Chronic Obstructive Pulmonary Disease Overview Epidemiology, Risk Factors, and Clinical Presentation Joan B. Soriano1 and Roberto Rodrı´guez-Roisin2 1
Fundacio´n Caubet-CIMERA Illes Balears, Bunyola, Spain; and 2Servei de Pneumologia, Institut del To´rax, Hospital Clı´nic, Institut d’Investigacions Biome´diques August Pi i Sunyer (IDIBAPS), Universitat de Barcelona, and Centro de Investigacio´n Biome´dica en Red de Enfermedades Respiratorias (CIBERES), Barcelona, Spain
Chronic obstructive pulmonary disease (COPD) has been a major public health problem during the 20th century, and will remain a challenge for the foreseeable future. Worldwide, COPD is in the spotlight, because its high prevalence, morbidity, and mortality create formidable challenges for healthcare systems. However, there remain many ongoing, contentious issues in COPD, including the definition and staging of COPD itself. Similarly, it appears that there is no consensus as yet on how, when, and where spirometry and other tools (symptoms assessment, imaging, biomarkers, and so on) should be conducted and implemented to screen, label, and treat for COPD, if any. Our current knowledge on the epidemiology, risk factors, and clinical presentation of COPD has been reasonably well documented in several previous reviews. We aim to summarize new developments surrounding the epidemiology of COPD, both at the population and at the clinical level, in comparison with other major burden contributors, while debating old and novel risk factors. Cigarette smoking is the principal causal factor, but other factors play a role in causing and triggering COPD. Likely, the clinical presentation of COPD and its contributing phenotypes within the remainder of the 21st century will be different than the ‘‘blue bloaters’’ and ‘‘pink puffers’’ observed one or two generations ago. Hopefully, the COPD clinical course will shift to better outcomes and prognosis than in the past. Keywords: chronic obstructive pulmonary disease; epidemiology; prevalence; smoking; trends
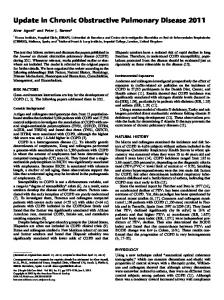
The epidemiology of chronic obstructive pulmonary disease (COPD), or the study of COPD and its determinants at the population level, aims to quantify the burden of COPD on society and to compare it with other diseases. There is indeed more interest in COPD now than ever before. Looking back at 50 years of research, the available 106 prevalence estimates from the 79 published COPD studies as of February 2011 are unevenly distributed (Figure 1). By plotting the year of publication of these studies, many with different methodologies and definitions, it can be seen that determining the size of the problem and the distribution of COPD did not engage investigators worldwide in the 1970s and 1980s. It is only from the mid-1990s, and especially at the turn of the century, that an outburst of publications produces a healthy cloud of dots. Describing, the epidemiology of any given disease is fundamental to reducing its burden. Despite the well established public health principle: ‘‘to measure a health problem is the first step to identify a strategy to tackle it,’’ the spread of the burden of COPD is and will remain a hot topic, as resources for any health
(Received in original form February 4, 2011; accepted in final form February 17, 2011) Supported by AstraZeneca. Correspondence and requests for reprints should be addressed to Joan B. Soriano, M.D., Ph.D., Director, Program of Epidemiology & Clinical Research, Fundacio´ Caubet-CIMERA Illes Balears, Recinte Hospital Joan March, Carretera Soller Km 12, 07110 Bunyola, Mallorca, Illes Balears, Spain. E-mail:
[email protected] Proc Am Thorac Soc Vol 8. pp 363–367, 2011 DOI: 10.1513/pats.201102-017RM Internet address: www.atsjournals.org
intervention are always limited, and they need to be used carefully. Many initiatives worldwide have aimed to better describe the epidemiology of COPD, including: the Global Burden of Disease (GBD) studies (1), the European Lung White Book (2), the Global Initiative for Chronic Obstructive Lung Disease (GOLD) (3), the Global Alliance Against Chronic Respiratory Diseases (4), and a number of field studies that will be listed subsequently here. There are already many, recent contributions summarizing the topics of this review, namely, the epidemiology of COPD, its risk factors, and clinical presentation (5–7). Furthermore, all major national and international COPD guidelines, both at the primary and specialized care levels, also include chapters on related topics, namely, the American Thoracic Society/European Respiratory Society (ATS/ERS) (8), GOLD (3), the International Primary Care Research Group (9), Spanish Society of Pulmonology and Thoracic Surgery/the Latin American Thoracic Society (10), and the United Kingdom-National Institute for Health and Clinical Excellence (UK-NICE) (11), among others. We therefore aim to summarize new developments surrounding the epidemiology of COPD, both at the population and at the clinical level, and also in comparison with other major burden contributors, while discussing old and novel risk factors, both contributing to feature the new face of COPD.
EPIDEMIOLOGY The highly cited, influential GBD studies estimated that COPD causes the death of at least 2.9 million people annually. Estimates of global mortality in 1990 (1) were updated in 2006 (12), and will be next available and expanded in 2011 (13). The GBD highlights that COPD was the sixth leading cause of death in 1990, has been the fourth since 2000, and is projected to be the third by 2020. These estimates are likely to be conservative, as they did not account for deaths where COPD is a contributory cause, although misclassification can be large (14). Subsequent to that date, even assuming the most pessimistic scenario regarding the global spread of human immunodeficiency/acquired immune deficiency virus, by 2030, COPD will be the direct underlying cause of 7.8% of all deaths, and represent 27% of deaths related with smoking, only surpassed by 33% for cancer and 29% by cardiovascular disease (15). Even the simplest of questions, ‘‘How many individuals are there in the World with COPD?’’ was surrounded by a halo of vagueness until very recently. Estimates varied by author and publication, and figures up to 600 million have been widely used, and are available elsewhere (16). It is agreed by consensus that an estimated number of 210 million people have COPD worldwide (Table 1) (4, 17). In the absence of population spirometry, and with a staggering 80–90% COPD underdiagnosis in all world regions and scenarios (18), this figure is useful, yet must be used with caution. Overall, the prevalence of COPD in the general population is estimated to be around 1% across all ages, rising steeply to 8–10% or higher among those aged 40 years or older (19). Both the Proyecto Latinoamericano de
364
PROCEEDINGS OF THE AMERICAN THORACIC SOCIETY VOL 8
2011
Figure 1. Prevalence surveys of chronic obstructive pulmonary disease (with varying definitions), by year of publication.
Investigacio´n en Obstruccio´n Pulmonar (20) and the Burden of Obstructive Lung Disease (BOLD) (21) initiatives have greatly expanded our knowledge on COPD distribution worldwide. Yet the former involved only five Latin American cities, whereas the latter, as of November 2010, has been completed in 21 centers worldwide plus 15 BOLD subsites in Australia, Canada, and China. There are many areas in the world, especially in Asia and Africa, with an absence of data—not only any type of spirometric data, but even rates of physician-diagnosed COPD, or the old terms, ‘‘chronic bronchitis’’ and ‘‘emphysema,’’ with all its intrinsic limitations. However, diseases change with time, and with an aging population (22) and countries transitioning within different stages of the tobacco epidemic (23), current estimates may need to be updated periodically. In contrast to asthma and other conditions, there is a lack of repeated surveys assessing time trends in COPD. Two recent, controversial studies are available from Spain and Finland (24, 25), and, when applying objective population spirometry, it appears that COPD prevalence might have plateaued or even decreased in certain countries. However surprising these conclusions might be, and whether these findings be real or confounded with methodological issues (26, 27), they indicate that perhaps subtle changes in the risk factors, or in the way in which we perform spirometry (apart from the aforementioned demographic changes), other factors being the same, make spirometry-based measurements difficult to compare over time. Of interest, the expected geographic homogeneity of COPD estimates (note that all Proyecto Latinoamericano de Investigacio´n en Obstruccio´n Pulmonar and BOLD estimates are from urban cities from different countries) might also be a complex issue. Also very recently, the EPIdemiologic Study of Copd in SpAiN (EPISCAN) study in Spain concluded that there were significant TABLE 1. ESTIMATED CURRENT PREVALENCE OF SELECTED RESPIRATORY CONDITIONS Condition COPD Smoking Rhinitis (excluding asthma) Asthma Sleep-disordered breathing disorders Other chronic respiratory diseases
Estimated No. 210 1.1 400 300 100 50
million billion million million million million
Definition of abbreviation: COPD 5 chronic obstructive pulmonary disease. Data obtained from References 4 and 17.
variations in the distribution of COPD in the 11 centers participating, up to threefold, either in prevalence or in underdiagnosis and undertreatment of COPD, and observed even within two nearby neighborhoods of Madrid (28). Current projections to 2030 indicate that, although major vascular diseases will remain leading causes of global disease burden, with human immunodeficiency/acquired immune deficiency virus the leading cause, diarrheal diseases and lower respiratory infections will be outranked by COPD, in part reflecting the projected increases in death and disability from tobacco use (29). These factors will be taken into account when producing GBD III estimates (13).
COPD DEFINITION Spirometry is the most common of the pulmonary function tests, and enables any health professional to make an objective measurement of airflow limitation and the degree to which it is reversible. As a diagnostic test for COPD, spirometry fulfills criteria of being a reliable, simple, noninvasive, safe, and inexpensive procedure to detect airflow limitation. It is envisaged that early diagnosis of COPD should have an impact on individual and population outcomes, including supporting smoking cessation and reducing societal burden of COPD. However, the thresholds to diagnose and stage COPD have been/are a major setback to many efforts, and medical societies disagree (18). It is of note that the updated NICE guidelines in 2010 have stepped back on using prebronchodilator spirometry alone (11), and now all major COPD guidelines, both at the primary and secondary levels, recommend the use of postbronchodilator spirometry (3, 8–11). To make things even less simple and more confounding, the historical debate on using a fixed ratio of FEV1:FVC less than 0.70 versus its lower limit of normal or other indices, remains a recurrent debate (30–33); it might appear that new evidence actually produces more gaps and more questions (32, 34), polarizing all positions. Perhaps learning how those in other medical specialties solved similar problems to define diabetes mellitus, arterial hypertension, or other concomitant disorders would be of help in the COPD definition saga (35).
RISK FACTORS There are comprehensive lists of risk factors associated with the development and triggering of COPD exacerbations, available
Soriano and Rodrı´guez-Roisin: COPD Epidemiology in the 21st Century
elsewhere (3, 8–11). Some of them are amenable to being modified, whereas others are not, and some apply at the individual and/or group level, so that, with all likelihood, any strategies to limit each burden will differ (36). However, the recent literature is packed with reports aimed at explaining COPD apart from smoking. Other than tobacco smoking, risk factors for developing COPD are being increasingly recognized (3), and include many other environmental exposures, such as occupational exposures to dust and fumes in the developed and developing countries (37), and indoor biomass fuel burning in many developing countries (38). Reduction of such exposures on a population basis or at an individual level might be worthwhile. Factors that seem to be less important in the development of COPD, although they may worsen disease, include outdoor pollutants and passive smoke exposure. A number of factors associated with COPD development may not currently be possible to modify; these include the aging lung, sex, comorbidities, and child or adult repeated respiratory infections. The bestknown genetic factor linked to COPD is a1-antitrypsin deficiency (a1-ATD), which arises in up to 3% of patients with COPD and, combined with smoking, increases the risk of panlobular emphysema (39). Several other genes have been implicated in COPD, but the consistency of their effect in the development of COPD is currently unproven. The one concomitant disorder consistently shown to be associated with COPD development is asthma, and it appears that people with asthma who smoke lose lung function more rapidly than individuals without asthma (40). Recent reports have also aimed at a direct link with tuberculosis (41). At this early stage, spirometry as a screening tool of disease has only been explored in a1-ATD probands and their relatives, smokers, and those workers with occupational exposures. Apart from marijuana consumers (42, 43) and biomass exposure in selected developing countries (44), it is unlikely that spirometry will prove to be a successful screener with other types of exposures. We believe that the current emphasis on nonsmoking COPD (45, 46) might distract many from the real problem. There are now more smokers worldwide than ever, and calculating the population-attributable fraction can be a tricky formula, and its interpretation misleading. A classical quote from the U.S. Surgeon General Reports is that ‘‘90% of COPD can be attributed to smoking’’ (47). However, recent studies have reduced these estimates to 44–45% only (48–50), and it is now suggested that, even in developed countries, cigarette smoking causes COPD in only 50–70% of patients (51). The population-attributable fraction of a given risk factor should only be estimated for causal factors, and the vast, available epidemiologic evidence is sufficient to infer a causal relationship between active smoking and COPD. The calculation of the population-attributable fraction of smoking in COPD is proportional to two factors: the relative risk of smoking in producing COPD (which should be constant and close to 10), and the prevalence of smoking in the population (which has been decreasing from 60% or higher in the 1940s to below 30% in many Western countries worldwide) (23). The elimination of smoking could largely prevent most COPD. Apart from COPDologists, all doctors can be considered public health practitioners as well, and tackling tobacco should be a continued priority. The damage done by tobacco and other types of smoking in the lungs and other tissues of the smoker, as well as in involuntary, passive smokers, has been extensively documented. It is our opinion that journal space, resources, and energy dedicated to nonsmoking COPD issues indirectly benefit the big tobacco industry (52). We agree that the diagnostic process should start, and not stop, at the point of a spirometric diagnosis of airflow limitation, as it is wrong to assume that individuals with airflow limitation who do not smoke are a case of nonsmoking COPD.
365
CLINICAL PRESENTATION OF COPD The clinical presentation of COPD is likely changing. After more than 200 years, its cardinal symptoms remain cough, phlegm, and dyspnea (53). In the 19th century, the diagnosis of COPD, formerly known as emphysema and bronchitis, depended on symptoms, signs of a hyperinflated chest, and reduced expiratory breath sounds. The airflow obstruction evident on spirometry was identified in that century, but did not enter into clinical practice until much later. Cigarette smoking only became recognized as its dominant cause in the last half of the 20th century. Yet the COPD-contributing phenotypes in the remainder of the 21st century will be different than the blue bloaters and pink puffers observed one or two generations ago (54). The evaluation of COPD phenotypes is an area of great interest, and determining their clinical outcomes and long-term consequences will need further examination (55). There is little controversy that spirometry must be part of the patient diagnosis and of the COPD definition. However, the growing evidence that COPD can clearly exist in the absence of airflow limitation, namely in patients with imaging evidence of emphysema, decreased diffusing capacity, but preserved forced spirometry, is of note. That said, in patients with COPD, the correlation of lung function with emphysema assessed via chest X-ray, high-resolution computed tomography, or other imaging tools is modest (56). In addition, a high proportion of people with restrictive spirometry may, in fact, be obstructive (57). There is now a plethora of multicomponent indices, apart from the original BODE (58) and all posterior modifications, including mBODE (that replaces 6-minute-walking distance [6MWD] for VO2) (59); e-BODE (BODE plus exacerbations) and BODE-x (that replaces exacerbations for 6MWD) (61); ADO (age, dyspnea, and FEV1) (61); the COPD Prognostic Index, made up of cardiovascular disease, FEV1, age, sex, BMI, and exacerbations (62); SAFE (SGRQ score, airflow limitation, and exercise tolerance; cardiovascular disease, FEV1, and 6MWD) (63); and DOSE (including dyspnea, smoking status, FEV1, and exacerbations [64]). It is likely that more multicomponent indices will be produced, shuffling some old or new variables. Survival of the fittest is considered a universal law in biology, and natural selection is a well documented method by which Mother Nature produces changes in living organisms (65). However, it could be considered that diseases also change with time, in size, as well as in face, subject to a changing environment, including less smoking, population aging, concomitant disorders, treatment with respiratory and nonrespiratory medications, or other. Indeed, a change to milder, younger clinical expressions at the population level has been documented in asthma (66), and close to zero emergency room admissions and hospitalizations due to asthma are reported in selected countries, such as Finland, Poland, and parts of Brazil (67, 68). The same can be already occurring with COPD in Finland, where a national COPD program is already yielding positive results, including a decrease in smoking and a reduction in both total number of hospitalization periods and hospitalization days due to COPD, as well as in the number of pensioners and daily sickness days due to COPD (69). The long-term prognosis after a COPD-related hospitalization appears improved at least in one study, likely due to a better management of COPD comorbidities (70).
FUTURE A number of investigators (71), societies, and nonprofit international initiatives have elegantly outlined some of the burning, pending questions in COPD, both for now and for the foreseeable future, with the intention of helping funding agencies either to
366
prioritize limited resources in competitive calls, or to streamline alternative routes to reduce the COPD burden. They include documents from the American Thoracic Society/European Respiratory Society (2, 72), Global Alliance Against Chronic Respiratory Diseases (4), GOLD (3), the International Primary Care Research Group (73), and NICE (71). Innovative ideas, more brainstorming, and close collaboration of respiratory physicians with primary care and internal medicine colleagues are winning formulas. Author Disclosure: J.B.S. acted as a consultant for and received travel accomodation from AtraZeneca, but does not have a financial relationship with a commercial entity that has an interest in the subject of this manuscript. R.R.-R. does not have a financial relationship with a commercial entity that has an interest in the subject of this manuscript. Acknowledgments: The authors express thanks to Professor A. Sonia Buist for forwarding Burden of Obstructive Lung Disease initiative updates and other related information, and to Professor Alan D. Lopez for comments in a previous version of the manuscript for this article.
References 1. Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet 1997;349:1498–1504. 2. European Respiratory Society. European lung white book. Huddersfield: European Respiratory Society Journals Ltd.; 2003. 3. Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, Calverley P, Fukuchi Y, Jenkins C, Rodriguez-Roisin R, van Weel C, et al.; Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med 2007;176:532–555. 4. Bousquet J, Khaltaev N. Global surveillance, prevention and control of chronic respiratory diseases: a comprehensive approach [updated 2007; accessed June 30, 2011]. Available from: http://www.who.int/ gard/publications/GARD%20Book%202007.pdf 5. Stockley RA, Mannino D, Barnes PJ. Burden and pathogenesis of chronic obstructive pulmonary disease. Proc Am Thorac Soc 2009;6: 524–526. 6. Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet 2007;370:765–773. 7. Chapman KR, Mannino DM, Soriano JB, Vermeire PA, Buist AS, Thun MJ, Connell C, Jemal A, Lee TA, Miravitlles M, et al. Epidemiology and costs of chronic obstructive pulmonary disease. Eur Respir J 2006; 27:188–207. 8. Celli BR, MacNee W. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J 2004;23:932–946. 9. Bellamy D. Bouchard J, Henrichsen S, Johansson G, Langhammer A, Reid J, van Weel C, Buist S. International Primary Care Respiratory Group (IPCRG) guidelines: management of chronic obstructive pulmonary disease (COPD). Prim Care Respir J 2006;15:48–57. 10. Peces-Barba G, Barbera` JA, Agustı´ A, Casanova C, Casas A, Izquierdo JL, Jardim J, Lo´pez Varela V, Monso´ E, Montemayor T, et al. Diagnosis and management of chronic obstructive pulmonary disease: joint guidelines of the Spanish Society of Pulmonology and Thoracic Surgery (SEPAR) and the Latin American Thoracic Society (ALAT) [in Spanish]. Arch Bronconeumol 2008;44:271–281. 11. O’Reilly J, Jones MM, Parnham J, Lovibond K, Rudolf M; Guideline Development Group. Management of stable chronic obstructive pulmonary disease in primary and secondary care: summary of updated NICE guidance. BMJ 2010;340:c3134. 12. Lopez AD, Shibuya K, Rao C, Mathers CD, Hansell AL, Held LS, Schmid V, Buist S. The Global Burden of COPD: future COPD projections. Eur Respir J 2006;27:397–412. 13. Murray CJ, Lopez AD, Black R, Mathers CD, Shibuya K, Ezzati M, Salomon JA, Michaud CM, Walker N, Vos T. Global burden of disease 2005: call for collaborators. Lancet 2007;370:109–110. 14. Jensen HH, Godtfredsen NS, Lange P, Vestbo J. Potential misclassification of causes of death from COPD. Eur Respir J 2006;28:781–785. 15. Mathers CD, Roncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med 2006;3:2011–2030. 16. International COPD Coalition. Quick facts about COPD [updated 2011; accessed June 30, 2011]. Available from: http://www.internationalcopd. org/materials/patients/learn/facts.aspx.
PROCEEDINGS OF THE AMERICAN THORACIC SOCIETY VOL 8
2011
17. Bousquet J, Kiley J, Bateman ED, Viegi G, Khaltaev N, Cruz AA. Prioritized research agenda for prevention and control of chronic respiratory diseases. Eur Respir J 2010;36:995–1001. 18. Soriano JB, Zielinski J, Price D. Screening for and early detection of chronic obstructive pulmonary disease. Lancet 2009 29;374:721–732. 19. Halbert RJ, Natoli JL, Gano A, Badamgarav E, Buist AS, Mannino DM. Global burden of COPD: systematic review and meta-analysis. Eur Respir J 2006;28:523–532. 20. Menezes AM, Perez-Padilla R, Jardim JR, Muino A, Lopez MV, Valdivia G, Montes de Oca M, Talamo C, Hallal PC, Victora CG; PLATINO Team. Chronic obstructive pulmonary disease in five Latin American cities (the PLATINO study): a prevalence study. Lancet 2005;366:1875–1881. 21. Buist AS, McBurnie MA, Vollmer WM, Gillespie S, Burney P, Mannino DM, Menezes AM, Sullivan SD, Lee TA, Weiss KB, et al.; BOLD Collaborative Research Group. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet 2007;370:741–750. 22. Christensen K, Doblhammer G, Rau R, Vaupel JW. Ageing populations: the challenges ahead. Lancet 2009;374:1196–208. 23. Shafey O, Erisksen M, Ross H, MacKay J. The tobacco atlas 2009, 3rd ed. Atlanta: American Cancer Society and the World Lung Foundation; 2009. 24. Soriano JB, Ancochea J, Miravitlles M, Garcı´a-Rı´o F, Duran-Tauleria E, Mun˜oz L, Jime´nez-Ruiz CA, Masa JF, Viejo JL, Villasante C, et al. Recent trends in COPD prevalence in Spain: a repeated crosssectional survey 1997–2007. Eur Respir J 2010;36:758–765. 25. Vasankari TM, Impivaara O, Helio¨vaara M, Heistaro S, Liippo K, Puukka P, Saarelainen S, Kanervisto M, Jousilahti P. No increase in the prevalence of COPD in two decades. Eur Respir J 2010;36:766–773. 26. Celli BR. The light at the end of the tunnel: is COPD prevalence changing? Eur Respir J 2010;36:718–719. 27. Cerveri I, De Marco R. What makes large epidemiological studies comparable? Eur Respir J 2010;36:720–721. 28. Soriano JB, Miravitlles M, Borderı´as L, Duran-Tauleria E, Garcı´a Rı´o F, Martı´nez J, Montemayor T, Mun˜oz L, Pin˜eiro L, Sa´nchez G, et al. Geographical variations in the prevalence of COPD in Spain: relationship to smoking, death rates and other determining factors [in Spanish]. Arch Bronconeumol 2010;46:522–530. 29. Lopez AD, Mathers CD. Measuring the global burden of disease and epidemiological transitions: 2002–2030. Ann Trop Med Parasitol 2006; 100:481–499. 30. Celli BR, Halbert RJ. Point: should we abandon FEV1/FVC ,0.70 to detect airway obstruction? No. Chest 2010;138:1037–1040. 31. Enright P, Brusasco V. Counterpoint: should we abandon FEV1/FVC , 0.70 to detect airway obstruction? Yes. Chest 2010;138:1040–1042. 32. Quanjer PH, Enright PL, Stocks J, Ruppel G, Swanney MP, Crapo RO, Pedersen OF, Falaschetti E, Schouten JP, Jensen RL, et al. Open letter to the members of the GOLD committee [in French]. Rev Mal Respir 2010;27:1003–1007. 33. Quanjer PH, Enright PL, Miller MR, Stocks J, Ruppel G, Swanney MP, Crapo RO, Pedersen OF, Falaschetti E, Schouten JP, et al. Open letter: the need to change the method for defining mild airway obstruction. Prim Care Respir J 2010;19:288–291. 34. Garcı´a-Rio F, Soriano JB, Miravitlles M, Mun˜oz L, Duran-Tauleria E, Sa´nchez G, Sobradillo V, Ancochea J. Subjects ‘‘over-diagnosed’’ as COPD by the 0.7 fixed ratio have a poor health-related quality of life. Chest (In press) 35. Chobanian AV. Shattuck Lecture: the hypertension paradox—more uncontrolled disease despite improved therapy. N Engl J Med 2009; 361:878–887. 36. Rose G. Sick individuals and sick populations. Int J Epidemiol 1985;14: 32–38. 37. Blanc PD, Menezes AM, Plana E, Mannino DM, Hallal PC, Toren K, Eisner MD, Zock JP. Occupational exposures and COPD: an ecological analysis of international data. Eur Respir J 2009;33:298– 304. 38. Ezzati M, Hoorn SV, Rodgers A, Lopez AD, Mathers CD, Murray CJ; Comparative Risk Assessment Collaborating Group. Estimates of global and regional potential health gains from reducing multiple major risk factors. Lancet 2003;362:271–280. 39. Stoller JK, Aboussouan LS. a1-Antitrypsin deficiency. Lancet 2005;365: 2225–2236. 40. Lange P, Parner P, Vestbo J, Schnohr P, Jensen G. A 15-year follow-up study of ventilatory function in adults with asthma. N Engl J Med 1998;339:1194–1200.
Soriano and Rodrı´guez-Roisin: COPD Epidemiology in the 21st Century 41. Menezes AM, Hallal PC, Perez-Padilla R, Jardim JR, Muin˜o A, Lopez MV, Valdivia G, Montes de Oca M, Talamo C, Pertuze J, et al.; Latin American Project for the Investigation of Obstructive Lung Disease (PLATINO) Team. Tuberculosis and airflow obstruction: evidence from the PLATINO study in Latin America. Eur Respir J 2007;30: 1180–1185. 42. Tashkin DP. Smoked marijuana as a cause of lung injury. Monaldi Arch Chest Dis 2005;63:93–100. 43. Aldington S, Williams M, Nowitz M, Weatherall M, Pritchard A, McNaughton A, Robinson G, Beasley R. Effects of cannabis on pulmonary structure, function and symptoms. Thorax 2007;62:1058–1063. 44. Torres-Duque C, Maldonado D, Pe´rez-Padilla R, Ezzati M, Viegi G; Forum of International Respiratory Studies (FIRS) Task Force on Health Effects of Biomass Exposure. Biomass fuels and respiratory diseases: a review of the evidence. Proc Am Thorac Soc 2008;5:577–590. 45. Anonymous. COPD—more than just tobacco smoke. Lancet 2009;374: 663. 46. Eisner MD, Anthonisen N, Coultas D, Kuenzli N, Perez-Padilla R, Postma D, Romieu I, Silverman EK, Balmes JR; Committee on Nonsmoking COPD, Environmental and Occupational Health Assembly. An official American Thoracic Society public policy statement: novel risk factors and the global burden of chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2010;182:693–718. 47. US Department of Health and Human Services. The health consequences of smoking: a report of the surgeon general. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2004. 48. Lundba¨ck B, Lindberg A, Lindstrom M, Ro¨nmark E, Jonsson AC, Jo¨nsson E, Larsson LG, Andersson S, Sandstro¨m T, Larsson K, et al. Obstructive lung disease in Northern Sweden studies: not 15 but 50% of smokers develop COPD? Report from the Obstructive Lung Disease in Northern Sweden Studies. Respir Med 2003;97:115–122. 49. Lindberg A, Bjerg-Backlund A, Ronmark E, Larsson LG, Lundback B. Prevalence and underdiagnosis of COPD by disease severity and the attributable fraction of smoking: report from the Obstructive Lung Disease in Northern Sweden Studies. Respir Med 2006;100:264–272. 50. Mannino DM, Buist AS, Petty TL, Enright PL, Redd SC. Lung function and mortality in the United States: data from the first National Health and Nutrition Examination Survey follow up study. Thorax 2003;58: 388–393. 51. Chilvers ER, Lomas DA. Diagnosing COPD in non-smokers: splitting not lumping. Thorax 2010;65:465–466. 52. Brandt AM. FDA regulation of tobacco—pitfalls and possibilities. N Engl J Med 2008;359:445–448. 53. Warren CP. The nature and causes of chronic obstructive pulmonary disease: a historical perspective. The Christie Lecture 2007, Chicago, USA. Can Respir J 2009;16:13–20. 54. Rennard SI, Vestbo J. The many ‘‘small COPDs’’: COPD should be an orphan disease. Chest 2008;134:623–627. 55. Han MK, Agusti A, Calverley PM, Celli BR, Criner G, Curtis JL, Fabbri LM, Goldin JG, Jones PW, Macnee W, et al. COPD Phenotypes: the future of COPD. Am J Respir Crit Care Med 2010;582:598–604. 56. Grydeland TB, Dirksen A, Coxson HO, Pillai SG, Sharma S, Eide GE, Gulsvik A, Bakke PS. Quantitative computed tomography: emphysema and airway wall thickness by sex, age and smoking. Eur Respir J 2009;34:858–865. 57. Hyatt RE, Cowl CT, Bjoraker JA, Scanlon PD. Conditions associated with an abnormal nonspecific pattern of pulmonary function tests. Chest 2009;135:419–424.
367 58. Celli BR, Cote CG, Marin JM, Casanova C, Montes de Oca M, Mendez RA, Pinto Plata V, Cabral HJ. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med 2004;350:1005–1012. 59. Cote CG, Pinto-Plata VM, Marin JM, Nekach H, Dordelly LJ, Celli BR. The modified BODE index: validation with mortality in COPD. Eur Respir J 2008;32:1269–1274. 60. Soler-Cataluna JJ, Martinez-Garcia MA, Sanchez LS, Tordera MP, Sanchez PR. Severe exacerbations and BODE index: two independent risk factors for death in male COPD patients. Respir Med 2009; 103:692–699. 61. Puhan MA, Garcia-Aymerich J, Frey M, ter Riet G, Anto JM, Agusti AG, Gomez FP, Rodriguez-Roisin R, Moons KG, Kessels AG, et al. Expansion of the prognostic assessment of patients with chronic obstructive pulmonary disease: the updated BODE index and the ADO index. Lancet 2009;374:704–711. 62. Briggs A, Spencer M, Wang H, Mannino D, Sin DD. Development and validation of a prognostic index for health outcomes in chronic obstructive pulmonary disease. Arch Intern Med 2008;168:71–79. 63. Azarisman MS, Fauzi MA, Faizal MP, Azami Z, Roslina AM, Roslan H. The SAFE (SGRQ score, air-flow limitation and exercise tolerance) index: a new composite score for the stratification of severity in chronic obstructive pulmonary disease. Postgrad Med J 2007;83:492–497. 64. Jones RC, Donaldson GC, Chavannes NH, Kida K, Dickson-Spillmann M, Harding S, Wedzicha JA, Price D, Hyland ME. Derivation and validation of a composite index of severity in chronic obstructive pulmonary disease—the dose index. Am J Respir Crit Care Med 2009; 180:1189–1195. 65. Darwin C. On the origin of species by means of natural selection, or the preservation of favoured races in the struggle for life. London: John Murray; 1859. 66. Raherison C, Janson C, Jarvis D, Burney P, Cazzoletti L, de Marco R, Neukirch F, Leynaert B. Evolution of asthma severity in a cohort of young adults: is there any gender difference? PLoS ONE 2009;4: e7146. 67. Haahtela T, Tuomisto LE, Pietinalho A, Klaukka T, Erhola M, Kaila M, Nieminen MM, Kontula E, Laitinen LA. A 10 year asthma programme in Finland: major change for the better. Thorax 2006;61:663– 670. 68. Kupczyk M, Haahtela T, Cruz AA, Kuna P. Reduction of asthma burden is possible through National Asthma Plans. Allergy 2010;65: 415–419. 69. Pietinalho A, Kinnula VL, Sovija¨rvi AR, Vilkman S, Sa¨yna¨ja¨kangas O, Liippo K, Kontula E, Laitinen LA. Chronic bronchitis and chronic obstructive pulmonary disease: the Finnish Action Programme, interim report. Respir Med 2007;101:1419–1425. 70. Almagro P, Salvado´ M, Garcia-Vidal C, Rodriguez-Carballeira M, Delgado M, Barreiro B, Heredia JL, Soriano JB. Recent improvement in long-term survival after a COPD hospitalisation. Thorax 2010;65:298–302. 71. Agusti A, Barnes PJ. What the journal would like to publish on chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2010;182:1–2. 72. Cazzola M, MacNee W, Martinez FJ, Rabe KF, Franciosi LG, Barnes PJ, Brusasco V, Burge PS, Calverley PM, Celli BR, et al. Outcomes for COPD pharmacological trials: from lung function to biomarkers. Eur Respir J 2008;31:416–469. 73. Pinnock H, Thomas M, Tsiligianni I, Lisspers K, Østrem A, Sta¨llberg B, Yusuf O, Ryan D, Buffels J, Cals JW, et al. The International Primary Care Respiratory Group (IPCRG) research needs statement 2010. Prim Care Respir J 2010;19:S1–S20.