Acta Ophthalmologica 2012
Automated alternation flicker for the detection of optic disc haemorrhages Zeba A. Syed,1 Nathan M. Radcliffe,1 Carlos Gustavo De Moraes,2,3 Scott D. Smith,4 Jeffrey M. Liebmann2,3 and Robert Ritch2,5 1
Department of Ophthalmology, Weill Cornell Medical College, New York, New York, USA 2 Einhorn Clinical Research Center, New York Eye and Ear Infirmary, New York, New York, USA 3 Department of Ophthalmology, New York University School of Medicine, New York, New York, USA 4 Department of Ophthalmology, New York Presbyterian Hospital, New York, New York, USA 5 Department of Ophthalmology, New York Medical College, Valhalla, New York, USA
ABSTRACT. Purpose: Optic disc haemorrhages are associated with active glaucomatous neurodegeneration and ongoing visual field loss. We sought to determine whether automated alternation flicker enhances the detection of disc haemorrhages in serial images from patients with glaucoma when compared to sideby-side photographic evaluation and single-image display. Methods: Serial sets of optic nerve photographs of 394 eyes from 234 patients followed for glaucoma at the authors’ institutions were included in this study. Eyes with disc haemorrhages were graded for difficulty level and randomized along with nondisc haemorrhage control images into one of three presentation groups (automated alternation flicker, side-by-side or single image). Seven graders viewed all images and assessed for the presence or absence of disc haemorrhages. Results: The sensitivity of automated alternation flicker for disc haemorrhage detection (0.878) was higher than side-by-side (0.705; p = 0.002) and single photographs (0.757; p = 0.01). There was no specificity difference between pairs of presentation groups (all p ‡ 0.7). Conclusion: Automated alternation flicker was a more sensitive method for disc haemorrhage detection than the current clinical standards and may have an important role in the management of glaucoma. Key words: automated alternation flicker – disc haemorrhages – glaucoma – progressive optic neuropathy
Acta Ophthalmol. 2012: 90: 645–650 ª 2011 The Authors Acta Ophthalmologica ª 2011 Acta Ophthalmologica Scandinavica Foundation
doi: 10.1111/j.1755-3768.2010.02094.x
Introduction Glaucoma is a progressive optic neuropathy and the second leading cause of irreversible blindness worldwide, affecting over 60 million people (Quigley & Broman 2006). Identifying the risk factors for glaucoma progression is important for disease management (Nouri-Mahdavi et al. 2004). Optic disc haemorrhages, visible by ophthalmoscopy or optic disc photography, are associated with active glaucomatous neurodegeneration and ongoing visual field loss (Diehl et al. 1990; Siegner & Netland 1996; Ishida et al. 2000; Leske et al. 2007; De Moraes et al. 2009). Clinically, disc haemorrhages are areas of extravascular blood within the retinal nerve fibre layer (RNFL). They are often located adjacent to existing, focal RNFL defects and neuroretinal rim notches, which may correspond to regions of perimetric loss (Jonas & Xu 1994). Disc haemorrhage detection has proven to be challenging mainly for two reasons. First, they are transient, and unless patients are photographed often, there is a high probability that
645
Acta Ophthalmologica 2012
they will be missed during a single or few examinations (Heijl 1986). Second, clinical evaluation of the optic disc during slit-lamp examination may be insufficient to detect cases of disc haemorrhage when they are subtle or when they are close to vascular or pigmented tissues. In a study comparing detection rates for disc haemorrhages using clinical examination (biannual optic nerve observation via direct or slit-lamp biomicroscopy) versus stereophotographic review (annual inspection of stereoscopic disc photographs), 25.2% of disc haemorrhages were detected on clinical examination versus 89.5% in photographs, demonstrating the higher sensitivity of stereophotographs for detection (Budenz et al. 2006). Still, disc haemorrhages may be small and easy to overlook on photographs, requiring a series of side-by-side disc photographs examined in chronological order to visualize differences. While detection is enhanced with photographic review compared to clinical examination, the ideal photographic review technique has not been established. A new technique called automated alternation flicker may facilitate the detection of disc haemorrhages. Alternation flicker (automated or manual) involves alignment and alternation of serial optic nerve photographs, allowing observers to discern structural optic nerve changes over time. The automated alternation flicker software automatically aligns two images by identifying vascular intersections or other salient image features, superimposing the photographs to a sub-pixel level after several global transformations (such as rotation and magnification) and alternating the images at a frequency dictated by the user. A study comparing the detection of parapapillary atrophy (PPA) using automated alternation flicker and side-by-side photographs found that graders identified more PPA progression cases using automated alternation flicker (Vanderbeek et al. 2010). Furthermore, interobserver agreement using automated alternation flicker was better than photographic review (Vanderbeek et al. 2010). The ability of automated alternation flicker to detect disc haemorrhages, another feature of glaucomatous optic neuropathy, has not been investigated.
646
The purpose of this study was to determine whether automated alternation flicker enhances the detection of disc haemorrhages in serial images from glaucoma patients when compared to side-by-side photographic evaluation and single-image display. In addition, we assessed whether detection time varied across these evaluation methods to determine their efficiency in detecting disc haemorrhages.
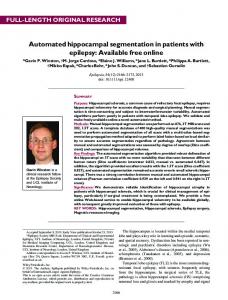
Methods Approval for this study was obtained from the Institutional Review Boards at Weill Cornell Medical College (New York, NY, USA) and the New York Eye and Ear Infirmary (New York, NY, USA). Serial sets of digital optic nerve photographs of 394 eyes from 234 consecutive patients followed for glaucoma at the authors’ practices were included in this study. Of the 394 photographs, 221 revealed clinically documented disc haemorrhages, the presence of which was agreed upon using disc photographs by two glaucoma specialists not involved in grading (NR and CD). The remaining 173 images without disc haemorrhages were included as the control group. One of the authors not involved in grading (NR) rated the difficulty of detection of disc haemorrhage in each eye’s image set as easy (52 eyes), moderate (88 eyes) or difficult (81 eyes) to
detect (Fig. 1). Images designated to be easy contained large disc haemorrhages greater than one clock hour in width. Moderate disc haemorrhages were smaller than 1 clock hour in size but were distinct, without masking from nearby blood vessels. Difficult disc haemorrhages were either very small, partially or mostly resolved, or partially masked by adjacent blood vessels. An example from each difficulty group and a control image is provided (Fig. 1). Easy, moderate and difficult disc haemorrhages were randomized into one of three presentation groups (flicker, side-by-side or single image), and each presentation group had a similar number of eyes from each difficulty level. The 173 eyes without disc haemorrhages were also randomized into one of these three groups. For each eye in the flicker presentation group, a pair of serial photographs was imported into MatchedFlicker8 software (V1.2: EyeIC, Narberth, PA, USA). Screen captures (resolution 1280 · 800 pixels) from the software were then used to generate an animated gif file in Adobe Photoshop CS3 (V9.0: Adobe Systems, San Jose, CA, USA), which alternated the baseline and follow-up photographs of the serial photographic pairs at a flicker rate of 2 Hz (0.5s per image). For eyes in the side-by-side presentation group, baseline and follow-up digital photographs were placed adjacent to each other on the same screen, with baseline
Fig. 1. Examples of disc haemorrhages that were graded as easy (top left), moderate (top right) or difficult (bottom left) to detect. The image at the bottom right does not contain a disc haemorrhage.
Acta Ophthalmologica 2012
versus follow-up and disc haemorrhage versus nondisc haemorrhage images randomized with respect to placement on the left or right side of the screen. For eyes in the single-image presentation group, one photograph (containing or not containing a disc haemorrhage) was displayed on the screen. The magnification and resolution of the flicker, side-by-side and single-image photographs were equivalent. All images were presented using PowerPoint 2007 (Microsoft Corporation, Redmond, WA, USA) and TurningPoint 2008 (Turning Technologies, Youngstown, OH, USA) and displayed on a standard 19-inch LCD computer display. Three medical students, two ophthalmology residents and two attending physicians (paediatric and retina fellowship-trained ophthalmologists) performed the grading. Prior to the grading session, each individual was shown a five-minute presentation that included 10 example images of disc haemorrhages and one example of a normal optic nerve, none of which was included in the study sample. These images were presented without their accompanying baseline or follow-up images. Additionally, one example of automated alternation flicker and one example of side-byside photographs were given. Graders were masked to all clinical patient data and to the frequency of disc haemorrhages in the study sample. They were masked to the duration of follow-up (which was case-matched between the disc haemorrhage and control groups) and to the fellow raters’ determination. The graders viewed a presentation of 394 slides. One-third of the slides were automated alternation flicker (132 slides), one-third were side-by-side (131 slides) and one-third were single images (131 slides). The slides were shown over the course of six blocks, each containing 21 or 22 slides of each presentation type. The graders were asked to assess each automated alternation flicker, side-byside or single-image slide for the presence or absence of disc haemorrhage. The graders were instructed that a haemorrhage might be present at baseline or follow-up (positive for disc haemorrhage) or that there might be no disc haemorrhage present in any of the images (negative for disc haemorrhage). The graders verbally indicated
‘yes’ if they saw or ‘no’ if they did not see a disc haemorrhage in each slide, and responses were recorded. TurningPoint 2008 also measured and reported the time interval between the appearance of an image on the screen and the keystroke response, providing response times for each slide. Statistical analysis was performed using Stata 8.1 statistical software (Stata Corporation, College Station, TX, USA). Response times were compared between the three presentation groups using one-way analysis of variance (anova). Statistical significance between individual pairs of presentation groups was calculated using the Bonferroni correction. The effect of difficulty level on response time was further analysed using analysis of covariance (ancova). This statistical model included presentation group and difficulty level as predictors of response time. Sensitivity and specificity of accurately identifying images with and without disc haemorrhages were determined by computing the proportion of correct responses of each grader. The effect of presentation type and difficulty level on the accuracy of responses was evaluated by logistic regression modelling. The statistical models were generated within a generalized estimating equation (GEE) framework to account for correlations in the data, as each of the 7 graders viewed the same sets of images. One model was computed for images without disc haemorrhages, permitting the statistical comparison of specificity between presentation groups. A separate model was computed for images with disc haemorrhages, permitting the estimation of adjusted effects of presentation type and difficulty level on sensitivity. Statistical significance was defined by p-values £0.05.
Results Digital optic nerve photographs of 439 eyes from 234 patients were considered for inclusion in this study, of which 256 eyes contained disc haemorrhages and the remaining 183 were control images without disc haemorrhages. Forty-five eyes (35 with disc haemorrhages and 10 controls) were excluded prior to randomization owing to poor quality of either baseline or follow-up images.
For disc haemorrhage detection, the sensitivity of automated alternation flicker (0.878) was higher than side-byside (0.705; p = 0.002) and single photographs (0.757; p = 0.01). There was no difference in sensitivity for disc haemorrhage detection between sideby-side presentation and single images (p = 0.5). There was a larger sensitivity difference between automated alternation flicker and nonflicker groups for difficult disc haemorrhages compared to moderate difficulty disc haemorrhages and a negligible sensitivity difference between automated alternation flicker and nonflicker groups for easy disc haemorrhages (Table 1). There was no specificity difference (rate of false positives) between pairs of presentation groups (all p ‡ 0.7). The advantage of automated alternation flicker over side-by-side and single images appeared across all levels of expertise – medical students, residents and attending physicians (Table 2). Mean response times using automated alternation flicker (3.7 seconds) were shorter than using side-by-side images (5.4 seconds, p < 0.0005). Graders also responded faster to single images (4.0 seconds) than to sideby-side images (p < 0.0005). There were no significant differences in response times between automated alternation flicker and single images (p = 0.3). Automated alternation flicker had shorter response times relative to side-by-side images for easy, moderate, difficult and nondisc haemorrhage images (Table 3).
Discussion In this comparison of three techniques for identifying disc haemorrhages in optic disc photographs, automated alternation flicker demonstrated greater sensitivity in disc haemorrhage detection compared to both side-byside and single images. As expected, Table 1. Sensitivity for detecting disc haemorrhage by image difficulty and method of presentation.
AAF Side-by-Side Single
Easy
Moderate
Difficult
0.984 1.000 0.933
0.995 0.818 0.857
0.689 0.397 0.527
AAF = automated alternation flicker; Sideby-Side = side-by-side photographs; Single = single images.
647
Acta Ophthalmologica 2012
Table 2. Sensitivity ⁄ specificity for detecting disc haemorrhage by level of training and method of presentation.
AAF Side-by-Side Single
Medical students
Residents
Attending physicians
0.840 ⁄ 0.865 0.621 ⁄ 0.874 0.717 ⁄ 0.845
0.927 ⁄ 0.930 0.801 ⁄ 0.940 0.829 ⁄ 0.966
0.887 ⁄ 0.939 0.733 ⁄ 0.897 0.747 ⁄ 0.940
AAF = automated alternation flicker; Side-by-Side = side-by-side photographs; Single = single images.
Table 3. Response time (seconds) by disc haemorrhage detection difficulty and method of presentation.
AAF Side-by-Side Single
No disc haemorrhage
Easy
Moderate
Difficult
4.96 6.42 4.68
1.85 2.42 1.57
2.19 4.10 2.94
3.88 6.52 4.66
AAF = automated alternation flicker; Side-by-Side = side-by-side photographs; Single = single images.
the predetermined detection difficulty of each disc haemorrhage (determined by size, degree of resorption and masking by adjacent vessels) influenced the ability of graders to visualize disc haemorrhages independent of the methodology used to view the optic nerve photographs. The sensitivity advantage conferred by automated alternation flicker in this study was greatest for difficult disc haemorrhages, while no advantage seen for disc haemorrhages deemed to be easily detected. The utility of automated alternation flicker is therefore greatest for small, resolved or masked disc haemorrhages – ones that may otherwise go unobserved using side-by-side photographs, single-image assessment or clinical examination. Given that the presence of disc haemorrhages is one of the strongest negative prognostic indicators for glaucoma, an increased rate of detection would likely result in changes to the clinical management of glaucoma patients (Siegner & Netland 1996; Ishida et al. 2000; Coleman et al. 2004; Budenz et al. 2006; Leske et al. 2007; Bengtsson et al. 2008; De Moraes et al. 2009). One potential criticism of alternation flicker is the concern that the matching algorithm could generate artefacts mimicking disc haemorrhages, contributing to an artificially elevated level of sensitivity and reduced specificity. This has been described for
648
other features of glaucomatous optic neuropathy with nonautomated alternation flicker techniques (Bengtsson & Krakau 1979). These nonautomated techniques include the projection of sequential images onto a screen after manual alignment of two overlapping projectors (Heijl & Bengtsson 1989) and registration of serial computerized images with a reference image, altering size and rotation to align the images and allow for sequential display (Algazi et al. 1985). In the present work, however, automated alternation flicker allowed for greater sensitivity without a reduction in specificity, indicating a similar rate of false-positive results across techniques. A higher degree of sensitivity without a reduction in specificity suggests that automated alternation flicker may have potential for disc haemorrhage detection in screening populations with glaucoma. We also demonstrated a slightly more rapid analysis of images overall using automated alternation flicker compared to side-by-side images, highlighting the potential value of automated alternation flicker for enhanced management of glaucoma. The clinical value of a 1.7-second (31%) time reduction using automated alternation flicker compared to sideby-side images is uncertain. The number of available data points was identical between automated alternation flicker and side-by-side images as was
the magnification of the images, suggesting that the automated alternation flicker presentation did facilitate detection by slightly reducing the time required for analysis. Regardless of the presentation method, this study found that the expected time required to detect a disc haemorrhage of any difficulty is shorter than the time required to rule one out. Automated alternation flicker was associated with shorter response times for images across all categories (difficult, moderate, easy or no disc haemorrhage). Taking into account the time needed to generate flicker movies and side-byside displays, it is arguable that the total difference in time involved may not differ significantly or could even be longer for automated alternation flicker. Notably, graders in this study did not view optic disc videos using flicker software; rather, images created with automated alternation flicker were imported into Adobe Photoshop CS3 prior to the generation of movies, a process that required more time than flicker software alone would involve. While it was necessary to extract images from the automated alternation flicker software to present them appropriately and time responses in this experimental setting, the flicker images used in the study were generated from screen captures of the flicker software and presented at identical magnification and should not differ meaningfully from the software’s presentation. Furthermore, in clinical settings, the creation of automated alternation flicker movies would likely be performed by technicians rather than by physicians. Finally, with the potential for the integration of automated alternation flicker into electronic medical records, any additional time needed to create videos may be reduced through a facilitated interface to use this software in viewing serial optic disc images. The presence of disc haemorrhages is among the strongest predictive factors for glaucoma progression. The development of primary open-angle glaucoma in the Ocular Hypertension Treatment Study increased by a factor of 3.7 after the occurrence of a disc haemorrhage (Budenz et al. 2006). The risk attributable to disc haemorrhage was greater than that of older age (>50 years), having a cornea that was 80 lm thinner, having a 0.5 unit
Acta Ophthalmologica 2012
larger vertical cup-to-disc ratio or having a level of intraocular pressure elevated by 12 mmHg (Coleman et al. 2004; Budenz et al. 2006). These findings reinforce the pathogenic and diagnostic importance of disc haemorrhages for progressive glaucoma. In addition, there is a likely benefit of treatment in slowing progressive visual field loss in eyes with disc haemorrhages. Differences in rates of visual field loss pre- and postdisc haemorrhage are significantly related to the reduction in intraocular pressure in the postdisc haemorrhage period relative to the predisc haemorrhage period, although several studies examining this issue have produced conflicting results (Hendrickx et al. 1994; Budenz et al. 2006; Miyake et al. 2006; Bengtsson et al. 2008; Medeiros et al. 2010). Hence, the occurrence of a disc haemorrhage must be followed closely by a rigorous treatment protocol to address the high risk of future progressive glaucomatous neuropathy and a more efficient method for disc haemorrhage detection would likely enhance the management of this disease. This study has several strengths and limitations. We asked seven graders to review 394 image pairs containing 221 unique instances of disc haemorrhage. Similar investigations have typically used fewer reviewers or fewer image pairs, particularly for disc haemorrhage evaluation (Gaasterland et al. 2001; Azuara-Blanco et al. 2003; Chauhan et al. 2009; Jampel et al. 2009). We used seven graders with different levels of experience to balance the effects of experience on the outcome of disc haemorrhage detection. However, even with this number of graders, it was still not possible to perform a powered statistical analysis of expertise level and its effect on ability to detect disc haemorrhages across the three presentation methods. However, qualitative assessment did suggest an advantage for automated alternation flicker regardless of a grader’s level of expertise. Given that disc haemorrhage is a clinical diagnosis, we chose to define eyes with disc haemorrhage as eyes with photographic evidence of haemorrhage agreed upon by two glaucoma specialists. It is possible that one or more eyes could have been misclassified using our clinical definition,
although we believe this is unlikely to have biased the results towards a particular technique. It is also possible that some disc haemorrhages in this study were misclassified by both of the two original graders. Bias resulting from misclassification tends to reduce the magnitude of differences in the effect of factors on an outcome and is thus unlikely to explain the advantages of automated alternation flicker that were found. Finally, while we found an advantage using automated alternation flicker in this study, a relatively high rate of disc haemorrhage detection occurred across all techniques – perhaps higher than would occur in a clinical setting. Therefore, one suggestion of this study is that disc haemorrhage detection is generally good (with a sensitivity between 71% and 88%) when it is approached as a binary task, without an accompanying comprehensive optic nerve complex evaluation. Graders in this study were asked specifically to look for disc haemorrhages, whereas in a routine clinical setting, an ophthalmologist may not search as carefully for disc haemorrhages given their relatively low incidence. Although the prevalence of disc haemorrhages in glaucomatous eyes is significantly greater than in normal eyes (Bengtsson et al. 1981; Airaksinen 1984), it varies with glaucoma diagnosis; 14% of subjects with open-angle glaucoma (8% with high-pressure glaucoma and 25% with low-pressure glaucoma) and 1.5% with ocular hypertension have disc haemorrhages (Healey et al. 1998). Prevalence also varies with stage of glaucoma, and the frequency of disc haemorrhage increases from an early stage of glaucoma to mediumadvanced stages (Jonas & Xu 1994). The Early Manifest Glaucoma Trial (EMGT) found that 55% of glaucoma patients develop disc haemorrhages at some point during a median follow-up of 8 years as assessed with biannual photography (Bengtsson et al. 2008). This study provides the first evidence that a new automated flicker technology may be a more sensitive method to detect disc haemorrhages than the current clinical standards. Further research is needed to assess the value of automated alternation flicker in the clinical management of patients with glaucoma and to correlate its findings with visual field progression.
Acknowledgements This research was supported in part by the Edward B. Goodnow Glaucoma Research Fund, New York Eye and Ear Infirmary, New York, NY. The authors of this study have no financial disclosures to report. Approval for this study was obtained from the Institutional Review Boards at Weill Cornell Medical College (New York, NY) and the New York Eye and Ear Infirmary (New York, NY). Informed Consent for the research was obtained from the subjects, and the study is in accordance with HIPAA regulations.
References Airaksinen PJ (1984): Are optic disc haemorrhages a common finding in all glaucoma patients? Acta Ophthalmol (Copenh) 62: 193–196. Algazi RV, Keltner JL & Johnson CA (1985): Computer analysis of the optic cup in glaucoma. Invest Ophthalmol Vis Sci 26: 1759–1770. Azuara-Blanco A, Katz LJ, Spaeth GL, Vernon SA, Spencer F & Lanzl IM (2003): Clinical agreement among glaucoma experts in the detection of glaucomatous changes of the optic disk using simultaneous stereoscopic photographs. Am J Ophthalmol 136: 949–950. Bengtsson B & Krakau CE (1979): Flicker comparison of fundus photographs: a technical note. Acta Ophthalmol (Copenh) 57: 503–506. Bengtsson B, Holmin C & Krakau CE (1981): Disc haemorrhage and glaucoma. Acta Ophthamol (Copenh) 59: 1–14. Bengtsson B, Leske C, Yang Z & Heijl A (2008): Disc hemorrhages and treatment in the Early Manifest Glaucoma Trial. Ophthalmology 115: 2044–2048. Budenz DL, Anderson DR, Feuer WJ et al. (2006): Detection and prognostic significance of optic disc hemorrhages during the Ocular Hypertension Treatment Study. Ophthalmology 113: 2137–2143. Chauhan BC, Hutchison DM, Artes PH, Caprioli J, Jonas JB, LeBlanc RP & Nicolela MT (2009): Optic disc progression in glaucoma: comparison of confocal scanning laser tomography to optic disc photographs in a prospective study. Invest Ophthalmol Vis Sci 50: 1682–1691. Coleman AL, Gordon MO, Beiser JA & Kass MA (2004): Baseline risk factors for the development of primary open-angle glaucoma in the Ocular Hypertension Treatment Study. Am J Ophthalmol 138: 684–685. De Moraes CG, Prata TS, Liebmann CA, Tello C, Ritch R & Liebmann JM (2009): Spatially consistent, localized visual field loss before and after disc hemorrhage. Invest Ophthalmol Vis Sci 50: 4727–4733.
649
Acta Ophthalmologica 2012
Diehl DL, Quigley HA, Miller NR et al. (1990): Prevalence and significance of optic disc hemorrhage in a longitudinal study of glaucoma. Arch Ophthalmol 108: 545–550. Gaasterland DE, Blackwell B, Dally LG, Caprioli J, Katz LJ & Ederer F (2001): The Advanced Glaucoma Intervention Study (AGIS): variability among academic glaucoma subspecialists in assessing optic disc notching. Trans Am Ophthalmol Soc 99: 177–185. Healey PR, Mitchell P, Smith W & Wang JJ (1998): Optic disc hemorrhages in a population with and without signs of glaucoma. Ophthalmology 105: 216–223. Heijl A (1986): Frequent disc photography and computerized perimetry in eyes with optic disc haemorrhage: a pilot study. Acta Ophthalmol (Copenh) 64: 274–281. Heijl A & Bengtsson B (1989): Diagnosis of early glaucoma with flicker comparisons of serial disc photographs. Invest Ophthalmol Vis Sci 30: 2376–2384. Hendrickx KH, van den Enden A, Rasker MT & Hoyng PF (1994): Cumulative incidence of patients with disc hemorrhages in glaucoma and the effect of therapy. Ophthalmology 101: 1165–1172. Ishida K, Yamamoto T, Sugiyama K & Kitazawa Y (2000): Disk hemorrhage is a significantly negative prognostic factor for
650
normal-tension glaucoma. Am J Ophthalmol 129: 707–714. Jampel HD, Friedman D, Quigley H, Vitale S, Miller R, Knezevich F & Ding Y (2009): Agreement among glaucoma specialists in assessing progressive disc changes from photographs in open-angle glaucoma patients. Am J Ophthalmol 147: 39–44. Jonas JB & Xu L (1994): Optic disk hemorrhages in glaucoma. Am J Ophthalmol 118: 1–8. Leske MC, Heijl A, Hyman L, Bengtsson B, Dong L & Yang Z (2007): Predictors of longterm progression in the early manifest glaucoma trial. Ophthalmology 114: 1965–1972. Medeiros FA, Alencar LM, Sample PA, Zangwill LM, Susanna R Jr & Weinreb RN (2010): The relationship between intraocular pressure reduction and rates of progressive visual field loss in eyes with optic disc hemorrhage. Ophthalmology 117: 2061–2066. Miyake T, Sawada A, Yamamoto T et al. (2006): Incidence of disc hemorrhages in open-angle glaucoma before and after trabeculectomy. J Glaucoma 15: 164–171. Nouri-Mahdavi K, Hoffman D, Coleman AL et al. (2004): Predictive factors for glaucomatous visual field progression in the Advanced Glaucoma Intervention Study. Ophthalmology 111: 1627–1635.
Quigley HA & Broman AT (2006): The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol 90: 262– 267. Siegner SW & Netland PA (1996): Optic disc hemorrhages and progression of glaucoma. Ophthalmology 103: 1014–1024. Vanderbeek BL, Smith SD & Radcliffe NM (2010): Comparing the detection and agreement of parapapillary atrophy progression using digital optic disk photographs and alternation flicker. Graefes Arch Clin Exp Ophthalmol 248: 1313–1317.
Received on September 30th, 2010. Accepted on November 26th, 2010. Correspondence: Nathan M. Radcliffe, MD Department of Ophthalmology Weill Cornell Medical College Weill Greenberg Center 1305 York Ave at East 70th St New York NY 10021 USA Tel: 646 962 2020 Fax: 646 962 0603 Email:
[email protected]