Pulmonary Perspective Asthma and Chronic Obstructive Pulmonary Disease Common Genes, Common Environments? Dirkje S. Postma1,2, Marjan Kerkhof2,3, H. Marike Boezen2,3, and Gerard H. Koppelman2,4 Departments of 1Pulmonology, 3Epidemiology, 4Pediatric Pulmonology and Pediatric Allergology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands; and 2Groningen Research Institute for Asthma and COPD, The Netherlands
Asthma and chronic obstructive pulmonary disease (COPD) show similarities and substantial differences. The Dutch hypothesis stipulated that asthma and COPD have common genetic and environmental risk factors (allergens, infections, smoking), which ultimately lead to clinical disease depending on the timing and type of environmental exposures (Postma and Boezen, Chest 2004;126: 96S2104S). Thus, a particular group of shared genetic factors may lead to asthma when combined with specific environmental factors that are met at a certain stage in life, whereas combination with other environmental factors, or similar environmental factors at a different stage in life, will lead toward COPD. Multiple genes have been found for asthma and COPD. In addition to genes unique to these diseases, some shared genetic risk factors exist. Moreover, there are both common host risk factors and environmental risk factors for asthma and COPD. Here we put forward, based on the data available, that genes that affect lung development in utero and lung growth in early childhood in interaction with environmental detrimental stimuli, such as smoking and air pollution, are contributing to asthma in childhood and the ultimate development of COPD. Additional genes and environmental factors then drive specific immunological mechanisms underlying asthma, and others may contribute to the ultimate development of specific subtypes of COPD (i.e., airway disease with mucous hypersecretion, small airway disease, and emphysema). The genetic predisposition to the derailment of certain pathways may further help to define subgroups of asthma and COPD. In the end this may lead to stratification of patients by their genetic make-up and open new therapeutic prospects. Keywords: asthma; COPD; genetics; risk factors
Genetic factors contribute to the development of lung diseases such as cystic fibrosis, sarcoidosis, interstitial fibrosis, lung cancer, asthma, and chronic obstructive pulmonary disease (COPD). Cystic fibrosis is a monogenic disease, most frequently caused by a deletion of three nucleotides from the CFTR gene. In contrast, asthma and COPD are complex diseases wherein multiple genes and their interaction with environmental factors contribute to disease development. Thus, there is not a one-toone relationship between a gene and a disease. Notwithstanding this complexity, genetic studies have discovered genes and pathways contributing to disease development, and some of them are targets for therapy (1). (Received in original form November 6, 2010; accepted in final form February 3, 2011) Correspondence and requests for reprints should be addressed to Dirkje S. Postma, M.D., Ph.D., Department of Pulmonology, University Medical Center Groningen, Hanzeplein 1, PO Box 30001, 9700 RB Groningen, The Netherlands. E-mail:
[email protected] This article has an online supplement, which is accessible from this issue’s table of contents at www.atsjournals.org Am J Respir Crit Care Med Vol 183. pp 1588–1594, 2011 Originally Published in Press as DOI: 10.1164/rccm.201011-1796PP on February 4, 2011 Internet address: www.atsjournals.org
The field of genetics has evolved over the past decennia due to completion of the HapMap project, applications to perform genomic studies with high-throughput techniques, and developments of statistical analyses to test for association of a million single nucleotide polymorphisms (SNPs) at the same time and to assess gene–gene and gene–environment interaction. The current challenge is to unravel the relation between variants in newly identified genes and their function to better design treatments of respiratory diseases. Genetic studies initially addressed single genes that are candidates for disease development and/or performed linkage analyses followed by positional cloning in families of an affected proband. Recently, genome-wide association studies (GWAS) have identified novel genes, mostly without known function associated with diseases. However, these findings do not easily lead to a genetic test for a specific disease, because the positive predictive value of a single-gene test is limited and multiple genes and environmental factors have to be incorporated (2). This requires methods to model all these risk factors at the same time, and large cohort sizes with all data available for validation of the test. This review gives a bird’s-eye view of the past and present of genetics in asthma and COPD in the context of their common and differential origins.
DUTCH HYPOTHESIS In 1961, Orie and colleagues postulated the Dutch hypothesis, which stipulates that asthma and COPD have genetic and environmental risk factors such as allergens, infections, and smoking in common, which then ultimately lead to clinical disease depending on the timing and type of environmental exposure (3). This has led to a wide variety of research investigating similarities and differences between asthma and COPD in cross-sectional studies. However, this type of study will never give the answer to whether this hypothesis has a valid basis. Only when investigating genes, environmental exposures, and the timing of these environmental stimuli will we understand whether asthma and COPD have similar, different, or both similar and different underlying genetic and environmental factors. At this time we can make a (small) step forward, because we have increased our knowledge on both genetic and environmental factors for asthma and COPD development.
ENVIRONMENTAL RISK FACTORS FOR ASTHMA AND COPD In the search for risk factors for asthma and COPD, a distinction can be made between host factors (genetic predisposition, sex) and environmental factors (smoking, air pollution). Many studies have tried to assess risk factors of asthma and found evidence that, for example, atopy (4), hyperresponsiveness (5), (passive) smoking (6, 7), air pollution (8), and respiratory tract
Pulmonary Perspective
infections (9) could be considered as single risk factors. There are additional protective factors, such as breastfeeding (10), maternal diet (11), and farming conditions (12). Smoking is the predominant risk factor for development of COPD. However, recent studies have shown that there are a considerable number of people who develop COPD without having smoked cigarettes (13). This signifies that indoor and outdoor air pollution (14) and other environmental triggers, such as maternal smoking (15, 16), may be important as well. As for asthma, airway hyperresponsiveness (AHR) and low lung function are important determinants of COPD development (17). Table 1 shows an overview of common and different environmental risk factors of asthma and COPD. Of interest, host factors such as hyperresponsiveness, family history of asthma, and low lung function are common risk factors for asthma and COPD, as are environmental stimuli such as environmental tobacco smoke and air pollution. It is difficult in this respect to dissect whether maternal smoking during pregnancy, and parental smoking during early childhood confer separate risks. Hence, many studies report on environmental tobacco smoke (ETS) exposure in general (Figure 1).
SINGLE CANDIDATE GENE ASSOCIATION STUDIES Candidate genes are generally selected for their known biological function, differential expression in tissues or cells involved in the pathogenesis of a disease, and/or based on findings in relevant animal models. Association studies aim to show that affected individuals in a population are more likely to have a particular variant of a gene than healthy controls in the same population. Association between the gene variant(s) and disease may imply causality. However, association can also occur if the allele is in linkage disequilibrium with another polymorphism in the same or a nearby gene that is the real causative polymorphism, or in the case of population admixture. Even discrepant findings may not exclude a gene to be important in disease development. In atopy, for instance, one allele in the CD14 gene has been reported as a risk for disease in one study and as protective in another study. Although this initially was interpreted as nonreplication of a gene, it later became apparent that other environmental levels of exposure may underlie the discrepancy (18). Asthma
There are at least 1,000 papers published examining SNPs in genes that are candidates for asthma and allergy. Although
1589
many of these genes have not been replicated, which is needed to reflect whether finding of this gene is a true observation, there is a group that is replicated many times: ADAM33, ADRB2, CD14, FCER1B, HLA-DRB1, HLA-DQB1, IL4, IL13, IL4RA, and TNF (19). Meta-analyses do not always find these genes as being significantly associated with asthma, but when comparing different meta-analyses and large replication studies, ADAM33, IL13, IL4RA, TNF, and TBXA2R appear as consistent genes and may represent common major asthma genes (19). Because multiple interactions between genes may occur in disease development, it is important to perform statistical interaction analyses between genes in biologically plausible pathways of asthma development. Nevertheless, the number of studies actually investigating gene–gene interactions in pathways so far is limited. The Toll-like receptor–related pathway is such a pathway (including CD14) and was investigated in more than 3,000 children (20). Several genes in this pathway were associated with atopy and/or asthma as a single gene, such as IL1RL1 (also found with GWAS), BPI, NOD1, NOD2, and MAP3K7IP1 (20). Of interest, multifactor dimensionality reduction analysis showed novel, significant gene–gene interactions in association with atopy and asthma. IL1RL1 and TLR4 significantly interacted for their effect on specific IgE to indoor allergens and IRAK1, NOD1, and MAP3K7IP1 with asthma (20). An important finding was that an SNP in a gene located in this pathway may not be associated with asthma on its own, but the SNP does so in interaction with other SNPs in genes in this pathway. COPD
Candidate genes involved in established pathogenetic pathways have been investigated for their association with COPD (i.e., oxidative stress, protease–antiprotease imbalance, chemokines, cytokines, and extracellular matrix breakdown and repair). COPD results from accelerated lung function decline; thus it is plausible to investigate genes in association with accelerated lung function decline in general populations. Some candidate genes have been identified in this way, such as ADRB2, CHRNA5, CSF3, EPHX1, IL1RN/IL1B, IL4R, IL6, IL8, IL10, INFg, ADAM33, MMP1, GSTP1, GSTT1, GSTM1, HMOX1, and SERPINA1 (21–26). An additional list of genes has been associated with COPD in case-control studies, wherein a COPD diagnosis was based on FEV1/FVC less than 70% and FEV1 less than 80% predicted, or less than 75% predicted. These genes involve, among others, EPHX1, GSTM1, GSTO2, HMOX1, MMP12, SERPINA1,
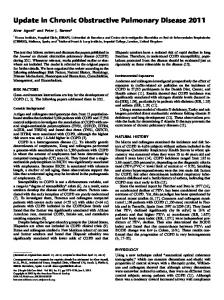
Figure 1. Graph representing lung development, lung growth, and decline in interaction with genetic and environmental factors. Green line represents normal lung development, growth, and decline; orange line represents abnormal prenatal lung development and growth; red line represents abnormal lung decline due to (environmental) tobacco smoke (E)TS exposure. COPD 5 chronic obstructive pulmonary disease.
1590
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
VOL 183
2011
TABLE 1. RISK FACTORS FOR ASTHMA AND CHRONIC OBSTRUCTIVE PULMONARY DISEASE Asthma Host factors
Perinatal factors
Environmental exposures in childhood
Environmental exposures in adulthood
COPD
Male sex childhood, female sex in adulthood (68) (Family) history of asthma (71) Genetic constitution Airway hyperresponsiveness (5) Atopy (4) Low lung function (69) Overweight (70) Maternal smoking (72) Maternal diet (11) Mode of delivery (73) No breastfeeding (10) Viral respiratory infections (9) Microbial deprivation (12) Environmental tobacco smoke exposure (6) Air pollution (74) Occupational exposures (75) Cigarette smoking (7) Outdoor air pollution (8)
Family history of COPD Family history asthma/atopy (71) Genetic constitution Airway hyperresponsiveness (17, 71) Low lung function (17)
Maternal smoking (72)
Lower respiratory tract infections (13, 71) Maternal smoking (16) Indoor air pollution (13) Occupational exposures (13) Cigarette smoking (71) Outdoor air pollution (8) Indoor air pollution (13)
Definition of abbreviation: COPD 5 chronic obstructive pulmonary disease.
SERPINE2, SFTPB, SMOC2, TGFB1, and TNF (27). However, recent meta-analyses on published candidate gene studies on COPD using strict and well-defined criteria to include studies showed that there are only a few genes reaching statistical significance for their association with COPD, namely: GSTM1, TGFB1, TNF, SOD3, IL1RN, VNTR, TNFA, GSTP1, and EPHX1 (27, 28) (http://caes.webfactional.com/copddb/ copd). It is of interest to note that these genes are positioned in biologically plausible pathways of oxidative stress response and defense against oxidative stress, like GSTM1, TGFB1, TNF, SOD3, TNFA, GSTP1, and EPHX1. These studies have provided insight into genetic susceptibility to COPD. So far the only environmental factor studied substantially in relation to COPD is smoking, and lately the role of gene-bysmoking interaction has received attention. More recently, gene–environmental interaction was expanded to nutritional factors. Higher vitamin C intake has been reported to be associated with better lung function. It was shown that for every level of vitamin C intake, lung function was worse if smokers had an SNP in the GCL gene, a detoxifying gene associated with COPD in two cohorts (29). Individuals with the variant in the GCL gene and the lowest vitamin C intake had the lowest lung function in the general population. COPD encompasses small airway disease, emphysema, and airway obstruction with chronic bronchitis. It is therefore not surprising that different GWAS on COPD merely defined by the severity of airway obstruction (e.g., FEV1 % predicted , 70%) usually do not find identical genetic variants. This is probably because genes associated with small airway fibrosis are likely different from genes determining emphysema. Moreover, some patients with COPD show evidence for both emphysema and small airway obstruction. It is now widely acknowledged that COPD is a heterogeneous disease (30). Some patients with COPD may have predominantly cough and phlegm, and others may have dyspnea (on exertion); some patients express predominantly emphysema, others express airway disease or any combination. It can be envisaged that these disease phenotypes are different in their genetic origins and constitute unique diseases. Thus, genetic GWAS only analyzing lung function as a COPD phenotype will not dissect the full spectrum, and many genes will go undetected that are relevant for emphysema, chronic mucous hypersecretion, or small airway disease. Also,
GWAS encompassing patients with all different subphenotypes may dissect the overlapping genes, just as is aimed for with asthma and COPD. Table 2 shows the current data available with respect to candidate genes associated with accelerated lung function decline in the general population and COPD defined by lung function criteria, emphysema on CT, and airway wall changes on CT. We have also included information on the association with asthma of these candidate genes. Asthma and COPD
Common genes identified for both asthma and COPD using single candidate association studies are ADRB2, GSTM1, GSTP1, IL13, TGFB1, and TNF. This so far limited list of candidate genes underlying both asthma and COPD might be extended in the near future, because some genes identified in COPD have not been studied yet in asthma (e.g., SERPINA2) or too few studies have been performed up to now trying to replicate genes associated with asthma in COPD, and the other way around.
TABLE 2. GENES ASSOCIATED WITH DIFFERENT PHENOTYPES OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE AND WITH ASTHMA Gene ADRB2 CHRNA3 EPHX1 GSTP1 HMOX1 SERPINE2 TGFB1 TNFa
FEV1 COPD: COPD: CT: Airway Decline Lung Function CT Emphysema Wall Thickening Asthma 1 NT 1* 1 1* NT — —
— 1* 1* 1 1 1* 1* 1*
— 1 1† 1 1 1 # #
1 NT 1 — NT 1 1 NT
1 NT — 1 — NT 1 1
Definition of abbreviations: COPD 5 chronic obstructive pulmonary disease; CT 5 computed tomography; NT 5 not tested. Data from References 59–61, 70, 71. * Replicated genetic finding. † Loose replication because different Reference SNP (rs) numbers were associated. # Marginally associated, likely due to small sample sizes.
Pulmonary Perspective
LINKAGE ANALYSIS AND POSITIONAL CLONING In diseases wherein the underlying biochemical or physiological disorder is unknown, linkage analysis is one of the methods used to identify novel genes. Linkage analysis is performed in families, preferably in families with many members. A set of polymorphic markers is spread out over the entire genome and their linkage (i.e., coinheritance) with a trait is tested. For example, it is tested whether a certain marker allele located on chromosome 5q that is present in a proband with asthma is also present in offspring with asthma and not in offspring without asthma. Asthma
In 1996 the first genome-wide search for asthma susceptibility genes was presented and showed six potential linkages (31). Twenty-two different linkage studies for asthma or its related phenotypes have been performed in populations across the world (32). Although the results are difficult to compare due to the use of different phenotypes, markers, and P values, they show consistent results in some regions (i.e., chromosome 5q, 6p, 11q, 12q, 13q, and 21q) (33). By this method several genes have been identified, for example ADAM33, DPP10, GPRA, HLA-G, PHF11, PTGDR, PLAUR, and PCDH1 (31, 33–37). Despite these successes, linkage studies are performed less frequently, because they are time consuming and expensive and their power is limited. Of importance, meta-analyses of linkage studies have replicated loci associated with AHR, but not with asthma, suggesting this is due to heterogeneity of asthma as a disease (32). COPD
One genome scan linkage study has been published in COPD, performed in the Boston Early-Onset COPD Study, showing that chromosomes 2q, 12p, and 19q are likely locations of COPD susceptibility genes (38). Asthma and COPD
Because only one linkage study has been published in COPD, looking for overlap in chromosomal regions that are linked to both asthma and COPD is of limited value, and available studies showed no overlap whatsoever.
GWAS GWAS are applied to identify novel genetic variants that are associated with disease. Contrary to candidate gene approaches, GWAS are hypothesis-free, because the markers that are set throughout the genome are merely used to identify loci associated with the disease and are not selected based on their assumed biological function (39). On the basis of phase I HapMap data, it was shown that approximately 500,000 of these markers are required to capture all common SNPs in human populations (40). Current technologies can evaluate more than 1,000,000 SNPs simultaneously, interrogating the entire genome in one assay. Asthma
To date, several GWAS have been performed on asthma. The first GWAS on asthma identified a region on 17q12-12 including the genes ORMDL3 and GSDMB (41). Several genes were identified in this linkage block, and still it has not been fully elucidated which SNP in this region is the culprit of the association with asthma. ORMDL3 was suggested to be important because gene expression studies in Epstein-Barr Virustransformed lymphoblastoid B-cell–derived cell lines showed transcript levels from ORMDL3 to be associated with disease-
1591
associated markers on the genome (41). Subsequent studies have replicated the association between rs7216389 and childhood asthma in ethnically diverse populations (42). Functional studies revealed that the asthma-associated haplotype affects nucleosome distribution and that this regulatory region governs the transcriptional activity of at least three genes (ZPBP2, GSDMB, and ORMDL3) in the chromosome 17q12-q21 region (43). The recently published large GWAS on asthma of the Gabriel consortium found rs2305480 at the ORMDL3/GSDMB locus to be specifically associated with childhood-onset asthma (44). This study reported additional genome-wide significant associations with asthma for rs3771166 within the IL18R1 gene, a gene in linkage disequilibrium with IL1RL1, where significant association was found with several polymorphisms: rs9273349 in the HLA-DQ region; rs1342326 flanking IL33; rs744910 within the SMAD3 gene; and rs2284033 within IL2RB. Other genes or gene regions previously identified by GWAS are DENND1B at chromosome 1q, IL1RL1 at 2q12, HLA-Dr/DQ region at 5q, PDE4D at 5q12, RAD50-IL13 region on chromosome 5q, WDR36 at 5q22, TLE4 at 9q21.31, and MYB at 6q23 (44–49). Furthermore a GWAS in a population from African ancestry showed DPP10 (2q), PRNP at 20pter-p12 and ADRA1B (5q) to be significantly associated with asthma, without replication in European populations, although DPP10 had been found with positional cloning in previous studies (50). COPD
The two reported GWAS on COPD identified variants in the nicotinic acetylcholine receptors (nAChR) subunit genes such as CHRNA3/5 and CHRNB3/4 (51, 52). These SNPs have been associated cross-sectionally with nicotine dependency and smoking status. Other studies have found a cross-sectional association of the same variants with the level of lung function and COPD (defined by airway obstruction) and lung cancer (51–53). The gene is associated with the presence and severity of emphysema as well, an association independent of packyears. Therefore, it was suggested that the nAChR cluster is causally involved in alveolar destruction as a potentially shared pathogenic mechanism in lung cancer and COPD. However, because this gene is also associated with nicotine addiction and smoking is a risk factor for COPD itself, it is not clear from these cross-sectional studies whether the effect of the nAChR variants determine COPD development directly or indirectly via smoking addiction. Longitudinal analyses on the association of the nAChR variants with changes in smoking habits and course of lung function will be needed to elucidate whether the gene is involved in lung function loss per se, as suggested, or only through the effects of nicotine addiction. Asthma and COPD
So far, no common genes have been identified for both asthma and COPD using GWAS. This might be due to a number of reasons, the first one being that the number of GWAS so far is relatively limited, specifically in COPD. A second, more theoretical explanation for the lack of overlap might be the nature of most GWAS performed so far, which focus on one disease outcome (e.g., either on asthma or COPD) in populations that are specifically selected to study these outcomes. Comparing the top hits of these distinct GWAS in different populations may not constitute the most appropriate way to study shared genes in a GWA approach. A more fruitful method might be searching for shared genetics of asthma and COPD by performing a GWAS in one underlying population, which includes both individuals with asthma and those with COPD.
1592
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
THE GENETICS OF LUNG FUNCTION: OVERLAP WITH ASTHMA OR COPD? The trajectory of lung function growth appears to be established early in life. Genes involved in lung development together with in utero exposures may have important implications for lung function later in life and may influence the development of asthma and COPD. Genes differentially expressed during in utero airway development, such as Wnt signaling genes, have been shown to be associated with impaired lung function in children with asthma (54). In addition, decreased Wnt signaling /b-catenin activity was found in COPD in humans and during COPD/emphysema development in mice (55). Two large GWAS in the general population, studying individuals with predominantly normal lung function, suggest several novel genes related to FEV1 and FEV1/FVC ratio (56, 57). The number one locus identified in these two papers was near HHIP. It is of interest that HHIP was previously identified in two GWA papers as a COPD susceptibility gene (51, 52). A number of other novel loci have been identified at different chromosomal locations, such as 4q24 (GSTCD), 2q35 (TNS1), 5q33 (HTR4), 6p21 (Ager), and 15q23 (THSD4) (56, 57). However, the Gabriel consortium found no evidence for these loci to influence susceptibility to asthma (44). A next step will be to assess whether genes that are associated with COPD are additionally associated with lung function at birth and/or growth during childhood and subsequent asthma development. This may then add further to the notion that common genetic and environmental factors contribute to asthma and COPD.
ASTHMA AND COPD: COMMON ORIGINS? So far GWA studies in asthma and COPD have not identified overlapping genes, suggesting that these diseases have—at least in part—a unique genetic setup. Yet, there are examples from the candidate-gene approach that may illustrate a genetic overlap in asthma and COPD (see Table E1 and Figure E1 in the online supplement for an overview). These overlapping genes include ADAM33, GSTM1, GSTP1, IL13, TGFb, and TNF. Examples like ADAM33 and members of the GST family are of interest because they have been implicated in both lung function growth in childhood and lung function decline in adulthood. During lung development, ADAM33 is expressed in the mesenchymal progenitor cells that surround the primitive tubular airway structures (58). ADAM33 polymorphisms were associated with lung function in 3- to 5-year-old children (59) and interacted with in utero smoking on the development of low lung function and AHR (60). In adulthood, ADAM33 SNPs were associated with accelerated FEV1 decline in asthma (61) and the general population (62), which implied that the gene is a risk factor for the development of COPD in still-healthy subjects. The role of ADAM33 in COPD became even more apparent by results showing that a number of SNPs are also associated with the severity of AHR and airway inflammation in patients with COPD (63). Although the function of ADAM33 is still largely unknown, a recent study has indicated a role of a soluble ADAM33 variant in angiogenesis (64). The Glutathione S transferase (GST) genes are involved in detoxification pathways. This gene family consists of four members (designated A, M, P, and T), and each family member has several members. Whole gene deletions of GSTM1 and GSTT1 may result in impaired detoxification of toxic substances, such as those involved in air pollution and cigarette smoke. A study on 2,108 8-year-old children showed that genetic variation across the GST mu locus is associated with 8-year lung
VOL 183
2011
function growth. Importantly, children exposed to in utero smoking carrying GSTM2 risk alleles had lower lung function growth (65). In a subset of this cohort, GSTM1 and GSTP1 genotypes were associated with lung function growth in children (66). The GST genes are considered to play a role in the development of COPD as well, through their association with accelerated lung function decline in the general adult population (67).
CONCLUSIONS Multiple genes have been found for asthma and COPD. In addition to genes unique to these diseases, some shared genetic risk factors exist. Moreover, there are common host risk factors and environmental risk factors for asthma and COPD. Based on the data available, we put forward that genes that affect lung development in utero and lung growth in early childhood in interaction with environmental detrimental stimuli, such as smoking and air pollution, are contributing to asthma in childhood and the ultimate development of COPD (see Figure 1). Additional genes and environmental factors then drive specific immunological mechanisms that underlie asthma (like the Th2/ Th1 balance) and mechanisms that may determine asthma subphenotypes and others may contribute to the ultimate development of specific subtypes of COPD. In this respect it seems important to dissociate airway disease with mucous hypersecretion, small airway disease, and emphysema in COPD. The genetic predisposition to the derailment of certain pathways may further help to define subgroups of asthma and COPD. The next steps in genomics era will help to further unravel the common and disease-specific backgrounds of asthma and COPD (i.e., gene–gene and gene–environment interaction) on a genome-wide scale and gene regulation, such as epigenetics and modulations of gene expression and translation. In the end this may lead to stratification of patients by their genetic makeup and open new therapeutic prospects. Author Disclosure: D.S.P. received consultancy fees from AstraZeneca, Nycomed, GlaxoSmithKline, and Boehringer and serves on the advisory board for Teva. D.S.P. received lecture fees from Nycomed and GlaxoSmithKline. D.S.P. received grants from GlaxoSmithKline, Netherlands Asthma Foundation, and European Union. M.K. does not have a financial relationship with a commercial entity that has an interest in the subject of this manuscript. H.M.B. does not have a financial relationship with a commercial entity that has an interest in the subject of this manuscript. G.H.K. received lecture fees and a sponsored grant from GlaxoSmithKline. G.H.K. also received sponsored grants from Netherlands Asthma Foundation, European Union, and University Medical Center Groningen, the Netherlands.
References 1. Postma D, Koppelman G. Genetics of asthma: where are we and where do we go? Proc Am Thorac Soc 2009;6:283–287. 2. Koppelman GH, te Meerman GJ, Postma DS. Genetic testing for asthma. Eur Respir J 2008;32:775–782. 3. Postma DS, Boezen HM. Rationale for the Dutch hypothesis. Allergy and airway hyperresponsiveness as genetic factors and their interaction with environment in the development of asthma and COPD. Chest 2004;126:96S2104S. 4. Pearce N, Pekkanen J, Beasley R. How much asthma is really attributable to atopy? Thorax 1999;54:268–272. 5. Anto JM, Sunyer J, Basagana X, Garcia-Esteban R, Cerveri I, de Marco R, Heinrich J, Janson C, Jarvis D, Kogevinas M, et al. Risk factors of new-onset asthma in adults: a population-based international cohort study. Allergy 2010;65:1021–1030. 6. Strachan DP, Cook DG. Health effects of passive smoking. 6. Parental smoking and childhood asthma: longitudinal and case-control studies. Thorax 1998;53:204–212. 7. McLeish AC, Zvolensky MJ. Asthma and cigarette smoking: a review of the empirical literature. J Asthma 2010;47:345–361. 8. Brunekreef B, Forsberg B. Epidemiological evidence of effects of coarse airborne particles on health. Eur Respir J 2005;26:309–318.
Pulmonary Perspective 9. Busse WW, Lemanske RF Jr, Gern JE. Role of viral respiratory infections in asthma and asthma exacerbations. Lancet 2010;376: 826–834. 10. Scholtens S, Gehring U, Brunekreef B, Smit HA, de Jongste JC, Kerkhof M, Gerritsen J, Wijga AH. Breastfeeding, weight gain in infancy, and overweight at seven years of age: the prevention and incidence of asthma and mite allergy birth cohort study. Am J Epidemiol 2007;165:919–926. 11. Willers SM, Wijga AH, Brunekreef B, Kerkhof M, Gerritsen J, Hoekstra MO, de Jongste JC, Smit HA. Maternal food consumption during pregnancy and the longitudinal development of childhood asthma. Am J Respir Crit Care Med 2008;178:124–131. 12. Douwes J, Brooks C, Pearce N. Protective effects of farming on allergies and asthma: have we learnt anything since 1873? Expert Rev Clin Immunol 2009;5:213–219. 13. Salvi SS, Barnes PJ. Chronic obstructive pulmonary disease in nonsmokers. Lancet 2009;374:733–743. 14. Andersen ZJ, Hvidberg M, Jensen SS, Ketzel M, Loft S, Sorensen M, Tjonneland A, Overvad K, Raaschou-Nielsen O. Chronic obstructive pulmonary disease and long-term exposure to traffic-related air pollution: a cohort study. Am J Respir Crit Care Med 2011;183:455– 461. 15. Boy E, Bruce N, Delgado H. Birth weight and exposure to kitchen wood smoke during pregnancy in rural Guatemala. Environ Health Perspect 2002;110:109–114. 16. Svanes C, Sunyer J, Plana E, Dharmage S, Heinrich J, Jarvis D, DeMarco R, Norback D, Raherison C, Villani S, et al. Early life origins of chronic obstructive pulmonary disease. Thorax 2010;65: 14–20. 17. Postma DS, de Vries K, Koeter GH, Sluiter HJ. Independent influence of reversibility of air-flow obstruction and nonspecific hyperreactivity on the long-term course of lung function in chronic air-flow obstruction. Am Rev Respir Dis 1986;134:276–280. 18. Martinez FD. CD14, endotoxin, and asthma risk: actions and interactions. Proc Am Thorac Soc 2007;4:221–225. 19. Undarmaa S, Mashimo Y, Hattori S, Shimojo N, Fujita K, Miyatake A, Doi S, Kohno Y, Okamoto Y, Hirota T, et al. Replication of genetic association studies in asthma and related phenotypes. J Hum Genet 2010;55:342–349. 20. Reijmerink NE, Bottema RW, Kerkhof M, Gerritsen J, Stelma FF, Thijs C, van Schayck CP, Smit HA, Brunekreef B, Koppelman GH, et al. TLR-related pathway analysis: novel gene-gene interactions in the development of asthma and atopy. Allergy 2010;65:199–207. 21. Molfino NA. Genetic predisposition to accelerated decline of lung function in COPD. Int J Chron Obstruct Pulmon Dis 2007;2:117–119. 22. He J, Shumansky K, Connett JE, Anthonisen NR, Pare´ PD, Sandford AJ. Association of genetic variations in the CSF2 and CSF3 genes with lung function in smoking-induced COPD. Eur Respir J 2008;32: 25–34. 23. Joos L, McIntyre L, Ruan J, Connett JE, Anthonisen NR, Weir TD, Pare PD, Sandford AJ. Association of IL-1beta and IL-1 receptor antagonist haplotypes with rate of decline in lung function in smokers. Thorax 2001;56:863–866. 24. He J, Connett JE, Anthonisen NR, Sandford AJ. Polymorphisms in the IL13, IL13RA1, and IL4RA genes and rate of decline in lung function in smokers. Am J Respir Cell Mol Biol 2003;28:379–385. 25. He JQ, Foreman MG, Shumansky K, Zhang X, Akhabir L, Sin DD, Man SF, DeMeo DL, Litonjua AA, Silverman EK, et al. Associations of IL6 polymorphisms with lung function decline and COPD. Thorax 2009;64:698–704. 26. van Diemen C, Postma D, Vonk J, Bruinenberg M, Schouten J, Boezen HM. A disintegrin and metalloprotease 33 polymorphisms and lung function decline in the general population. Am J Respir Crit Care Med 2005;172:329–333. 27. Castaldi PJ, Cho MH, Cohn M, Langerman F, Moran S, Tarragona N, Moukhachen H, Venugopal R, Hasimja D, Kao E, et al. The COPD genetic association compendium: a comprehensive online database of COPD genetic associations. Hum Mol Genet 2010;19: 526–534. 28. Smolonska J, Wijmenga C, Postma DS, Boezen HM. Meta-analyses on suspected COPD genes: a summary of 20 years’ research. Am J Respir Crit Care Med 2009;180:618–631. 29. Siedlinski M, Postma D, van Diemen C, Blokstra A, Smit H, Boezen HM. Lung function loss, smoking, vitamin C intake, and polymorphisms of the glutamate-cysteine ligase genes. Am J Respir Crit Care Med 2008;178:13–19.
1593 30. Rennard SI, Vestbo J. The many ‘‘small COPDs’’: COPD should be an orphan disease. Chest 2008;134:623–627. 31. Daniels SE, Bhattacharrya S, James A, Leaves NI, Young A, Hill MR, Faux JA, Ryan GF, le Souef PN, Lathrop GM, et al. A genome-wide search for quantitative trait loci underlying asthma. Nature 1996;383: 247–250. 32. Bouzigon E, Forabosco P, Koppelman GH, Cookson WO, Dizier MH, Duffy DL, Evans DM, Ferreira MA, Kere J, Laitinen T, et al. Metaanalysis of 20 genome-wide linkage studies evidenced new regions linked to asthma and atopy. Eur J Hum Genet 2010;18:700–706. 33. Bouzigon E, Corda E, Aschard H, Dizier MH, Boland A, Bousquet J, Chateigner N, Gormand F, Just J, Le Moual N, et al. Effect of 17q21 variants and smoking exposure in early-onset asthma. N Engl J Med 2008;359:1985–1994. 34. Van EP, Little RD, Dupuis J, Del Mastro RG, Falls K, Simon J, Torrey D, Pandit S, McKenny J, Braunschweiger K, et al. Association of the ADAM33 gene with asthma and bronchial hyperresponsiveness. Nature 2002;418:426–430. 35. Zhang Y, Leaves NI, Anderson GG, Ponting CP, Broxholme J, Holt R, Edser P, Bhattacharyya S, Dunham A, Adcock IM, et al. Positional cloning of a quantitative trait locus on chromosome 13q14 that influences immunoglobulin E levels and asthma. Nat Genet 2003;34: 181–186. 36. Barton SJ, Koppelman GH, Vonk JM, Browning CA, Nolte IM, Stewart CE, Bainbridge S, Mutch S, Rose-Zerilli MJ, Postma DS. PLAUR polymorphisms are associated with asthma, PLAUR levels and lung function decline. J Allergy Clin Immunol 2009;123:1406–1415. 37. Koppelman G, Meyers D, Howard T, Zheng SL, Hawkins G, Ampleford E, Xu J, Koning H, Bruinenberg M, Nolte I, et al. Identification of PCDH1 as a novel susceptibility gene for bronchial hyperresponsiveness. Am J Respir Crit Care Med 2009;180:929–935. 38. Silverman EK, Mosley JD, Palmer LJ, Barth M, Senter JM, Brown A, Drazen JM, Kwiatkowski DJ, Chapman HA, Campbell EJ, et al. Genome-wide linkage analysis of severe, early-onset chronic obstructive pulmonary disease: airflow obstruction and chronic bronchitis phenotypes. Hum Mol Genet 2002;11:623–632. 39. Boezen HM. Genome-wide association studies: what do they teach us about asthma and chronic obstructive pulmonary disease? Proc Am Thorac Soc 2009;6:701–703. 40. The International HapMap Consortium. A haplotype map of the human genome. Nature 2005;437:1299–1320. 41. Moffatt M, Kabesch M, Liang L, Dixon A, Strachan D, Heath S, Depner M, von Berg A, Bufe A, Rietschel E, et al. Genetic variants regulating ORMDL3 expression contribute to the risk of childhood asthma. Nature 2007;448:470–473. 42. Halapi E, Gudbjartsson DF, Jonsdottir GM, Bjornsdottir US, Thorleifsson G, Helgadottir H, Williams C, Koppelman GH, Heinzmann A, Boezen HM, et al. A sequence variant on 17q21 is associated with age at onset and severity of asthma. Eur J Hum Genet 2010;18:902–908. 43. Verlaan DJ, Berlivet S, Hunninghake GM, Madore AM, Larivie`re M, Moussette S, Grundberg E, Kwan T, Ouimet M, Ge B, et al. Allelespecific chromatin remodeling in the ZPBP2/GSDMB/ORMDL3 locus associated with the risk of asthma and autoimmune disease. Am J Hum Genet 2009;85:377–393. 44. Moffatt MF, Gut IG, Demenais F, Strachan DP, Bouzigon E, Heath S, von Mutius E, Farrall M, Lathrop M, Cookson WO. GABRIEL Consortium. A large-scale, consortium-based genomewide association study of asthma. N Engl J Med 2010;363:1211–1221. 45. Sleiman P, Flory J, Imielinski M, Bradfield J, Annaiah K, Willis-Owen S, Wang K, Rafaels N, Michel S, Bonnelykke K, et al. Variants of DENND1B Associated with Asthma in Children. N Engl J Med 2010; 362:36–44. 46. Li X, Howard T, Zheng S, Haselkorn T, Peters S, Meyers D, Bleecker E. Genome-wide association study of asthma identifies RAD50–IL13 and HLA-DR/DQ regions. J Allergy Clin Immunol 2010;125:328–335. 47. Himes B, Hunninghake G, Baurley J, Rafaels N, Sleiman P, Strachan D, Wilk J, Willis-Owen S, Klanderman B, Lasky-Su J, et al. Genomewide association analysis identifies PDE4D as an asthma-susceptibility gene. Am J Hum Genet 2009;84:581–593. 48. Gudbjartsson D, Bjornsdottir U, Halapi E, Helgadottir A, Sulem P, Jonsdottir G, Thorleifsson G, Helgadottir H, Steinthorsdottir V, Stefansson H, et al. Sequence variants affecting eosinophil numbers associate with asthma and myocardial infarction. Nat Genet 2009;18: 902–908. 49. Hancock DB, Romieu I, Shi M, Sienra-Monge JJ, Wu H, Chiu GY, Li H, del Rio-Navarro BE, Willis-Owen SA, Weiss ST, et al. Genome-wide
1594
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
association study implicates chromosome 9q21.31 as a susceptibility locus for asthma in Mexican children. PLoS Genet 2009;5:e1000623. Mathias R, Grant A, Rafaels N, Hand T, Gao L, Vergara C, Tsai Y, Yang M, Campbell M, Foster C, et al. A genome-wide association study on African-ancestry populations for asthma. J Allergy Clin Immunol 2010;125:336–346. Pillai SG, Ge D, Zhu G, Kong X, Shianna KV, Need AC, Feng S, Hersh CP, Bakke P, Gulsvik A, et al. A genome-wide association study in chronic obstructive pulmonary disease (COPD): identification of two major susceptibility loci. PLoS Genet 2009;5:e1000421. Cho M, Boutaoui N, Klanderman B, Sylvia J, Ziniti J, Hersh C, DeMeo D, Hunninghake G, Litonjua A, Sparrow D, et al. Variants in FAM13A are associated with chronic obstructive pulmonary disease. Nat Genet 2010;42:200–202. Wang JC, Cruchaga C, Saccone NL, Bertelsen S, Liu P, Budde JP, Duan W, Fox L, Grucza RA, Kern J, et al. COGEND collaborators and GELCC collaborators. Risk for nicotine dependence and lung cancer is conferred by mRNA expression levels and amino acid change in CHRNA5. Hum Mol Genet 2009;18:3125–3135. Sharma S, Tantisira K, Carey V, Murphy AJ, Lasky-Su J, Celedon JC, Lazarus R, Klanderman B, Rogers A, Soto-Quiros M, et al. A role for Wnt signaling genes in the pathogenesis of impaired lung function in asthma. Am J Respir Crit Care Med 2010;181:328–336. Kneidinger N, Yildirim AO, Callegari J, Takenaka S, Stein MM, Dumitrascu R, Bohla A, Bracke KR, Morty RE, Brusselle GG, et al. Activation of the WNT/fbetag-catenin pathway attenuates experimental emphysema. Am J Respir Crit Care Med (In press) Repapi E, Sayers I, Wain L, Burton P, Johnson T, Obeidat M, Zhao J, Ramasamy A, Zhai G, Vitart V, et al. Genome-wide association study identifies five loci associated with lung function. Nat Genet 2010;42: 36–44. Hancock D, Eijgelsheim M, Wilk J, Gharib S, Loehr L, Marciante K, Franceschini N, van Durme Y, Chen T, Barr RG, et al. Meta-analyses of genome-wide association studies identify multiple loci associated with pulmonary function. Nat Genet 2010;42:45–52. Haitchi HM, Bassett DJ, Bucchieri F, Gao X, Powell RM, Hanley NA, Wilson DI, Holgate ST, Davies DE. Induction of a disintegrin and metalloprotease 33 during embryonic lung development and the influence of IL-13 or maternal allergy. J Allergy Clin Immunol 2009;124:590–597, 597.e1–11. Simpson A, Maniatis N, Jury F, Cakebread JA, Lowe LA, Holgate ST, Woodcock A, Ollier WE, Collins A, Custovic A, et al. Polymorphisms in a disintegrin and metalloprotease 33 (ADAM33) predict impaired early-life lung function. Am J Respir Crit Care Med 2005;172:55–60. Reijmerink NE, Kerkhof M, Koppelman GH, Gerritsen J, de Jongste JC, Smit HA, Brunekreef B, Postma DS. Smoke exposure interacts with ADAM33 polymorphisms in the development of lung function and hyperresponsiveness. Allergy 2009;64:898–904. Jongepier H, Boezen HM, Dijkstra A, Howard TD, Vonk JM, Koppelman GH, Zheng SL, Meyers DA, Bleecker ER, Postma DS. Polymorphisms of the ADAM33 gene are associated with accelerated lung function decline in asthma. Clin Exp Allergy 2004;34:757–760. van Diemen CC, Postma DS, Aulchenko YS, Snijders PJLM, Oostra BA, van Duijn CM, Boezen HM. Novel strategy to identify genetic
63.
64.
65.
66.
67.
68. 69.
70.
71.
72.
73.
74.
75.
VOL 183
2011
risk factors for COPD severity: a genetic isolate. Eur Respir J 2010;35: 768–775. Gosman MM, Boezen HM, van Diemen CC, Snoeck-Stroband JB, Lapperre TS, Hiemstra PS, Ten Hacken NH, Stolk J, Postma DS. A disintegrin and metalloprotease 33 and chronic obstructive pulmonary disease pathophysiology. Thorax 2007;62:242–247. Puxeddu I, Pang YY, Harvey A, Haitchi HM, Nicholas B, Yoshisue H, Ribatti D, Clough G, Powell RM, Murphy G, et al.. The soluble form of a disintegrin and metalloprotease 33 promotes angiogenesis: implications for airway remodeling in asthma. J Allergy Clin Immunol 2008;121:1400–1406, 1406.e1–4. Breton CV, Vora H, Salam MT, Islam T, Wenten M, Gauderman WJ, Van den Berg D, Berhane K, Peters JM, Gilliland FD. Variation in the GST mu locus and tobacco smoke exposure as determinants of childhood lung function. Am J Respir Crit Care Med 2009;179:601– 607. Gilliland FD, Gauderman WJ, Vora H, Rappaport E, Dubeau L. Effects of glutathione-S-transferase M1, T1, and P1 on childhood lung function growth. Am J Respir Crit Care Med 2002;166:710– 716. Imboden M, Downs SH, Senn O, Matyas G, Brandli O, Russi EW, Schindler C, Ackermann-Liebrich U, Berger W, Probst-Hensch NM; SAPALDIA Team. Glutathione S-transferase genotypes modify lung function decline in the general population: SAPALDIA cohort study. Respir Res 2007;8:2. McCallister JW, Mastronarde JG. Sex differences in asthma. J Asthma 2008;45:853–861. Haland G, Carlsen KC, Sandvik L, Devulapalli CS, Munthe-Kaas MC, Pettersen M, Carlsen KH. ORAACLE. Reduced lung function at birth and the risk of asthma at 10 years of age. N Engl J Med 2006;355: 1682–1689. Scholtens S, Wijga A, Seidell J, Brunekreef B, de Jongste J, Gehring U, Postma D, Kerkhof M, Smit H. Overweight and changes in weight status during childhood in relation to asthma symptoms at 8 years of age. J Allergy Clin Immunol 2009;123:1312–1318. de Marco R, Accordini S, Marcon A, Cerveri I, Anto JM, Gislason T, Heinrich J, Janson C, Jarvis D, Kuenzli N, et al; European Community Respiratory Health Survey (ECRHS). Risk factors for chronic obstructive pulmonary disease in a European cohort of young adults. Am J Respir Crit Care Med (In press) Stein RT, Holberg CJ, Sherrill D, Wright AL, Morgan WJ, Taussig L, Martinez FD. Influence of parental smoking on respiratory symptoms during the first decade of life: the Tucson Children’s Respiratory Study. Am J Epidemiol 1999;149:1030–1037. Roduit C, Scholtens S, de Jongste JC, Wijga AH, Gerritsen J, Postma DS, Brunekreef B, Hoekstra MO, Aalberse R, Smit HA. Asthma at 8 years of age in children born by caesarean section. Thorax 2009;64: 107–113. Gehring U, Wijga AH, Brauer M, Fischer P, de Jongste JC, Kerkhof M, Oldenwening M, Smit HA, Brunekreef B. Traffic-related air pollution and the development of asthma and allergies during the first 8 years of life. Am J Respir Crit Care Med 2010;181:596–603. Malo JL, Chan-Yeung M. Agents causing occupational asthma. J Allergy Clin Immunol 2009;123:545–550.