L; normal,