CHAPTER 1 INTRODUCTION
The spring, summer, and fall of 1999 had America in shock from the latest waves of violence in its schools and suburban communities. Youth violence and its impact on the suburban community of Littleton, Colorado, and the recent killing spree and "hate crimes" committed by Benjamin Smith in Illinois and Indiana have caused President Clinton, the U.S. Congress, and Americans in general to debate muchneeded solutions to the hate and violence sweeping our schools and local communities. Illegal automatic weapons and handguns in the hands of angry youth are proving to be the instruments used in many of the violent attacks on the innocent victims of these troubled youth. Local communities are recognizing that America needs to address the problem and take action in reducing all forms of community violence. A recent nationwide survey of more than 20,000 middle-school and highschool students by the American Public Health Association ("Survey Shows," 1999) paints a grim picture of American youths' attitudes and actions related to guns and the problem of violence. The survey was conducted by the Josephson Institute of Ethics, an alliance of more than 300 national and regional groups working to help students develop the six basic character traits of trustworthiness, respect, responsibility, fairness, caring, and citizenship. Results from the Josephson Institute survey illustrate that schools need to bolster their violence prevention efforts because: • 24.0% of male high schoolers and 18.0% of male middle schoolers said they took a weapon to school at least once in the past year;
2
• 70.0% of high schoolers and 73.0% of middle schoolers said they hit a person in the last 12 months because they were angry; and • 43.0% of high schoolers and 47.0% of the middle schoolers said they did not feel safe at school. As a response to the health and school safety problems faced by adolescents, Chavis (1995, p. 237) focused on the need to develop a local community's capacity for prevention or "the ability to effectively develop, mobilize, and use resources to manage change" (p. 237). Complex problems such as youth violence require broad coalitions of professionals, government officials, and citizens to evaluate systems, services, and products. Coalitions or partnerships serve as "enabling systems" to obtain needed resources, create incentives for change, and educate the community to important public health issues. Such partnerships consist of members from multiple sectors in the community--churches, business, government, grassroots citizens' organizations, schools, health-care organizations, and social service agencies--who have a stake in solving a problem and achieving a goal. Elliott, Hamburg, and Williams (1998) stressed that building comprehensive violence prevention strategies requires the collaborative input of adults responsible for delivering needed services to youths and the involvement of youths themselves. The response of Aurora area health-care professionals, educators, clergy, and social services professionals to concerns about student safety and character building was the formation of the Teen CARE Network (TCN), a library/community agency partnership supported generously by Provena Mercy Center Hospital. For the professionals intimately involved in the formation and implementation of the TCN and for the academic community at large, this case study details the processes and structures of a successful library/community agency partnership committed to the
3
improvement of community health-information services and school safety. This research project focuses on the outcomes and effectiveness of a local community's collaborative efforts to create systemic change in all areas of the community-business, human services, education, government, community agencies, and libraries of all types (Doz & Hamel, 1998; Kaluzny, Zuckerman, & Ricketts, 1995; LipmanBlumen & Leavitt, 1999). For the Illinois library community at large, the TCN serves as a model program supported by the Illinois State Library (1998) and DuPage Library System (DLS). The Illinois State Library envisions the establishment of partnerships among Illinois libraries as one of its priority long-range goals for library development and social progress. Library/ community agency partnerships, as defined by the Illinois State Library, are composed of both human and electronic linkages that promote a coordinated "seamless information delivery system" for Illinois citizens. It was the financial and consulting support provided by the Illinois State Library that stimulated the formation of the TCN, facilitated the data-gathering activities to measure local Aurora, Illinois, health-information improvement activities and permitted the preparation of this case study on a library community agency dedicated to violence prevention and peacemaking for teens and their parents. Kerka (1997) noted that collaborative efforts are needed to solve problems of fragmentation of client needs caused by specialized and "bureaucratic" human service categories and definitions that ignore interrelated causes, gaps in service, and viable solutions to community-wide social problems. Collaboration overcomes "bureaucratic" gaps in service by positively influencing and facilitating partner communication that is made possible using modern communication technologies and telecommunications tools available to local communities via the Internet and World Wide Web. A project coordinator position created in the TCN partnership permitted
4
Provena Mercy Center to organize cooperative projects with other local agencies and involve partners in resource sharing and website development. The literature shows that collaborative projects facilitate feelings of mutual ownership, enthusiasm, and commitment in a local community, and this case study research shows that high involvement of the partner agencies did produce effective TCN library/community health education programming (Wilson, 1990). "Reflective Practitioners," Participatory Action Research, and Collaboration Bradshaw (1998a) noted that "when you are `building' a partnership, reflection and celebration are important at every stage" (p. 1). The participatory action research (PAR) methods employed and results described in this dissertation research project lay the foundation for medical, school, and public librarians to assume the role of "reflective practitioners" and to strike a harmonious balance between theory and practice, ideas and emotions, and serious work and joyful play. The dissertation itself is a "celebration" of the journey undertaken by a group of committed librarians and youth services professionals to create the TCN, a library/community agency partnership committed to improving access to consumer health information (CHI) for teens and their parents in Aurora, Illinois. Medical Librarians, Community Public Health Partnerships, and the Internet At the 96th annual meeting of the Medical Library Association (MLA) (1996a) in Kansas City, Missouri, a conference session on violence as a public health issue was sponsored by three divisions of MLA--the Public Health/Health Administration Libraries, Mental Health Librarians, and the Relevant Issues Section. A panel of
5
speakers addressed the need for interdisciplinary collaboration between medical librarians, physicians, researchers, and prevention specialists in seeking communitylevel solutions to violence in America. This MLA conference session, "The Crisis of Violence in America," alerted medical librarians to the scope of violence in America and the need for library outreach and librarian involvement in important community work typically not viewed as a primary service focus of medical libraries. The MLA panelists challenged medical librarians to create new programs within their local communities to reduce violence. A recent article by Tremblay-McGaw (1999) calls for librarians to take a value-laden stand against the epidemic of gun violence. It is evident from the publication of this article that the American Library Association envisions a role for librarians as activists and advocates in preventing gun violence and helping save lives. But it is also clear that librarians need to enlist the cooperation of other community agencies in the "call" for and building of peaceful communities. In 1989, the American Hospital Association developed a program manager's kit for hospitals interested in forming local partnerships with community agencies to promote adolescent health. Publication of this program manager's kit reflected the growing concern of many U.S. hospitals to become involved in health promotion in their communities and to improve access to health care to the underserved adolescent population. One chapter in this adolescent health-promotion planning publication by Giloth and Jellen (1989) notes that medical librarians are experts at tapping the network of health-information resources and can find literature to guide program design and to implement effective adolescent health programs. Medical librarians also have the transformational leadership skills needed to facilitate community change through Internet-based community networking and partnership programming. Recent
6
successful efforts to build Internet-based community networks with librarians in key leadership roles are summarized in Bajjaly (1999). When organizations begin to collaborate on a common prevention goal such as the reduction of community violence and improving adolescent health services, a shared and long-term commitment to working together develops and increases the effectiveness of mutually agreed-upon outcomes. The unique contributions of each partner lead to a more effective prevention effort. The connections made between organizations in a partnership produce positive outcomes that would not have occurred by any one organization acting on its own.
Statement of the Problem One solution to youth violence identified in the professional literature is the formation of a partnership among community agencies affected by a common problem. This case study describes the formation, implementation, and outcomes of the TCN, a library/community agency partnership formed in 1997-1998 to improve access to health information for teens and their parents in Aurora, Illinois. By using a qualitative methodology, the TCN library/community agency partnership is described in detail, and the "meaning of the partnership" is depicted for the partners intimately involved.
Purpose of the Research The purpose of this case study is to assess the outcomes, impact, and effectiveness of a library/community agency partnership in improving access to CHI for 12,000 teens and their parents in Aurora, Illinois, a city with approximately 110,000 residents. A needs analysis of Aurora teen youth risk behaviors, using a
7
modified Youth Risk Behavior Survey (YRBS), was a key part of the problem definition process and priority setting employed in this PAR project (Kolbe, Kann, & Collins, 1993). The effectiveness of the partnership was assessed based on the individual responses of partner professionals to a "partnering behaviors" checklist and to a series of six to seven open-ended exit interview questions posed to 18 of the partners at the end of the implementation phase of the Library Services and Technology (LSTA) grant project in July to September 1999.
Research Questions The research questions to be answered by this investigation are: 1. What are the phases and processes involved in the formation and implementation of a CHI network partnership/alliance? 2. What are important coordinating structures in developing effective library/community agency partnerships? 3. What are barriers to collaboration that partners perceive may limit the effectiveness and growth of a partnership? 4. How do the partners define successful outcomes in evaluating the partnership in addressing a mutually defined problem and seeking community-level solutions? How are successful partnering practices and collaborative behaviors defined by the partner agencies involved in the network? 5. How is the partnership sustained over time? Many writers believe that synergy characterizes the relationship among partners and promotes exceptional performance (Bradshaw, 1998a; Mattessich & Monsey, 1992; Sujansky, 1991; Sullivan, 1998). According to Saltiel (1998), partnerships have the "power to transform ordinary learning experiences into dynamic
8
relationships, resulting in a synergistic process of accomplishment" (p. 5). This research study is intended to identify the factors that contribute to exceptional performance by a library/community agency partnership. The partnership evaluation framework of Alter and Hage (1993) and Mattessich and Monsey (1992) on interorganizational networks and the action research (AR) model of Gray (1989) on the process and phases of partnership collaboration are employed in the analysis of qualitative data gathered.
Definitions of Terms Used The following definitions of terms are provided to make explicit the underlying assumptions employed by the primary investigator in conducting this case study of a library/community agency partnership. Boundary spanners: "Boundary spanners are individuals who engage in networking tasks and employ methods of coordination and task integration across organizational boundaries" (Alter & Hage, 1993, p. 46). Boundary spanners collect and process information for the organization from its relevant environment (Alexander, 1995). Collaboration: "Collaboration involves a process of joint decision making among key stakeholders of a problem domain about the future of that domain. Five features are critical to the process: (1) the stakeholders are interdependent, (2) solutions emerge by dealing constructively with differences, (3) joint ownership of decisions is involved, (4) stakeholders assume collective responsibility for the future direction of the domain, and (5) collaboration is an emergent process" (Gray, 1989, p. 11). "Collaboration is defined as a dynamic, transforming process of creating a
9
power sharing partnership for pervasive application in health-care practice, education, research, and organizational settings for the purposeful attention to needs and problems in order to achieve likely successful outcomes" (Sullivan, 1998, p. 65). Consumer Health Information (CHI): CHI refers to "information on medical topics that is relevant and appropriate for the general public. CHI covers not only information on signs and symptoms, diagnosis, treatment, and prognosis of diseases, but also includes information on access, quality, and utilization of health-care services" (Rees, 1998, p. 1). Cooperation: Cooperation is "the quality of the relationship between human actors in a system consisting of mutual understanding, shared goals and values, and an ability to work together on a common task" (Alter & Hage, 1993, p. 86). Joint projects promote mutual ownership, team building, and conflict resolution processes in interorganizational networking (Wilson, 1990). Coordination: Coordination is "the articulation of elements in a service delivery system so that comprehensiveness, accessibility, and compatibility among elements are maximized" (Alter & Hage, 1993, p. 87). "Coordination involves more resources [and] higher ranked individuals and presents more threat to organizational autonomy than does cooperation" (Pennbridge, 1988, p. 22). Effectiveness: Effectiveness is defined as the "ability [of an organization] to exploit its environment in the acquisition of scarce and valued resources to sustain its functioning" (Hall, 1999, p. 252). Enactment: Enactment is the concept that when people act, they bring structures and events into existence and set them in action. "People, often alone, actively put things out there that they then perceive and negotiate about perceiving. It is that initial implanting of reality that is preserved by the word enactment" (Weick,
10
1979, p. 165). Integrative coordination: "When organizations providing one type of service refer clients to, get information about, and otherwise interact with organizations providing other types of services, the interests of multiple-need clients are served more effectively than if such interaction does not occur. Integrative coordination is the structural integration of different organizations in a network where barriers are permeable, with strong connections existing among the groups" (Bolland & Wilson, 1994, p. 346). Interorganizational coordination (IOC): "Interorganizational coordination is a set of organizations' recognition and management of their interdependence by creating or using IOC structures to decide on their actions together" (Alexander, 1995, p. 271). Coordination structures describe "the relationships or linkages between organizations that have evolved . . . or have been designed . . . to bring about IOC" (p. 277). Coordination tools are "the specific elements of organizational action, interaction, or behavior that enable IOC. Meetings, telephone calls, and shared mailings are examples of tools in informal linkages" (p. 278). Interorganizational relationships (IORs): "An interorganizational relationship (IOR) occurs when two or more organizations transact resources of any kind (money, physical facilities and materials, customer or client referrals, technical staff services). The major processes in an IOR are . . . resource flows and information flows" (Van de Ven & Ferry, 1980, pp. 297, 301). Networking: "Networking is the act of creating and/or maintaining a cluster of networks for the purpose of exchanging, acting, or producing among the member organizations" (Alter & Hage, 1993, p. 46).
11
Networks: "Networks constitute the basic social form that permits interorganizational interactions of exchange, concerted action, and joint production. Networks are unbounded or bounded clusters of organizations that, by definition, are nonhierarchical collectives of legally separate units" (Alter & Hage, 1993, p. 46). Participatory action research (PAR): PAR is a set of theories and research practices built on the intention of democratizing society by increasing control over decision making and extending social justice to the disempowered (Greenwood & Levin, 1998). PAR emphasizes a bottom-up approach to research and emphasizes useful outcomes. PAR deemphasizes the "generalizeability of findings" in favor of localized, individually meaningful action outcomes. Any design can be used as long as the evaluation/research is participant-directed (key informants serve as collaborators) and action outcome-driven. (Scherer & McKee, 1993, pp. 2-3) Partnerships: "Collaborative partnerships represent an intense relationship centered on mutual goals. Wisdom is constructed within the social reality of the partnership as well as within the wider social context in which the partnership exists" (Saltiel, 1998, p. 6). Partnering: Partnering is the cooperative behaviors and commitment to mutual goals and effective outcomes perceived and reported by the members of a partnership or collaborative network. "Partnering involves two or more individuals working collaboratively toward a desired outcome. Effective partnering is characterized by a collaborative mode of working together, resulting in win-win situations" (Sujansky, 1991, p. 3). Qualitative case study research: This type of research refers to "any kind of research that produces findings not arrived at by means of statistical procedures or other means of quantification" (Strauss & Corbin, 1990, p. 17). Case study does not claim any particular methods for data collection or data analysis. Any and all methods of gathering data, from testing to interviewing, can be used in a case study, although certain techniques are used more than others. . . .
12 Researchers are interested in insight, discovery, and interpretation rather than hypothesis testing. By concentrating on a single phenomenon or entity (the case), the researcher aims to uncover the interaction of significant factors characteristic of the phenomenon. The case study focuses on holistic description and explanation" (Merriam, 1998, pp. 28-29). Reflective practitioner: Professionals conduct reflective conversations when solving problems in unique and "uncertain" client cases. In an effort to solve a problem, the practitioner reframes the problem and makes new discoveries that call for new reflection-in-action. "The process spirals through stages of appreciation, action, and reappreciation. The unique and uncertain situation comes to be understood through the attempt to change it and changed through the attempt to understand it" (Schön, 1983, p. 132). Sensemaking: Sensemaking is a thinking process that uses retrospective accounts to explain surprises. People engage in sensemaking because they are confused by too many interpretations. In organizational life, people often produce part of the environments they face through authoritative acts they make. Choosing to act changes what a person knows. Actions create relationships that then become binding or releasing. Sensemaking is a process of making do with whatever resources are at hand (Weick, 1995). Symbiotic relationships: "Symbiotic relationships occur among organizations that may have some similarities but operate in different sectors" (Alter & Hage, 1993, p. 47). Youth services: Any agency providing educational and social support to youth aged 10-18. Youth services include schools, social service agencies, libraries, healthcare providers, churches, voluntary organizations (e.g., Girl Scouts, Young Women's Christian Association [YWCA], and Young Men's Christian Association [YMCA]), and government agencies (e.g., Aurora Township Youth Services, Fox Valley Park
13
District, and Kane County Health Department).
Theoretical Framework and Assumptions There are a number of organizational development theories that influence the AR strategies employed in the TCN partnership case study. This section reviews open systems theory, social exchange theory, an interorganizational collaboration model, transformational leaders as organizing agents, and networks as theories of action and the relevance of these theories for the TCN partnership. Synergy characterized the TCN project as a result of applying these theories and assumptions to the gaps found in community health-information services offered to teens and parents in the Aurora, Illinois, area.
Open Systems Theory The theoretical framework underlying this case study is open systems theory as defined by Katz and Kahn (1978). Organizations are understood to be energic inputoutput systems in which the energic return from the output reactivates the system. "Social organizations are flagrantly open systems in that the input of energies and the conversion of output into further energic input consist of transactions between the organization and its environment" (p. 20). According to Katz and Kahn, organizations can be identified and their function determined by (a) tracing the pattern of energy exchange or activity of people as its results in some output, and (b) ascertaining how the output is translated into energy that reactivates the pattern. Thus, the boundaries of an organization are determined by analyzing the energic and informational transactions as they relate to the cycle of activities of input, throughput, and output. As defined by Katz and Kahn (1978), open systems share 10 common
14
characteristics: 1. Importation of energy: social organizations import some form of energy from the external environment such as people, supplies, or financial resources. 2. Throughput: energy received is transformed and reorganized into new products, services, or processes. 3. Output: the products or services created by open systems are exported into the environment. 4. Cycles of events: the pattern of activities of the energy exchanges is cyclic in nature, and the product exported into the environment furnishes the sources of energy for the repetition of the cycle of activities. For example, voluntary organizations provide expressive satisfactions to their members so that energy renewal comes directly from the organizational activity itself. Open systems can be identified from the input of energy through its transformation to the closure of the energic chain of events. 5. Negative entropy: survival of an open system is based on increasing inputs, maintaining a comfortable margin of operation, and maintaining the ability to transform itself. 6. Information input, negative feedback, and the coding process: open systems react to information signals to which they are attuned and that fit into the meaningful and basic categories for a given social system. 7. Steady state and dynamic homeostasis: open systems maintain some constancy in energy exchange and exhibit a growth or expansion dynamic in which they maximize their basic character. 8. Differentiation: open systems move in a direction of differentiation and elaboration of roles.
15
9. Integration and coordination: integration of open systems is achieved through shared norms and values and coordination results through the functional articulation of tasks and roles. 10. Equifinality: open systems reach the final state from differing initial conditions and a variety of process paths. For the TCN, open systems theory explains how the financial resources, communication, and energy of the professionals who joined the organization contributed to its growth and maintenance over the 18-month grant period. Shared norms and values, the project director, and meaningful projects arose as these inputs were transformed and information services and health education programs were delivered to the community.
Social Exchange Theory Social exchange theory, as defined by Blau (1970), states that individuals become part of organizations for the benefits gained through exchange: "individuals associate with one another because they all profit from their association. . . . They do not necessarily all profit equally nor do they share the cost of providing the benefits equally" (p. 128). Blau believed that beneath the altruism of social life is found an underlying "egoism." Rather than helping others for unselfish reasons, Blau noted that people frequently are motivated by the expectation that doing so will bring social rewards. From this perspective, social structures such as alliances, IORs, networks, and partnerships arise from the repeated exchange of rewards between actors--"human beings tend to be governed in their associations with one another by the desire to obtain social rewards of various sorts, and the resulting exchanges of benefits shape
16
the structure of social relations" (Blau, 1970, p. 129). Social exchange theory explains why individual actors participate in collaborative ventures--benefits are assessed in relationship to the rewards gained, and these rewards motivate the individual to participate and contribute to the group undertaking. As is presented later in partner exit interview comments, the ability to share resources acquired through the grant (books, pamphlets, professional expertise, and health information) with students and their families was a crucial factor in the continuing commitment of many professionals to the library/community agency partnership mission.
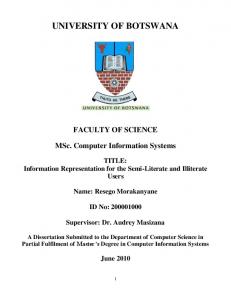
Interorganizational Collaboration Model In contrast to Blau's (1970) social exchange theory, Alter and Hage (1993) argued that both self-interest and moral commitments operate in the rational choices of private and public organizations. There is a desire both to gain more resources and to accomplish exemplary goals. The growth of knowledge in modern society has led to a recognition among decision makers that problems are more complex and that cooperation is the only alternative for solving multidimensional problems. The solution of a complex problem is the joint good. A synthesis of theories of interorganizational collaboration focuses on four driving forces, as summarized by Alter and Hage (1993) in Figure 1.
17
Figure 1. A synthesis of interorganizational collaboration theory (Alter & Hage, 1993, p. 39)
According to Alter and Hage (1993), two conditions must exist for interorganizational collaboration to occur. First, there must be a willingness to collaborate, which is a basic requirement and affects the perception of the costs and benefits involved for potential network members. The willingness to cooperate springs from an awareness and understanding of other organizations' needs and the perception that these are compatible in some way with the needs of one's own organization. Second, organizational members must also believe that collaboration will result in adaptive efficiency--solving a problem with greater speed, flexibility, and quality. In line with Nohria (1992), this synthesis of interorganizational collaboration theories explains the factors that facilitate or impede organizing efforts leading to the creation of a new venture or those that involve mobilizing collective action. After a network is created, there is a continuing need for network maintenance, and transformational leadership is needed to create a collaborative vision and to respond to internal and external change. In the formation of the TCN partnership, potential partners were asked to submit a letter of support and a statement of a minimum amount of professional time devoted to the library/community agency activities. This arrangement formalized each agency's "willingness to collaborate" and set the "ground rules" for future participation (i.e., attendance at meetings and involvement with community health-education
18
programs). The mission of the partnership was also formalized, so partners could clearly see the relationship of their agency's mission to the collaborative activities and measure results. When the grant was awarded to the fledgling partnership in March 1998, the TCN partners believed that their time investment would "make a difference" and improve the gap in community health-information services through efficient, high school-focused programming and outreach to Aurora teens and parents.
Transformational Leaders as Organizing Agents Katz and Kahn (1978) defined leadership as "the exertion of influence on organizationally relevant matters by any member of the organization" (p. 571). Leadership implies that expectations are exceeded over and above mechanical compliance with the routine directives of a network. Leaders provide benefits to their followers and are thus empowered by the group: "If the benefits followers derive from a leader's guidance exceed their expectations of a fair return for the costs they have incurred, both by performing services and by complying with directives, their collective approval of [his or her] leadership legitimates it" (Blau, 1970, p. 135). Even in mature organizations, leadership is needed to address incompleteness of the organization's design, to monitor the changing external conditions in the environment, to achieve internal balance by changing and coordinating the organization's subsystems, and to teach and motivate individual members to perform needed organizational roles. Rolls (1995) defined transformational leaders as managers who broaden and elevate the interests of their co-workers, generate awareness and acceptance of the purposes and mission of the group, and motivate co-workers to look beyond their own self-interest for the good of the whole group. "The new leaders have an extraordinary
19
effect on their colleagues because they create meaning for them" (p. 108). Transformational leadership is central to the type of supportive environment required to facilitate collaboration (Sullivan, 1998). Leaders serve as organizing agents in making change happen through the creation of partnerships and encouragement of self-direction among partnership members. Transformative leaders are effective because they have "a vision of what collaboration can accomplish, sensitivity and the ability to develop relationships with diverse stakeholders, and a sense of optimism and process literacy" (Gray, 1989, p. 279). In retrospect, many members of the TCN believed that the partnership offered leadership development opportunities and provided effective role modeling behaviors among the health-care professionals, educators, and youth services professionals. Provena Mercy Center's medical librarian assumed the leadership of an optimistic, diverse, and motivated group of professionals and worked to transform and mold the organization in line with the evolving vision of community service.
Networks Building on open systems theory, Nohria (1992) described the new model of organization--the network, which consists of lateral and horizontal linkages within and among organizations. Competitive success of networks depends on collaboration with vendors, customers, and market competitors. Networks are described as "strategic alliances" that are responses of organizations to mitigate and manage competitive uncertainties and resource interdependencies. A new set of disaggregated, distributed, and flexible working arrangements among organizations has been made possible as a result of new information technologies and the Internet. According to Nohria (1992), the overall network defines a stable ecology that
20
operates as a learning system. Five basic assumptions underlie the network perspective on organizations: 1. All organizations are social networks and need to be addressed and analyzed as such. Social networks are defined as "a set of nodes (e.g., persons, organizations) linked by a set of social relationships (e.g., friendship, transfer of funds, overlapping membership) of a specified type" (Nohria, 1992, p. 4). Both informal and emergent relationships and formal and prescribed relationships shape the recurring relationships and linkages among the network components. 2. An organization's environment is seen as a network of other organizations. The environment consists of a field of relationships that bind organizations together. 3. The actions (i.e., attitudes and behaviors) of actors in organizations are explained in terms of their position in networks of relationships. An actor's network position and personal attributes (e.g., sex, age, ethnicity, educational level) offer insight into actions taken. 4. Networks constrain actions and in turn are shaped by them. Networks are constantly being socially constructed, reproduced, and altered as the result of the actions of actors. Networks are process and structure, continually shaped and reshaped by the actions of actors who are in turn constrained by the structural position they hold. 5. Comparative analysis of organizations must take into account network characteristics--the pattern of interaction among market players. Network organizations are governed by theories of action, which filter and interpret signals from the environment and tie stimuli to organizational outputs. Theories of action are metalevel systems that supervise the identification of stimuli and the assembling of responses. To identify stimuli properly and to select adequate responses, organizations map their environments and infer what causal relationships operate in their environments. These maps constitute theories of action which organizations elaborate and refine as new situations are encountered. (Weick,
21 1995, p. 121). For the TCN's operations, it was important to recognize the different perspectives and "theories of action" that each agency brought to the partnership. The network notion also meant that the partnership leadership needed to be aware both of formal interactions and informal connections being made among the partner agencies to maximize the desired community outcomes and impact. This summary of open systems, social exchange, interorganizational collaboration, transformational leadership, and network theories reveals the assumptions and cognitive maps that the primary investigator brought to the table about network development and potential partner buy-in. These assumptions and cognitive maps influenced the direction taken by the partnership's project director and leadership team as the TCN expanded and identified health-information access issues and solutions, employed community networking technologies, and developed youth service projects. Significance of the Study for Research and Practice The research described in this dissertation reflects the trend in our contemporary, knowledge-based society toward an increased number of partnerships, alliances, and interorganizational networks in business, education, government, and health and human services (Alexander, 1995; Bazzoli, Stein, Alexander, Conrad, Sofaer, & Shortell, 1997; Hall, 1999; Hord, 1985; Mays, Halverson, & Kaluzny, 1998; Scott & Thurston, 1997; Wilson, 1990). There is an increasing awareness of the interdependence between the health and human service sectors and the need for the provision of basic services directly to youth in the school setting. School-based services support the creation of "connections" and emotional bonds to the community
22
at large and improve the quality of life for students (Blum & Rinehart, 1997; Dryfoos, 1994; Giloth & Jellen, 1989; Wang, Haertel, & Walberg, 1993). The research described in this dissertation enhances our understanding of the development and interpersonal dynamics of partnerships in addressing critical community healthinformation needs and in working toward personal growth and social change. The literature reveals the importance of community-wide coalitions for youth development, prevention, health promotion, and service delivery (Barton, Watkins, & Jarjoura, 1997; Butterfoss, Goodman, & Wandersman, 1993; Cheadle et al., 1998; Feinberg & Feldman, 1996; Gamm, 1998). Many writers stress the importance of partnerships in working with families to develop needed health decision-making skills and to share knowledge of available health and social services. The research described in this dissertation highlights the role that the partnership assumed in improving access to health information for teens and parents. According to a group of social scientists studying organizations, there is great research potential for IOCs and the exploration of a continuum of interorganizational networking processes (Hall, 1999; Ring & Van de Ven, 1994; Wilson, 1990). For example, Wilson (1990), in summarizing her research on a New York State network of 18 adolescent pregnancy prevention agencies, noted that a continuum of interagency networking exists that initially functioned with mutual support, moved into joint projects, and built toward collaborative planning and programs. Understanding this process is key to implementing new programs in all areas of youth services partnership development and practice. Ring and Van de Ven (1994) stressed that "personal relationships can serve to shape and modify the evolving structures of a cooperative IOR" (p. 93), and this is an area of potential investigation in IOR research. Bazzoli et al. (1997) noted that much research on organizational collaboration has focused on
23
partnership formation, and thus, more research is needed to document partnership action in health and human services alliances and networks. This research is also valuable because it contributes to a further understanding of how partnerships function as learning organizations for the library and community agency partners involved (Millard, 1999; Recardo, Molloy, & Pellegrino, 1995; Rowley, 1997; Sullivan, 1998; Watkins & Marsick, 1993). Through exploration of a mutually defined problem, the members involved in the partnership addressed their uncertainties, became engaged in continuous learning, and defined solutions to improvements in health-information delivery to teens and parents. As a result of this process, information was collected, widespread access to that information was provided on the partnership's website, rewards and recognition for learning and improvement were provided to the partners and teens, and sharing of what was learned was collectively and continuously made possible through the website, seven days per week, 24 hours per day. "Coalition formation and utilization is all about responding to change and complexity through connections" (Sullivan, 1998, p. 253). In the case of the TCN partnership, the connections were and continue to be human and electronic linkages. The findings of this case study are particularly relevant to managers of community networking agencies and library administrators as they seek to build connections with other organizations to share human and technical resources more effectively. Finally, AR contributes to a redefinition of the roles of libraries and librarians in community development, health and human service networks, and violence prevention. The "virtual library" of health-information resources developed on the Internet at www.aurora.il.us/teencare for teens and parents in Aurora transformed librarians into community activists and leaders in the health and wellness movement.
24
Nagle (1996) wrote that quality initiatives in health science libraries are best served if the client base for health information is broadened to reach "distributed communities." The TCN is a project that extends the reach of librarians and multitype libraries into the local Aurora community. The grassroots professional networking and collaboration that occurred in the TCN partnership contributed to the updating and electronic publication of the Healthy Teens Handbook (Kane County INFO, 1994) and to online coordination of available community health and social service resources in the greater Aurora area. The TCN's website makes community health and human service agency programs more visible and easily accessible for teens, parents, and the professionals serving this important segment of our local community.
CHAPTER 2 REVIEW OF THE LITERATURE
Youth Violence As a Public Health Issue
Recent Reports in the News Media Reports of children killing children in small towns, seemingly safe havens for raising families, have dominated the headlines of newspapers and television news broadcasts over the last four years. The small towns of Jonesboro, Arkansas; Springfield, Oregon; Pearl, Mississippi; West Paducah, Kentucky; Littleton, Colorado; and most recently, Mt. Morris Township, Michigan, have been touched by the tragedy of school violence and senseless, untimely deaths of innocent youth and their teachers. As consumers of these news reports, we sense the sadness and anger of family members and friends of these victims of school violence. Outrage and empathy for the victims and their families dominate editorials in local newspapers and television news stories concerning these violent, senseless, and tragic events. Government and school officials struggle with the reasons for and solutions to these recurring episodes of school violence. Clergy point to the erosion of moral values in our homes and communities, and psychologists stress the break-up of the traditional family unit, a cultural history of violence, and the mass media as causes of the increased violence in American society. Unfortunately, the news media stories of school violence are reinforced with hard statistics that illustrate the great potential for violence in our schools. Dwyer (1998), a school psychologist, reported that 250,000 or more weapons will be
26 "sneaked" into school this year (Lash, 1998, p. 12). The National Center for Health Statistics reported that 14 children per day were killed with guns in 1997. FBI statistics reveal that approximately 420 children die every month from gunshot wounds (Hill, 1997). A recent study by the National School Safety Center found that there have been 220 violence-associated school deaths since 1992 (Illinois Attorney General, Advisory Group on School Safety and Firearms, 1998). In a recent survey of adolescent health risk behaviors, 24.2% of respondents reported that guns were easily accessible at home (Resnick et al., 1997). The media stories and statistical data show that weapons are readily available and have deadly consequences for both school children and school personnel. Weapons in the hands of angry youth have significantly changed our concept of schools as "safe havens" for students and school personnel. Gun control legislation has come to the forefront among a number of possible solutions to the ready availability of guns in homes and school buildings, and an Associated Press poll shows that gun control is a key issue in the 2000 presidential election, with most Americans wanting tougher gun controls (Lester, 2000). Responding to the recent wave of highly publicized school shootings, President Clinton urged states and Congress in July 1998 to support measures that would punish adults whose guns are used by children to commit crimes (Greene, 1998). Fifteen states already have a law that targets adults whose firearms are taken by a child to kill or injure someone. These states have made adults legally responsible for injuries or deaths caused by unsecured handguns. The latest events in Littleton, Colorado, and Mt. Morris Township, Michigan, have caused the U.S. Congress to rekindle its debate on appropriate gun control measures. In June 1999, Illinois passed the Safe 2 Learn program endorsed by the
27 Advisory Group on School Safety and Firearms through the Office of Illinois Attorney General Jim Ryan (Illinois Attorney General, Advisory Group on School Safety and Firearms, 1998). Governor George Ryan signed the bill into law to provide financial support to schools that want to develop school safety plans and conduct training programs for staff and students on appropriate school safety measures. The Illinois Violence Prevention Authority plans to administer a grant program to local schools to develop school safety plans and inservice training programs for teachers, parents, and students. In addition to the federal government and state of Illinois, a number of private organizations are involved in initiatives to reduce the availability of handguns to youth and criminals. A recent report in the Houston Chronicle describes the current efforts of the Center to Prevent Handgun Violence in soliciting the medical community's help in teaching youngsters that guns can kill and urging firearm owners to lock up their weapons when not in use. Sarah Brady, the group's chairman, indicated that the Washington-based center plans "to distribute brochures and posters to doctors and their aides, encouraging them to tell young patients and parents that guns intended for protection can end up killing family members if left within children's reach" (Lash, 1998, p. A-12). A number of health-related organizations are involved in violence prevention initiatives. The American Academy of Pediatrics is working on a public awareness program to curb youth violence in 1999. The American Medical Association (AMA) Alliance is continuing its implementation of the Stop America's Violence Everywhere (SAVE) initiative that has taught more than 300,000 children effective ways to manage anger (Booth, 1999; Potts, 1999). The AMA is stepping up its safer schools and antibullying activities as a result of the Littleton, Colorado, high-school massacre.
28 During the last two decades in the U.S., violence among youth has increased dramatically in numbers and severity despite an overall decline of violence in society in general. Since 1988, the adolescent homicide rate has more than doubled to become the second leading cause of death among Americans ages 15-24 (Hamburg, 1998). In Illinois, the rate of teen deaths by accident, homicide, or suicide increased has 42.0% since 1988, although it rose only 3.0% nationally during the same time period. Jerome Stermer of the Chicago-based Voices for Illinois Children emphasized that "there's no talking ourselves out of the reality that we've got real problems with violence among adolescents. It's not something we can skip over or say it's not about my neighborhood" (Beaupre, 1998, p. 16).
Professional Views on Youth Violence Physicians, educators, and public health professionals perceive youth violence as a critical public health problem that requires community-wide initiatives to be reduced. Dr. David Satcher, who became U.S. Surgeon General in 1997, perceives violence as a public health problem tied to poverty and racial injustice. Satcher, who was formerly the director of the Centers for Disease Control (CDC) and Prevention, perceives the solution to violence in prevention, not punishment: One of the strategies we have to use in dealing with the problem [of violence] is prevention; understanding what are the conditions that give rise to violence, whether those conditions are environmental or mental health. . . . We believe some of the homicide we're seeing arises from . . . ideation; in other words, people are in an environment where they feel hopeless. This is especially true for some of the Black youth in the inner city; growing up in an environment that has them believing they are not going to live past 20 or 25; living with a lot of anger and a lot of hopelessness and therefore putting themselves and others in harm's way by their behavior. Violence is one of the forms of that behavior. (Christian, 1998, pp. 2-3) Dr. Deborah Prothrow-Stith (1996), a former emergency-room physician and currently a professor with the Harvard University School of Public Health, agreed with
29 Dr. Satcher that public health, with its prevention-oriented approach, has a huge untapped potential for reducing violence. Public policy issues on violence fail to address the most common kind of violence--violence between people who know each other. According to Dr. Prothrow-Stith, approximately half of the homicides in the U.S. occur between people who know each other, who get into an argument, who are drinking alcohol, and who have a handgun. "Gangs, sociopathic personalities, and basic bad guys" (Prothrow-Stith, 1996, p. 21) are not responsible for most of the violence in the U.S.
Strategies for Reducing Youth Violence Prothrow-Stith (1996, 1997) stressed that violence prevention requires a change in fundamental aspects of American society and its values. First, we must stop perpetuating the "spirit of meanness" in the U.S. Second, we need to learn how to get along with each other as adults. Third, we need to teach our children how to get along. Fourth, we need to redefine the "hero" in our society. Fifth, we need to celebrate nonviolence. Sixth, we need to concentrate on primary and secondary prevention--spend time, attention, money, and resources early in the development of children and in a preventive way. Prothrow-Stith believed American society must literally build healthy communities around all of its children. Parents and professionals need to assume the role of "advocate" by calling television stations, elected officials, and influential community leaders. Advocates can convince U.S. congressional leaders that the costs of violence are astronomical both economically and socially; each year violence costs the United States $64 billion (Hill, 1997). The AMA (1993) reported that the direct medical costs of violence-related
30 injuries add over $5.3 billion to U.S. health-care expenditures. The major economic and social impact of violence leads many professionals to the conclusion that effective solutions must be implemented to reduce interpersonal violence and resolve conflicts peacefully in our communities, schools, and families. In a recent American Medical News article, physicians were urged to discuss gun safety with patients (Stapleton, 1999).
Youth Development and an "Ethic of Care" Writers such as Noddings (1992), Lantieri and Patti (1996) and McGinnis (1993) have envisioned a need for developing an "ethic of care," with an emphasis on emotional intelligence and prosocial skills, which reaches the "hearts" of students and which teachers and administrators can model in our schools. Schools need to build ideas and minds, exchange information, and stimulate personal development, but they also play an important part in transmitting values to our children in a turbulent and often confusing world of mixed messages. Schools play a key role in reducing youth violence by providing support to parents and collaborating with "experts" from community agencies. Lasley (1994) perceived the solution to violence in the teaching of "selflessness" in American society--"an extra-centeredness where the person learns to feel with and for others: empathy, tolerance, brotherhood" (p. 3). Noddings (1992) believed school curricula need to be restructured around "centers of care" that encourage the growth of competent, caring, loving, and lovable people. The Josephson Institute's "Character Counts" curriculum and the Joseph P. Kennedy, Jr., Foundation's Community of Caring program for schools are examples of programs developed to inculcate basic values to youth for the strengthening of families and community ties.
31 Many writers see future success in violence reduction as a total community undertaking. Kolbe et al. (1993) stated that "success in reducing health risks will require a focused, sustained, concerted campaign that integrates the efforts of parents, families, schools, health and social service agencies, religious organizations, media, and young people themselves" (p. 8). Elliott et al. (1998) cited research that shows the need for early, comprehensive interventions in the lives of at-risk children and families in improving their ability to prevent aggressive behavior and later violence-related outcomes in schools and communities. Partnerships and Partnering as a Youth Violence Prevention Strategy Because many writers point to the importance of community partnerships in reducing violence, the following literature review defines and examines the key processes and structures involved in partnership formation and implementation: (a) the interpersonal dynamics in forming and implementing a partnership; (b) the phases of partnership development; and (c) partnerships as a form of IOR. Partnering as Interpersonal Behavior and Enactment Sujansky (1991) noted that efffective partnerships have three main ingredients: (1) a vision of what the partners want to accomplish and how they will use partnering to get there; (2) a commitment to specific goals as well as to the partnership; and (3) a plan of action to accomplish these goals, including responsibilities, project resources, and deadlines. In her research on a 10-year-old New York State adolescent pregnancy prevention partnership, Wilson (1990) found that the strength of interorganizational networking and reciprocity was based on the fact that the activities were consistent
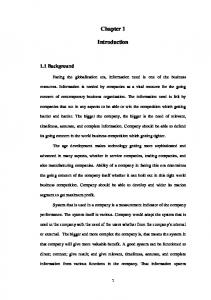
32 with members' values and tied to negotiation among the members in reaching "common ground." Sujansky (1991) believed that the establishment of partnering relationships is critical to the effectiveness of an organization. Partnering contributes to the overall growth and success of an organization in solving problems and seizing opportunities. Sujansky identified ten behaviors for successful partnering within an organization or corporation that are depicted in Figure 2.
Figure 2. Ten behaviors for successful partnering (Sujansky, 1991, p. 17)
The partnership model presented by Sujansky (1991) outlines processes that
33 foster partner agency agreement about the diagnosis and solutions for an existing problem or that support research activities to seize a new opportunity. "Partners use insight to search for others who are well-matched, who have a vested interest in the goal, and who are willing to work mutually and collaboratively" (p. 41). This model is supported by and includes a number of elements from the performance technology and AR models (Mager & Pipe, 1984; Stolovitch & Keeps, 1992; Stringer, 1996). The literature of IORs also cites the need for more research into the interpersonal dynamics of partnership building, a neglected area of partnership research (Hall, 1999; Kanter & Eccles, 1992). Due to these gaps in research on "partnering behaviors," this research project covers the interpersonal dynamics of partnership building based on partner evaluations of the TCN using the Sujansky (1991) "partnering behaviors survey" (see Appendix A for a copy of the survey). From Sujansky's model, it is expected that successful partnerships consist of interpersonal relationships among the members that reflect high levels of vision, commitment, risk-taking, creativity, recognition, flexibility, and challenge. The TCN is assessed using this partnership relationship building model adapted from the corporate world. Partnerships and Collaboration as Negotiated Order Gray (1989) defined collaboration as a method for solving interorganizational problems and managing interdependence: Finding creative solutions in a world of growing interdependence requires envisioning problems from perspectives outside our own. We need to redesign our problem-solving processes to include the different parties that have a stake in the issue. Achieving creative and viable solutions to these problems requires new strategies for managing interdependence. (p. xviii) Interdependence is a basic fact of interorganizational coordination, as found in this
34 definition from Alexander (1995): "Interorganizational coordination . . . is a set of organizations' recognition and management of their interdependence by creating or using IOC structures to decide on their actions together" (Gray, 1989, p. 271). From these two definitions, certain common conceptual elements arise: problem-solving, managing interdependence, multiple stakeholders, decision-making and creating structures/ action-taking or enactment. Gray's (1989) concept of collaboration as "negotiated order" is important because it emphasizes the perceptions of the partnership members in creating and continually redefining the organizational context. Negotiated order is "a social context in which relationships are negotiated and renegotiated. The social order is shaped through the self-conscious interactions of participants" (p. 228). Gray introduced the concept of "appreciation" to reflect the changes that occur as the partnership matures. Arriving at a negotiated order requires joint appreciation. An essential notion of appreciation is the power of collective thought to transform existing circumstances. This "myth-making process occurs during collaboration as stakeholders negotiate an image of their desired future. Myth making involves abandoning existing interpretations and creating new or expanded interpretations for existing problem domains" (Gray, 1989, pp. 271-272). Gray's (1989) notion of "negotiated order" to describe the process of collaboration is similar to the "sensemaking" and "enactment" concepts of Weick (1979, 1995) regarding organizing and organizational behavior. Colloborative processes unleash catalytic power and mobilize joint action among the partnership's stakeholders. Three conditions in the group produce social energy: first, ideas about what to accomplish and what actions to take; second, shared values about how to accomplish desired ends; and third, a climate of trust in which to proceed. The
35 primary advantage of collaboration abides in its transformative potential. "Acting together, stakeholders muster the social energy to introduce desired change" (p. 271). And as a partnership evolves, the members develop an appreciation of the contributions by individual members to the total group effort and partnership outcomes.
How and Why Partnerships Emerge Van de Ven and Ferry (1980) noted that "organizations do not coordinate for coordination's sake. Instead, organizations strain to maintain their autonomy" (p. 307). Two compelling reasons for interagency activity are: (1) an internal need for resources (resource dependency model), and (2) a willingness to respond to an external problem, opportunity, or mandate (system change model). Thus, the emergence and functioning of partnerships as a form of IOR is viewed by Van de Ven and Ferry (1980) as a result of: (1) a need for resources or a response to external issues, (2) interorganizational communications to spread awareness and consensus, (3) resource transactions, and (4) structural adaptation and pattern maintenance over time. From this viewpoint, partnerships emerge to reduce environmental turbulence and increase the stability of organizations in the face of rapid change through the sharing of resources (people, expert knowledge, information, materials, etc.).
How IORs Evolve Ring and Van de Ven (1994) examined the developmental processes of cooperative IORs. From their developmental process perspective, Ring and Van de Ven (1994) defined cooperative IORs as "socially contrived mechanisms for collective action, which are continually shaped and restructured by actions and symbolic
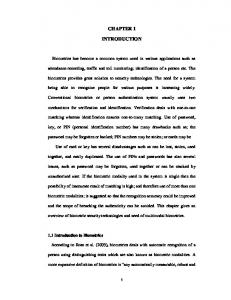
36 interpretations of the parties involved" (p. 96). IORs consist of a "repetitive sequence of negotiation, commitment, and execution stages, each of which is assessed in terms of efficiency and equity" (p. 97). Figure 3 presents the Ring and Van de Ven IOR development process model. Although Ring and Van de Ven (1994) focused on cooperative IORs, a macrolevel phenomenon, IORs only emerge, evolve, grow, and dissolve over time as a consequence of individual actions. The authors believed that the developmental processes associated with cooperative IORs are cyclical, not sequential, and that IORs are maintained due to balance--balance between formal and informal processes. There are three ways in which the actions of individuals are seen to have an effect on a cooperative IOR: (1) in defining the degree of uncertainty associated with the exchange, (2) in specifying the extent to which the parties can rely on interpersonal trust as an alternative form of conflict resolution, and (3) in defining the parties' outcome expectations to include both efficiency and equity. Agencies become committed to a partnership when principles of efficiency and equity are applied fairly to group transactions.
Trust and Personal Relationships A number of authors have stressed the importance of trust as an important factor in evolving interorganizational and collaborative relationships (Alter & Hage, 1993; Ring & Van de Ven, 1994; Sujansky, 1991; Sullivan, 1998). Trust "emphasizes faith in the moral integrity or goodwill of others, which is produced through interpersonal interactions that lead to social psychological bonds of mutual norms, sentiments, and friendships in dealing with uncertainty" (Ring & Van de Ven, 1994, p. 93). Over time, personal relationships increasingly supplement role relationships in a
37 cooperative IOR. The personal bonds that flow from congruent sense making and congruent psychological contracts are likely to produce trust in
38
Figure 3. Process framework of the development of cooperative IORs (Ring & Van de Ven, 1994, p. 97)
39 the other party's goodwill, or if the goodwill preexists, it will give the parties greater flexibility to transcend their organizationally specific roles in adapting to changing circumstances. The embedding of friendship ties to formal role relationships-personal and professional--provides dual bases for the resolution of conflicts. Alter and Hage (1993) cited research studies from Sweden that found the sharing of technical, organizational, commercial, or market information leads to adaptiveness, and it is success derived from IOR adaptiveness and relationship building that also contributes to the development of trust. There are powerful social-psychological motivations for preserving relationships that entail transaction-specific investments. The investments include not only economic and technological resources of participating agencies but also social commitments and entanglements of individual agents (Ring & Van de Ven, 1994). IORs fulfill individual partner needs for inclusion, predictability, and security. In their article, Ring and Van de Ven (1994) concluded that trust builds over time but, once in place, reduces transaction costs in a partnership: Trust in the goodwill of other parties is a cumulative product of repeated past interactions among parties through which they come to know themselves and evolve a common understanding of mutual commitments. The greater the ability to rely on trust, the lower the transaction costs (time and effort) required of parties to negotiate, reach agreements, and execute a cooperative IOR. (p. 110) As these authors suggest, high levels of trust developed in a partnership promote quicker program start-up, group decision-making, goal attainment, and overall project effectiveness. Technology, Learning, and Knowledge Production A complementary perspective is provided by Osborn and Hagedoorn (1997) in their review of the literature on IORs. Osborn and Hagedoorn described the
40 "interorganizational field perspective" on alliance and network relationships. The interorganizational field in which a firm is embedded is viewed as a characteristic of that firm's environment. This perspective "provided a foundation for many current studies emphasizing technology and organizational learning, social and individual dynamics, and institutionalization" (p. 269). Three research directions are derived from the field perspective. First, changing technological conditions require agencies to make mutual adjustments and to seek varied learning opportunities through alliances. Numerous recent studies have suggested that the use of alliances has been common in areas in which agencies face daunting technological challenges. An organizational learning framework focuses on collaboration as a response by organizations to environmental changes demanding improvement in their know-how and competencies, their technological expertise, or both (Alter & Hage, 1993; Osborn & Hagedoorn, 1997). From this perspective, alliances speed up the learning curve because individuals and units do not need to unlearn traditional routines. Cooperative learning that occurs within alliances and networks increases a firm's learning capacity due to the cooperative learning context found in partnerships. A second interorganizational field approach is the emphasis on social and individual characteristics in operating networks. Osborn and Hagedoorn (1997) claimed that "the important role of individuals in operating alliances remains virtually unexplored" (p. 271). The study of developing and managing nonhierarchical relationships is particularly important for the voluntary, emergent patterns of relationships found in many alliances and networks. A third approach tied to the interorganizational field perspective focuses on the process of institutionalization or "institution building." This perspective is concerned
41 with "socially constructed action takers" (Osborn & Hagedoorn, 1997, p. 272) and is important in understanding how and why common alliance practices emerge, are copied over time, and eventually become generally accepted practice. In the "interorganizational field perspective," alliances and networks are conceptualized as solving economic, technical, and strategic problems for their sponsors by developing, producing, and marketing goods, services, and knowledge (Osborn & Hagedoorn, 1997). The institutional view focuses attention on the alliance itself and on the successful rules of association that are based on reciprocity and balanced exchange rather than on bounded self-interest as found in a market or in a hierarchical organization. The "interorganizational field perspective" suggests that partnerships arise as a result of the need to implement new technologies; stimulate learning; and share expertise on a voluntary, informal basis. Partnerships are seen to stabilize environmental turbulence through the sharing of expertise in the face of technological challenges posed to individual organizations.
Resource Dependency According to Galaskiewicz (1985), resource dependence is a primary motivator for organizations to join partnerships and alliances: Participants will join in a collective action if there are selective incentives made available to them. Organizations may be lured into collective action because the collective actor controls resources they value and cannot get elsewhere. At the same time they are bringing about changes in the institutional environment, collective actors may have to monopolize control over some divisible resource in order to provide selective incentives to their membership. At this point, resource dependency theory once again becomes important. (p. 295) Resource dependency theory assumes organizations enter into relationships to
42 obtain needed resources. The assumption is that resources are scarce, that organizational survival is due to the extent that organizations can outmaneuver each other in the acquisition of scarce resources, and that relations are asymmetrical between organizations (Pennbridge, 1988). Given a scarce resource perspective, the collective interest is best served by distributing resources selectively and strategically by the network coordinator in cooperation with partnership members. "The direct procurement of facilities, materials, products, or revenues to ensure organizational survival has been an overriding reason for establishing interorganizational relations" (Galaskiewicz, 1985, p. 282). Thus, organizations join partnerships to obtain needed resources and to maximize benefits for organizational members via coordination.
Reciprocity, Exchange and Domain Consensus Oliver (1990) noted that relationships between organizations can also be based on reciprocity. Motives of reciprocity emphasize cooperation, collaboration, and coordination among organizations, rather than domination, power, and control. Assumptions underlying approaches to IORs based on reciprocity include the possibilities that "(1) resource scarcity may induce cooperation rather than competition; (2) the process of linkage formation typically will be characterized by balance, harmony, equity, and mutual support rather than by coercion, conflict, and domination; and (3) potential partners will anticipate that the benefits of forming a linkage far exceed the disadvantages, particularly the loss of decision-making latitude and the cost of managing the linkage. Oliver (1990) identified determinants of IORs in a comprehensive review of the literature. According to Oliver, domain consensus (the degree to which
43 organizations accept each other's claims to specific goals and functions) has facilitated the formation of many different types of social service sector IORs. Oliver also concluded that much research has shown that the greater the degree of domain consensus among or between public sector or social service sector organizations, the higher the probability that these organizations will establish relations. Domain similiarity is another factor identified by Oliver (1990) that influences the formation of IORs. This concept refers to the similiarity of agencies' services, clients, and outputs. "When organizations have moderately similar domains, they are likely to have complementary resources" (p. 255). Oliver agreed with the resource dependency perspective that agencies establish links with community and government sponsors in order to reduce the uncertainties of resource acquisition. Partnerships that consist of a representative mix of organizations offer complementary resources to their members and enhance reciprocity and exchange. These partnerships are described by Alter and Hage (1993) as symbiotic.
Partnership Development Phases Gray (1989) identifies three phases in the formation of partnerships: (1) problem setting, (2) direction setting, and (3) implementation. Gray indicated that common issues arise repeatedly and conform to this general sequence independent of the specific circumstances and content of the negotiations among the various parties involved.
Phase 1: Problem Setting Problem setting encompasses arriving at a common definition of a problem. Multiple sources of information are necessary to foster as complete an understanding
44 of the problem as possible. Stakeholders involved include those whose expertise is essential to constructing this comprehensive picture. Awareness of the interdependence of the stakeholders occurs as they work together in gathering information and identifying other organizations that have a stake in solving the problem. A convening organization or "convener" invites and persuades other stakeholders to participate. At this point in the partnership, resources are needed to launch the deliberations, to fund joint information search, and to pay for the services of one or more mediators. These problem-setting tasks are outcomes of this first phase and serve as "critical preconditions" for later phases (Gray, 1989).
Phase 2: Direction Setting Direction setting involves stakeholders in the identification of the interests that brought them to the table, the articulation of the values that guide their individual pursuits, and the development of a sense and appreciation of a common purpose and direction. Ground rules outline acceptable and unacceptable behavior for parties and remove some uncertainty for participants and lessen the likelihood of misunderstandings. Agenda setting requires that important issues be considered, with none of the legitimate stakeholders left out of the process. Organizing subgroups or task forces to deal either with a large number of issues or the circumstance of the number of stakeholders exceeding the 12-15 member limit for effective group functioning also occurs during this phase. Joint information search, managing complex or controversial data, involving third parties in the information search, and exploring all options precede reaching agreement among the stakeholders and finalizing the agreement.
45 Phase 3: Implementation Phase 3, implementation, involves issues that include dealing with constituencies, building external support, structuring and monitoring the agreement, and ensuring compliance. During implementation, the stakeholders need to create longterm structures to support and sustain (a) their collective appreciation, (b) a forum for future problem solving, and (c) a regulative framework for the domain (Gray, 1989).
Summary of Gray's Model Partnerships evolve in a temporal sequence of problem setting, direction setting, and implementation. A sense of interdependence and mutuality arises among the members, and social structures (roles and a division of labor) are defined as the members make decisions crucial to the maintenance of the partnership. Common Characteristics of Interorganizational Networks Alter and Hage (1993) asserted four normative characteristics common to all forms of interorganizational networks and noted that networks can be analyzed in terms of their (a) processes (coordination), (b) technologies, (c) structures, and (d) performances. The four normative characteristics held in common by all interorganizational networks or partnerships are (1) interorganizational networks are cognitive structures; (2) interorganizational networks are nonhierarchical; (3) interorganizational networks have a division of labor; and (4) interorganizational networks are self-regulating. These normative characteristics of partnerships are elaborated below. Interorganizational Networks Are Cognitive Structures
46
A mutually shared conceptual framework must be held by the individuals who have common perceptions about their mutual technical competencies and who have made similar judgments about strategies relative to their environments. In this exchange relationship, each party to the partnership has mutual knowledge of the other's capabilities, their own needs, and the match between the two. These cognitive structures build both commitment and trust. Although there is agreement on the objectives of the partnership, there can be disagreement over the methods and strategies to be used. This is an area of conflict management for the partnership's leadership. Interorganizational Networks Are Nonhierarchical Networks, unlike bureaucracies, are composed of lateral linkages. The defining elements in a partnership are joint decision making and problem solving. Networks dominated by one large organization are often less effective and riddled by conflict, delays, and errors. Interorganizational Networks Have a Division of Labor Each agency brings a technical competency to the interorganizational network. Failure to demonstrate this competency can lead to a termination or failure of the relationship, but once demonstrated, it results in mutual dependency. "This division of labor also militates against the development of a dominant actor who attempts to control the network" (Alter & Hage, 1993, p. 79). Interorganizational Networks Are Self-Regulating
47
Order in networks is achieved through negotiation and mutual adjustment. Solidarity is achieved through democratic principles and diffusion of power. Due to the increasing complexity of the environment, self-regulation and interde-pendency are key factors in making the necessary adjustments for survival as a network.
Summary of Alter and Hage's Model Partnerships as a form of interorganizational networks exhibit several key elements, which include cognitive structures among the members, collegial relationships, a division of responsibilities among the members, democratic decision-making, and a diffusion of power. These elements influence the mission and objectives of the partnership and contribute to the "negotiated order" that results.
Evaluation of IORs Alter and Hage (1993) identified four models of assessing interorganizational networks, which are drawn from the earlier work of Yuchtman and Seashore (1979). These are the goal model, system-resource model, internal process model, and strategic constituencies model. The definition of effectiveness employed by these authors emphasizes the multiple stakeholders' evaluations of the network: "Effectiveness in interorganizational systems is a perception among administrators and workers that their collective effort is achieving what it was intended to achieve, that it works smoothly, and that is is reasonably productive" (Alter & Hage, 1993, pp. 197198). Figure 4 presents the four alternative models for assessing interorganizational networks. Hall (1999) introduced models of organizational effectiveness and indicated that a "contradiction" model of effectiveness is more appropriate than an overall
48 concept of organizational effectiveness. The models Hall introduced include systemresource model, goal model, participant-satisfaction model, and dominant coalition/constraint model. According to Hall (1999), "Achieving a goal on top of the constraint is effectiveness" (p. 264). "The effectiveness-for-whom issue" is crucial in an effectiveness formulation" (p. 266).
A network system is effective to the extent that
Useful when
Goal model
...it accomplishes its consensual goals.
...goals are clear and not measurable.
System-resource model
...it acquires needed resources.
...inputs can be specified and measured.
Internal process model
...it has an absence of strain and exhibits smooth internal functioning.
...there is clear causal connection between internal processes and desired output.
Strategies constituencies model
...all strategic constituencies are at least minimally satisfied.
...constituencies have powerful influence.
Theoretical Model
Figure 4. Four models of assessing interorganizational networks (Alter & Hage, 1993, p. 196)
Different parties are affected in different ways by organizational actions. There are compromises that must be made among pressing constraints, goals, constituents, and time frames. The ordering of the compromises is based on power relationships and coalitions within the organizations, coupled with external pressures. . . . It is quite clear that controlling the relevant environment, over time and conditions, and structuring the organization to acquire sufficient resources and to pursue and move to accomplish major goals is a key to any consideration of effectiveness. (Hall, 1999, pp. 269-270, 272) For Hall, effectiveness is dependent on resource acquisition, goal attainment, and the views of the multiple stakeholders involved in the network. Zammuto (1984) described how organizational effectiveness models have evolved over time from goal-based and systems-model approaches to "multiple constituency models." Multiple constituency models, unlike the goal and systems
49 approaches, derive criteria for assessing effectiveness from the preferences of multiple constituencies for the outcomes of organizational performance. From this viewpoint, organizations are seen as "intersections of particular influence loops, each embracing a constituency biased toward assessment of its own exchanges within the loop. . . . Constituent preferences for organizational performance are the raw materials on which evaluations of organizational effectiveness are based" (pp. 606, 614). This research study seeks to present the multiple viewpoints of the TCN stakeholders as suggested by the literature review findings. In concluding this section on the evaluation of IORs, it is clear that no one model of interorganizational effectiveness is adequate to explain the factors influencing effective partnerships. Current literature reveals that a multidimensional evaluation model best addresses the concept and operationalization of interorganizational effectiveness--goals, resources, group processes, and the perceptions of key constitutencies involved. Factors Influencing the Success of Partnerships In their review of the literature on successful partnerships, Mattessich and Monsey (1992) identified 19 factors that influence the success of collaborations formed by human service, government, and other nonprofit agencies. The 19 factors fall into six categories: (1) environment, (2) membership, (3) process and structure, (4) communication, (5) purposes, and (6) resources.
Environmental Success Factors Environmental factors that affect the success of a partnership encompass three areas. First, a history of collaboration or cooperation exists in the com-munity and
50 offers the potential partners an understanding of the roles and expectations required in collaboration and enables them to trust the process. Second, the collaborative group is perceived within the community as a leader in regard to the goals and activities the partnership intends to accomplish. Third, the political leaders, opinion-makers, persons who control resources (e.g., the United Way or City of Aurora), and the general public support the mission of the collaborative group.
Membership Characteristics Membership characteristics that have an impact on the success of a partnership as derived by Mattessich and Monsey (1992) from their review of the literature include (a) mutual respect, understanding, and trust for each other and each respective organization; (b) appropriate cross-section of members from the community who will be affected by the partnership's activities; (c) members' belief that the benefits of collaboration will offset costs such as loss of autonomy or "turf"; and (d) compromise among collaborating partners.
Process and Structure Factors related to process and structure focus on five issues. First, members of a collaborative group share a stake in both process and outcome and feel "ownership" of the way the group works and produces its work. Second, every level within the partnership participates in decision making. Third, the partnership remains open to varied ways of organizing itself and accomplishing its work. Fourth, the collaborating partners clearly understand their roles, rights, and responsibilities and how to carry out those responsibilities. Fifth, the collaborative group has the ability to sustain itself in the midst of major changes, even if it needs to change some major goals or members
51 in order to deal with changing conditions.
Communication Communication factors of importance in successful partnerships include open and frequent communication and established informal and formal communication links. Successful partnerships convey all necessary information to one another and to people outside the group. Members formalize communications in writing to ensure information flow, but they also establish personal connections that contribute to an informed and cohesive group working on a common project (Mattessich & Monsey 1992).
Purpose Purpose covers the goals and objectives, shared vision, and unique purpose of the partnership. According to Mattesich and Monsey (1992), goals and objectives need to be clear to all partners and realistically attainable. Collaborating partners need to have the same vision with clearly agreed upon mission, objectives, and strategy at the time of formation or as the partnership works together. The missions and goals or approach of the collaborative group differs in part from the mission and goals of the member organizations.
Resources Partnership resources must be adequate and consistent to support its operations. And the individual who convenes the collaborative group must have organizing and interpersonal skills to carry out the role with fairness. As a result of
52 these personal skills and characteristics, the convener is granted respect or "legitimacy" from the collaborative partners (Mattiessich & Monsey, 1992).
Summary of the Mattiessich and Monsey Literature Review A comprehensive review of 12 studies on partnership success factors by Mattiessich and Monsey (1992) concludes that researchers have found a consistent pattern of practical factors that influence successful partnerships--mutual respect, understanding and trust, representation of an appropriate cross-section of members addressing a community issue, open and frequent communications, sufficient funds, and a skilled convener. Eight Recommendations for Successful Health-Care Alliances Mays et al. (1998) summarized the successful strategies for development and management of health-care alliances they discovered in studying 60 local communities in the U.S. Observations were drawn from a nonrandom, nationally selected group of 60 local communities and from detailed interviews with organizations operating in a subset of eight case-study communities. Local health department directors were used as the key informants about community health alliances occurring within their jurisdiction. A structured telephone survey was used to collect information about the 60 health alliances. In-person, semistructured interviews were conducted with the administrators of hospitals, managed care plans, and local health departments operating within eight case-study communities. Mays et al. (1998) offered these eight recommendations on developing and
53 managing alliances based on their interviews with key informants: 1. Identify a boundary spanner. 2. Secure buy-in from key stakeholders and opinion leaders. 3. Recognize and respond to participation constraints. 4. Keep the alliance structure simple, preferably based on informal agreements and simple contractual agreements. 5. Ensure incentive compatibility among participants. 6. Ensure effective communication and information flows among participants. 7. Develop an explicit evaluation strategy. 8. Maintain momentum through staged successes. Health-care alliances are influenced by similar success factors as found by Mattessich and Monsey (1992). As well-known health-care administration experts, Mays et al. (1998) summarized the current thinking of health-care administrators on practical strategies in developing health-care partnerships and alliances.
Obstacles to Successful Collaboration Gray (1989) identified a number of obstacles to collaboration, which include institutional disincentives, historical and ideological barriers, power disparities, cultural norms rooted in individualism and competition, differing perceptions of risk, technical complexity, and political and institutional cultures. Kappeli (1995) discussed the difficulties inherent in interprofessional cooperation in health care and stressed the need for flattened hierarchies and a strong commitment to the value of cooperation if collaboration is to be effective. Other barriers to collaboration among professionals mentioned by Kerka (1997) include negative past experiences with the collaborative process; difficult past/present relationships among agencies; competition
54 and turf issues; personality conflicts; differing organizational norms, values, and ideologies; and fear of risk. In their survey research on the Smoke Free Class of 2000 program coalitions, Gottlieb, Brink, and Gingiss (1993) found that respondents did report some common problems in coalition functioning due to perceived organizational and personnel barriers. The most commonly reported problems in coalition functioning related to availability of funds, competing priorities among organizations, coordination of activities among agencies, and differences in agency service areas. Each of these organizational barriers was reported as either a major or minor problem by at least 49.0% of the coalitions. Key areas of concern related to staff and volunteer functioning as reported by at least half of the respondents were (a) the availability of staff and volunteers for the project and (b) staff priorities. Conflicting staff priorities was reported as a major problem by 25.0% of the coalitions, as were staff availability (22.4%) and staff turnover (22.4%). Among the SFC-2000 coalitions, the researchers found that perceived effectiveness and perceived activity were both related to organizational barriers, personnel barriers, and formality of structure and were significantly correlated with each other (Gottlieb et al., 1993). Conducting a multiple regression analysis, the researchers found that personnel barriers and formality of the coalition structure was positively related to perceived effectiveness of the coalition. In other words, "independent of the organizational and personnel barriers experienced, the more structured the coalition, the more effective the respondents perceived the coalition to be" (p. 382). Based on their findings, the researchers recommended that coalitions move to formalize interagency agreements, mission statements, and goals and objectives. The researchers also noted the potential for conflict between agency and
55 coalition activities in situations of high turnover among the coalition representatives and the need for training of "boundary spanners" to resolve role conflicts. The literature reveals a number of obstacles and barriers to partnerships that must be recognized and addressed by a partnership's leadership to ensure effectiveness. Gottlieb et al. (1993) believed that four types of barriers must be addressed by every coalition: barriers of organization, of attitude, of vision, and of ignorance. Specific barriers are tied to differences in professional culture and training, competition, fear of risk-taking, adequacy of funding, formalization of communication and policies, perceived equity and fairness of resource distributions to partners, and individual agency "turf issues."
Research on Partnerships as IORs There are three significant bodies of literature from which research findings on partnerships have been drawn to support this AR project--human services, health care, and education/libraries. Much of the relevant research conducted to date has been qualitative and exploratory in nature. National Survey of Public-Private Health-Care Partnerships Bazzoli et al. (1997) conducted important survey research on public-private health-care partnerships in an attempt "to identify the range of collaborative activities in which these broad-based partnerships are engaged and to assess the factors that may affect the types and extent of their collaboration" (p. 534). These researchers gathered data from 243 partnerships that applied, in the spring of 1995, to the Community Care Network (CCN) demonstration program, which was designed by the American Hospital Association; the Hospital Research and Educational Trust; the Catholic
56 Health Association; and VHA, Inc. Funding for the demonstration program was provided by the W. K. Kellogg Foundation and the Duke Endowment. Surveys were returned from 172 of the 243 applicants (70.8% return rate). The 243 CCN applicant partnerships each had an average of 10 partnering organizations, representing a wide spectrum of private and public institutions including private health providers, public health departments, human service agencies, local government, educational institutions, health plans, and managed care organizations. As described by Bazzoli et al. (1997), the CCN partnership vision seeks to advance four principal goals: "(1) a focus on the health status of communities, (2) a seamless continuum of care, (3) management within fixed resources, and (4) community accountability" (p. 535). Given these broad-based partnership objectives of the CCN program, the authors believed a unique opportunity existed for understanding the kinds of collaborative actions and strategies that are being implemented in the health and human services arena by studying the CNN applicants. Focusing on the neglected area of partnership action rather than partnership formation, Bazzoli et al. (1997) concentrated on three main research questions: 1. What are the principal dimensions of collaborative activity in which these publicprivate partnerships engage? 2. How active are the partnerships in these different dimensions? 3. What factors about the partnership and its environment affect collaborative activity? (p. 535) In their national research on community health partnerships, Bazzoli et al. (1997) found that health education was a service offered collaboratively by 72.0% of the CCN applicants, followed by child immunization (62.0%), prenatal care for the uninsured (52.0%) and injury prevention (52.0%). Bazzoli et al. (1997) also reported that collaborative action appears to be common in over two thirds of the partnerships
57 in these activities--convening meetings of staff members involved in service provision, conducting meetings of providers and community organizations, and reviewing existing health data. In addition, future plans were commonly reported, including studies to evaluate cultural and financial barriers. After performing a factor analysis to identify patterns of collaboration among the public-private partnerships applying to the CCN program, seven dimensions of collaborative activity arose: (1) preventive health and educational services; (2) traditional acute and chronic care services; (3) behavioral health services; (4) community reporting; (5) cost-effectiveness and expenditure control; (6) community studies of health needs; and (7) coordination of services. On average, Bazzoli et al. (1997) found the partnerships implemented 4.88 different collaborative actions within the category of preventive health and education services. Bazzoli et al. (1997) concluded that their findings were consistent with expectations drawn from theories of resource dependence, IORs, political science and public finance economics. Organizations are willing to work together on activities that do not disrupt existing power and control. Also, organizational collaboration is common when individual organizations stand to benefit in terms of added prestige and visibility (through association with community health initiatives or community reporting, for example) and potential increases in client volume and referrals (through efforts to improve service coordination). (p. 554) An important implication of these research findings from Bazzoli et al. is that incentives can be developed to motivate collaborative action among organizations that might otherwise participate in a partnership only for symbolic reasons. Bazzoli et al. (1997) noted that several crucial concepts were not able to be operationalized in their survey research. First, organizational willingness and the ability to collaborate as defined by Alter and Hage (1993) were not included in the survey questions. Second, the researchers did not gather information on the leadership
58 structure, vision, and values of the individual organizations involved in the CCN partnerships. Information about the organizational cultures, capabilities, or financial and human resources are important factors "affecting the underlying objectives of organizations and thus their desire and ability to share power and control through collaborative action" (Bazzoli et al., 1997, p. 556). Bazzoli et al. (1997) also noted there is a need for longitudinal research to improve understanding of collaborative action and what motivates collaborative action among public-private partnerships. There is also a pressing need to better understand (a) how these collaborative networks operate and sustain themselves; (b) the processes and mechanisms partnerships establish to plan, implement, and monitor collaborative action; (c) approaches used by partnerships to engage the community and give it a voice; and (d) efforts by the partnership to sustain itself and its collaborative initiatives. Bazzoli et al. (1997) pointed to the importance of trust among partners in accepting partnership actions and the use of recognition as a reward for organizational participation. Bazzoli et al. suggested that other research questions of future importance include (a) how partnerships balance the needs for both organizational and partnership recognition, (b) how partnerships balance attending to maintenance with carrying out initiatives, (c) how supporting information systems to assess and monitor partnership progress and impact are developed and maintained, and (d) how partnerships build capacity and capabilities to maintain their efforts into the future. To summarize, the Bazzoli et al. (1997) survey is the first major research study of the dynamics and operations of U.S. public-private health-care partnerships. Their survey provides a basis for comparison and benchmarking for other operating healthcare partnerships such as the TCN. The Bazzoli et al. conclusions illustrate the
59 importance of resource distribution as an incentive for the initial participation and sustaining involvement of community agencies in partnership activities. Health-Care Research on Partnerships and Effectiveness Provan and Brinton (1995) studied four community mental health systems in four U.S. cities to test their theory of network effectiveness. These authors argued that much previous research was simply an extension of the outcomes of individual organizations and ignored the nonstructural outcomes of network performance as a whole. Particularly in the area of community-based health care and social services for such groups as the homeless, people with severe mental illness, drug and alcohol abusers, and the elderly, a focus on organizational outcomes is insufficient because such outcomes reflect only how well individual providers are performing their particular component of the many services offered by their clients. (p. 2) Provan and Brinton (1995) organized their study around a single fundamental research question concerning network effectiveness: "What, if any, is the relationship between the structure and context of mental health networks and their effectiveness?" (p. 3). The study used a multitrait, multiperspective comparative case research methodology designed to assess the overall well-being of severely mentally ill clients collectively served by the health and human service delivery networks in four midsized cities in the U.S.--Albuquerque, New Mexico; Providence, Rhode Island; Tucson, Arizona; and Akron, Ohio. The authors collected qualitative and questionnaire data from hundreds of individuals and organizations, which they aggregated by system and then compared across the four systems for network performance. The authors found that a single measure of network effectiveness--combining the perspectives of key constituent groups: clients, families, and case managers--was
60 not feasible due to variations they found between the professional case manager group and client-family groups. Instead, they reported on the client and family views, which demonstrated convergent validity for the measures they employed. Provan and Brinton (1995, p. 7) noted that it is the "experiences of families and particularly the clients themselves that ultimately matter the most, since they are the ones who actually receive the system's services, are most knowledgeable about the client's overall wellbeing, and must live with the results" (p. 7). Provan and Brinton (1995) also discovered that network integration--the interconnectedness between provider agencies and the extent to which provider agencies are integrated and coordinated through a central authority--was positively related to network performance. Monitoring and control over activities and outcomes by core agencies was made possible when a network became centralized, as discovered by Provan and Brinton in their comparative case study research. Provan and Brinton (1995) believed that such centralized control is critical for encouraging otherwise autonomous agencies to act in ways that lead to system-level, as opposed to agency, goals. Network effectiveness was found to be highest when mechanisms of external control were direct and not fragmented. Provan and Brinton also found that network effectiveness was enhanced under conditions of general system stability. Finally, funding level of the network (i.e., resource munificience) was found to be critical to enhancing the number and quality of services provided to clients. However, the authors found in their research that the funding level was not as critical to effectiveness as network/system-level factors for either overcoming problems of resource inadequacies or taking advantage of resource munificence. Provan and Brinton (1995) concluded that the following explanatory factors need to be explored in future studies that examine network effectiveness: historical
61 patterns of funding, system evolution, patterns of treatment, mix and distribution of services among providers, levels of involvement by staff members at certain key agencies, and levels of commitment by individual members of key agencies. Their study shows that, consistent with multiple-constituency approaches in measuring and conceptualizing organizational effectiveness, the factors that best explain network outcomes appear to depend on whose effectiveness perspective is considered. An important policy implication of the Provan and Brinton (1995) research study is tied to network integration and coordination. By creating incentive structures and monitoring mechanisms so that services are provided through a system that is centrally integrated and coordinated through a single, powerful core agency, system effectiveness for clients can be increased by state funding agencies. In an era of scarce funding, networks and strategic alliances can increase administrative efficiencies and enhance the level of services for clients by working with agencies such as the Illinois State Library. In 1990, Gottlieb et al. (1993) conducted survey research on 50 state and local coalitions that carried out the Smoke Free Class of 2000 program of the American Cancer Society, American Heart Association, and American Lung Association. The researchers distributed a predominately closed-item survey to obtain descriptive information regarding (a) the level and type of coalition activities over the previous year (including fund-raising, extent of media coverage, number of purchases and requests for materials, the distribution network in the state, use of volunteers, and innovative methods of disseminating materials) and (b) the outcomes of this process (number of curriculum kits distributed, number of clients reached, and use of other related tobacco prevention materials). Organizational barriers, personnel barriers, and formality of coalition structure
62 were independent variables constructed in the regression analysis of the survey data compiled. Perceived effectiveness, perceived activity, and mean number of curriculum kits sent per elementary school were the dependent variables. The researchers noted that a limitation of their study was the "lack of behavioral measures of coalition effectiveness" (Gottlieb et al., 1993, p. 378). Because the researchers relied on self-reports from contact persons at each coalition, there was bias due to response sets. The SFC-2000 state coalitions averaged five member organizations and were highly centralized, with over 70.0% of the coalitions reporting that decisions on products, evaluation, and goal-setting were state-level functions. For the measure of perceived effectiveness, the respondents reported the coalitions to be most effective in product purchase and program focus, public relations, and communications, with over 75.0% of the coalitions having performance ratings of effective or very effective. Among coalitions that reported these activities, over half indicated that the functions of fundraising (60.5%), training teachers (58.0%) and volunteer coordination (51.0%) were ineffective or extremely ineffective. Over a third (36.2%) noted problems in effectively evaluating the programs. Alter and Hage (1993) argued that collaborative action depends on the perceived need for collaboration and the organizations' willingness to collaborate. These concepts constitute central themes in resource dependence and interorganizational relations theories. These theories focus on dependencies among organizations and on their environments as they seek to achieve their own objectives. The potential dependencies include such factors as the need for human or financial resources by a partner organization, the need for working capital, the need to manage business risks, the desire to expand human and technological expertise, and the importance of
63 maintaining flexibility to allow adaptation in a rapidly changing market. From this review of the research conducted on health-care coalitions, it is apparent that coordination is an important factor in network performance. Coordination involves the monitoring and control over activities and outcomes by the core agencies involved in a partnership. The program focus, communication, public relations, fundraising, training, and product purchase are all aspects of partnership coordination. The assessment of the TCN's IOC activities is presented in Chapter 5, using the Alter and Hage (1993) and Mattessich and Monsey (1992) models. Research on the Elements of Successful Library Partnerships Millard (1999) compared perceptions of Delaware education and policy leaders with the literature on partnerships to determine the successful elements of university library-school partnerships. The elements that Millard (1999) identified in her literature review and research included (a) commitment from top leaders; (b) mutual interest and needs; (c) clear focus, goals, and planning; (d) dynamic nature/energy/action orientation; (e) effective communication; (f) adequate resources and fiscal support; (g) leadership; (h) sufficient time; (i) understanding the culture of partnerships; and (j) evaluation. Millard (1999) conducted 13 interviews with Delaware university leaders, state of Delaware government officials, and local school-district leaders who were involved in implementation of a statewide Internet network between the University of Delaware Library and local school districts. The state picked up costs of the $30-million project over a three-year period, and the project was completed in 1999. Millard (1999) found a number of common themes expressed by the leaders she interviewed. The first theme was the importance of communication in gaining the
64 legislative approval for the Internet project budget. Millard noted that the policy leaders reported that "communication was the most important element of successful partnerships--communication among partners and about the partnership to stakeholders" (p. 63). Another recurring theme Millard (1999) found in her interviews was that partnerships are personal in nature and are based on what the individual representatives agree are important, whether it be an end product to be designed or a service to be provided. A third theme revealed during the interviews was the concern that the partnership activities actually benefited the target audience. For example, was there a high volume of use by targeted end-users? A final theme identified by Millard in the Delaware policy-leader interviews was that the small size of the state allowed for immediacy of informal communication so that the Internet linkage and training project proceeded rapidly and effectively. This case study conducted by Millard (1999) was the first major research study in the library and information science field that examined the factors that contribute to partnership effectiveness and perceptions of success. Millard's research highlights the importance of communication, personal fulfillment, perceived benefits to the agencies involved, the role of key decision makers within the university, local schools and state government, and the actual use of partnership products and services by the project target audience--students and teachers.
Evaluating the Outcomes of Partnerships Gray (1989) identified a number of objective and subjective factors for judging the success of partnerships based on the findings of earlier case-study research she reviewed. According to Gray, two clear objective criteria of success are whether or
65 not an agreement was reached and whether the agreement was implemented. Subjective success criteria reflect the participating stakeholders' assessments of the outcomes. The importance of succeeding with respect to these subjective standards is often just as critical as achieving objective success because if the parties are unhappy with the process of collaborating, they are unlikely to accept the outcome. (Gray, 1989, p. 256) The parties must believe the real issues were addressed and their own interests satisfied for the collaboration to be considered successful. A list of the subjective and objective criteria of importance for judging the success of interorganizational collaboration is found in Gray (1989, pp. 256-257) and summarizes the key points to consider when evaluating partnership activities: • Does the outcome satisfy the real issues in dispute? • Do the parties feel they affected the decision? • Are the stakeholders willing and able to implement the decision? • Does the agreement produce joint gains for the parties? • Did communication between the parties increase and did the working relationships improve? • Has the agreement held up over time? • Was the process efficient in terms of time and resources? • Does the solution conform to available objective standards? • Do the parties perceive the procedures were fair? • Did the procedures conform to accepted standards of procedural fairness? (p. 256257) Hall (1999) noted that an important partnership research result is the "consistent research finding . . . that integrated IORs or partnerships contribute to improved health and social care at the community level" (p. 221). The outcomes of partnership activities are more effectively evaluated when a combination of objective and subjective data is made available to the involved
66 partners and to outside agencies. Both Gray (1989) and Hall (1999) pointed to the importance of partnerships in having a measurable impact on the local community's overall health and wellness. Youth Risk Behaviors, Youth Development, and Protective Factors Resnick et al. (1997) reported on the health status of youth in the U.S. According to these researchers with the Adolescent Health Program at the University of Minnesota, the main threats to adolescents' health are predominantly the health-risk behaviors and the choices teens make. "Data indicate that more than three of every four deaths in the second decade of life are caused by social morbidities: unintentional injuries, homicides, and suicides" (p. 823). Resnick et al. sought to identify protective factors in the lives of young people--factors that, if present, diminish the likelihood of negative health and social outcomes. The authors found consistent evidence, based on data from the Add Health sample of 80 high schools and 90,000 adolescents, that perceived caring and connectedness to others is important in understanding the health of young people today. Blum and Rinehart (1997), also utilizing the National Longitudinal Study of Adolescent Health (Add Health) data, reported that adolescent health is influenced by teens' social settings--family, school, neighborhood, and friends. "What emerges most consistently as protective is the teenager's feeling of connectedness with parents and family. Feeling loved and cared for by parents matters in a big way" (p. 31). The school environment also makes a difference in the lives of youth, and what matters is the students' sense of connection to the school they attend: "If students feel they are a part of the school, are treated fairly by teachers, and feel close to people at school, they have better emotional health and lower levels of involvement in risky behavior"
67 (p. 32). Results of the 1997 national school-based survey were recently released by the CDC (Kann et al., 1998). The YRBS national survey employed a three-stage cluster sample to produce a nationally representative sample of students in grades 9-12 in private and public schools in the 50 states and the District of Columbia. For the 1997 national survey, 16,262 questionnaires were completed in 151 schools. The school response rate was 79.0%, and the student response rate was 87.0%. As defined in the YRBS project, "priority health-risk behaviors" are those behaviors that contribute to the leading causes of mortality and morbidity among youth and adults and often are established during youth, extend into adulthood, and are interrelated (Kann et al., 1998). The behaviors that contribute to intentional injuries in youth are important in recognizing the extent of violence in the lives of adolescents in the U.S. School-related violence is tied to the following risky behaviors as reported in the 1997 YRBS results: Carrying a weapon: Almost one fifth (18.3%) of students nationwide carried a weapon (e.g., a gun, knife, or club) on one or more of the 30 days preceding the survey. Overall, male students (27.7%) were significantly more likely than female students (7.0%) to have carried a weapon (Kann et al., 1998). Physical fighting: Among students nationwide, 36.6% had been in a physical fight one or more times during the 12 months preceding the survey. Overall, male students (45.5%) were significantly more likely than female students (26.0%) to have been in a physical fight (Kann et al., 1998). School-related violence: Nationwide, 4.0% of students had missed one or more days of school during the 30 days preceding the survey because they had felt unsafe at
68 school or when traveling to or from school. Overall, Hispanic and Black students (7.2% and 6.8%, respectively) were significantly more likely than White students (2.4%) to have felt unsafe. In Chicago, 13.9% of the students reported they had missed one or more days of school during the 30 days preceding the survey because they had felt unsafe (Kann et al., 1998). Suicide ideation and attempts: Nationwide, 20.5% of students had seriously considered attempting suicide during the 12 months preceding the survey. Overall, female students (27.1%) were significantly more likely than male students (15.1%) to have considered attempting suicide. Overall, Hispanic students (23.1%) were significantly more likely than Black students (16.4%) to have considered suicide. Serious suicide plans were reported by 15.7% of students nationwide. Overall, females students (20.0%) were signficantly more likely than male students (12.2%) to have made a suicide plan during the 12 months preceding the survey. A total of 7.7% of students in the survey had attempted suicide one or more times during the 12 months preceding the survey. Nationwide, 2.6% of the students reported having made a suicide attempt during the 12 months preceding the survey that resulted in an injury, poisoning, or overdose that had to be treated by a doctor or nurse (Kann et al., 1998). In reviewing comprehensive community initiatives for youth, Barton et al. (1997) reported that approximately 50 comprehensive local initiatives have been established through funding from foundations and partnerships with local or state governments. Such initiatives are based on a holistic, broad understanding of community infrastructures and their subsequent influence on the needs of children and families. The "state of the art" from these initiatives includes the following: • There must be a unifying vision or perspective about youth development, the inseparability of the many problems of adolescents, and the inadequacy of focusing on problems to the exclusion of healthy outcomes. • There must be a framework for developing a comprehensive community approach to
69 promote healthy youth development. • There are guidelines for the planning process and examples of promising programs from other communities that address risks and protective factors at various levels. (p. 491) Barton et al. (1997) argued that communities seeking to adopt a comprehensive approach to youth development must promote that unifying vision through education of key community leaders. Then they need to conduct baseline assessments of current risks and resources; develop priorities for appropriate support, prevention, and intervention programs; select and implement those programs; and monitor their effectiveness against the baseline assessments. (p. 491) Dryfoos (1998) believed that "full-service community schools" can integrate quality education delivery with whatever health and social services are required in a community. These innovative programs, located in such states as Florida, Iowa, California, New York, and Missouri, draw resources from the school and from outside community agencies that come into the schools. The school and outside agencies join forces to provide seamless delivery programs. Dryfoos reported that successful fullservice community schools have the school principal actively involved as well as a full-time coordinator or program director to ensure that personnel carry out their assigned roles and responsibilities in educational, health, and social service program delivery. Key elements that are present in all these programs include (a) plenty of individual attention is provided to students; (b) there is a heavy emphasis on parental involvement and services for parents; (c) health centers and family resource rooms are made available; (d) after-school activities are offered; (e) there are many cultural and community activities offered; (f) extended hours of operation exist on evenings, weekends, and summers; and (g) respect and high expectations for students is evident. The concept of "full-service schools" is beginning to take hold with the medical community. Physicians Stiffman, Earls, Dore, Cunningham, and Farber
70 (1996) noted that violence has only recently been conceptualized as a province of health-care services. According to Stiffman et al. (1996), mounting preventive interventions in the health sector require that violent youths are identified. Stiffman et al. (1996) perceived the need for medical personnel to become directly involved in programming and advocacy for increased funding for violence-focused health care. More importantly, the health-services sector is mandated to network with both the criminal justice and educational arenas for effective violence prevention programs. Prevention-oriented health services networks need to involve health personnel in the development of employment programs for high-risk adolescents; in the implementation of alcohol and drug abuse prevention programs; in the teaching of conflict resolution skills, family life, and child-rearing education; and in supporting families within the community (Stiffman et al., 1996). School reform objectives, as reflected in the National Education Goals Panel (1995) document, Building a Nation of Learners, illustrate the growing recognition of student health and safety needs within the school setting. The optimistic outlook for student health and safety is reflected in Goal 7: Safe Schools: "By the year 2000, every school in the United States will be free of drugs, violence, and the unauthorized use of firearms and alcohol and will offer a disciplined environment conducive to learning" (p. 1). The health-care community and educational community working in partnership can ensure that our schools are "safe havens" for learning. Trends in CHI, Self-Help, Health Promotion, and Patient Education Public health coalitions are currently active in the U.S. through the Coalition for Healthier Cities and Communities (www.healthycommunities.org) and the Healthy People Consortium. Health promotion programs offered by hospitals in shopping
71 malls and schools are indicative of the trend toward community outreach reported by McCain and Stratton (1994) and Newbold (1998). Managed care is the driving force behind the expanded interest in wellness and prevention due to reduced health-care costs (Collins & Sasser, 1997; Humphries & Kochi, 1994). In short, wellness has become "trendy" and a significant social movement in the U.S. Deeper understanding of human potential and a growing perception that the old order has failed are leading more people to question top-down, expert-driven solutions to health-care problems. Two core themes are emerging: (1) an appreciation of the power that clients and patients have to become problem-solvers themselves, and (2) an awareness of the creative power of collaborative human relationships. "Viewing selfhelp as a microcosm of public problem solving, . . . many communities are healing themselves" (Appleby, 1995, p. 43). The power of self-help is that it turns problems into solutions. For millions of people reaching out both for help and to help, this movement reweaves our social fabric, establishing connectedness based on mutual responsibility and respect. Healthy communities depend on this connectedness. (p. 44) The increased importance of health information for decision making and empowered health consumers is reflected in both the public health arena and in healthcare accreditation standards. The U.S. Public Health Service (PHS) (1995) has been working with state public health departments and local communities to meet the 22 priority areas for health established in Healthy People 2000. Public review of the new Healthy People 2010 prevention agenda is underway on the PHS web site at http://web.health.gov/healthypeople/ and through a series of five regional meetings. The Joint Commission for the Accreditation of Health Care Organizations (JCAHO) (1998) revised its hospital standards manual several years ago to reflect the increasing importance of patient education. JCAHO stated that the goal of patient and family education is
72 to improve patient health outcomes by promoting healthy behavior and involving the patient in care and care decisions. Education promotes healthy behaviors, supports recovery and a speedy return to function, and enables patients to be involved in decisions about their own care. (p. 105) To meet patient education standards, hospitals are required to demonstrate evidence of the following activities: • Assessing organization-wide patient education programs and activities; • Formulating patient education program goals; • Allocating resources for patient education; • Determining and prioritizing specific patient education needs; and • Providing education to meet identified patient psychosocial, spiritual, and cultural needs. JCAHO (1998) supported the need for developing collections of educational resources to support patient education objectives as defined by the hospital: "The hospital identifies and provides the educational resources required to achieve its educational objectives" (p. 111). Educational resources for patient education include the following: "educational materials such as pamphlets and videotapes, materials and resources that accommodate persons with disabilities, community resources for education, and referrals to programs that can meet special needs" (p. 111). Hospital libraries are being called upon to provide knowledge-based services and consultation to patients, nursing staff, physicians, and the community-at-large on appropriate consumer health resources. Collaboration is seen by many health-sciences librarians as broadening resources within the hospital setting and in the local community for patient education (Collins & Sasser, 1997; Gall & Miller, 1997; Humphries & Kochi, 1994). JCAHO requirements for knowledge-based information also incorporate an expanded role for hospital libraries in providing CHI: The hospital provides systems, resources, and services to meet its need for knowledgebased information in patient care, education, research, and management.
73 Knowledge-based information is authoritative and up to date. It supports clinical and management decision making, performance-improvement activities, patient and family education, continuing education of staff, and research. (JCAHO, 1998, p. 207) In understanding current trends in health care, empowered health-care consumers and accrediting agencies are the driving forces behind improvements in the delivery of health information. The scope of CHI needs makes libraries of all types key players in improving access to health information for their patrons who are adopting a proactive self-help role. Building Consumer Health-Information Networks and the "Utopian Health-Information Network" The federal government has played a major role in the expansion of CHI and in the building of the national infrastructure to support Internet access to free health and medical information through grant funding of innovative programs. Dahlen (1993) stated that the PHS is a major producer and distributor of information supportive of healthy lifestyles. But the role of libraries in the dissemination and delivery of CHI to the public is an area not clearly defined. Thus, an opportunity exists, with the increased access to health-information resources on the Internet, for librarians in developing the "Utopian Health Information Network," as highlighted by Dahlen in her report on the status of health-information delivery in the U.S. Librarians working in all types of libraries can assist their patrons with locating appropriate health information and work cooperatively with health-care professionals, social service providers, and schools to realize the dream of the "Utopian Health-Information Network" to support healthy lifestyles. The Department of Health and Human Services (DHHS) was cited in Putting the Information Infrastructure to Work: Health Care and the National Information
74 Infrastructure (1994) in which it was stated that its long-term goal is for "universal access" to health information at the "point of need." The National Library of Medicine added a Medline Consumer Health-Information Service in 1998. In 1997, Healthfinder, an Internet gateway, was launched by the DHHS. The Healthfinder website provides access to more than 10,000 general consumer health websites and thousands of sites on specific diseases and conditions. These major Internet-based information networks make the "Utopian Health-Information Network" a valuable component of library information service programs. The explosion of the Internet and CHI resources available via the Web makes the "Utopian Health-Information Network" discussed in the early 1990s a reality in 2000. Expectations for just-in-time delivery of health information at the "point of need" is revolutionizing health care and medical library reference services.
Growing Demand for CHI and Support National polls continue to indicate a strong interest in health information and health among the general public. Deering and Harris (1996), for example, cited a number of surveys of families and individual consumers that estimated the value of and interest in CHI based on actual consumption patterns. In one 1995 study, Deering and Harris (1996) reported that researchers asked a group of 1,005 adults if anyone in their households had had a health problem within the past 12 months. Overall, 35.0% of consumers in this survey indicated someone in their household as having had a physical or mental health problem, and 85.0% of these same consumers attempted to obtain information about the problem. The Reference Point Foundation survey found no variations of this pattern across gender, race, or disability status (Deering & Harris, 1996).
75 Recently, a Harris Poll from August 5, 1999, that estimated Web use found that 70 million Americans went online between June 1998 and June 1999 looking for health information. This same Harris Poll indicated that the number of Internet health users increased 45.0% over the last year to reach 24.8 million U.S. adults as of July 1999 ("Intel, Health Care Leaders," 1999, p. 1). A second recent report by Deloitte and Touche-VHA, Inc. found that 17.5 million adults are using the Internet to search for health information ("Consumers Go Online," 1999). The Deloitte and Touche-VHA, Inc. report also found that people turn to the Internet for health information in part because of a lack of information available from traditional sources. The report found more than two thirds of patients in the U.S. do not receive information (i.e., printed literature) about their condition or their child's condition while at the doctor's office and only one third receive information about their medications. In September 1999, drkoop.com, a site developed by the former U.S. surgeon general and a leading proponent of empowered health consumers, was among the top 50 websites, with 5,539,000 unique users, according to PC Data Online ("Top 50 Web Sites," 1999). National surveys of consumer demand for health information in libraries also reflect a high demand by library patrons. "Studies estimate that as many as 10.0% of all reference questions--or as many as one million each week--are health-related" (Deering, 1996, p. 206). Public librarians report that health issues are among the top three to five concerns for their patrons. Deering and Harris (1996, p. 211) stated that "health information is the single largest subject for popular and professional consumption" (p. 211). Deering and Harris also reported that they identified more than 40,000 producers, publishers, and providers of health information in their research conducted.
76 The supply of medical information is staggering. More than 1,400 healthrelated books are published annually. There are over 150 popular, health-related magazines and newsletters available for consumers. Rees (1998) indicated that "network nightly news devotes as much as 20.0% of its total coverage to health-related matters" (p. ix). Currently, Internet health-information websites such as Onhealth.com and CBS.Healthwatch.com are advertising in prime-time television slots and radio to increase awareness and use by consumers. Providers of health information include physicians, hospitals, libraries, voluntary health agencies and associations, clearinghouses, information and referral services, mass media, federal programs, and employers. With this multiplicity of providers and the "glut" of health information of unknown quality, consumers need guidance in the interpretation of the information obtained from these multiple and often contradictory sources. Often, these consumers require emotional support if faced by serious illness. There is a growing recognition among health professionals that healthy communities support and promote informed health consumers: The health of individuals is intertwined with the health of their communities. When individuals seek healthcare, they look for high-quality medical attention. But they also need clear information with realistic assessment, a connection with others who share their illness, knowledge of what they personally can do to aid recovery, and emotional support. (Appleby, 1995, p. 44) Partnerships between health-care providers and information professionals expand the capabilities of the health-information delivery network and produce satisfied, health-conscious consumers. Individual health-care providers and libraries are becoming more effective in addressing community needs for health information by creating partnerships and networks. Gaps in health-care information delivery are addressed effectively at the local level with the national infrastructure currently in
77 place. Dealing with the Complexities of Health Information "People have many problems with health information, including how to interpret conflicting or differing information, how to judge reliability, and how to decide what to do when given many choices" (Deering & Harris, 1996, p. 213). Deering and Harris believed these problems reinforce the need for librarians to serve as intermediaries and assist consumers with interpretation of the information obtained. Librarians are in a strategic position to serve as intermediaries and mentors in helping parents and youth to navigate the health-information network and to simplify information retrieved for health-care decision making. The Potential of Electronic Sources of Health Information for Consumers and Providers "Networked health information can result in response to demand and fulfillment that is more timely and more complete than that of any other media" (Deering & Harris, 1996, p. 214). Just-in-time delivery is possible with networked health-information sources, although inequities in delivery and access need to be addressed if there is a sole reliance on networked information. The just-in-time delivery features of the Internet make it particularly useful for students. Deering and Harris anticipated that "younger people . . . seem more likely to use new sources for information, such as the Internet and other computer technology" (p. 209). The Internet provides access to health information for personal health questions and school homework assignments. Deye, Kahn, Jimison, Renner, Wenner, and Gabello (1997) recommended a number of quality sites in patient education for
78 inexperienced users of the Internet in locating CHI. To meet the demand for and improve delivery of CHI, two consistent patterns are evident that have implications for librarians. First, people with specific information needs use multiple sources of health information. This suggests that hospitals should link with other institutions or services that can fill the roles of information provider or navigator for their patients. Second, the supply of health information is overwhelming. Potentially lifeand cost-saving information cannot be effectively accessed without better organizational and navigational tools. "In both respects, medical and public libraries can be useful partners. They provide information management, inquiry assistance, knowledge of information resources, and an established delivery channel that could be effectively harnessed to serve the nation's health-information needs" (Deering & Harris, 1996, p. 215). Libraries provide convenient community sites and experience with online searching. They are a "vital component of a health-information infrastructure" (Deering & Harris, 1996, p. 215). As such, libraries and librarians serve a key function in the provision of health information based on their convenient locations; ease of access to clients; and expert knowledge of available health-information sources, training, and online search techniques. Libraries as Partners in Collaboration and Cooperation Collaboration is presented in the library literature as increasing the number of library/information services available, improving the accessibility of services, and enhancing the desirability of services to clients. Ultimately, collaboration makes information service delivery seamless.
79 "Any time there is a shared user community, partnerships can be instrumental in determining the quality of service provided to users. Some of the best partnerships are set up by local, informal cooperative arrangements rather than by formal, bureaucratic networking" (Allen, 1992, p. 6). "The first step in developing useful partnerships is to admit that libraries share many goals and objectives with a variety of community agencies. Competition can then give way to cooperation, and new and innovative ways of meeting users' needs can follow. (Allen, 1992, p. 7). Collaborative partnerships represent an intense relationship centered on mutual goals. Wisdom is constructed within the social reality of the partnership as well as within the wider social context in which the partnership exists (Saltiel, 1998). Common values make partnerships effective: The first is that a partnership always involves two or more people or groups who are working together toward a common goal. The second is that partners bring different contributions to the partnership. The library may bring its collection of materials and its experienced staff. A service agency may bring its in-depth knowledge about people with specific problems or concerns. (Allen, 1992, p. 8) Collaboration, in contrast to cooperation, makes use of each partner's unique talents and produces outcomes that could not have been done at all or done as well alone. In addition to goals, a common mission, and shared expertise, successful partnerships exhibit important attitudes among the partners. Mutual respect, trust, and ownership over the direction of the enterprise are key aspects of successful partnerships. "By forming alliances and establishing collaborative relationships with other agencies and organizations, libraries can ensure the centrality of their own role in their communities. This centrality can, in turn, have an impact on the availability of resources for libraries" (Allen, 1992, p. 10). Allen believed that partnerships build
80 caring human relationships that contribute to the survival of libraries into the future: "Confrontation is replaced by humility, and new relationships are forged with our partners and library patrons. This is one road to survival for libraries in the 1990s" (p. 10). Collaborative library/community agency partnerships are characterized by synergy. A synergistic relationship "empowers the partners . . . to achieve more than they set out to do as individuals. The partners fuel one another, creating an energized dynamic, electric in its feel" (Saltiel, 1998, p. 8). As seen in the earlier literature reviewed, library-community agency partners are equals who select one another with the expectation that they will learn from one another, hold a deep commitment to one another, and believe in the success of the endeavor. A recent example of cooperative programs between public libraries and healthcare providers in Illinois is the Babies First program, an adaptation of the Decatur, Illinois, Baby TALK program in Centralia, Illinois (Gross, 1998; Handy, 1992). Centralia Public Library coordinates the program, which presents a Babies First child development calendar, picture board books, and newsletters to mothers and fathers enrolled in prenatal classes at St. Mary's Hospital and to mothers enrolled in the local Women, Infants, and Children (WIC) program. Local service clubs and social service agencies donate monies to purchase the board books for parents. The local community college also provides funds for calendar publication, literacy materials, and mailing of newsletters (Handy, 1992). Ultimately, successful collaborations such as the TCN focus on process improvements that change service delivery systems. The essence of successful partnerships is found in the quality of personal and professional relationships among the people and agencies involved--the human connections (Kerka, 1997; Sgroi &
81 Saltiel, 1998). Library cooperation and collaboration has a long history in the state of Illinois. Resource-sharing programs and the development of a statewide computerized infrastructure extends back into the 1960s with the use of OCLC. A much-needed component to state-level efforts is collaboration at the local community level. Local efforts need to focus on health-information needs and the building of human connections to ensure future effective library services and information networks. The TCN project fulfills the statewide vision for cooperation and builds bridges at the local level among libraries, health-care providers, and youth service agencies. Librarian's Role in Providing CHI and Patient Education Rees (1991) and Longe and Thomas (1998) believed that medical consumerism is driven by the notion that more individual responsibility is desirable and necessary. The rising costs of health care and changes in the delivery of health care are leading employers, health-care providers, and managed-care organizations to promote health, to promote disease management strategies, and to supply individuals with the information needed to maintain healthy lifestyles. The provision of health information is consistent with the notion of library professionals as "empowering" clients, operating with an "ethic of care" and supporting knowledge of "care for self," as defined by Noddings (1984; 1992; 1996) and Maack (1997). The library response to the growing demand for CHI has evolved over the past 20 years. Traditionally, medical school and hospital libraries denied access to nonprofessional users. But the mid-1970s marked the beginning of a revolution in CHI services. Several pioneer medical librarians began providing organized healthinformation services to the general public in the communities their hospitals served.
82 Access to health information was fostered through a series of Library Services and Construction Act (LSCA) grants provided by state libraries in the late 1970s and early 1980s in California, Nebraska, Massachusetts, Ohio, Illinois, Connecticut, and Pennsylvania. These grants involved cooperative efforts between medical and public libraries with programming focused on collection development, training, reference services, community information and referral networks, and library networking (Rees, 1991). Recently, the MLA (1996b) issued a policy statement that identified six leadership roles for librarians in providing CHI and patient education. Collection management, knowledge and resource sharing, advocacy, access and dissemination of information, user education, and research are key functions of librarians in delivering CHI services. These recommended roles for librarians in CHI delivery do not include interpretation of information. There is a question about how to handle conflicting evidence found in the medical literature. Generally, it is recommended that patients have a dialogue with their physicians rather than solely rely on the advice of library professionals. Rees (1998) recommended that librarians provide assistance in locating information and in educating patrons in effective access methods but leave information processing and decision-making up to clients and their physicians. Rees (1991) and Longe and Thomas (1998) perceived the strengths of librarians to be their technical and interlibrary loan skills. The MLA (1996b) recommended that librarians assume a broad role and serve as leaders in the development, implementation, promotion, and evaluation of effective community-wide CHI services. This was the position adopted by the TCN partnership in Aurora, Illinois.
83 Summary of the Literature Review This review of the literature has highlighted basic concepts and related research on partnerships. Literature was scanned in the fields of health-care administration, management, anthropology/sociology, instructional technology, education, and library science to gain an understanding of (a) the nature of and rationale for library/community agency partnerships, (b) the concepts of "partnering behaviors" and IOR development, (c) the processes and structures that contribute to successful partnerships, (d) barriers to partnership development, (e) criteria for judging the outcomes of partnership activities, (f) the impact of protective factors on adolescent health and risk behaviors, and (g) the expanded role of librarians in providing CHI inside the library building and to the community via the Internet. The literature review reveals that resource dependency theory serves as an explanation for the creation of partnerships (Aldrich & Pfeffer, 1979). Resource dependency assumes that organizations are not able to generate sufficient resources required to maintain themselves and the need for additional resources leads organizations to enter into relationships with other organizations within their environment that can supply the needed resources and services. According to the resource dependency model, organizations are constructed or enacted systems that must satisfy the demands of members, owners, or constituents and are subject to evaluation. Administrators of organizations are faced with the task of ensuring a continuing supply of resources and performances and also working toward the satisfaction of powerful groups within their environment. The resource dependency model implies that both resource and information flows are exchanged between and among organizations that implement a partnership. Organizations are conceived as shaping their environments to fit their capabilities.
84 Therefore, a key consideration for the TCN, a library/community agency partnership, was the development of an Internet website for the exchange of strategic information about community health-information needs, the health and social services available to meet the needs of both teens and their parents, and new programs to increase access to health information. The TCN partnership undertook the development of an Internet website to provide a stable basis for information exchange among the partners and between the partnership and its target audience--teens and parents in the Aurora, Illinois, community. A listserv and e-mail delivery of information requests from Aurora teens and their parents became important features of the website as the project evolved over time. As this case-study narrative progresses and findings are subsequently reported, it will become clear to the reader that the knowledge management skills, networking skills, and ethical perspective of professional librarians involved in the TCN partnership contributed significantly to the local Aurora, Illinois, community development and youth development initiatives undertaken and continuing into the future. Establishing partnerships with health-care and social service providers, government agencies, schools, churches, businesses, libraries, and "librarian boundary-spanners" solved important community problems, built human connections, established support mechanisms within the partnership, and strategically created "seamless delivery systems" for improved access to health information in Aurora and neighboring communities. Librarians crossed organizational boundaries in an attempt to better coordinate resources, people, and services to assist their respective client groups (Sarason & Lorentz, 1998). The TCN grew over time, based on the belief that the empowerment of healthinformation consumers and an enhanced quality of life in one's local community are
85 the ultimate measures of an effective library/community agency partnership. It was a common set of values that drove the partnership in its first two years of operation.
CHAPTER 3 METHODOLOGY
This chapter covers the AR perspective adopted for the TCN partnership project, provides the rationale for the case study methodology employed, and identifies the data-collection methods and sources used to construct the case study. AR as a Qualitative Methodology in the TCN The TCN employed AR as a collaborative approach to investigation of community violence and its solutions. The AR methodology provided the partners with a means to take systematic action to resolve a specific problem--improving access to health information for Aurora teens and their parents on safety issues and violence prevention. The TCN steering committee was intimately involved in the (a) investigation of the problems and issues to be addressed, (b) formulation and sharing of their accounts of the problem and the partnership actions to take, and (c) planning of group solutions to deal with the problems at hand. Steering committee meetings were occasions for the sharing of research results and reactions to proposed plans for violence prevention programs and services. Elaborate statistical procedures and technical language were discarded in this research in favor of rich, qualitative data that was accessible both to laypersons and professional practitioners.
Overview and Assumptions AR is summarized in a recent article for the medical library community by
87 Hannigan (1997). AR principles can be traced to the ground-breaking work of Kurt Lewin in the social sciences and John Dewey in education. According to Hannigan, AR employs a variety of research methods and data sources. "Data collection methods include but are not limited to checklists, attitude scales, self-reports, focus groups, individual interviews and field notes. Methods of analysis include, but are not limited to, descriptive and inferential statistics and content analysis" (Hannigan, 1997, p. 55). AR emphasizes a bottom-up approach to research and emphasizes useful outcomes (Scherer & McKee, 1993). Hannigan (1997) identified a number of characteristics basic to the AR methodology: • Action research is based in practice. • Action research is participative. • Action research occurs in naturalistic settings. • Action research is cyclic and reflective. • Action research uses appropriate research methods and data sources. (p. 54) The assumptions underlying AR are important in understanding the methodology. Stringer (1996) highlighted the postmodern underpinnings and assumptions of AR methods. Zuber-Skerritt (1996) and Hall (1996) tied AR to critical theory and its power to emancipate through the engagement of participants in self-conscious critique. Both schools of thought stress the notion that there can be no objective truth because there is an essential relationship between the ways in which knowledge is produced and the way power is exercised. The logic of AR leads the researcher to examine the ordinary, everyday, taken-for-granted ways in which people organize and carry out their private, social, and professional activities. Qualitative AR focuses on particular contexts, on the meaning of the context to the participants, and on the processes
88 occurring in these contexts (Maxwell, 1998). Stake (1995) noted that AR is qualitative inquiry that is subjective and honors multiple realities versus a single view. A second assumption underlying AR is that it is a form of experiential learning that supports professional and personal development (McGill & Beaty, 1995; ZuberSkerritt, 1996). "The process of action learning is intentionally iterative between the objective world of things and the subjective world of feelings and works on making explicit the links between them" (McGill & Beaty, 1995, p. 38). One of the aims of an AR project is to bring about the practitioners' better understanding of their professional practices. A third assumption underlying AR is the general systems approach. AR relies heavily on the holistic view of the world presented in general systems theory: Humans are understood to exist only within social systems, and these systems have properties and processes that condition human behavior and are in turn conditioned by that behavior. Social systems are not mere structures but are processes in continual motion. They are dynamic and historical. They are also interlinked, entwining the individual social structures and the larger ecology of systems into complex interacting macrosystems. (Greenwood & Levin, 1998, p. 71) AR can also be understood as an effort to transform society into more open systems as conceptualized in general systems theory. Knowledge emerges and is evaluated through acting or as a consequence of actions. From the AR perspective, inquiry itself is treated as a coherent social field or system in which truth is not a thing to be acquired but rather an aim of an endless process of collaborative social inquiry. Womack (1997) saw AR as a methodology that introduces a "treatment" and attempts to establish cause and effect on a local scale.
Rationale for the Use of AR
89 AR is an effective strategy for solving practical problems, making process improvements and changes, and evaluating the consequences. "AR is not a research method, as many methods of data collection may be used in AR projects. It is, rather, a way of doing research and acting to change situations at the same time" (Hughes, 1997, p. 2). For Hart and Bond (1995), AR is an appropriate research choice when problem solving and improvement are on the agenda. Many practitioners are using this approach already, even if they do not identify the process as AR: The combination of enquiry, intervention, and evaluation which powers the AR cycle mirrors the iterative processes employed by professional staff in assessing the needs of vulnerable people, responding to them, and reviewing progress. Thus, many practitioners will already be familiar with an AR approach, even though they might not explicitly label what they do as such. (Hart & Bond, 1995, p. 3) AR was designed specifically to bridge the gap among theory, research, and practice. In arriving at an understanding of AR, the primary investigator took a number of themes into consideration from Hart and Bond (1995). First, Hart and Bond identified the theme of the researcher as a "change agent." Many of the AR studies reviewed by Hart and Bond depicted the researcher as promoting a climate of change, taking charge of the change, empowering others to take the change forward, and creating alliances that open up space for others to become change agents themselves. Second, there is a conflict of values and of methodological approach between top-down goal setting and bottom-up, grassroots initiatives, despite a convergence of interests around a particular problem. The researcher needs to work with the group to arrive at consensus on the goals and methods that apply to the problem. The typical bureaucratic vision of formalization and hierarchy for consensus is rejected in favor of a democratic, participatory approach from the professionals involved in the AR
90 project. Third, timescale has an impact upon the process and outcomes of AR projects such as the TCN project. A top-down assigned project moves away from a task focus and toward a more empowering, diffuse, and multi-level approach, given a sufficient length of time. This developmental movement issue influences the role of the professional over time and occurred in the TCN, which spanned an 18-month grant period and continued into the 1999-2000 school year. Over the span of a project, the professional leading an AR project often decides to step back from the project to initiate another one elsewhere, or decides to lay aside his or her professional "expert identity" in favor of an "insider role" or "advocacy role." A fourth factor to consider in AR projects is the way in which a project is funded and by whom. The extent of funding and the nature of the relationships among stakeholders is likely to influence the development, objectivity, and outcomes of the research. If the researcher and stakeholders are under an obligation to the funding body, the perceived independence of the researchers is at stake. Of significance to this research project, the Illinois State Library as a key funding agency did not dictate the research methods, interventions, or anticipated outcomes of the TCN project, so the project was driven at the grass-roots, community level. Finally, there are a variety of forms that the researcher/practitioner relationship takes in AR projects. No one form is better than another, and there are certain problem contexts that are helped by the intervention of an outside researcher, just as there are others that are best tackled by an inside practitioner (Hart & Bond, 1995). In AR, the most important lesson appears to be the process of defining the problem and formulating research questions so that the process is collaborative in nature. Later research findings drawn from the TCN project
91 illustrated that the project director and partner members collaborated extensively on the school safety problem and the practical questions to address through focus groups, surveys, informal communication and monthly partnership meetings. The generalization of findings from AR studies, or external validity of the research, can take a number of forms. Findings from a project can be used to initiate another project and to extend what has been learned to a different setting. Or case studies may be evaluated in relationship to similarities with one's own situation, and comparisons of more general relevance to practice are possible. Transferring knowledge from one context to another relies on understanding the contextual factors in the situation where the inquiry took place, judging the new context where the knowledge is supposed to be applied, and making a critical assessment of whether the two contexts have sufficient processes in common to make it worthwhile to link them. (Greenwood & Levin, 1998, p. 79) This comparative approach leads to an evaluation of practice and can prompt further action for improvement. In the final concluding chapter, practical implications of the TCN experience are identified for the Aurora community and library professionals in general. The TCN's Leadership Team has been provided with the case-study research results for benchmarking so future planning of health-information service improvements can utilize the needs-analysis data gathered. AR projects are part of a "strategic view" of professional practice described by Carr and Kemmis (1986). From this viewpoint, professional practice is conceptualized as incorporating a form of "consciousness," a way of thinking about work based on four assumptions. First, educational and caring activities are historically located with a past that influences present practice and a current practice that aims for improvement in the future. Second, these activities are social activities with consequences for both individuals and the wider society. Third, educational and caring activities are intrinsically political as they affect the life chances of people and
92 shape the services available to them. Finally, every act of teaching and caring is problematic and therefore has the potential to be reflected upon and reconsidered to inform future practical judgments and interventions. Reflective teaching and caring activities have the ability to promote progress toward a more rational and just society. The TCN activities were rooted in these assumptions drawn from AR, and it was the intent of the partner members to have an impact on health-information services offered in the local Aurora community for teens and their parents. Hart and Bond (1995) saw AR and its project approach perspective of "critical communities of enquirers" as a fundamental expression of the strategic view of professional practice. Acccording to Stringer (1996), the solutions are built collaboratively through consensus: Community-based research starts, as does all research, with a problem to be solved. Unlike traditional approaches to research, however, the goal is not the production of an objective body of knowledge that can be generalized to large populations. Instead, its brief is to build collaboratively constructed descriptions and interpretations of events that enable groups of people to formulate mutually acceptable solutions to their problems. (p. 145) This process is particularly relevant to the TCN project because the participating agencies came together to define and address a local community problem: school safety and youth violence.
Credibility, Validity, and Workability in AR Credibility in qualitative AR, as compared to validity of quantitative research findings, involves "the arguments and processes necessary for having someone trust research results" (Greenwood & Levin, 1998, p. 80). There are two different types of credibility that need to be considered in AR projects--internal credibility and external credibility. Questions of validity are not as crucial in qualitative research studies as are workability and credibility (Maxwell, 1998).
93 Knowledge that has internal credibility is based on the acceptability of the knowledge to the group generating it. From an AR viewpoint, the TCN steering committee is the forum that assesses the internal credibility of the knowledge gained from this research project. External credibility, on the other hand, is knowledge capable of convincing someone who did not participate in the inquiry that the results are believable. As the research project evolved, the Northern Illinois University (NIU) educational technology dissertation committee provided the necessary feedback on appropriate criteria to judge this study's external credibility. External validity, or the ability to generalize beyond the specific instances or people studied, is usually not of prime importance for AR or case-study research investigators (Grady & Wallston, 1988).
AR and PAR Models AR is described in the literature as consisting of spirals and cycles of diagnosing, action planning, action taking, evaluating, and specifying learning (Kock, McQueen, & Scott, 1997). Figure 5 illustrates the phases involved in the process. Smith (1997) described the AR cycle as primarily a praxis or a dialectic: Individuals make connections with others, recognize a common need, and know it well. Then a praxis begins--reflecting, taking action, and reflecting on that action. PAR develops a repetitive, transforming rhythm of reflection-action, action-reflection in which spiralling moments of "think, discover/recover, and do," "think, discover/recover, and do" extend into the future. (pp. 186-187) Much of the current AR literature examined in education, social sciences, and management sees the researcher working in partnership with members of the group as "co-researchers" (McTaggart, 1991; Reason, 1994; Scherer & McKee, 1993; Smith, 1997; Whyte, 1991). The term "participatory action research," or PAR, is used to describe this form of AR. For purposes of this research project, the PAR methodology
94 is seen to apply to the TCN partnership.
Figure 5. The Action Research Cycle (adapted from Kock et al., 1997, p. 8)
Qualitative Research Focus of This Study According to Savenye and Robinson (1996), qualitative researchers are committed to developing an understanding of human systems. To develop this understanding, qualitative research is conducted in natural settings and involves detailed, rich descriptions of human behaviors and attitudes. "Multiple realities" are presented in qualitative studies because individuals involved in various social settings cognitively construct the environment. Because new issues and questions arise in qualitative studies as the researcher interacts with those studied, the research design emerges as the study progresses. Merriam (1998) indicated that one of the assumptions underlying qualitative research is that "reality is holistic, multidimensional, and ever-changing" (p. 202). This assumption of qualitative research directs the investigator to observe people's construction of reality and how they understand the world. Miles and Huberman (1984) described qualitative research
95 as "context-embedded qualitative inquiry" (p. 15). There are a number of advantages to qualitative data as reported by Miles and Huberman (1984): "Qualitative data are a source of well-grounded, rich descriptions and explanations of processes occurring in local contexts. With qualitative data one can preserve chronological flow, assess local causality, and derive fruitful explanations" (p. 15). The qualitative data gathered from partners involved in the TCN partnership included anecdotes about youth affected by community violence and the program impact, exit interviews, open-ended comments to questions about partnership effectiveness and partnering behaviors, benchmarking comparisons on youth risk behaviors, and a project journal. Gathered throughout the 18-month TCN project, these data sources emphasized the multiple viewpoints and voices of the partners in forming and building the Aurora, Illinois-based network devoted to the improvement of health-information access for teens and their parents. The reality of the TCN is the vision built and picture drawn by its partner members through the partnership violence prevention and community change activities. Partnership themes identified in later chapters were pulled from the anecdotes, interviews, survey responses, and written comments inductively to understand the dynamics of the partnership. The primary investigator held the dual role of project director and researcher and was an influential participant-observer in the AR project.
Case-Study Research and Defining the Case According to Crowl (1993), Yin (1994), and Maxwell (1998), case studies are the preferred strategy when "how" or "why" questions are being posed, when the investigator has little control over events, and when the focus is on a contemporary
96 phenonemon within some real-life context. The case is also considered the unit of analysis. The research questions being asked in this contemporary research study do address "how" and "why" partnerships develop and grow, so it is apparent that the TCN study matches the conditions for a case-study research project. Case studies also typically involve direct observation and systematic interviewing to gain insight into the case. Miles and Huberman (1994) defined the case as "a phenomenon of some sort occurring in a bounded context" (p. 25). Often, the boundaries between phenonemon and context are not clearly evident. For the researcher, it is important to clearly define the case from the context. "Case studies are differentiated from other types of qualitative research in that they are intensive descriptions and analyses of a single unit or bounded system, such as an individual, program, event, intervention, or community" (Merriam, 1998, p. 19). For the Teen CARE network project director, it was important to distinguish members from nonmembers of the partnership as the TCN formed and expanded over the 18-month grant period. It was also important to obtain feedback from partner members about partnership activities and future directions in the form of written comments and interviews. Yin (1994) noted that case studies are used extensively in evaluation research to explain the causal links in real-life interventions such as new program implementation. For purposes of this research project, the TCN partnership was considered to be the case or unit of analysis, but the case also included "embedded" units of diverse members and funding agencies. The context of the study was the Provena Mercy Center community hospital service area, which included schools and public libraries in Aurora, Batavia, North Aurora, Montgomery, and Sugar Grove. Limitations of the Case-Study
97 Research Methodology Quantitative researchers have found that self-reporting as used in qualitative research is influenced by social desirability factors (Dolcini, Adler, & Ginsberg, 1996; Grady & Wallston, 1988). Self-reporting also introduces systematic error and bias because persons in stronger relationships are more likely to confirm their interaction patterns (Wilson, 1990). For example, Calloway and Morrissey (1993) found, in their study of four U.S. cities with Robert Wood Johnson Foundation Programs on Mental Illness sites, that 7 out of every 10 relationships cited by either respondent were confirmed in their study of 31 to 44 organizations that provided mental health and other community support services to persons with a chronic or serious and persistent mental illness. Data was gathered from a key informant or "boundary spanner" in each organization. Interviews plus a questionnaire with 16 questions produced a 100.0% response rate among the key informants (Calloway & Morrissey, 1999). The anonymity of the partner member responses is a second limitation of the case-study methodology. Although names can be changed, the working relationships among the partner agencies become a part of the public record as the case-study report evolves. To ensure that partners agreed to the use of exit interviews in the final casestudy report, the TCN Program Evaluation/Partner Release Form was developed. Each partner interviewed signed the release form, so the names of exit interview respondents are tied to the quotes presented in the Chapter 5 findings. Tied in with the observations and interviews used in this case study are threats to validity. The primary investigator was aware of possible researcher effects such as reflexivity or "the mutual influence of the research participants and the researcher on each other" (Maxwell, 1998, p. 86). Reactivity during meetings and interviews is a
98 related threat to validity that the primary investigator addressed through member feedback. To check for self-report bias, the primary investigator conducted "member checks" with interviewees as meeting minutes were produced and transcripts compiled. Reactions of interviewees to the transcripts confirmed in all instances that the transcripts were accurate and a complete record of the interview process. To further ensure validity, the primary investigator employed triangulation, feedback from a variety of people, "member checks," "quasi-statistics," and comparison with other case studies and multisite studies as suggested by Maxwell (1998). Examples of related case-study research examined as a credibility and validity check include Bazzoli et al. (1997), Millard (1999), Pennbridge (1988), and Plaut and Landis (1992). Case-Study Data Collection and Analysis Techniques Employed in This Study Yin (1994) indicated that two major tasks of collecting qualitative data involve (1) gaining access to key organizations or interviewees and (2) having sufficient resources to gather and analyze data. Fortunately for this research project, the Illinois State Library provided major funding of the TCN partnership in 1998 and 1999 over an 18-month period. As a result of the LSTA grant of $104,890 plus a match by Provena Mercy Center of 15.0% and a strong commitment on the part of the member agencies, routine access to partner member representatives for meetings, exit interviews, and evaluation surveys was facilitated. LSTA funding supported the modification of the YRBS questionnaire for Aurora and its administration at local high schools. Funds were also available to hire the NIU Educational Testing Service and Social Science Research Institute/ Public Opinion Laboratory to assist with Statistical Package for the Social Sciences (SPSS) data analysis.
99
Convenience and Purposive Sampling of TCN High-School Students and Partner Agency Representatives Interviewed Boyatzis (1998) indicated that sampling decisions affect and determine the degree of reliability and validity attainable in qualitative research studies. Miles and Huberman (1994) noted that sampling involves decisions about which people to observe and interview and about which settings, events, and social processes to describe. Convenience samples of high-school students were drawn from the Aurora private and public high schools for the youth risk behavior needs assessment in 1998. Only those students who completed a signed consent form were provided a YRBS form from either their physical education or health education teacher in May/June 1998. Appendix B contains a copy of the YRBS Survey Consent Form approved by the NIU Institutional Review Board in May 1998. For exit interviews with partners, signed consent forms were required to be on file before conducting an exit interview with partner agency representatives. Appendix B contains a copy of the TCN Program Evaluation/Partner Release Form. Partnering behavior surveys were sent to representatives of all 40 TCN partner agencies. The primary investigator recruited member agency representatives for interviews that represented the mix of agencies involved in the partnership. After two mailings to TCN partners about exit evaluation interviews, time constraints dictated that volunteers were selected over nonrespondents. The final group of 18 partner members who provided exit interviews reflected a convenience sample bias toward the more committed and involved partners. However, the results of the exit interviews reveal that these agency representatives provided honest
100 feedback about partnership program strengths and weaknesses and future directions for the organization as a whole. The first exit interview was conducted by the investigator in an unstructured, conversational style in early July 1999. After a verbatim transcript was compiled of the first interview, it became apparent to the investigator and several dissertation committee members that a series of structured questions was required for comparison of later interviews. It was also recommended to the interviewer by the dissertation committee co-chairs that the interviewer avoid "leading questions" and bias in the wording of questions. A final series of questions for the 30-45-minute exit interviews was compiled with this advice in mind and utilized in the remaining l7 interviews conducted over the time period of July 1999 to September 1999. Appendix C contains a copy of the final exit interview questions. The exit interview schedule ensured the reliability of the qualitative data produced and enhanced comparative analysis techniques employed.
Qualitative Data Analysis Techniques Employed Miles and Huberman (1984) stressed that decisions concerning how qualitative data is to be processed should be documented to ensure reproducibility of findings. Data reduction is one consideration for the qualitative researcher. Which data chunks to code, which to pull out, and which patterns to summarize are analytical choices that affect the evolving case-study narrative. Data displays, including narrative text, graphs, matrices, and charts, contribute to the conclusions drawn and allow future verification by other researchers. All qualitative data analysis is intended to contribute to an understanding of what events mean and their uniqueness (Miles & Huberman, 1984; Stake, 1994).
101 The multiple data sources gathered throughout the TCN grant project contributed to the process of triangulation or "convergent validation" (Jick, 1979; Miles & Huberman, 1984). Although the methodology focused on gaining insight, both qualitative data and quantitative data were viewed as complementary and allowed for multiple viewpoints and greater accuracy. The triangulation techniques employed in this research were seen to enrich understanding of partnerships by allowing for new or deeper dimensions to emerge. An assumption underlying triangulation is that the weaknesses in each single method will be compensated by the counter-balancing strengths of another (Jick 1979).
Thematic Analysis, Coding Categories, and Reliability The interorganizational network effectiveness model of Alter and Hage (1993) (see Figure 4) was used to analyze the TCN effectiveness data from LSTA grant project final reports and meeting minutes. The problem setting, direction setting, and implementation phases were employed from Gray (1989) to illustrate the development of the partnership over the 18-month grant period. The analysis of data was deductive in this instance and based on prior theory and research. A full chronology of the grant implementation activities is found in Appendix D. Codes for analyzing the exit interviews and open-ended comments were developed inductively through open coding based on the constant comparative method (Merriam, 1998; Strauss & Corbin, 1990). In this research project, the themes were derived from the data itself for exit interviews and open-ended questions. Boyatzis (1998) indicated that themes found in qualitative data can describe or explain a case: "A theme is a pattern found in the information that at minimum describes and organizes possible observations or at the maximum interprets aspects of
102 the phenomenon" (p. vii). For Boyatzis, reliability is critical in thematic analysis. Reliability of observation, labeling, and interpretation is enhanced through standardization of coding to ensure consistency over time and events. Consistency is attained when different people observing or reading the information see the same themes in the same information. Multiple observations, observers, and data sources increase confidence in the dependability of the judgments related to qualitative data interpretation. The standardization of the exit interview protocol and use of member checks are examples of how the reliability of the methodology employed was addressed in this research project.
Ethical Issues Addressed Winter (1996), in an article on fieldwork methods, identified a number of issues to address when conducting qualitative research. It is important for the researcher to consult all relevant persons, committees, and authorities impacted by the research study and its findings. It is also important to conduct all research in a visible and open manner so that the researcher is open to suggestions from others and feedback on methods. In conducting the TCN partnership research, the primary investigator obtained permission before making written observations or examining documents produced for other purposes. For example, Provena Mercy Center's marketing department was asked for access to the Professional Research Consultants, Inc. (PRC) Community Health Assessment report issued in late 1998 for the Aurora, Illinois, community by Provena Mercy Center and Rush-Copley Medical Center (1998). The Provena Mercy Center marketing department approved the primary investigator's request and confirmed that that there was agreement between the PRC findings on general
103 community needs in Fall 1998 and the youth-needs assessment conducted by the TCN partnership in May-June 1998. The researcher also must accept responsibility for maintaining the confidentiality of responses provided by research subjects. The NIU Institutional Review Board approved the YRBS protocol in May 1998, and procedures were put in place in the event students objected to some of the sensitive questions asked related to violence and sexuality. Informed consent forms for students answering the YRBS were distributed by teachers in advance of YRBS questionnaire administration. Signed consent forms were also required from TCN partners before exit interviews were conducted. Samples of these consent forms are found in Appendix B.
Data Sources Focus Group Meetings and Teen Health Concerns Inventory Two focus group meetings were held with teachers, guidance counselors, librarians, school nurses, youth service agencies, and health-care providers in October 1997 and November 1997. A Teen Health Concerns Inventory, adapted from Weiler, Sliepcevich, and Sarvela (1993), was administered to professionals attending the two meetings held at West Aurora High School. A copy of the inventory is found in Appendix E. Minutes of the meetings were compiled by the group facilitator.
Secondary Data Consulted Available data sources consulted for this research project include: · National Youth Risk Behavior Surveillance Survey (YRBSS) data (Kann et al., 1998), which focuses on self-reports of health risk behaviors rather than related
104 knowledge, attitudes, or beliefs across the United States (Kolbe et al., 1993, p. 6); · Illinois YRBSS (1995), an Illinois subset of the National YRBSS data for 1995; · Community needs assessments available for the greater Aurora community, including the United Way of the Aurora Area (1995; 1996), Kane County Health Department (1997), and Provena Mercy Center and Rush-Copley Medical Center (1998); · Newspaper articles from the Beacon-News, Chicago Tribune TribWest Section, and the Lexis-Nexis database that includes select Copley News Service and Chicago Tribune articles since 1995; · School report cards from the East Aurora School District #131 (1998) and West Aurora School District #129 (1998); and · Brochures and program handouts from Aurora and Illinois community agencies serving youth and advocating for prevention, peacemaking and non-violence. An example of an Illinois document of interest to this research project is the Illinois Violence Prevention Authority's statewide violence prevention plan (1998).
National YRBS Data In reviewing the data gathered from the Aurora Schools YRBS, it was important to compare the Aurora freshmen sample with 1997 national and 1995 State of Illinois results. Data for students in grades 9 and 10 became a "benchmark" for comparisions with the final sample of responding Aurora high-school students. As reported by Kann et al. (1998), students in grades 9 and 10 were more likely than students in grades 11 and 12 to report the following risk behaviors nationally: · Weapon carrying;
105 · Being threatened or injured with a weapon on school property; · Participating in a physical fight; · Having property stolen or deliberately damaged on school property; · Feeling too unsafe to go to school; · Suicide-related behaviors; · Lifetime inhalant use; · Initiating cigarette, alcohol, and marijuana use before 13 years of age; · Initiating sexual intercourse before 13 years of age; · Not using birth control pills; and · Eating more than two servings of foods typically high in fat content daily. (pp. 2930)
Instrumentation and Data Sources A decision was reached by the TCN steering committee to utilize a modified YRBS instrument to assess the health risk behaviors of Aurora teens. The TCN steering committee arrived at this decision over the course of four months at regularly scheduled meetings. As a result of the convenience sampling employed, the YRBS was administered primarily to freshmen in May and June 1998 through physical education and health education classes at East Aurora High School, Rosary High School, and West Aurora High School.
Aurora Schools YRBS, May-June 1998 The Aurora Schools YRBS was conducted in May-June 1998 after the NIU Institutional Review Board approved survey protocols. A copy of the final modified YRBS survey is found in Appendix A. The TCN steering committee reviewed the 84
106 questions from the YRBS; made minor modifications in wording of these questions; and added 16 questions that covered teen media preferences, empathy for others, health decision-making, and problem-solving. These questions were based on similar questions found in inventories constructed and validated over time by Heppner (1988), Baker and Roberts (1989), and Bryant (1982). A total of 503 students responded to the YRBS. Students were selected primarily from the freshman class at East Aurora, West Aurora, and Rosary High Schools (N = 408). Freshmen were selected for participation based on the potential impact of survey results for health education programming over the next three years in the high schools. The total population of Aurora freshmen attending public and private high schools was estimated at 1,750. The final availability sample of responding freshmen students (N = 408) represented 23.3% of the total high-school freshmen population in Aurora. West Aurora freshmen represented 69.6% of the sample (N = 284), Rosary High School freshmen represented 20.3% of the sample (N = 83), and East Aurora High School freshmen represented 10.0% of the sample (N = 41). The East Aurora High School freshmen were underrepresented in this final sample due to the fact that (a) health education classes were mixed with freshmen through senior years in school, and (b) the groundwork in communicating information about the YRBS to health education teachers was less effective at East Aurora High School than at West Aurora High School and Rosary High School. The library contact persons at West Aurora and Rosary High Schools, Mary Hauge and Sister Bernadette Marie McGuire, worked closely with health education teachers, the heads of the physical education department, and building principals to obtain permission for administration of the YRBS.
107
Steering Committee Minutes and Reports The TCN formed a steering committee in December 1997 to prepare a grant proposal and respond to proposed youth violence prevention initiatives. The steering committee met monthly at various partner facilities, and minutes from these meetings were compiled. The LSTA grants required the production of Preliminary Narrative and Financial Reports and Final Reports used for program review by the Illinois State Library's Development Office.
Partnering Behaviors Survey A Partnering Behaviors Survey was distributed to the TCN partner agencies in June and July 1999. The survey was adapted from a partnering checklist, "How Well Did We Partner?", developed by Sujansky (1991). A copy of the checklist is available in Appendix F. The Partnering Behaviors Survey is based on a model of 10 behaviors that Sujansky (1991) identified and believed contribute to successful partnering in corporations: (1) identify the desired results; (2) agree to make a difference; (3) clarify roles; (4) assess needs; (5) recognize achievements; (6) make ongoing corrections; (7) be willing to take risks; (8) encourage creativity; (9) challenge one another; and (10) evaluate the results and the partnership (see Figure 2). A total of 10 surveys were returned by the initial return date of June 28, 1999. A second round of follow-up surveys was mailed on June 10 to increase the return rate and potential pool of follow-up partner evaluation interviews in July and August. A total of 20 respondents, or 50.0% of the TCN partnership membership, participated in the partnering behaviors evaluation survey.
108
TCN Proiect Exit Interviews The TCN project director conducted semistructured interviews with TCN partners beginning in July 1999. These interviews continued through September 1999. A total of 18 interviews were conducted with TCN partners who signed a release form. Audiotapes were made of the interviews, and verbatim transripts were compiled into Word (.doc) computer files from the audiotapes with the assistance of WordWorks of Aurora. Notes were also compiled from the face-toface interviews when appropriate and were drafted by the primary investigator as the interviews progressed.
Evaluation Checklists Evaluation checklists were distributed for all public programs held in 1998-1999. An assessment of TCN overall programming effectiveness was distributed to TCN steering committee members in August 1998. An assessment of collection development activities and collection use by partner library clientele was distributed in October 1998. Narrative comments were compiled from the seven response forms returned. Public program and collection evaluation assessments were developed for reflection, diagnosis, action planning, and grant reporting purposes by the steering committee and project director. Copies of these assessment tools are presented in Appendix G.
Videorecordings of Programs A statewide teleconference on the TCN project held on March 17, 1999, at the DLS, Geneva, Illinois, was recorded and edited. Lynn Elam, DLS programming
109 director, served as moderator of a panel of TCN partners and experts on media violence and the psychological impact of violence on children. Discussion topics covered the formation of the partnership, the mission of the partnership, implementation of programs, important outcomes of the teen health-information network, how the TCN could be accessed and used, and what practitioners could do to promote school safety and community peacemaking. Several of the public programs were also videorecorded and edited by Video Perfections for distribution to local community cable television stations. The content of these programs was analyzed for themes related to peacemaking and violence prevention.
Artifacts Items produced by the TCN are a record of the partnership's formation and implementation. Examples of artifacts include the Internet website (www.aurora. il.us/teencare), news articles published, press releases issued, brochures, bookmarks, posters, hats, t-shirts, logo, website buttons, displays, photographs, scrapbooks, games, and umbrellas. Brochures, committee minutes, and program handouts from Aurora peacemaking agencies such as the YWCA (1999) were examined to gain an understanding of the prevention, peacemaking, and nonviolence programs already in existence for schools and families.
The Case Study/PAR Results Reporting Style Because the primary investigator of this case study was also the partnership's project director, a decision was made to present the findings in Chapters 4 and 5 from the viewpoint of a participant/observer. These chapters present certain qualitative
110 findings in the first person. Community violence and possible solutions were a matter of great concern to me as an action-researcher and to the partner agency representatives of the TCN. "Value-free" was not the perspective adopted by any member of the TCN. Rather, our partnership and member agencies are committed to community service and care for others. The TCN's "ethic of care" demanded that the findings presented in later chapters make clear my values and perceptions as primary investigator as well as the values of the key TCN stakeholders serving teens and parents in the Aurora, Illinois, community. The voices of the TCN partners are highlighted in Chapter 5 as the findings about partnership effectiveness are discussed.
CHAPTER 4 FINDINGS: PARTNERSHIP PROBLEM SETTING, DIRECTION SETTING, AND YRBS NEEDS ANALYSIS
To facilitate the understanding of why the TCN mobilized around the issues of nonviolence and peacemaking in arriving at its core vision of improving access to health information, this chapter presents background on the critical events occurring in the city of Aurora for the time period of 1994-1997 as reported in major Beacon News and Chicago Tribune news accounts indexed in Lexis-Nexis Universe. News media acounts were used to refresh and validate my observations and judgments concerning the reality of community violence in Aurora and for potential partner agencies. This chapter also introduces the reader to the Teen Health-Information Network (THINK) LSCA grant project initiated by Aurora Public Library in 19941995, how the THINK project and Kane County Public Health Department's Healthy Teens Initiative served as a foundation for the TCN and profiles of the key community agencies involved in the TCN project coordinated by Provena Mercy Center Hospital. Finally, youth risk behavior survey results for Aurora, benchmarking of Aurora YRBS data with Illinois and national results, and an analysis of the "root causes of violence" are presented as part of the problem-setting and direction-setting phases in the development of the TCN project.
Community Violence: A Key Issue for Aurora, Illinois
112
In 1995, Alderman Marc Roberts of the 2nd Ward, a ward that includes some of the city's tougher neighborhoods, summed up the concern of many citizens about gang activities in a Chicago Tribune article as follows: "We're still struggling with how to stop the violence, particularly the random nature of it. So many innocent people are at risk" (Baniak, 1995, p. 1). And on May 20, 1995, I remember attending "A Night of Hoops . . . and Hope," a basketball game at Aurora University, with my husband Jim, son Ken, and friend Jennifer to support a scholarship fund in memory of Moshe Rogers, the slain Aurora Central Catholic High School basketball star who had hoped to attend college but instead became a victim of gang violence on Aurora's east side in February 1995. Crime, it struck me, was "the number-one issue" in the city, and it was reported in the Beacon News that some older people were afraid to leave their homes or even stand near windows. Later, in conducting research on Aurora community social problems, I discovered that several United Way surveys in 1995 and 1996 showed crime and gang activities were among the top concerns of Aurora residents. In addition, I recalled that many people claimed that Police Chief David Stover defeated incumbent Mayor David Pierce in the 1997 Aurora mayoral election because Pierce was believed to be "too soft" on crime. According to other reports in the Beacon News I read, many Aurora citizens believed law and order needed to be restored to the city and that racial tensions needed to be reduced. Racism was seen as an issue tied to increased gang activities in Aurora, and many community leaders believed that a great deal of polarization existed in the city as a result of racial attitudes. A number of study circles were organized by the YWCA for "people [to] become sensitized to the issues and [to] mitigate the polarity with which we live" (Dardick, 1995, p. 1).
After attending several training sessions
113 offered by the Illinois Center for the Prevention of Violence and Aurora Community Study Circles in spring and summer 1998, I developed a better appreciation for the unique violence prevention initiatives already in place in Aurora. As a participant/observer of the violence prevention movement in Aurora, I learned about the Aurora Community Mobilization Advisory Board, Prayer Coalition for Reconciliation, Aurora Community Study Circles, Project Unity's Back to School Fair, and the YWCA's Week Without Violence. My mind and heart opened to the broader Aurora community, and I understood who might be the key community agencies and libraries to commit to forming a partnership of caring library and youth service professionals. Gandhi (1958) called the process that occurred in my growth "ahimsá," or the way of nonviolence and love. Lynn Elam, director of programming with the DLS, believed we could reach a "second generation" of teens by proactively forming a partnership devoted to improving access to health information for teens and their parents. From my present vantage point, I recognize that a solid history of cooperation among the key partnership stakeholders led to renewed dialogue between the libraries and key community agency stakeholders. The Illinois State Library agreed that these were crucial community problems and that we could assess actual Aurora youth risk behaviors and develop a multimedia Internet website for improved access to health information for teens and parents. Fortunately, the LSTA funding provided the needed energic input to make the project happen, build a learning community, and transform the professionals committed to the change project.
Aurora, Illinois, Community Demographics and Diversity
114 According to the latest population figures found on the City of Aurora Internet site (www.ci.aurora.il.us), Aurora has a diverse population of approximately 117,000 residents. The Aurora population consists of 12.0% Black, 22.9% Hispanic, 1.3% Asian, and 53.8% White and other races. Aurora has two public school districts--East Aurora School District #131 and West Aurora School District #129--and a number of private church-affiliated schools (Aurora Central Catholic High School, Aurora Christian, Marmion Academy, and Rosary High School).
Aurora's health delivery
system includes two community hospitals that are part of larger, integrated Illinoisbased health-care networks--Provena Mercy Center and Rush-Copley Medical Center. Dreyer Medical Clinic, a physican group practice, is a major provider of health-care services and affiliated with Advocate Health Care in 1996. As of September 30, 1997, the East Aurora School District #131 (1998) reported a total enrollment of 9,836 students in its 1998 School Report Card. The West Aurora School District #129 (1998) reported an enrollment of 9,238 students in its 1998 Report Card. Although the total population of students is close in number, the racial/ethnic mix and income levels of the students enrolled in the two school districts is not similar. As shown in Table 1 for the high schools only, East Aurora High School reports higher percentages of students in the low-income, limited-English proficient, dropout, and chronic truant categories than does West Aurora High School. Table 1 illustrates the great diversity of students enrolled in the two Aurora public high schools. East Aurora has Hispanic and Black students in the majority (78.6%), and West Aurora's majority student population is White (57.6%). The ethnic diversity and poverty that exists in Aurora is both the city's promise and its challenge. Educational opportunities exist for motivated students with a clear vision of the future. Yet there exist a significant number of students in both school districts who are
115 dropping out (313 students at East and 161 students at West), chronically truant (377 students at East and 21 students at West) and failing to benefit from their high-school educational experience. For these students, high school is seen not as a "ladder of opportunity" or as a "growth experience" but as an arena of failure and unfulfilled promise. Table 1 Aurora High-School Student Population, 1997-1998 East Aurora High School (#131) N
%
West Aurora High School (#129) N
%
White
410
19.7
1,446
57.5
Black
385
18.5
468
18.6
1,249
60.1
546
21.7
30
1.4
49
1.9
2
0.1
5
0.2
2,076
99.8
2,514
99.9
Low-income
677
32.6
350
13.9
Limited-English proficient
222
10.7
68
2.7
Dropouts
313
15.1
161
6.4
Chronic truancy
377
20.0
21
0.9
Hispanic Asian/Pacific Native American
TOTAL
Source: Aurora East School District #131 (1998); West aurora School District #129 (1998).
A Beacon News story on the new "Bright Futures" class at East Aurora High School taught by Jonathan Switzer, pastor of high school, college, and career
116 ministries with Aurora Community Church, supports this perspective on teen dropouts. Dropouts lack a vision of their futures, as Jonathan Switzer quickly learned from East Aurora High School's building principal: "Last October, I [Jonathan Switzer] met with [East High School Principal] Dr. Barwa, and he told me the biggest problem with kids who drop out is they have no vision for the future" (Roth, 1998, p. A3). To reach Aurora students and parents with its healing message of hope, health promotion, and wellness, Provena Mercy Center's Medical Library convened a series of meetings between the Aurora public and private schools, public libraries, the DLS, youth service agencies, and health-care providers in Fall 1997. These meetings were intended to build connections between a major Aurora, Illinois, health-care provider and professionals serving youth to improve the delivery of community-wide health information to teens and their parents. Stakeholders in the Library/Community Agency Partnership
Provena Mercy Center: The Core Agency Mercy Center for Healthcare Services, founded by the Sisters of Mercy in 1911, became part of the Provena Health system in December 1997. Provena Mercy Center, as it is now called, is a 356-bed community hospital and multiple-site healthcare provider of general medical and behavioral health services with approximately 900 full-time equivalent employees. The hospital served 11,092 admitted patients, 56,157 outpatients, and 29,429 emergency-department patients in 1998. Mercy Center for Healthcare Services formed the integrated Provena Health Catholic system in 1997. The system includes seven other Illinois hospitals and a
117 large number of long-term care and residential facilities; home health agencies; primary care, diagnostic, and specialty clinics; pharmacies; medical laboratories; and medical equipment outlets. The Provena Health system extends from northern Illinois south to Kankakee and Champaign and into west central and northwest Indiana. With the move to a larger health-care system, Provena Mercy Center adopted its new name and a new mission with a renewed emphasis on community outreach into its surrounding southern Kane and Kendall County service area. In 1997, the Educational Services Department of Provena Mercy Center supported the hospital's overall training mission through the provision of orientation classes, nursing education, in-service education, safety education, management development, a speakers' bureau, community education class offerings, patient education classes and resources, audiovisual services, library services, and individualized continuing education for affiliated physicians. The Educational Services Department consulted on program development and marketing of health and wellness programs to local employers and individual consumers. Through June 1998, the Educational Services Department also handled the booking of meeting rooms for local nonprofit agencies and support groups such as the Community Resource Team (CRT), a social services networking group based in Aurora that meets on a monthly basis. In the mid-1990s, nearby hospitals were building fitness centers on their campuses and investing significant capital funds to support community health and wellness needs. Rather than make a major capital investment as had its competitors, Rush-Copley Medical Center and Delnor-Community Hospital, Provena Mercy Center adopted a different strategy. The hospital administration endorsed partnerships with already existing fitness centers to keep costs down and extend the new Provena "brand name" into the surrounding community. For example, Provena Mercy Center
118 established a partnership with the Westbank Health and Fitness Center in Batavia, Illinois, in 1997, which led to the recent purchase of Westbank and the expansion of fitness services in November 1999 by Provena Health. Provena Mercy Center's support of "empowered health-care consumers" through community-based health and wellness programs was translated into outreach efforts to Aurora churches through a three-year parish nurse grant program begun in 1998 at St. Nicholas Church, a predominantly Hispanic Catholic parish on Aurora's east side. Provena Mercy Center's vice president for human resources and director of education saw the TCN partnership between libraries and schools in 1997-1998 as part of the overall corporate strategy of community outreach and improved healthinformation services to teens and their parents. The administration believed that both general medical and behavioral health areas at Provena Mercy Center would benefit from the proposed community outreach project. Figure 6 illustrates the central role that Provena Mercy Center assumed in developing the TCN partnership. The Medical Library, as part of the Educational Services Department, joined in the expanded community education outreach efforts to propose the addition of wellness information centers in public libraries and school buildings. The rationale for the library's outreach effort was based on the experience gained and lessons learned from the THINK grant experience of 1994-1995. Partners were sought from all sectors of the community that had an interest in teens, effective parenting, and health-information services.
119
Figure 6. Library/community agency partnership development stakeholders
120 Marketing of the partnership was particularly focused on the church community through the Aurora Area Clergy Association and Prayer Coalition for Reconciliation and on social service providers through the CRT. These organizations were involved in nonviolence and peacemaking activities in Aurora and the sharing of information about social service programs provided in the southern Kane County and Kendall County hospital service area. Outreach from Provena Mercy Center to these agencies reflected a grassroots approach to informing and involving interested community partner agencies. Aurora Public Library's THINK Project and the Kane County Health Department's Healthy Teens Initiative in 1994-1995 In the THINK grant implementation, Aurora Public Library worked with a number of public and school libraries along with DLS, Mercy Center for Healthcare Services, the Kane County Health Department, and Kane County INFO to provide updated health information to teens and parents in local libraries. Aurora Public Library served as the lead agency and concentrated its efforts on cooperative collection development on teen health topics, a health-information needs survey at East and West Aurora high schools, the addition of the Health Reference Center on CD-ROM at Aurora Public Library's Reference Department, and community education programs for teens and parents on teen abstinence and AIDS. During the same time period, several teen health-related products and services were being developed under the auspices of the Kane County Health Department's "Healthy Teens Initiative," funded with a grant from the Illinois Department of Public Health. First, a printed handbook, Healthy Teens Handbook (Kane County INFO, 1994), which identified health and social services available in Kane County for teens,
121 was produced in quantity (10,000 copies) for distribution to schools and agencies serving youth in 1995. This handbook was compiled by the staff at Community Contacts/Kane County INFO. The handbook's content was based on an assessment of teen health-information needs in the county. It was a logical and natural arrangement for Kane County INFO. This agency had 20 years of experience with its telephone-based information and referral service for Kane County as a whole and with its biennial production of the printed Directory of Human Services in Kane County (Kane County INFO, 1996), first published in 1980, and the Senior Handbook (Kane County INFO, 1976), first issued in 1976. These comprehensive tools identify all available health, human, and social services in the county. Thus, production of the Healthy Teens Handbook (Kane County INFO, 1994) was efficient, accurate, and authoritative under Kane County INFO's leadership, and their new product for teens identified an extensive network of health and social services available to teens and their parents in Kane County. A second service supported with funds from the Kane County Health Department's Healthy Teens Initiative (1994-1997) was the Crisis Line/INFO's Teen Talk Line established in 1995. Adolescent peer counselors were trained in crisis intervention and I&R procedures by crisis-line professionals. The Teen Talk Line service that was started in 1995 remains in operation today at 630-482-9595. The phones are staffed by teens on Friday, Saturday, and Sunday from 3-9 p.m. and at other times by trained adult counselors to handle the many questions received about relationships and personal health. There were two missing pieces from the 1994-1995 THINK project that remained in the "memory bank" of the partners involved. First, how could the Internet and World Wide Web be used to facilitate community-wide access to consumer health
122 databases? Second, how could the THINK partnership be expanded to include a broader representation of youth service agencies, churches, government officials, and health-care providers? Fortunately for the Aurora community and original THINK library partners, these two missing pieces were incorporated into the Provena Mercy Center LSTA grant project in 1997-1999. By late 1997, Internet technology had evolved as the primary means of delivering health information to consumers. Website development was a skill that was being taught to teens in the high schools. The Aurora Online Community Network (AOCN) project, supported by a City of Aurora grant under Mayor David Pierce, was expanding e-mail and web search access to the Internet for teachers and students alike. And a change in mayor from David Pierce to former chief of police David Stover did not dampen the spirit of the Greater Aurora Chamber of Commerce in promoting the Internet and AOCN through private contributions at an Aurora University Internet exhibit in early 1998. It was clear that a health-information partnership involving libraries needed to reflect the Aurora community and the promise of emerging Web technologies; this was an important lesson learned from the THINK project. Working in collaboration with West Aurora High School's head librarian and the director of education at Provena Mercy Center, the medical librarian arranged several focus group meetings at Provena Mercy Center and West Aurora High School. These focus group meetings were held to determine the priority of teen health concerns from the viewpoint of professionals working closely with Aurora teens and parents. The meetings were also necessary to identify the media and Internet linkages needed to reach the estimated 12,500 Aurora teens and their parents with varied needs for health information.
123 Important Stakeholders in Teen Health and Health Information The important stakeholders in teen health issues and the delivery of health information were not limited to the city of Aurora proper. Librarians, health-care providers, and agencies serving youth identified below, joined the partnership because of a shared mission and vision for improving the delivery of health information to teens and their parents in Aurora and the state of Illinois as a whole.
Illinois State Library The Illinois State Library provided the funds that supported the TCN's start-up period. The mission of the Illinois State Library (www.library.sos.state. il.us), located in Springfield, Illinois, is to develop and promote libraries in order to enrich the quality of life for the people of Illinois. Inherent in this mission is the State Library's advocacy of the right of Illinois citizens to read and have full access to information. This mission is accomplished by sharing library resources through the Illinois Library and Information Network (ILLINET), first established in 1980 and now an automated resource network of 3,000 Illinois libraries. Federal funds through the Library Services and Technology Act became available to libraries of all types in 1997, which made Provena Mercy Center's LSTA grant application possible. Historically, federal funds have been used for the automation of Illinois libraries and have enabled the development of innovative programs regarding access to information. The LSTA program is seen as both strengthening basic service available at all Illinois libraries and supporting the development of "cutting edge library services" using technology to build com-munity networks (Illinois State Library, 1998). The key contact with the Illinois State Library was Amy Kellerstraus, LSTA Program Coordinator.
124
DuPage Library System (DLS) DLS (www.dupagels.lib.il.us), located in Geneva, Illinois, is a regional multitype system funded by the Illinois legislature through the Office of the Secretary of State/State Librarian. Members include 149 academic, public, school, and special libraries in 335 facilities in parts of Cook, DuPage, Kane, Kendall, and Will counties. DLS supports its member libraries in their efforts to enhance and expand local library services and meet statewide standards through a variety of services and programs-automation and networking, coordinated buying, consulting, and continuing education. The key contacts with the DLS were Lynn Elam, programming director; Don Nims, Internet coordinator; and Pamela Feather, executive director. Provena Mercy Center Library utilized DLS consulting services in writing the TCN grant and in developing the information services consistent with statewide library service standards and innovative practice. DLS also offers an annual grant, the Millennium Service Award, to a member library that best exemplifies service planned to meet the challenges of the future through adaptations, innovations, or extensions of traditional service to meet the changing needs of library clientele.
Kane County Health Department A third stakeholder in the TCN was the Kane County Health Department (www.co.kane.il.us/health.htm). This department provides services aimed at the promotion of health and the prevention of disease. The Kane County Health Department was established by resolution of the Kane County Board in December 1985. It is governed by the Kane County Board of Health, which consists of all the members of the Kane County Board. Ongoing accountability to the Board of Health is
125 provided through the Health Committee, which is advised by an appointed advisory committee consisting of seven public members. The Personal Health Division of the Kane County Health Department provides community education on AIDS and sexually transmitted disease (STD) prevention and human sexuality. Personnel from the Personal Health Division and Planning Division were involved in the start-up of the TCN. The Kane County Health Department's support of teen health was evident from their Healthy Teens Initiative (1993-1997), which was funded in part by the Illinois Department of Public Health. This consortium was also committed to improving the delivery of health and social services to teens. The key contacts from both divisions of the Kane County Health Department included Uche Onwuta, I-Plan coordinator; Judy Zwart, nurse case manager; and Yvonne Pena, disease investigation specialist. The Kane County Health Department (1997) also issued a report on domestic violence in 1997 that further justified program development in violence prevention in Aurora and the county as a whole. Kane County was found to have a higher rate of violence compared to the surrounding counties of DeKalb, DuPage, and Kendall. The 1996 Kane County Criminal and Juvenile Justice Profile cited in the Kane County report shows the number of Violent Index offenses, which includes murder, criminal sexual assault, robbery, and aggravated assault reported to police, as increasing 8.0% in Kane County between 1993 and 1995. From 1993 to 1995, this 8.0% increase in the Violent Index represented a change from 513 to 552 offenses per 100,000 of the population in Kane County. At the same time, the Violent Index offense rate for surrounding counties decreased 19.0%, from 357 to 291 offenses per 100,000 of the population in these nearby counties. Violence, as presented in this Kane County (1997) report, was clearly on the
126 rise in Kane County when compared to its nearby counties. This preliminary needs assessment conducted by the Health Department also found that most community residents believed gangs to be the most prominent issue in Kane County. Most professionals surveyed reported domestic violence as the most pressing issue.
United Way of the Aurora Area The United Way supports various social service programs in the Aurora area through private contributions including the annual YWCA's "Week Without Violence" in late October. The United Way conducted a series of community-needs surveys to identify the key problems to be addressed in Aurora beginning in 1995. A July 1996 United Way Community Needs Study Team found that nearly 100 community leaders saw the most serious problems in Aurora to be gang activity (89.8%), crime (89.7%), drug abuse (75.6%) and teenage pregnancy (59.2%) (United Way of the Aurora Area, 1996). This pattern of concern related to gang and crime activity was consistent with findings from an earlier community needs assessment for Aurora (United Way of the Aurora Area, 1995). The United Way currently is involved in a Funders' Consortium that provides financial support to health care, mental health, education, and social service projects. The key person at the United Way is Arlyn Brower, executive director.
Kane County Region Office of Education #31
127 School Health and Safety Initiatives According to two recent annual reports from the Kane County Region Office of Education (ROE) (www.kane.k12.il.us), student safety and school security have become major concerns across the nation as well as in Illinois. Kane County ROE #31 has sponsored numerous related programs that have involved all nine school districts within its jurisdiction. Illinois State Board of Education (ISBE) support has helped fund several of the programs, and a "Regional School Safety Resource Center minigrant" provided $5,000 to support three workshops for principals interested in proactive school security planning. More than 500 Kane County school administrators, teachers, and professional support staff have attended classes in Crisis Management, School Survival 101, Second Step Violence Prevention Training, Aggression Replacement Training, Proactive School Security Planning, Encouraging Student Responsibility, and Social Skills and Antiviolence Curriculum during the last two school years.
Kane County Regional Safe Schools Program The Regional Safe Schools Program (RSSP) began with a planning and implementation grant in the school year 1996-1997. This program is a result of legislation providing programs for disruptive students who are eligible for suspension or expulsion. The Illinois Legislature appropriated $15 million for safe-schools programs. ROEs wrote program grants to access this money. These funds are renewable on an annual basis. Funds are used by Kane County to provide educational programs to disruptive students in a variety of ways. Districts #U-46, #129, #131, and #300 operate alternative-to-suspension programs. These programs keep students in school during the term of their suspensions.
128 During the 1997-98 school year, approximately 1,400 students were served in the Kane County RSSPs at 15 different sites. Seventy-four of these students were eligible for expulsion. In 1998-99, approximately 1,155 students were served in these programs. Seventy-six of these students were eligible for expulsion. Instead, they attended RSSP sites in their local districts. Eighty-nine percent of these students completed the program successfully in 1998 and 1999. Due to the RSSP activities, expulsions have been reduced by 50.0% in Kane County since the 1994-1995 school year. Suspensions were also reduced due to the alternative-to-suspension program at all 15 Kane County ROE-sponsored sites. The key contact with the Kane County ROE is Kim McLevain, social worker with the Safe School Program. Health Education in Aurora Public and Private Schools Local Aurora schools have been undergoing curriculum change in response to the needs of youth for accessible health information, early prevention interventions, and school-to-work transition programs. West Aurora School District #129 has offered a peer mentoring and mediation program as part of its Safe and Drug-Free Schools program for three years. Health education was expanded to be included for one quarter per year in grades 6-8 at the middle-school level in 1998-1999 for District #129 students. Freshman students are required to take one semester of health education at West Aurora High School. A three-year "school-within-a-school" Health Career Academy started in 1994-95 that serves 90 sophomore- through senior-level students interested in health occupations after high school. The key contacts at West Aurora District #129 include Carolyn Kerkla, assistant superintendent for instruction; Mary Hauge, head librarian; Miriam Wade-Hicks, social worker; and April Sonnefeld, health careers academy coordinator.
129 In the East Aurora School District #131, a character education curriculum for K-8 elementary students was developed in 1997-98 by a team of elementary teachers. High-school students, grades 9-12, are required to take one semester of health education to graduate. Students may also choose "health occupations" as an elective class in vocational education. The key contact with East Aurora High School is Olive Poliks, special needs guidance counselor. Rosary High School, a private Catholic girls high school, requires health education for sophomore students. Seniors may choose the class "Social Justice and Ethical Issues" as an elective. Rosary's school library has identified a need to update its materials collection in health, psychology, and human relations to support the school curriculum. Rosary's Drama Club performs a play on a health-related topic for upper elementary-school children during Spring semester every year. The key contact with Rosary High School is Sister Bernadette Marie McGuire, school librarian.
Public Libraries The public libraries of Aurora, Sugar Grove, and North Aurora serve the student population of the two Aurora school districts. The public libraries struggle financially to update their collections in many subject areas to support library services using the latest technologies available. As previous participants in the THINK project, the public libraries were familiar with the health-information needs of teens and their parents, and these public libraries were interested in expanding access to health information via the Internet. Key contacts at the public libraries include Betsy Tatar, Aurora Public Library science/AV/periodicals librarian; Beverly Holmes, Sugar Grove Public Library director; and Paul Murphy, Messenger Public Library of North Aurora director.
130
Aurora Online Community Network (AOCN) The Aurora Online Community Network (AOCN) operated from 1995 to 1997 at host institution Aurora University. The project was funded by the city of Aurora under Mayor David Pierce to promote the adoption of new Internet technologies throughout all sectors of the community and to support lifelong learning. Although the total project is no longer operating due to city of Aurora funding cuts, the web server at Aurora University continues to operate as a community information resource, hosting information for nonprofit, educational, and social-service organizations that need web hosting and e-mail services (Kolar, 1999). The key contacts at Aurora University include Dr. Thomas Zarle, president; Christopher Kolar, AOCN coordinator; and Dr. Susan Ross, School of Social Work.
Health-Care Providers
Dreyer Medical Clinic As a major provider of health-care services, Dreyer Medical Clinic (www. dreyermed.com) is dedicated to providing and making available the most progressive and cost-effective health care in the Fox Valley area. Dreyer's medical staff has over 115 physicians, with 106 of these physicians board-certified in 27 medical specialties. In addition to its medical staff, Dreyer support staff includes certified nurse/midwives, nurse practitioners, psychologists, social workers, and other allied health professionals. Dreyer physicians are affiliated with Provena Mercy Center; RushCopley Medical Center; Edward Hospital in Naperville, Illinois; and DelnorCommunity Hospital in Geneva, Illinois. Dreyer offers classes and programs on
131 wellness topics, support groups, prenatal classes, clinical trials, and a patient information line called Dreyer OnCall at 630-906-5004, with an audio library of health-information topics (Dreyer Medical Clinic, 2000). Key contacts at Dreyer Medical Clinic include Nancy Webb, RN; Dr. Phillip Jacobson, pediatrician; and Nancy Hopp, director of marketing.
Visiting Nurse Association (VNA) The Visiting Nurse Association (VNA) of the Fox Valley (www.vnafox valley.com) provides a variety of in-home and ambulatory health-care services throughout Kane County. The VNA supports new mothers and babies through the Healthy Families America initiative, a program intended to help first-time parents with the stresses of caring for a new baby. The program includes home visits, information on child development, and referrals to parent support groups and daycare providers. The VNA Health Center provides a WIC nutrition program for pregnant and breastfeeding women and their infants and small children who are determined to be at nutritional risk. A Women's Wellness Program provides annual preventive health exams and health education and promotion activities for women on a sliding fee schedule. Women's Wellness staff participate in the Truancy Alternative Program (TAP) offered at the Aurora YWCA to help teen mothers stay in school. The VNA also offers well-child and immunization clinics program to assure that children receive their necessary immunizations. The key contact at the VNA is Nancy Snider, RN.
Youth Services Agencies
132 Breaking Free, Inc./Family Support Center Breaking Free, Inc. (www.breakingfreeinc.org) is a private, not-for-profit behavioral health-care organization serving Chicago's western suburbs, including Aurora. Children and families are offered comprehensive family and communitybased prevention and counseling services with the goal of strengthening families and promoting healthy communities. In March 1998, the Family Support Center became part of Breaking Free, Inc., which expanded the organization into child abuse prevention and family-based services. In 1998, Breaking Free, Inc. received a grant from the Office of Juvenile Justice Department to identify needs and resources for youth to prevent juvenile delinquency in the city of Aurora. The Breaking Free, Inc. program incorporates the Character Counts! (www.charactercounts.org) core ethical values or "six pillars of character"--trustworthiness, respect, responsibility, fairness, caring, and citizenship-and has trained members of the Aurora Community Mobilization Advisory Board (ACMAB) and Aurora school teachers and administrators (Howrey, 1999b). Mayor David Stover and the Aurora Police department are supporting Character Counts! values as a crime prevention measure (Dardick, 1999). The key contact at Breaking Free, Inc., is Darnae Scales, community mobilization specialist. The key contact at the Family Support Center is Amy Stickler, programming coordinator.
Aurora Police Department, Juvenile Division The Aurora Police Department's Juvenile Division offers prevention education on drug use, domestic violence, and tobacco use to students and teachers in the Aurora schools. The DARE program reaches students in fifth grade about the pitfalls of drug use. The Aurora Police Department also offers a "drive-along" program for any
133 Aurora resident over the age of 16 who wants to learn about law enforcement work. The Police Department also has a program for the disposal of unwanted weapons or ammunition by Aurora citizens (Howrey, 1998a). The key contacts at the Aurora Police Department include Steve Wennmacher, head of Juvenile Division, and Diane Sanchez, DARE officer. Crisis Line, Association for Individual Development/Teen Talk Line The Association for Individual Development offers telephone crisis intervention through its crisis line service 24 hours per day, seven days per week, at 630482-9393. Volunteer counselors make referrals to community agencies as needed based on the caller's inquiry. The Teen Talk Line with teen counselors operates Friday, Saturday, and Sunday from 3-9 p.m. Kane County INFO, which began as a telephone and referral service for the Aurora United Way in 1974 and was a program of Community Contacts in Geneva, Illinois, became part of the Association for Individual Development's Crisis Line in 1997. INFO currently handles confidential Kane County information and referral and publishes of a number of countywide directories on social services and senior services. The Healthy Teens Handbook (Kane County INFO, 1994) continues to be updated based on caller inquiries and new programs for teens and parents as announced by area social service, education, and health-care agencies. A thorough screening process and 11-week training program with 80 hours spent on crisis intervention techniques is provided to volunteers who staff the 24-hour crisis hotline. The key contact at Kane County INFO/Crisis Line is Holly Cherry, INFO/Crisis Line coordinator.
Aurora Township Youth Services
134 The Aurora Township Youth Services has a free, extensive Community Outreach Program for youth ages 12-17 years old residing in the Aurora Township service area. Youth are referred to the program by the Aurora Police Department, Juvenile Judicial Court, or Department of Human Services. Services offered by Aurora Township include mentoring, advocacy, crisis intervention, support counseling, tutoring, recreation, and referral services. Other programs supported by Aurora Township Youth Services include youth employment, the Youth Center, Free Lunch Program, recreation, tutoring, Right Choices Summer Day Camp, public information and education, and community restitution (Howrey, 1999a). The key contacts at the Aurora Township Youth Services include Jeff Scull, director, and Kim McLevain.
Churches and Community Action The Aurora Area Clergy Association (AACA) is a voluntary association of clergy who serve in churches located in southern Kane and Kendall counties. The association represents over 200 ministers from all religious denominations. The AACA holds monthly networking meetings at Provena Mercy Center. The Prayer Coalition for Reconciliation, a church-related organization, was first started in 1994 by Reverend Dan Haas, pastor of Aurora Community Church, and Father David Engbarth, a Roman Catholic priest and pastor of St. Nicholas Church, to address violence in Aurora. The goal of the coalition is to "[denounce] violence by hosting vigils at the sites of violent death in the Aurora community" (Falcon & Nelson, 1998, p. A4). These community-serving clergy believe that the key to reducing violence is to bring religion to a group of people who desperately need guidance.
135 To foster cooperation among local ministers, Haas and Engbarth meet with interested area ministers in weekly prayer. Their ultimate goal is for Aurora's spiritual leaders to join the community's social movement against violence. According to Reverend Haas, however, the Prayer Coalition's efforts to date have not been as easy as it would appear--"It's something people acknowledge intellectually. But it's very hard to break out of your own circle (church congregation) and link hands with someone else. Unless you make time, it won't happen" (Falcon & Nelson, 1998, p. A4). In 1997, the Prayer Coalition held 27 vigils for victims of violence in Aurora (Roth, 1997). Key contacts from the Aurora church community include Sister Helen Schill, director of pastoral care, Provena Mercy Center; Reverend Harriet Cross, associate pastor, United Wesley Methodist Church; and Jonathan Switzer, youth minister, Aurora Community Church.
Images of 1994-1999 and Problem Definition
Personal Safety Concerns and Violence The THINK grant experience provided guidance and background information to Provena Mercy Center Medical Library and its potential community agency and library partners on teen health concerns and personal safety and on the status of teens' knowledge about the health-care system and resources available. The concerns of the original THINK library/community partners are reflected in this paragraph taken from the 1994 final grant proposal: Recent reports in the local Beacon News indicate that Aurora area teens are concerned about their personal safety and futures. Students at Cowherd Middle School recently commented that they were concerned about "not having a future at all" as a result of their fear of gang violence inside and outside of their school. Jefferson Middle School students indicated through a student survey that they feared gang violence. Stephanie Weber-Slepicka, director of the Crisis Line of the Fox Valley, recently commented that these circumstances may cause teens
136 to question their ability to solve problems and feel insignificant. . . . Teens are forgotten people. So little is expected of them that they feel a sense of purposeless. (Howrey, 1994, p. 3)
Teens Uninformed About Available Health and Social Services The Kane County Health Department's Healthy Teens Initiative also provided background information related to the knowledge level of teens concerning available health and social services. The November 1993 survey findings revealed that the majority of Kane County teens were unaware of resources at their disposal and identified a number of barriers for many teens in accessing available health and social services: Kane County teens are taking needless risks due to a lack of information about available health and social services. A Healthy Teens survey, conducted by the Kane County Health Department in November 1993, found that the vast majority of the 176 teens responding to the survey did not know specific agencies to go to for assistance. Barriers to use of services by teens mentioned most frequently included transportation, fear, "parents finding out," "don't know where to go," and cost. (Howrey, 1994, p. 3)
Aurora's Youthful Victims of Violence Remembered A series of tragic murders to Aurora youth occurred over a four-year period from 1994-1997. The city responded to these deaths by honoring its "fallen youth" through memorials and community action projects. When the new Aurora Community Center was dedicated on April 20, 1997, in the former Aurora Central Catholic High School building, pictures of Moshe Rogers and Armando Mendez adorned the walls of the gym. Located on Aurora's "rough-andtumble" east side, the pictures were placed in the Community Center to keep the memory of these murdered Aurora Central Catholic high-school students alive. In an
137 emotional ceremony, Mary Rogers stared up at a portrait of her slain son and expressed hope that her family's loss would provide inspiration to the children who pass under the painting: "When children see that mural, hopefully it will remind them of the value of life. Perhaps it will lead them to a better life" (Buchanan, 1997, p. 1). Elsa Mendez, Armando's sister, expressed some joy despite her grief as she observed the portrait of her brother in his Aurora Central football uniform: "It's a little light of hope for us" (Buchanan, 1997, p. 1). The stories of these Aurora murder victims are the basis for community mobilization efforts that followed. Armando Mendez, age 19, was confronted by several gang members on the evening of October 27, 1994, when his car ran out of gasoline about five blocks from his family's home on Aurora's east side. Believing Mendez to be the member of a rival gang, the group attacked the College of DuPage student, and one of the gang members shot him in the head. Mendez was on his way home from work at the Cracker Barrel restaurant in Naperville and was not in a gang when he was murdered (Buchanan, 1997). "The people that murdered him were strangers to him," said Mendez's brother Roberto. "He was in the wrong place at the wrong time. The guys who killed him probably did not even know his name" (Dardick, 1994, p. 5). On Friday, February 17, Moshe Rogers and Marchel Rogers, his younger brother, were driving home from Aurora Central Catholic High School after an away basketball game against Illiana Christian in Lansing, Illinois. As the boys began their drive home after leaving the team bus, they stopped a block away to offer a ride to Ramon Villa, a 14-year-old freshman at Aurora Central Catholic. A few moments later, at least one shot was fired from outside the car. The bullet struck Moshe Rogers in the head, causing him to lose control of the car and swerve into a nearby house. On Saturday night, Moshe was pronounced dead at Loyola University Medical Center
138 (Baniak, 1995). According to a later Chicago Tribune report, the killing of Moshe Rogers was tied to several weeks of shootings between rival gangs in the neighborhood and the fear created by the intense violence between the two gangs (Young, 1996). In response to the murder of Moshe Rogers, Mayor David Pierce noted that his death was tragic because there were no warning signs of the potential for danger to Rogers: "There is no question that we have had problems with violence and crime in this community," said Mayor David Pierce. "But in almost all of those cases, we had a clear indication that those people were involved in gangs or crime or other illegal acts. In this case, this young man was doing everything we ask our young people to do: a good student, a good athlete, a good son. That's what makes it especially tragic." (Baniak, 1995, p. 1) The family and friends of Moshe Rogers experienced his loss with great difficulty. They could not accept the shooting of a respected and talented athlete: Streamers of white tissue paper still danced in the wind from the branches of a tree in front of Moshe Rogers' house Monday morning. The paper had been strung through the branches three days before, a lighthearted prank by Rogers' friends at Aurora Central Catholic High School as they anticipated a victory in a high school basketball game Friday night. Over the weekend, in the aftermath of Rogers' shooting death on his way home from that game, his family just couldn't bring themselves to take the tribute down. "That was an act of love," said his older sister, Manisa. "It says a lot about his friends, about how he touched them. So we're going to let it stay there." (Baniak, 1995, p. 1) A final high-profile victim of violence in Aurora was Nicholas Contreras, a six-year old kindergarten student at Our Lady of Good Counsel school. Nico was murdered while sleeping overnight at his grandparents house on Aurora's east side: Nicholas Contreras was to have spent the afternoon Sunday celebrating his birthday with a couple dozen friends at Funway in Batavia. But the six-year-old's life ended early Sunday, when he was struck several times by gunfire as he slept at his grandparents' house in the 600 block of Aurora Avenue. He died immediately. Aurora police continue to investigate the slaying, which is the 25th in the city this year. (Falcon, 1996, p. 1) The Peacemaking and Antiviolence Movement in Aurora
139
In response to the rash of 81 killings in Aurora over the four-year period 19941997 described, a number of diverse community organizations and government agencies joined together to hold a series of peace conferences. Local news media reported on these Aurora peacemaking events in response to the wave of violence: To celebrate the peace in a city weary of gunfire, several of Aurora's leaders organized a musical prayer session Sunday in which African-American choirs, Latino singers, and white rock bands shared the stage of the Paramount Arts Centre. "We are a community in constant threat of gangs, drugs, and violence, a community in hiding, and we can no longer be indifferent to the deaths," said Elsa Mendez, sister of the slain student, Armando Mendez. "We want our community and neighborhood back." (Pelton, 1994, p. 1) With the memory of a record year for slayings still fresh, Aurora's municipal and social service agencies are coming together in an ambitious effort to stem violence. On Saturday [May 11, 1996], more than 100 residents, police officers, church leaders, and activists from organizations as diverse as the Boy Scouts and the Mutual Ground domestic violence shelter held the city's first "Peace Summit." (Bils, 1996a, p. 1) Lying in his casket Tuesday, six-year-old Nicholas Contreras looked like a child sleeping peacefully. All around him, a community was waking up. Even before the body of the outgoing and well-liked boy known as "Nico" was laid in a grave, plans were being made: a community prayer vigil, more intense neighborhood patrols, a program to reach out to troubled children in school. Aurora has been down this path before. Last year in February [1995], the shooting death of Moshe Rogers, 17, a promising high-school basketball and track star, galvanized the city and helped spark widespread community involvement. Now, after the death of Nico--who was killed early Sunday when someone shot through a window into the bedroom where he was sleeping--some see the movement renewing itself. (Bils, 1996b, p. 1) Spokesman for the Prayer Coalition for Reconciliation believed the murder of young Nico Contreras was a critical incident for Aurora, just as the murder of Moshe Rogers had been: "We will see this [murder of Nico] as a kind of second wakeup call, just as the death of Moshe Rogers was," said Reverend David Engbarth. "Our challenge now here in Aurora is not to give in to despair. We want to raise a strong, moral voice against this insanity." (Bils, 1996b, p. 1) And through community mobilization efforts involving the city of Aurora and local social service, health, and educational agencies, hope-inspiring programs got
140 underway. Aurora Community Mobilization Advisory Board (ACMAB) ACMAB reflects a joint effort of the city of Aurora, Aurora Police Department and about three dozen civic and social leaders. The group is dedicated to unifying the social service and antiviolence efforts among organizations in the city. Dr. Thomas Zarle, advisory board president, is retired president of Aurora University. The group is organized into three committees: human relations (developing the city's diversity as a strength), prevention, and suppression. Each committee meets separately and is developing its own sense of direction and structure and is in the process of setting action plans (Falcon & Nelson, 1998). According to Dr. Zarle, the board is focused on finding ways to triumph over violence--"You can see the excitement. There's a sense of readiness here. We think it's fixable (the city's violence problem), and we're not being naïve about it" (Falcon & Nelson, 1998, p. A4).
Project Unity Project Unity was organized in 1995 as a volunteer effort supported by the city of Aurora in response to the murder of Moshe Rogers. Concerned community members and the Rogers family wanted to find a way to assist needy children and their families in supporting school attendance and in improving the quality of life through information and education. The Back to School Fair was initiated in 1996 to provide free school supplies and free or reduced immunizations, dental and eye examinations. Supplies are bought from money donated by local churches, agencies, and businesses. Free health care has been provided by the VNA of the Fox Valley. In its first two years of operation, 4,000
141 lower income students were reached. In 1998, Project Unity's school fair won first place in the Governor's Home Town Awards youth project category (Dardick, 1998). According to one of its chief organizers, Diane Picciuolo-Jackson, "Project Unity is a thought you can't really measure. It's trying to get the community to unite for the same causes . . . to start volunteering and participating to make a change" (Sherlock, 1995, p. 3). Illinois Agencies Dedicated to Violence Prevention and Education In understanding the violence prevention movement in Aurora, key Illinois agencies were identified as resources for local programs under development. The following organizations are located in Chicago and are knowledgeable about statewide violence prevention programs. The following three agencies provide support to local communities through the loan and exchange of educational materials and resources, professional networking opportunities, grant programs, youth development, and educational outreach programs: Illinois Center for Violence Prevention (www.violenceprevention.com), Illinois Violence Prevention Authority (www.ivpa.org), and the Prevention Resource Center (www.prevention. org). Critical Decisions and Direction Setting from a Participant-Observer There were a series of critical decisions that needed to be made to develop the TCN as a Provena Mercy Center-endorsed project in Fall 1997. Because I was working collaboratively with DLS and West Aurora High School and could assume the role of grant writer (a role I had assumed for Aurora Public Library in 1994 for the THINK LSCA project), Virginia Koch, director of education, and Kathryn Stewart,
142 vice president for human resources, encouraged me to hold focus-group meetings and invite local agencies from a database I had compiled of health and social service agencies serving the Aurora school districts. It was clear to me that Provena Mercy Center supported a yet-to-be-defined LSTA grant and understood such a project would be library-driven, communityfocused, and resource-based. This was an unusual strategy for a community hospital. But the hospital was ready to employ the latest Internet technologies to reach the entire Aurora community with quality CHI resources. The Provena Mercy Center administration supported the provision of nontechnical, authoritative health information available in English and Spanish for the Aurora population on a website. The administration also believed that Provena Mercy Center's medical librarian was qualified to help make this technological leap happen for the hospital and local Aurora community. Stakeholder agencies were invited to two focus-group meetings in October and November 1997 to discuss the important teen health concerns for Aurora students. The results of these meetings were summarized and shared with the Provena Mercy Center administration. To further justify a decision on the grant's focus, I conducted a literature search on teen health needs. I discovered com-munity needs reports had been prepared by the United Way in 1995 and 1996, so I requested these from Arlyn Brower at the United Way to comprehend more fully the local Aurora picture. Beacon News articles were reviewed, local school administrators and youth service professionals were contacted by phone, and Provena Mercy Center health care professionals were questioned about hospital services delivered to adolescents to determine health-information priorities for teens and parents. The THINK grant survey results were dusted off and revisited from three years earlier to identify
143 "unfinished business" from the previous Aurora Public Library THINK grant experience. Questions I asked myself covered all options: "Should we be focusing on teen moms and babies?" "What about teen sexuality and abstinence as issues of importance?" "Is community violence still an important issue for Aurora residents and teens in particular?" As I struggled with defining the key teen health concerns and the writing of an LSTA grant, Sister Margaret Mary Knittel, Provena Mercy Center's grants writer, and Lynn Elam at DLS challenged me to consider both the human and technological issues involved in the project. "Who would host the website?" "Would we hire a consultant to actually construct the website?" "What information would we place on the site?" "How would we encourage use of the site?" "What other agencies should be invited to join?" "How could we encourage involvement once agencies became a partner?" "Should we make WICs available for all the potential library partners who have the space?" As I interacted with more agencies and talked with professionals at Provena Mercy Center, schools, youth service agencies, public libraries, and government agencies, the issues became clearer to me. On New Year's Day, January 1, 1998, an article in the Beacon News, part of a series on the year in review, discussed the quiet peace movement underway in our Aurora community (Falcon & Nelson, 1998). The article discussed the work of the Prayer Coalition for Reconciliation and the Aurora Community Mobilization Advisory Board and their concerns about community violence and planning efforts to reduce the violence. The hopeful and healing peace efforts of these local clergy and educators struck me as significant. "Could I somehow help?" I thought and questioned, "Should peacemaking and nonviolence be the focus
144 of the LSTA grant? Was student safety, community fear of violence, and a hopeful attitude toward solving the problem the vision I was seeking?" The image of the new Provena Mercy Center logo struck me--a dove holding an olive branch in its beak. "Wasn't this the answer I was seeking?" "Didn't Provena Mercy Center envision building a community of healing and hope?" "Wasn't a website for teens and parents supporting this new expanded mission of community service and outreach?" Problem Setting: Teen Health Concerns and Focus Groups Identifying teen health concerns and identifying health-information needs had been an important part of the health-information delivery improvement process for the THINK project. Books, videos, and related media were selected, and community health education programs arranged by Aurora Public Library were acquired and developed based on the results of a needs survey. A total of 889 students were surveyed in November 1994 for the THINK project about the sources students sought for health information (parents, mass media, doctors, teachers, school nurses, or counselors), health topics of interest, information formats preferred (books, pamphlets, speakers, computers, magazines, etc.), and equipment available in their homes (VCR, computer, and modem). An overview and summary of the total THINK project activities are found in the article written by Kuzel and Erickson (1995). To launch the TCN, I reviewed the THINK Teen Health Survey with permission of the coauthors and compared the Teen Health Survey with several other instruments developed for assessment of adolescent health concerns (Fisher, 1992; Weiler et al., 1993). Based on the results of my investigations, a shorter Teen Health Concerns rating sheet was developed and used with the health care, social service, and education professionals serving adolescents who attended one of the two focus-group
145 meetings. The TCN's Teen Health Concerns checklist is found in Appendix E. Table 2 summarizes the responses of focus-group participants to the Teen Health Concerns survey distributed at two focus-group meetings. The top five ranked teen health concerns of the 12 professionals responding to the Teen Health Concerns checklist were alcohol abuse, teen pregnancy, personal safety, substance abuse, and violence. The results of the Teen Health Concerns survey led me, as the LSTA grant writer, and members of the steering committee to reflect on the need for a comprehensive tool to measure the actual health behaviors of teens in Aurora. I conducted a literature search and located the YRBS from the CDC. Because this tool was used across the country and would allow benchmark comparisons, I assumed the data gathered would be important in further defining the mission and objectives of the TCN. Problem Setting: Monitoring of Risk Behaviors and Needs Analysis in Aurora To measure and reduce the risk behaviors of American youth, the CDC designed the YRBS in 1988. The YRBS project has evolved over time to measure six categories of priority health-risk behaviors among youth and young adults. The reliability of the YRBS over time has been established by Brener, Collins, Kann,
146 Table 2 Professionals' Ratings of Teen Health Concerns, 1997
Teen Health Concern
Mean Rank
Total N
Mode Score
Alcohol abuse
1.00
12
1
Teen pregnancy
1.00
12
1
Personal safety
1.08
12
1
Substance abuse (marijuana, cocaine, etc.)
1.08
12
1
Violence
1.09
11
1
Sexuality
1.17
12
1
Emotional distress
1.34
12
1
Relationships with others
1.34
12
1
Alienation (feeling out of hte stream of the school culture)
1.50
12
1, 2
Suicide
1.50
12
1, 2
Anger management
1.58
12
1
Body image
1.58
12
2
Child abuse and neglect
1.58
12
1, 2
Self-esteem
1.58
12
2
Cigarette smoking
1.75
12
1, 2
Parent-child communication and bonding
1.75
12
1, 2
Prejudice toward others
1.75
12
1, 2
Student achievement and success
1.82
11
2
Knowledge of community resources
1.92
12
1
Nutrition and dieting
1.92
12
2
Reckless autombile driving
2.00
12
2
Exercise and personal fitness
2.17
12
2
Contributing to the community
2.34
12
2
Health care network access
2.34
12
2
147 Warren, and Williams (1995). First implemented nationally in the spring of 1991, the YRBS monitors: 1. behaviors that contribute to unintentional and intentional injuries, 2. tobacco use, 3. alcohol and other drug use, 4. sexual behaviors that contribute to unintended pregnancy and STDs (including HIV infection), 5. unhealthy dietary behaviors, and 6. physical inactivity. The YRBS data is used to measure progress toward achieving 21 national health objectives from Healthy People 2000 (U.S. Public Health Service, 1995) and Goal 7 of the 8 National Education Goals Panel (1995), which covers safe, disciplined, and drug-free schools. The system is also used to support state and local policies and programs to reduce health risk behaviors among youth (Kolbe et al., 1993). Use of the YRBS data for problem identification and program evaluation is a key part of a public health approach to violence prevention according to Hamburg (1998), a physician with the New York City Department of Health. Dryfoos (1998) employed key 1995 YRBS survey data results to build her case for current high risk behaviors among youth and the key role parents play in ensuring "safe passage" of their offspring from adolescence into healthy, productive adulthood. Using the YRBS questionnaire allowed the TCN to draw comparisons between Aurora youth and the national sample for health-information program planning purposes. As the steering committee and Provena Mercy Center staff reviewed the YRBS, I agreed that several questions needed to be modified and questions added to the Aurora Schools YRBS on media preferences, health decision making, and empathy
148 toward others. I located questions on decision making, problem solving, and empathy in the literature and adapted questions on health information and health problem solving from inventories developed by Baker and Roberts (1989), Bryant (1982), and Heppner (1988). Needs Analysis: The 1998 Aurora Youth Risk Behaviors Findings In February 1998, the modified Aurora Schools YRBS questionnaire and administration protocol were submitted by me to the NIU Institutional Review Board (IRB). Due to the nature of the questions asked, the IRB required that a parental consent letter be added to the protocol before final approval was given to the research project. As project director, I sent building principals a letter of introduction to TCN and background on the YRBS in late April 1998. By late May 1998, the IRB approved the revised YRBS questionnaire administration procedures, and librarians and health and physical-education teachers were provided with the survey, scantron forms, parent consent forms, pencils and administration instructions (see Appendix A for copies of the letter of introduction, final questionnaire, and administration instructions and Appendix B for the informed consent form).
Final Convenience Sample Characteristics The final sample of students who responded to the Aurora Schools YRBS questions in May/June 1998 is a convenience sample of students drawn from physical education and health classes at East Aurora High School, West Aurora High School, and Rosary High School. The distribution of students responding to the Aurora Schools YRBS is presented in Table 3, with the sample broken down
149 Table 3 Aurora Schools YRBS Respondents, May 1998 Demographic
Number
Percentage
Year in School Eighth grade
5
1.0
408
81.3
Sophomore
54
10.8
Junior
21
4.2
Senior
14
2.8
Total
502
100.0
Female
311
62.3
Male
188
37.7
Total
499
100.0
White
300
59.9
Black
69
13.7
Hispanic
99
19.8
Other
33
6.6
Total
501
100.0
Freshman
Gender
Race
150 by school, gender, and race. The 502 students represent students who answered the YRBS in a consistent and valid manner. Students with an out-of-range response rate of 5.0% or higher were eliminated from the final YRBS data set. Table 4 shows the final distribution of the responding freshmen to the YRBS. There was a total of 508 usable surveys from the freshmen at East Aurora, Rosary, and West Aurora High Schools. West Aurora freshmen were heavily represented in the final sample of freshmen--69.6% of the freshmen responding were from West Aurora High School. As a result of the low response rate from East Aurora High School, the YRBS results are not representative of Aurora high school students as a whole. East Aurora High School students, who are likely to have the greatest concerns about school and community safety, are not well represented in the final sample. Therefore, the YRBS results do not report the total East Aurora freshmen student body concerns about school safety or the availability of guns and weapons. Table 5 shows the distribution of the YRBS respondents for the freshman class only. Because 1997 national YRBS data for freshmen was published by CDC and readily available for comparisons, the researcher and TCN steering committee members concluded that the Aurora data could be limited to the largest segment of respondents, freshmen students at all three participating Aurora high schools. Table 4 illustrates that the final convenience sample of responding freshmen had a high percentage of West Aurora and female students, which increased the likelihood of favorable responses to questions about violence occurring within the school and family settings. The results reported in Table 5 reflect the convenience sample bias. When results for Aurora are compared to the national YRBS results from 1997, as the TCN steering committee decided to gain an understanding of the
151 Table 4 Aurora Schools YRBS Freshman Profile, May 1998 Demographic
Total N
Percentage
School East Aurora High School
41
10.0
Rosary High School
83
20.3
West Aurora High School
284
69.6
Total
408
100.0
14 years old
86
21.1
15 years old
298
73.0
16 years old
24
5.9
408
100.0
Female
257
63.0
Male
150
36.9
1
0.2
408
100.0
White
256
62.7
Black
48
11.8
Hispanic/Latino
78
19.1
7
1.7
18
4.4
1
0.2
408
100.0
Yes
49
12.1
No
357
87.5
Total
408
100.0
Age
Total Gender
Not indicated Total Race/Ethnicity
Asian/Pacific Other Not indicated Total Free Lunch Program Participation
Table 5
152 Table 5 cont.
153 severity of Aurora youth risk behaviors, Aurora compares favorably with results from the U.S. as a whole and with Chicago. Selected results of the Aurora Schools Risk Behavior Survey (May/June 1998) are compared with the national U.S. data in Table 5. Table 5 reports responses to YRBS questions covering interpersonal violence and suicide. Percentages are shown for Aurora freshmen, Chicago youth, U.S. freshmen, the total U.S. sample for 1997, and the 1995 Illinois results for freshmen and the total high-school sample. Wiley, James, Furney, and Jordan-Belver (1997) took a similar approach in comparing Texas high-school and college students on selected health behaviors. As shown in Table 5, of the 430 Aurora freshmen students responding to the YRBS question, "During the past 30 days, how many days did you not go to school because you felt you would be unsafe at school or on your way to or from school?," 5.6% (N = 23) reported they had stayed home from school as a result of feeling unsafe at school or when traveling back and forth to school. In comparison, only 4.0% of the total U.S. 1997 sample reported this behavior. Of the 501 students responding to the question, "During the past 12 months, how many times has someone stolen or deliberately damaged your property such as your car, clothing, or books on school property?", 38.2% (N = 191) reported loss or damage at least once during the past 12 months. In contrast, 32.6% of the total U.S. high-school student sample for 1997 reported lost or damaged property on school grounds at least one time. Overall, the data in Table 5 illustrates for the convenience sample of responding Aurora freshmen that violence is not as critical a problem as the steering committee concluded from the results of the THINK survey conducted in 1994-1995 and the United Way surveys compiled in 1995 and 1996. As a result of
154 this contradiction with earlier data and the poor response from East Aurora students, the steering committee concluded that the Aurora YRBS data, although useful, could not be used solely to govern the TCN's violence prevention planning and program implementation. Needs Analysis: Health-Information Problem Solving Table 6 presents the results of Aurora teen responses to the question, "Which one of the following strategies do you normally use to gain an understanding of your personal health and wellness?" Of the 485 teens responding to this question, 153 or 31.5% indicated they did not seek out health information, 82 or 16.9% indicated they obtained information from a friend, 71 or 14.6% indicated a parent or doctor provided information, 71 or 14.6% indicated that books or magazines were a primary source of information, and 52 or 10.7% reported that they viewed videos or television to obtain health information. As shown in Table 6, the Internet was reported by only seven teens or 1.4% as a source of health information normally used. These findings suggest that teens require guidance and role modeling from parents, teachers, and health-care professionals in both seeking out health information and using the Internet as a primary resource for knowledge about their own health and wellness. Table 7 reports the Aurora teen problem-solving strategies identified in June 1998 as typical responses to a health problem. Of 468 teens responding to this question, 164 or 35.0% first talked with someone, 124 or 26.5% contemplated the problem on their own, 87 or 18.6% tried to calm down first, and 54 or 10.8% reacted with anger. Only 21 or 4.5% of the teens indicated they would seek out information as a first response to a health problem. Table 8 addresses the issue of perceived effectiveness in dealing with a
155 Table 6 Aurora Teen Health Information Seeking, June 1998 Seeks information from... N Doesn't seek out information
% 153
31.5
TV or videos
52
10.7
Friends
82
16.9
Parents or doctor
71
14.6
Teacher, high-school counselor
18
3.7
Books or magazines
71
14.6
Cassette tape
2
0.4
Internet
7
1.4
29
5.9
485
100.0
Educational programs Total
Table 7 Aurora Teen Problem-Solving Strategies, June 1998 When confronted with a health problem, the teens selected this as their first response: N
%
Try to calm down
87
18.6
Talk with someone
164
35.0
Think on my own
124
26.5
React with anger
54
10.8
Solve quickly/regret later
18
3.8
Seek information
21
4.5
468
100.0
Total
Table 8
156 Teen Perceptions of Effectivenss in Dealing with Medical or Health Emergencies, June 1998 I am usually pretty effective in dealing with medical and personal health emergencies. N
%
Strongly agree
147
36.3
Agree
147
36.3
Slightly agree
71
17.5
Slightly disagree
20
4.9
Moderately disagree
11
2.7
9
2.2
405
100.0
Strongly disagree Total
medical or health emergency. Aurora teens were asked the extent of agreement or disagreement with the statement, "I am usually pretty effective in dealing with medical and personal health emergencies." Of the 468 Aurora teens responding to this question, 147 or 36.3% strongly agreed with statement, 147 or 36.3% agreed with the statement, and 71 or 17.5% slightly agreed with the statement. A total of 40 teens or 9.8% of the respondents disagreed with the statement concerning their effectiveness in dealing with medical and personal health emergencies. Table 9 summarizes Aurora teen responses to the statement, "I usually feel sorry for other people when they are having health or personal problems." This statement reflects the level of empathy for others experiencing a health problem. Of the 443 teens responding to this statement, 254 or 57.3% strongly agreed with the statement, 106 or 23.9% moderately agreed with the statement, and 50 or 11.3% slightly agreed with the statement. A total of 28 teens or 7.5% disagreed with this statement, so a relatively small percentage of the Aurora teens as found
157 Table 9 Aurora Teen Empathy Toward Others With a Health or Personal Problem, June 1998 I usually feel sorry for other people when they are having health or personal problems. N
%
Strongly agree
254
57.3
Moderately
106
23.9
Slightly agree
50
11.3
Slightly disagree
18
4.1
5
1.1
10
2.3
443
100.0
Moderately disagree Strongly disagree Total
through the YRBS survey experience a lack of empathy for others with health or personal problems. Needs Analysis: Media Preferences of Aurora Teens Table 10 provides a rating of the preferred media by Aurora teens in obtaining health information. Television and videos were rated by 309 teens or 64.1% of respondents as either very valuable or valuable. Books were ranked second highest among the teens--287 or 60.3% rated books as either very valuable or valuable. Magazines were ranked slightly below books as a favorite medium--288 teens or 59.9% of those responding rated magazines as either very valuable or valuable as a source of health information. Computer programs and the Internet were rated as very valuable or valuable by 253 or 52.3% of the teens responding to the question. Finally, pamphlets were the least favorite medium of teens for health information, with only
158 201 or 41.5% rating pamphlets as very valuable or valuable. Computer programs and the Internet and pamphlets also had a large percentage of teens (14.9%) (N = 75) rating these media as having "No value for me." Table 10 Aurora Teen Media Preferences, June 1998 Media Rated Valuable or Very Valuable by Teens Media
N
Total Respondents
%
TV/videos
309
482
64.1
Books
287
476
60.3
Magazines/newspapers
288
481
59.9
Computer programs/Internet
253
484
52.3
Pamphlets
201
484
41.5
Direction Setting: The Root Causes of Violence and Responses to Violence On June 19-20, 1998, TCN sponsored two workshops to bring a hopeful message of peacemaking and nonviolence to teens, parents, and the professionals serving Aurora's youth. Jim and Kathy McGinnis (1998), influential peace educators and activists with the Institute for Peace and Justice, presented background information to nearly 90 participants in the one and a half days of training. The training session content is captured in three videos produced by Video Perfection, Aurora, Illinois, for the TCN's lending library collection, and the workshops were important in the laying the groundwork for the TCN agenda in 1998-1999 (McGinnis & McGinnis, 1998). In his introduction to community peacemaking, Jim McGinnis quoted from the "Declaration of Peace" compiled in 1997 by 30-40 Aurora citizens involved in the
159 Prayer Coalition for Reconciliation. The four root causes of violence in contemporary society, as identified by the Prayer Coalition in its "Declaration of Peace," are as follows: (1) the absence of a moral structure leading to a loss of vision and hopelessness; (2) the disintegration of family structures and the loss of a sense of community; (3) the breakdown of the criminal justice system; and (4) the increased presence of social and economic injustice (McGinnis & McGinnis, 1998). McGinnis presented the image of "circles of safety, love, and peace" to the workshop participants (McGinnis & McGinnis, 1998). He explained that the circles have been broken in America and have contributed to more youth feeling "alienated from the rest of society" (McGinnis & McGinnis, 1998). The four root causes found in the Prayer Coalition's "Declaration of Peace" provide a logical explanation on how these circles have been broken. Youth coming from frag-mented families and lacking a stable set of values or "moral vision" feel "disempowered" and "uncared for" and lash out for attention through violent behavior both within and outside the family. McGinnis believed it is the responsibility of adults in a community to remember the vision of a better society and "the common good" and bring back disenfranchised youth "into the safe circle of love and peace" we all expect (McGinnis & McGinnis, 1998). This task is especially difficult in today's American society because we have a history and culture of violence that is evident in the mass media. Professional sports, music, television, video games, and films have all become increasingly violent because violence "sells." McGinnis claimed that the "cycle of violence" and safety issues must be addressed on both a personal level and on an institutional/societal level for significant change to occur (McGinnis & McGinnis, 1998). McGinnis noted that responses to violence are based on how the problem is
160 diagnosed, and our responses to violence need to be realistic, given the scope of the problem. Suggestions offered by McGinnis and McGinnis (1998) for dealing with violence in the community include (a) creating feelings of solidarity with the victims of violence through unity rallies and support groups; (b) living and modeling the alternative to violence through the "Family Pledge of Nonviolence;" (c) building coalitions of concerned citizens and government officials at the local level and offering services to those in need; (d) influencing national social policy and advocating for legislation (such as gun control); and (e) keeping a sense of balance and wholeness through art, crafts, games, music, meditation, and nature (McGinnis, Lovingood, Lovingood, & Vogt, 1996). Positive and hopeful responses to the violence are crucial for the youth we want to nurture-- "Let's make our lives a witness to the society we want to create. Let's walk the talk" (McGinnis & McGinnis, 1998). Summary of Needs Analysis Findings and Direction-Setting Process The descriptive findings presented in this chapter on actual Aurora youth risk behaviors and the root causes of violence point to these needed improvements in the delivery of health information to Aurora teens and their parents: 1. Training to promote health information as a basic problem-solving tool for teens and parents, with health information provided through a variety of media including the Internet and pamphlets; 2. Programs to reduce the theft of personal property in Aurora high schools and to enhance school safety to reduce student fears about violence when traveling back and forth to school and during the school day; 3. Programs to enhance the character of Aurora youth to respond effec-tively and proactively to incidents of community, school, and family violence;
161 4. Programs to enhance parent-teen communication and to reinforce effective parenting practices and role-modeling; and 5. Establishment of an Internet site to make the Healthy Teens Handbook (Kane County INFO, 1994) and authoritative health-information resources accessible to teens and parents for effective problem solving and the identification of local health and social services on demand.
TCN Chronology and AR Process Selected aspects of the problem-setting and direction-setting phases of Gray's (1989) collaborative process model have been covered in this chapter for the TCN library/community agency partnership. The implementation phase of the project involved collaborative planning by the project director with the steering committee and Provena Mercy Center's administration for the website infrastructure and content, library partner collection development activities, health education programming, and media blitz and began in March 1998. Partners committed time and energy to the planning process and implementation of TCN services and products. The key activities in the implementation phase are listed in the chronology found in Appendix D and sample pages from the final TCN website are found in Appendix H. These events can also be depicted in terms of the AR process, which was described in Chapter 3. Table 11 provides one example of the AR process applied to TCN website development (http://www.aurora.il.us/teencare) over the 18-month grant project This matrix is based on the Queens University, Kingston, Ontario, model of AR reporting as found on the Queens University College of Education website at .
162 Table 11
163 Table 11 continued
164 Table 11 cont.
165 The findings summarized in Table 11 illustrate the key roles assumed by Provena Mercy Center, Aurora University, Sugar Grove Public Library, AID Crisis Line/INFO, and Breaking Free, Inc., in the website development. As the project director interacted with the representatives of these partner agencies, breakthroughs occurred; the commitment of space on Aurora University's webserver for the TCN website, the decision to use MicroSoft (MS) Frontpage software as the standard website development package, the contribution of Healthy Teens Handbook (Kane County INFO, 1994) as content for the website, the sharing of marketing expertise and programming between the partner agencies, and the willingness to seek additional funding sources proved critical to the maintenance of the organization as a learning organization and professional networking group. The next chapter covers these beneficial aspects of the TCN as described by the partners in the Partnering Behaviors Survey and through exit interviews. Partner views on the overall effectiveness of the grant project and partnership is assessed using two checklists found in the literature review: Alter and Hage (1993) and Mattessich and Monsey (1992).
CHAPTER 5 FINDINGS: PARTNERING BEHAVIORS AND PARTNERSHIP EFFECTIVENESS
Partnership Themes This chapter presents findings related to the effectiveness of the TCN grant project. Data was gathered to measure the partnership effectiveness using (a) the results of the Partnership Behaviors Survey, (b) TCN partner exit interview responses, (c) program evaluation responses, and (d) collection development and use comments. Appendices C, F, and G have copies of the instruments used to gather partnership evaluation data over the 18-month grant project. In this chapter, the voices of the partners are revealed in interview statements, open-ended evaluation survey comments, and meeting minutes. The secondary data sources, survey results, and exit interviews are analyzed to provide insight into these main themes: 1. the partner commitment and expansion of the membership, 2. the perceived mutual benefits of the partnership, 3. the coordinating structures established to monitor improvements, 4. project outcomes (website development, website use, other products, and services of the Internet TCN website developed), 5. perceived partnership barriers or obstacles, 6. the future vision for the partnership, 7. overall effectiveness and partnership impact, and 8. sustaining the partnership. The last section of this chapter evaluates the TCN partnership using the two
167 models from Alter and Hage (1993) and Mattesich and Monsey (1992). The TCN experience is assessed in terms of goals achieved, system resources acquired, internal processes, and constituencies. Finally, the partnership is assessed in terms of the 19 success factors identified in the literature review conducted by Mattessich and Monsey (1992). Partner Commitment and Expansion of the Membership As Sullivan (1998) noted, partnerships are characterized by a strong commitment to the professional welfare of the collaborating partners and involve four principles: mutuality, involvement, clarity, and reciprocity. A colloborative relationship involves mutual goals and benefits, a jointly developed structure and shared responsibility, action-minded follow-up, mutual authority and accountability for success, and the sharing of resources and rewards (Gardner, 1991; Mattessich & Monsey, 1992). To facilitate frequent communication, TCN established a steering committee as a forum for the development of mutual goals, joint program planning, and the sharing of resources for improved teen and parent access to health information. The TCN steering committee met formally on a monthly basis for the first two years of the partnership. To join the TCN, organizations were asked to submit a letter of support, which involved a commitment of staff time and the sharing of ideas and expertise through the steering committee. Because the purpose of the TCN steering committee was to serve as a forum for joint planning and information exchange about youth services programs offered in the Aurora area, TCN became the primary professional networking group in Kane County to focus on teen health and youth services. As one partner explained our
168 group's purpose in an exit interview, "We're target-specific to teens." Because the steering committee was conceived as a working committee, the frequency of meetings was often increased when partnership community education programs were approaching and program planning details needed to be ironed out and finalized. Derived from TCN steering committee minutes, Table 12 documents the agencies in attendance at these meetings and the frequency of attendance for the twoyear period. When an agency had two representatives present, the two individuals were counted independently. Based solely on the attendance figures as presented in Table 12, the partner agencies who were highly involved in the TCN (attending 10 or more meetings) include--West Aurora School District #129, Provena Mercy Center, East Aurora School District #131, Rosary High School, Breaking Free/Family Support Center, Dreyer Medical Clinic, and the Kane County Health Department (N = 7). The public library partners DLS, Kane County Region Office of Education, and Crisis Line/INFO fall into the moderately involved partner group, with attendance at 5-9 meetings (N = 7). The next group of agencies (N = 5) was somewhat involved in the partnership. The largest number of partners (N = 17) falls into the marginally involved category, a category based solely on meeting attendance that does not reflect the influence wielded by various community agencies. The actual level of commitment of partner agencies to TCN (i.e., willingness to collaborate) is revealed in the programs developed and sharing of resources by a number of key Aurora agencies serving youth. For example, the YWCA provided leadership in violence prevention programming through its Week Without Violence activities and public relations efforts. The TCN partners were invited to plan YWCA activities, participate on specific days highlighting school
169 Table 12 Frequency of TCN Meeting Attendance by Agency, November 1997-October 1999
Commitment Highly involved (7 agencies)
Moderately involved (7 agencies)
Somewhat involved (5 agencies)
Agency in Attendance
Total in Attendance
West Aurora School District #129
29
Provena Mercy Center Library
23
Provena Mercy Center (other departments)
23
East Aurora School District #131
21
Rosary High School Library
14
Breaking Free/Family Support Center
12
Dreyer Clinic
10
Kane County Health Department
10
Messenger Public Library of North Aurora
9
Batavia Public Library
7
Crisis Line/INFO, Association for Individual Development
7
Aurora Public Library
6
Dupage Library System
6
Sugar Grove Public Library
6
Kane County REO
5
Aunt Martha Youth Services
4
Visiting Nurse Association of the Fox Valley
4
Aurora Police Department
3
Aurora Township Youth Services
3
YWCA
3
(continued on following page)
170 Table 12 (continued) Marginally involved (17 agencies)
TOTAL present at meetings
Aurora Central Catholic High School
2
Aurora Community Church
2
Batavia High School Library
2
Fox Valley Girl Scout Council
2
Kane County Juvenile Justice Department (SHOCAP)
2
Marmion Academy
2
Wesley United Methodist Church
2
Aurora University
1
Cities in Schools
1
Family Counseling Service
1
Fox Valley Park District
1
Greater DuPage MYM
1
HOUSE (Home schoolers)
1
Illinois State Library
1
KDK Job Training and Employment Services
1
New England Congregational Church
1
Quad County Urban League
1 229
171 violence prevention, display a "Peace Sheet" at the YWCA building, publicize the TCN website and special events through the Beacon News to teens and parents, and receive financial support from the Aurora Exchange Club for TCN programs based on the YWCA executive director's recommendation. A second example of collaboration was the Fox Valley Park District sponsorship of the Safe Night USA program for Aurora middle schoolers in June and October 1999. Over 100 middle-school youth attended these two conferences and heard speakers discuss self-esteem and violence-prevention topics. Several TCN partners spoke to youth at the Safe Night USA conferences about the "School Pledge of Nonviolence," self-confidence, and goal setting (Project Snowball). A final example of an agency "minimally involved" in TCN meetings but a key player in community violence-prevention activities was Aurora University. With the help of Aurora University, the TCN's website was provided a "home" on the Internet and several new partner agencies joined as a result of referrals made by Aurora University's president, Thomas Zarle, chairman of the Aurora Community Mobilization Advisory Board. Clearly, meeting attendance revealed only part of the picture of TCN partner commitment. Based on the responses of 20 partners to the Partnering Behaviors Survey, it is clear that those organizations responding perceived a high level of commitment among partner agencies to youth development and "making a difference" in the Aurora community. In response to the statements, "We shared a commitment to our TCN mission and goals" and "We believed in making a difference in providing health information to Aurora area teens and their parents," 70.0% of the partners strongly agreed with these two statements and 30.0% agreed with the two statements concerning the commitment of partners to the mission, goals, and improvements in
172 health-information delivery. One of the partners noted in an exit interview that many of the TCN partners are over-extended but willing to collaborate: Everybody in the Teen CARE Network is from some poor agency who's already got more jobs than they can handle. And for them to want to be involved in the Teen CARE Network, I think, first of all, shows a real commitment. Commitment to our community. Commitment to wanting to help kids. Over the course of the 18-month grant project, the initial group of 15 partners who submitted letters of support for the TCN's LSTA grant application in January 1998 expanded to 40 members by September 30, 1999. According to the final reports of the LSTA grant project, the growth in the membership was tied to the visibility of the partnership through community health education programs offered, mailings of three newsletters, the TCN website, bookmarks, membership brochures, a "Peace Sheets" exhibit, a statewide library teleconference, cable television interviews, a cartoon contest, community resource fair booths, conference presentations, announcements about the partnership at monthly Aurora Community Resource Team meetings, news media coverage in Provena Mercy Center's external "Centerscope" and "CenterPage," and articles in the Beacon News, Kane County Chronicle, and Chicago Tribune (Howrey, 1998d, 1999c). Expansion of the partnership was gradual, and increases in membership occurred as outreach efforts "got the word out" about community education programs and the professional networking opportunities at TCN meetings. Appendix D contains the timeline for the major TCN project activities based on the Gray (1989) partnership development model. The chronology in Appendix D shows that in January 1998, the TCN partnership had 15 initial members. This number expanded to 23 partners by September 1998. In November 1998, the partnership totaled 25 member agencies. By January 1999, the first anniversary of the partnership, membership totaled 30
173 members, which represented a 100.0% increase from the initial membership. By the end of the grant activities, September 30, 1999, the membership totaled 40 partners (see Appendix I for a list of the partners). The overall growth in the partnership over the 18-month grant period was 25 new partners for a 167.0% increase in membership. In commenting on the success of the partnership, Steve Wennmacher, head of the Aurora Police Department Juvenile Division, commented that I measure it [success] by the simple fact that when I read the minutes, I see more people involved. To me, you get more people involved, you'll have a successful program because you'll have more opportunities for people to discuss things and more people to turn to. The more people you have as a resource, the better off the organization's going to be. The more resources you get, the more you can push people in the right direction. Holly Cherry, Kane County INFO/Crisis Line coordinator, noted the library roots of the partnership and the clear sense of outreach to other sectors of the community that brought more agencies into the fold: "The Teen CARE Network really mushroomed; it started small, with just some librarians, and it got bigger, bigger, and bigger. It was a wonderful experience in coming together as a community and reaching out to all different agencies and organizations." As reported by several partners in exit interviews, the membership expansion reflects the clear mission communicated inside the hospital as lead agency and to prospective members of the new library/community agency partnership about teen and parent health-information needs and violence. For Provena Mercy Center Hospital, there was conscious-raising that resulted from involvement with the librarycommunity agency project, as Sister Margaret Mary Knittel reported, There has been a certain conscious-raising occurring in the hospital relative to needs I think have always been there, but we feel we can be more a part of now. There are all these pieces out there, trying more and more to reach into the community.
174 Breaking Free, Inc., and Darnae Scales joined the partnership because of the visible outreach activities and clear partnership mission: What brought us to the Teen CARE Network? Actually, it was your outreach, you know, through your newsletters, and we read them, and we thought that your mission fit so well with our mission that we wanted to get on board. When new groups, committees, or new organizations form, and I think many times for a good reason, they just don't want to start out with a focus, with a vision. They take their time as far as providing a service to the community. Mostly, it seems like that first year is just about dialogue and what we should do. But the Teen CARE Network seemed to have that vision already and was off and running and provided resources and something tangible that you can use. According to Virginia Koch, former director of education at Provena Mercy Center, teen input was sought early in the partnership's participatory planning process: "It was very much a partnership from the very beginning with these organizations . . . with the schools and the survey that was done . . . to get input from the students themselves as to where their health care interests were." Several partners interviewed noted the timeliness of the partnership's school violence focus, a focus that resulted from listening to Aurora youth and responding proactively to national events: We were really "ahead of the ballgame," so to speak, in thinking to address those [school violence] issues because of what the kids had told us. . . . The focus that this particular project took and what the results of the needs assessment showed would be to focus on violence and prevention with families and children. It certainly turned out to be something that was very prophetic with the things that happened around the nation shortly afterwards. When you look back on it now, it is something that really was extremely timely, and the community had a focus early on of what the needs are in this particular area and wanting to place strong focus in this particular area. I think it's wonderful that this particular project helped, was already in place before some of the tragic events [of school violence] happened around the country. This shows . . . we weren't reactive but proactive in our own community in already recognizing the dangers that young people are in related to the violence, personally themselves and in their family. I do think, from that aspect, it was quite interesting that this was the focus of this particular project. Finally, Olive Poliks, counselor at East Aurora High School, noted that the partnership drew in people concerned about youth and willing to make a personal
175 sacrifice in helping kids: "I think people involved in the Teen CARE Network are caring people; what is the quality they all have? They really care about people. Why would they come out at the end of a hard day, they already have all these other committees?"
Perceived Mutual Benefits Learning Organization and Professional Networking A key benefit seen by TCN agencies was the opportunity to broaden knowledge of teen health-information needs and other community agencies. The partnership functioned as a learning organization and networking group for its members and fostered a sense of appreciation for the diverse perspectives and working styles of agencies serving youth. Olive Poliks, East Aurora High School guidance counselor, commented on the opportunities for professional growth and empowerment through resources acquired to better serve teens: It's been a wonderful learning and growing experience for me professionally. The resources we've gotten at [our high school] are terrific and very much appreciated and well used. I've been able to encourage other schools in [our district] to participate, and the Teen CARE Network has been a wonderful opportunity for our librarians to be empowered. I think the real heart of it [the Teen CARE Network] is the opportunity to network with other people. I think that's a real important part, but they've got to have something in their [teen's] hands. They have to have something besides a website number, tell me something I'm going to get that I couldn't get by reading on the website. What you [the project director] got was very unique, and all those little pamphlets are readable, they're easy; it's not like they're high-tech, complicated things. Lynn Elam, programming director with DLS, believed the partnership
176 provided avenues for understanding teen health and safety needs and for interaction with a variety of community agencies: Certainly we became more aware of the needs of teens in terms of health and safety. So that was a learning experience for us, and I think that's an area we need to continue to develop and work on. We were able to meet and work with a variety of agencies that are outside the scope of our normal activity. So that certainly was a benefit. Listening to concerns that those agencies work with every day and the way they do their own problem solving was very interesting and enlightening, and I think that all of us can borrow from each other's perspectives and do better work than what we do now. It was certainly a broadening and expansion of horizons for us, and a pleasure to get outside of the library community and work with other agencies. Holly Cherry, Kane County INFO/Crisis Line coordinator, believed that the TCN built closer connections between her agency and librarians: It [the TCN] was not only a networking group for me, it was an opportunity, I thought, to see what more librarians felt they could do for teens. That was kind of cool! I see the Teen CARE Network as not only a networking group but a working group. I think it's a benefit to be more closely connected with all the people you work with. Beverly Holmes, director at Sugar Grove Public Library, believed that the group contributed to better service for her library customers, broke down barriers, and fostered a sense of appreciation of the contributions of different community agencies and the public library she administered: The partnership has been made available for us to serve our patrons in a far better way. We're better informed about some of their needs, we've got materials and avenues for information to help them address those issues that they're facing. At least within the library community, we interact on different levels for different reasons with the school groups and all. And knowing somebody and being involved on a committee with somebody in one avenue helps sort of break that barrier for another avenue. You can call them for another reason, then, and it's very helpful. I've seen the partnership in almost two different ways. First of all has been the personto-person contact that I have been able to experience with the other working members of the partnership--that face-to-face sharing of information. Little incidental things that come up where you begin to realize, more and more, you appreciate a greater understanding of what those other agencies are doing. The same way they appreciate a little bit of what you're doing and some of the things you're up against.
177
Mary Hauge, head librarian at West Aurora High School, discovered that she became more aware of teen health concerns as a direct benefit of the TCN partnership activities. Amazement at the use of health-related materials by teens acquired through the grant is apparent in Mary Hauge's comments: Certainly, an awareness of health problems. You mean, you think of kids as . . . a fairly healthy bunch, and not . . . needing a tremendous amount of health material. But it seemed like . . . the more we got, the more they used! Besides the material resources, the ideas that people bring and getting to know people face-to-face is a real benefit. Nancy Prichard, head of Adult Services at Batavia Public Library, found that she became better acquainted with professionals in health care and safety organizations: I think it's a great networking experience. I never would have met some of these people otherwise, simply because I am in Batavia and don't get to know the organizations that would deal with some of my patrons from the Aurora and North Aurora communities otherwise. As far as networking, it's an excellent way to meet people in the health-care and safety organizations like the police department. Holly Cherry with Kane County INFO/Crisis Line commented on the benefits of discovering new youth services agencies and programs in the community through the TCN: Being a part of the Teen CARE Network is also very advantageous to me because I'm able to hear what new programs are out there, what people are doing, what new things are developing, if there's a new agency coming along, or something like that. All of that stuff! Just knowing what's going on with people who work with teens is really a big benefit for me. Carolyn Kerkla, assistant superintendent for instruction with West Aurora School District #129, sensed the positive connections being made between the diverse professionals in attendance at TCN steering committee meetings: I think the networking that went on--those meetings that I was able to attend and listen to groups of people. I loved to see "ahhhs" from the educators to the librarians to the health-care providers, back to the educators. And those are just so refreshing and so encouraging when they see there really are connections out
178 there that can be made. Harriet Cross, associate pastor at Wesley United Methodist Church, believed that the TCN facilitated her service to the community as a mentor and problem solver for families of different backgrounds: For myself, I think it's important to serve as a community mentor. The second reason [for joining the partnership] was in terms of being able to help. I feel like, actually, social issues really don't have economic boundaries. Sometimes a well-off family is not willing to admit that they might have the same social problems [as a low-income family]. Finally, Dr. Geraldine Holub, clinical psychologist, observed that the partnership was very much needed, given the fact that individual family members are unlikely to tackle the culture of violence on their own: I think the network aspect [of the TCN] is the thing that is attractive to me. The fact that schools, police, probation, mental health, hospitals, etc., can all work on the problems simultaneously. That's what it's going to take--no agency, institution, or individual can solve this alone. And the parent or individual family members are not going to do anything about the culture of violence that we live in. These exit interview comments are further reinforced from responses to the Partnering Behaviors Survey. Partners ranked these behaviors as among the highest in the TCN partnership--(a) found opportunities and empowered each other (85.0% strongly agreed or agreed), (b) solved problems creatively and sought opportunities and encouraged others to do so (80.0% strongly agreed or agreed), and (c) honest about our strengths and weaknesses and interacted effectively with one another (90.0% strongly agreed or agreed). Resources for New Programs and Resource Dependency A second important benefit was the support offered to youth service professionals by librarians through the website and learning resources acquired
179 through the grant. Kim McLevain, a social worker with the Kane County ROE, noted the strengths of the TCN in supporting her programming activities with at-risk youth. The new materials acquired under the grant and the website were seen as valuable for prevention initiatives at her agency: You have the much-needed resources that are hard to come by--either hard to locate or not enough funds to purchase--that we can just use here for free [at Provena Mercy Center Library]. And then the Internet access is great--a great place to find much needed resources. In the field of prevention, you're always looking for something, and money is scarce. Beverly Holmes, director of Sugar Grove Public Llibrary, stressed that each partnership member contributed its own resources, which made the partnership more effective: As individual agencies coming into a partnership, we all had our own resources to draw on and our own strengths and weaknesses. And the good thing about a partnership is that you can really seek to even those out and offer up a quality package even though some of your members aren't as strong as others. Olive Poliks, East Aurora High School guidance counselor, reported on the value of the WIC added at her building for parents and teens in crisis: When we had parent conferences in the gym, we wheeled out the Teen CARE Wellness Information Center display to the gym lobby where report cards were being distributed. It was a hit! Many of the students were attracted to the display and took advantage of all the literature. In addition, the parents were impressed to see all the information available to their teens. A student came to me in crisis. She was pregnant and being kicked out of her house. I was so glad to have literature to give her and resources to help her make decisions at this critical time in her life. The resources acquired under the grant were seen as an important incentive for agency participation. Resource dependency theory explains why Olive Poliks, guidance counselor, joined the partnership: People have to feel, "I'm going there [to meetings] because I'm going to get something." That isn't a selfish thing; I don't think it's a selfish thing. I think that's a practical thing. Every person there is very busy doing 24 jobs at the same time. Every person has tremendous demands made on their time. If they're going to take on one more job, one more commitment to meet regularly
180 or support some kind of activity, they have to say, "I'm going to bring something back to my agency that's going to say, `Your time is worth it'." That's what happened at the Teen CARE Network--everybody got all these wonderful materials, so of course they wanted to come, of course they wanted to support you. It isn't a selfish thing. I think it's just simply being practical. People are only going to be involved in something where they have something to walk away from it. Carolyn Kerkla, assistant superintendent for Instruction with West Aurora School District #129, saw the human resources and mentoring relationships as an essential element of the TCN partnership: [Our school district] is very proactive in seeking partnerships with outside organizations, with members of the community, with organizations in the community. I know the Health Academy teachers have made great strides with their inroads in the hospitals in the area. We've got kids that are jobshadowing, we've got kids that are being mentored by people at the hospitals and really capitalizing on those relationships. Resources were described in relation to directly helping abused students in crisis by Olive Poliks when she was working at Waldo Middle School as their guidance counselor: I've seen kids who have graduated to the next level of abuse. When they were at middle school, their father was abusing them, and now their boyfriend is abusing them. I need resources; I think the teachers perhaps feel the same way. It's a sense of not hopelessness but helplessness. I want to do something for you, I see you need help. Can I give you something? Can I give you a resource, a pamphlet, a name [for a referral], or something? And I think the materials the Teen CARE Network gave us are so good, really valuable. Just to be able to put something in the kids' or the parents' hands and say, "Here's some more information about that topic." It's a wonderful, nonthreatening way to be helpful. Kim McLevain with the Kane County ROE also stressed the importance of all types of resources for her prevention work with at-risk families and youth: Well, providing resources they need--that would depend on each family. Some families might just need money. It depends on the family. Providing alternative activities, providing education and literature enhancing the awareness of the problem. The more information you can get to them [youth and parents] about issues relating to prevention--it doesn't have to only be gangs.
181 Steve Wennmacher with the Aurora Police Department's Juvenile Division supported the availability of city ordinances on the TCN's website to further extend his ability to help teens and parents by increasing access to laws that affect them: Sometimes we have to spread ourselves so thin that we have a hard time getting everywhere [meetings, special events]. And I want everybody to understand if they have a question about the police department to call. If I don't get it to you today, I'll find out. That's why I think it's a good idea to put the city ordinances on the Internet. I think that's a great idea. It's right there for people to look at.
Coordinating Structures Alter and Hage (1993) discussed the nature of coordination as it applies to social service networks. The primary objective of coordination is "to obtain the resources and expertise necessary to produce needed outcomes" (p. 83). From this perspective, coordination is effective if it maximizes the functioning of a system to ensure that the services offered to clients are comprehensive, accessible, and compatible with client needs. Were all necessary resources and services present in the TCN and available to the teens and parents who needed them? The following coordinating structures were established in the TCN partnership to ensure that all necessary resources and services present in the network were available to teens and parents in the Aurora community: (a) a lead agency and project director, (b) mission and vision, (c) goals, (d) formalization and group facilitation, and (e) marketing of partnership products and services.
A Lead Agency and Project Director In exit interviews, two Provena Mercy Center administrators commented on the crucial role assumed by the hospital in initiating and coordinating the project.
182 Virginia Koch, then director of education at Provena Mercy Center, saw the TCN as another avenue to reach into the community with health information: In 1997, we had a strong component in our Provena Mercy Center Education Department of community outreach and providing community education programs. So it was under that particular aspect of the program that we wanted to look for ways to further pursue outreach in the community--and have an impact on the movement toward wellness and prevention health care education in the community. Also, we wanted to look for ways to partner with other organizations and be able to disseminate health-care information in the community. . . . And the expansion . . . of the access to information technology and being able to disseminate educational information in new ways to people were things we were interested in. That was our impetus for getting involved with this [grant project] and looking for ways we could have outreach. Sean Waite, vice president for Support Services at Provena Mercy Center, assumed responsibility for monitoring the TCN grant in December 1998. Provena Mercy Center Library's coordinating role in the grant project was clear: Our role has . . . been the driving partner in . . . overseeing it [the TCN]. We acquired the grants for that, our staff was involved in making sure the monies were accounted for, meetings were attended, and mailings went out from here. Really, it [Provena Mercy Center] was a coordinating body, definitely in the beginning and then through the second year of the program as well. As medical librarian at Provena Mercy Center, I assumed the position of project director when the grant was officially awarded in March 1998. This new parttime position was written into the grant to maintain and build key contacts with Aurora libraries and community agencies. Virginia Koch, former director of education at Provena Mercy Center, described how the project mushroomed as a result of my network of key contacts in the library field and with Aurora commu-nity agencies: I think much of the success of being able to align those partnerships [the TCN members] were from contacts you had made through the years. You made it look very easy! But from a few seeds of contacts, you were able to make that [the partnership] mushroom and grow. And it's one of those things where you can start out with a few and then it grows into something that people are interested in and want to support.
183 Holly Cherry, Kane County INFO coordinator, noted that the previous THINK grant stimulated her participation in the TCN project initiated by Provena Mercy Center: It was just natural when the Teen CARE Network came about--we were also involved in THINK before that. . . . We knew that was something that had started up, and we participated in it, at least for a while, while it was going. I know it [THINK] was fairly short-lived, but we thought that was a good thing to have available to be able to get more resources out there. And it's our philosophy really to join into anything in the area that enhances being able to get the information to people who need it. Beverly Holmes, Sugar Grove Public Library director, also believed that the previous THINK grant experience gave the TCN LSTA project a solid foundation for a quicker start-up: The THINK grant allowed us to put so many new materials into our collection, and I really don't think the Teen CARE Network would have taken off the same way if we hadn't already have broached that topic. If we hadn't addressed the health issues, done the survey in the high schools, and found out that their [teen] needs were really rather more than personal health issues that truly went to some personal safety issues.
Mission and Vision The mission and vision of the TCN as identified in the final LSTA grant proposal presented by Howrey (1998b) to the Provena Mercy Center administrative team was as follows: An Aurora library/community agency partnership committed to action, respect, and excellence (CARE) with the purpose-• To improve access to health-information resources in all formats • For 12,000 teens and their parents • With an emphasis on nonviolence and peacemaking • Conveniently found in Aurora homes, schools and the community at large • With the vision of Aurora as a "community of healing and hope." This vision and mission statement was consistently communicated in newsletters, at steering committee meetings, in press releases, in the membership
184 brochure developed and through the "Family Pledge of Nonviolence" adopted by the partnership on its bookmark. The clarity of the vision and mission communicated to the Aurora community is reflected in these written comments from Darnae Scales, community mobilization specialist with Breaking Free, Inc., in response to a question about effective partnering among TCN agencies-You [the TCN project director] are actually partnering and not just talking about it! Your greatest strength is your ability to create synergy by accurately assessing and communicating how TCN's mission, vision, and goals complement and enhance the mission, vision, and goals of agencies/organizations, teens, and families in our community. In an exit interview, Olive Poliks, East Aurora High School school guidance counselor, pointed to the mission of the TCN in noting that community pride underlies partner involvement: I think people want to say, "I don't want the violence anymore. I want the violence to stop." This is the problem with kids; they say, "Violence is bad for everybody else but me--I can go beat somebody up." So maybe that's what the Teen CARE Network's about--people who want to make a difference in other people's lives, and they can do it in one form or another. It seems like it's easiest to say, "Here, let me hand you a pamphlet," but it's really much more complicated than that. I think a lot of it is pride in our community and wanting to make our community better. This is my town. I want to clean it up. I don't want to live this way.
Goals The Teen CARE Network defined five goals and measurable objectives over the course of the 18-month grant. The final report of the Teen CARE Network summarized the partnership goals: 1. Build and expand the partnership from its current membership to 25 active partners; 2. Develop an Aurora Teen Health and Wellness Internet website; 3. Collaborate with local news media and heighten the visibility of the Teen CARE Network through a "media blitz";
185 4. Acquire materials in a variety of formats in both English and Spanish to be shared and housed among Teen CARE Network partners; [and] 5. Develop mentoring behaviors critical to violence prevention and peacemaking for teens, parents, and Teen CARE Network partners. (Howrey, 1999c, pp. 11-12) These five goals were consistent with the Illinois State Library's long-range goals for partnership development, the literature on effective health promotion strategies, and CHI trends for just-in-time delivery via the Web. These goals also reflected the concern of the partners for increasing local media efforts to promote the new services developed for teens and parents. These goals highlight the importance assigned to proactive and reflective mentoring of youth toward peacemaking and nonviolent behaviors.
Formalization and Group Facilitation Process Because the TCN took on the character of an informal and fluid profes-sional networking and support group, there was a conscious attempt to keep the amount of formalized policies and procedures to a minimum. The partnership maintained minutes of meetings, issued a newsletter to highlight partner activities and upcoming programs, and developed policies and forms to guarantee equity of partner access to resources acquired through the LSTA grant project. For example, a policy was developed over the course of six months to loan the two Sony still digital cameras and one Cannon ZR digital video camera to partners (see Appendix J for a copy of the final digital camera policy and loan agreement form approved by the steering committee). This digital camera loan policy was the only policy created for TCN agencies over the 18-months of the grant. A TCN order card form was also designed for library partners to request materials with LSTA grant funds. Provena Mercy Center Medical Library staff were
186 responsible for placing orders with vendors and for compiling the annotated bibliography using the order cards for items received. The intent of formalization was to promote communication among the partners and prospective partners, to increase operations efficiency, and to maintain a record of activities to meet LSTA grant reporting requirements. The following exit interview comments from Steve Wennmacher, head of the Aurora Police Department's Juvenile Division, suggest that TCN newsletters and minutes did function to communicate partnership initiatives, did keep "less active" partners connected to the organization in spite of busy work schedules, and made program information readily accessible to teens and parents: When we [the TCN] first started, I was impressed with the amount of people who came out to help. When we started there were--what?--10 or 12 of us? Ten or 12, and we're sitting around the table, not knowing what we were going to do. Now, there's a newsletter. I think that's great! And I like the newsletter. I look at the minutes, and another Juvenile Division officer and I both read them. We read the minutes all the time. If there's anything that really impresses me, it's the simple fact that it [the steering committee] went from 9 to 10 people who sat in that room to as many people as are involved now. I think that's great. When you have an organization that encompasses everybody, I think that's even better. Any time you can get information out to kids and parents, it's great, no matter what the information is--whether 90% of them use it or not, we've got it out there. It's available. It's something they didn't have before. And you're showing that there are people out there willing to take an extra step to help make their lives better. I think that's important to some of these kids. I think it's a pat on the back to some of these kids, set them on the straight, right direction. Someone out there who's interested in what they're doing. Based on these comments from an experienced Aurora police officer, the TCN's printed publications have communicated the mission and concerns of the TCN partner agencies to Aurora teens and their parents. And, the TCN partner diversity has grown over time as a result of outreach through its formal, printed publications. Responses from the Partnering Behaviors Survey also support the value of the minutes, newsletters, and other printed publications. For example, the highest ranked
187 partnering behavior noted by 90.0% of the responding partners was, "We kept one another informed throughout via scheduled meeting times, regular mailings, e-mail, and telephone." In spite of the formalization of communications, group facilitation was handled informally and found to be effective in steering committee meetings. As reported by TCN partners, these group facilitation behaviors ranked in the top five behaviors exhibited: (2) "We listened actively to one another's viewpoints;" (3) "We shared information about the partnership with those we served and actively marketed TCN services;" (4) "We created an environment of openness and trust for all involved;" and (5) "We recognized and celebrated our successes." Areas for improvement are reflected in the lower ranking assigned to these partnership operating principles taken from the Partnering Behaviors Survey: (17) "We established realistic time lines to accomplish our tasks;" (18) "We communicated throughout the process;" (19) "We evaluated the results we achieved in our services and programs offered;" (20) "We used a variety of diagnostic techniques (focus groups, checklists, interviews, needs assessments);" and (21) "We established checkpoints to monitor our progress."
Marketing of the Partnership An advantage of the TCN partnership was that there were multiple marketing channels and public relations activities employed to increase the visibility of the grant project. These activities were directed to the professional library community and the Aurora community. Even the Illinois State Library got involved in marketing the project by adding the TCN site to its list of "Grants You Wish You Thought of" (http://www.sos.state.il.us/isl/grants/wish/990311.htm).
188 DLS, as a partner in the LSTA grant project, actively marketed the partnership through the DLS website link, continuing education programs, and a statewide teleconference on March 17, 1999. As Lynn Elam, DLS programming director, noted in an exit interview, other state of Illinois library systems recognized the TCN as an effective LSTA project: We did a lot of public relations . . . that was one of the easy things! To me, it didn't seem that important. We linked the Teen CARE Network website to our own DLS website. We promoted it [the TCN website] as the Site of the Month. We promoted it in our printed newsletters, and everywhere we had an opportunity to talk about it and promote it, we did that. We included it in our continuing education offerings so that if a DLS instructor or consultant were doing Internet training, we always included that site as one that people should be aware of and look at. So we did do some promotion. . . . We did a teleconference around the state, and I think the concept was very good. There was some good interest from around the state. I think the consultants from the other [library systems] recognized that this was a good project. In recounting the early phase of the partnership, Virginia Koch, former director of education at Provena Mercy Center, described the multiple communication channels used in the TCN project to market the community health education programs and services offered through the partnership: There was very, very strong communication . . . and meetings in the schools, regular monthly meetings, and in addition to that, newsletters also being sent that helped to spread the word in the community, press releases, opportunities to come in and see exhibits--so high visibility and high communication around what the program was all about and what it hoped to accomplish. And also setting up a web page for people to have access to the community resources. A system was put in place to share health resources and materials throughout the community. Beverly Holmes, Sugar Grove Public Library director, commented on the effectiveness of TCN marketing and the response of her patrons to her appearance on the Fox Valley Today cable television interview show: I think the message was out there. The project did have the cable TV exposure with the interview show [Fox Valley Today] that some of the members participated in. I know that generated a lot of interest because I was on the show, and I heard a lot of people say how . . . they had seen me. You know, one channel out of so many in a cable environment. It's hard to imagine that so many
189 people you know would see a show. That one instance, that one time, that one time and place. It was pretty neat. Nancy Webb, a registered nurse at Dreyer Medical Clinic, suggested that the TCN approach high-ranking government officials to increase the partnership's visibility in the community and make it as well known as the DARE program in making a difference in the lives of Aurora youth: You need to capture key people in the community. I know you've brought in the YWCA, and that's wonderful. You know, you visualize the mayor wearing a Teen CARE Network t-shirt, and the fire chief, and the police chief. Who knows? Chris Lauzen--people like that who are state representatives and so forth. You need that kind of visibility--big time. Have a Teen CARE Network Day in Aurora or something similar! There is no reason again with repetition, word-of-mouth, constant awareness publicizing, talking about it [the TCN] that this can't be the same thing [like the DARE program], that it can be a vital link to the community. But I think, more important . . . is the people involved in it that will make the difference. It's making that move, it's role-modeling, it's information, and it's hope--we're talking a lot of kids who don't have a lot of hope in their lives for whatever reason. And they can be exposed to these kind of things, and hopefully, it will make a difference. Clearly, this experienced nurse and community activist had spent time reflecting about the possible range of TCN services and their impact on "making a difference" in the lives of teens.
Project Outcomes The major TCN project outcomes and results included (a) the development of a website, (b) materials and equipment acquired for local libraries, (c) community health education programs, and (d) other partnership products and services.
Website Development The TCN's website design evolved over an eight-month period, January 1998
190 through August 1998. After discussions with a number of Web development experts, including staff from Aurora University, DLS, and Integrated Technical Solutions, Inc., in Naperville, Illinois, the decision was made to adopt MS Frontpage 98 as the standard software for development of the TCN website. The Aurora University AOCN web server supported Microsoft extensions, so this permitted electronic publishing of the TCN's MS Frontpage website. The TCN project director assumed the responsibility for using MS Frontpage 98 and for training grant personnel in its use. A support contract was signed with Integrated Technical Solutions, Inc., to assist with advanced software features, navigation aids, and shortcuts. Discussions at steering committee meetings about the website design focused on the importance of having key contacts identified at each library for improved communication with website users. The idea for an "Ask-A-Librarian" program originated at the steering committee's March 13, 1998, meeting. This National Library Week program was seen as a means of encouraging librarians to think of themselves as "case managers" (Provena Mercy Center Library, 1998a). After a meeting in late March 1998 between the TCN project director and the director of Sugar Grove Public Library, a draft TCN site "mind map" was presented to the steering committee at the April 3, 1998, meeting (see Figure 7). At the April 3rd steering committee meeting, the project director reported that the AOCN coordinator had provided a URL for the website (see Appendix H). E-mail addresses for all the library partners were verified for the upcoming National Library Week promotion, Ask-A-Librarian, held from April 19-25, 1998. The important elements of the website presented in Figure 7 and agreed upon by the steering committee included (a) the TCN partnership mission, (b) a listing of the partner agencies with links to existing agency websites, (c) the Healthy Teens
191 Handbook (Kane County INFO, 1994), (d) peacemaking and violence prevention sites, (e) free health-information sites, (f) local teen service opportunities and success stories, (g) TCN resources acquired, (h) Aurora Schools Youth Risk Behaviors assessment data, and (i) the Ask-A-Librarian gateway. Agencies from the social service, education, and library communities endorsed the Internet as a way of facilitating access by teens to valuable health information resources:
192
Figure 7. TCN Website, 1998-99
193 We thought, in working with the Teen CARE Network, there might be a chance of being able to at least distribute the information [the Healthy Teens Handbook and Teen Talk Line phone number] in some way. So when we began to talk about having a website, it seemed . . . that was a very natural way to be able to plug into modern technology and be able to put it [the Healthy Teens Handbook] on the Web. Teens are really into computers and have access through school now and public libraries. . . . So I saw it as a way to really be able to expand again out knowledge distribution and just be a benefit for the teens and for me also. I think that the [steering] committee was real realistic in its approach to how best to reach students. I think they also tried to make use of the technology that was available at the time that might not have been there 10 years ago. I think that the surveys have brought some attention to students and given the schools fodder for discussion and some information as to where they might take certain things like the health program and the counseling program and some other programs that have been put in place. So it's providing some valuable information via the [health risk behavior] surveys and via the Internet sites. In June and July 1998, Donna Spanos, an Aurora University master's degree program social-work intern, assisted with entering the Healthy Teens Handbook (Kane County INFO, 1994) updates provided by the Crisis Line/INFO coordinator. Sections of the handbook were verified for accuracy by Crisis Line/INFO staff, and higher priority sections were entered first by grant personnel at Provena Mercy Center Library. The TCN project director also pulled together peacemaking and nonviolence sites located during her investigations into important programs and organizations advertised on the Internet. This new section on peacemaking and nonviolence Internet sites had not been a feature of the 1994-1995 print handbook edition. The Health Reference Center Academic Version, an online subscription service with full text of health-related articles and pamphlets from Information Access Corporation, was also added as a link to the TCN site in June 1998 (Provena Mercy Center Library, 1998b). The grant paid the costs for the license with Information Access Corporation. Several of the school librarians in attendance at the July 20th steering committee meeting commented that use of the Health Reference Center
194 "would increase once the schools were in full session in September" (Provena Mercy Center Library, 1998b, p. 2). At the July 20th steering committee meeting, a form was distributed for TCN agencies to complete in order to be listed on the website. Agencies with websites and e-mail addresses were encouraged to submit the form for easy communication with teens, parents, and youth service professionals (Provena Mercy Center Library, 1998b, p. 2).
Website Use In a September 1998 steering committee meeting, several public library directors suggested that "the Teen CARE Network site be registered free with Internet search engines such as Yahoo and Excite to increase the number of `hits' on the site" (Provena Mercy Center Library, 1998c, p. 2). The site was quickly registered with Yahoo, Excite, Infoseek, and Lycos in September 1998 and immediate increases in "hits" occurred; the site counter on the homepage jumped from just 25 hits in August to 115 hits in September 1998. In October 1998, we were able to determine the referring sites by reviewing the WebTrends reports generated by Aurora University. In commenting on the value of the TCN's new website, Beverly Holmes, public library director, noted, I can go to the Web site, and I can say, "I know of these other places, and here they are!" They [patrons] can print that information and take it home for themselves. . . . I didn't always have that opportunity with the [printed] handbooks, if I didn't have enough available. I can show them to the website, and I can explain that those things are there for them. . . . My patrons are coming out of the computer room happy and satisfied, and I know that I've shown them good places to go, so I'm hoping that they found what they really do need. After discussions with several librarians about creating an "electronic community" among the partners, Aurora University was approached about setting up a
195 listserv. In June 1999, Aurora University created the TCN's electronic mailing list at
[email protected]. In an exit interview, Mary Hauge, head librarian at West Aurora High School, expressed her hope that the listserv would stimulate youth service agencies adding Internet access to their offices so that an electronic youth services community would be established in Aurora: A listserv is a great idea, but what worries me is that some of the agencies don't have Internet access and e-mail. This is a great way to talk to one another--a channel of communication--for building an electronic community. Maybe the Teen CARE Network website will "wake up" these agencies to the possibilities of a supporting community on the Web. TCN use statistics are presented in Table 13. The figures were generated from the WebTrends provided online to the partnership by Christopher Kolar, AOCN volunteer coordinator. The available use data is summarized for the TCN website (www.aurora.il.us/teencare) for 1998-1999. The TCN website had a total of 3,384 users sessions for the nine months of WebTrends reports available. The average number of user sessions per month for the TCN website was 376 between October 1998 and October 1999. The highest use months for the TCN website were (in order from high to low) March 1999, April 1999, October 1999, and May 1999. Typically, March and October are the heaviest months for library research and interlibrary loan activity. The traffic patterns for the TCN website are consistent with general library use patterns. Table 13 also reports the pattern of new versus returning users to the TCN site. The WebTrends data shows a total of 1,795 users for seven months of reported use. Of these 1,795 website unique users, 1,141 or 63.6% were new users and 654 or 36.4% were repeat users. Approximately one out of every three users return to the TCN website, based on the data gathered by WebTrends. Table 14 provides use data for the Health Reference Center section of the
196 Table 13 TCN Website Usage, 1998-1999
Month
Number of User Sessions
Page Views
Hits for Entire Site
New Users
Returning Users
October 1998
303
783
1,148
---
---
March 1999
610
1,494
3,433
239
106
April 1999
555
1,117
2,503
217
119
May 1999
441
866
1,845
195
91
June 1999
340
517
1,214
128
87
July 1999
311
607
1,448
93
88
August 1999
250
542
1,208
117
56
September 1999
214
426
979
105
39
October 1999
360
720
1,603
147
68
3,384
7,072
10,456
1,141
654
Total
Table 14 Health Reference Center Usage, 1998-1999 Month
Sessions
Views
Avg. Session Time (in minutes)
August 1998
19
54
12
September 1998
47
146
11
October 1998
55
75
8
November 1998
47
67
8
December 1998
104
224
8
January 1999
12
122
10
February 1999
79
166
9
March 1999
217
518
12
April 1999
74
265
12
May 1999
27
56
8
681
1,693
Total
197 website only. Information Access Corporation has its own statistical reporting system for its online full-text databases of health-related magazine articles and pamphlets. For a 10-month period of reported use, Health Reference Center had 681 user sessions for an average of 68 sessions per month. The heaviest months of use for this online database service were December 1998 and March 1999. At its April 5, 1999, meeting, the TCN steering committee "agreed that the TCN website will switch to Ebsco's Health Source Plus effective June 1, 1999, to reduce costs and increase coverage of health resources" (Provena Mercy Center Library, 1999, p. 1). All three school librarians present at the meeting had a favorable opinion of Health Source Plus coverage, the reading level range of full-text articles included, and search result displays. A contract was signed with Ebsco in May 1999, and by mid-June 1999, Health Source Plus was added to the site along with a link to the OCLC First Search version of Health Reference Center. Use patterns for Ebsco's Health Source Plus are reported in Table 15. For the five months of reported data, the pattern of use is lower than for Health Reference Center. A major variation in usage appears in September 1999 for Ebsco's Health Source Plus--there are a reported 544 log-ins for this first month of school. It was discovered by Ebsco Information Services that the password for access to the service had been distributed to staff at the ISBE by a TCN partner and that ISBE had generated most of the log-ins during September 1999. As a result of this breach of security, the account was restricted to internal use by Provena Mercy Center only, and Ebsco's Health Source Plus URL was removed from the TCN website in late October 1999. In an exit interview, Beverly Holmes, public library director, explained that the primary value of the TCN website is the enabling of teens and parents to conduct self-
198 directed exploration and questioning on "filtered" health-information resources and to e-mail specific questions to librarians via the TCN website gateway: The Teen CARE Network website allows them [teens and parents] to do that exploring and questioning on their own. We're there, available to them, if they need real specific answers from us. They can e-mail us--they know where to find us in the physical form as well. But they can find the information that's been identified as being helpful, those resources and tools through the website, to help them answer the questions they've got related to their health issues, their safety issues, those other aspects of their life that they might be concerned about.
Table 15 Health Source Plus Usage, 1999 Month
Log-ins
Searches
Hits
June 1999
4
9
281
July 1999
26
160
20,457
August 1999
22
184
10,314
544
2,896
508,877
37
191
74,493
633
3,400
614,421
September 1999 October 1999 Total
In commenting on a continuing vision for the TCN, Darnae Scales with Breaking Free, Inc., pointed to the importance of the library resources acquired and the website developed for teens through the partnership: I see the Teen CARE Network continuing to maintain the resources that they provide to and through their libraries. I think that's the value--and their website. And if possible, . . . do some interactive things on the website . . . put some questions out there to teens and ask them, . . . "What do you think adults feel about teens? Do adults in Aurora feel that teens are a resource or a burden?" [Laughter] You know, things like that. Carolyn Kerkla, West Aurora District #129 school administrator, high-
199 lighted the TCN's key role in facilitating and assisting teachers and students evolving knowledge of health and safety issues: Keeping that website, keeping that out in front of the kids, keeping them informed that it's there, keeping those teachers informed that it's there, and keeping it up-todate is really important. Again, from a selfish point of view, we can't possibly provide all of the curriculum that anybody could have a question on. And it's impossible to keep those kinds of books in the library anymore. They've [students and teachers have] got to have that access, they've got to know how to use it, got to be able to sort through information; it's good practice, good resources, and it keeps them fresh and keeps their ideas fresh, too, and their information new. . . . We have increased curriculum in health, more opportunities for kids to do those kinds of things. Safety is going to continue to be an issue . . . because . . . the awareness is heightened, the expectations are heightened. Administrators, teachers, the community--even students--are more aware of safety issues. So whatever support we can get there, whatever networking we can do there, is going to be supportive and helpful.
Value and Use of Materials and Equipment Acquired One direct benefit of the TCN for library partners was a pool of collection development funds for acquisition of books, pamphlets, and nonprint media to be housed at partner agencies. School, public, and medical librarians selected mater-ials that addressed peacemaking and nonviolence during Phase I of the grant. Phase II of the grant concentrated on family resource center materials. Wellness Information Center racks were made available to library partners, and digital video cameras were acquired to develop the website and be loaned to partners to experiment with "digital imaging" techniques. As a result of the collection development activities, a decentralized collection of 853 titles was added to area libraries. Of the 853 titles, 535 titles were books and nonprint media (videos, cassette tapes, and posters), and 318 titles were pamphlets from Life Skills and Krammes. A total of 1,012 items were added, so duplication occurred 15.7% among the library partners. The bibliography of these materials is
200 found on the TCN website (http://www.aurora.il.us/teencare/resources). Many of the library partners monitored the use of added TCN materials and freely commented on the use and value of these materials. Nancy Prichard, head of Adult Services at Batavia Public Library, noted, The reference materials so far have been used quite extensively, especially with health care and diseases. The pamphlets, once we advertised the fact that we had these to the public in our newsletter, were used more exten-sively. In fact, some of them disappeared. So I'm sure someone really wanted them well enough to take that advantage. The Life Skills pamphlets can be shared nationwide because they have been cataloged and added to OCLC. Because of that, they have been shared with schools and other libraries and facilities across the nation. The items received through the grant are sources our library would not otherwise have been able to purchase. Beverly Homes at Sugar Grove Public Library used TCN health materials as part of a book display for a drug and gang awareness program tied to community safety activities: "Our materials from the Teen CARE Network and THINK served as the backbone to a display set-up in preparation for a Dennis Hastert program with Neighborhood Watch on Drug and Gang Awareness." Finally, Marilyn Wolf, Jefferson middle-school librarian, saw her circulation statistics double for students and teachers with the addition of TCN health books and audiovisual materials: Teen CARE Network books were put into circulation in October. Our circulation count for October almost doubled from the September count. Our December circulation was also higher than usual due to the addition of Teen CARE Network resources to our middle-school library collection. In summary, the TCN materials acquired were selected and housed by the library partners but easily identified through the online bibliography found on the TCN website. The DLS van delivery and standard interlibrary loan procedures allowed for direct borrowing of resources by patrons and by libraries. Several of the prevention and youth service agency partners borrowed audiovisual programs directly
201 from Provena Mercy Center Medical Library, which supported training initiatives within their own agencies (e.g., Character Counts!, self-esteem building). Hospital outreach efforts into the community and library resource sharing complemented each other in this partnership project. Community Response to TCN Health Education Programs To obtain program evaluation feedback from community members and members of the steering committee, a series of evaluation forms were developed. Copies of the evaluation feedback forms utilized for community health-education programs and the comprehensive program evaluation form for 1998 are found in Appendix G. The program with the highest turnout sponsored by the TCN and Provena Mercy Center was the "Street Smarts" program held on May 4, 1998. The Provena Mercy Center advertised this evening program in the local Beacon News; distributed flyers to local schools, churches, and community organizations; and presented a speaker/author with television celebrity status; these efforts along with the concern of Aurora area residents about personal safety drew in nearly 400 community members of all ages. Of 125 participants responding to an evaluation survey, 117 or 93.6% strongly agreed that the speaker was knowledgeable about the personal safety subject. Of the 137 surveys returned, 72 participants or 52.6% of those responding to the evaluation survey indicated they had seen J. J. Bittenbinder on television before, and 93 participants or 67.9% of those responding wanted to learn more about methods to ensure the safety of family and friends. Of the 137 surveys returned, 101 participants or 73.7% strongly agreed that the program met their expectations, and 102 participants
202 or 74.5% strongly agreed that the program content was adequately covered. The community response to subsequent TCN programs was not as strong as in the case of the "Street Smarts" program. Evaluation comments received from TCN partners in the September 1998 evaluation pointed to areas for improvement: "Would have had even better attendance if publicity to schools was done prior to the last week of school in June [1998];" "More publicity needed at schools;" "My vision for the Teen CARE Network in the next year is for higher attendance at programs. Show the correlation between Teen CARE Network programs and violence reduction in Aurora." In spite of the perceptions of low attendance at programs, the steering committee in the September 1998 evaluated the Clothesline Project and Building the Peaceable Community, School, and Family programs as among the most highly effective during the first six months of the LSTA grant. Materials and equipment acquisition and the website development with Search Bank also were ranked as highly effective by the seven steering committee members responding to the September 1998 evaluation. For a copy of the September 1998 evaluation form, see Appendix G. Despite vigorous marketing of TCN public programs in area newspapers, through school mailings, and on the website, program attendance did not increase. In general, program attendance averaged between 30 and 40 participants at each program over the course of the 18-month grant project. There was no question about the quality of programming, for as several program participants noted, the programs were "interesting" and "informative" and generated suggestions for additional teen healthinformation service offerings: I think the program with the McGinnis[es] was very interesting. The Father Bill Tomes [program] is the one that sticks in my mind. It struck a responsive chord with me--an extremely moving program. I wish there had been a lot more people there.
203 I found this seminar ["Surviving Your Adolescents"] to be extremely informative and held my interest. Look forward to other seminars through the Network. There was a lot of information to take in a short time [in the "Surviving Your Adolescents" program]. Offer children and teen group counseling. Provide more information on teen relationships with a significant other. What's health and what isn't? More education about teen survival in schools is needed. Over the course of the 18-month project, TCN community health-information programs reached over 600 Aurora area teens, parents, and community members. Without the financial support of the Illinois State Library grant, these programs would not have been offered to the community.
Other Partnership Products and Services
Newsletter To communicate information about TCN community education programs and member agency services, a printed newsletter, Teens CARE About... Newsletter, was issued in 1998 and 1999. Two issues were produced and distributed to 4,000 teachers, parents, and agencies in the Aurora area. The third issue, April-June 1999, was mailed first class to 9,100 parents of teens in the Provena Mercy Center service area, in addition to the TCN library/school/community agency mailing list developed, which had 1,100 names. When the LSTA grant ended, the newsletter was converted from a printed publication to an electronic newletter on the TCN's website.
Materials Bibliography A bibliography of the 853 titles acquired during Phase I and Phase II of the LSTA grant was compiled and added to the TCN website under "Resources." The
204 bibliography can be browsed on the website alphabetically by title, and the holding library or libraries are indicated for each bibliographical entry to ensure direct borrowing of materials by patrons or interlibrary loan. See Appendix H for sample pages from the TCN web-based materials bibliography or view the full bibliography at http://www.aurora.il.us/teencare/resources.
Cartoon Contest, March 1999 To involve teens directly in themes of peacemaking and nonviolence, the TCN steering committee initiated a cartoon contest in March 1999. Sixty teens from Aurora middle schools and high schools submitted cartoons on one of 10 possible themes. Three of the award-winning cartoons, selected by a panel of four judges, were scanned and loaded onto the TCN website. All students who participated received a TCN Cartoon Contest certificate of participation at the end of the 1998-99 school year. Darnae Scales with Breaking Free, Inc., saw the cartoon contest as an avenue for youth to become familiar with the TCN and become directly involved in peacemaking activities: "I think the cartoon idea that the Teen CARE Network has is excellent because it exposes the youth to what some of the things the Teen CARE Network is doing."
"Peace Sheets" Exhibit "Peace Sheets" were distributed to the high schools and middle schools who were partners in the TCN during October 1998 in anticipation of the Week Without Violence. The school librarians were encouraged to let teachers and students know they could sign the "Peace Sheets" and commit to peacemaking and nonviolence within their school, family, and community and write hopeful messages to share with
205 others at their school. Olive Poliks, East Aurora High School guidance counselor, described student response at her building to the "peace sheet" supplied by the TCN during the Week Without Violence in 1998: The sheet we got from the Teen CARE Network--we took it to the cafeteria and the "Just Say No Club." . . . They [the club students] sat there and encouraged kids to come in and sign their names. So many kids signed, "My cousin Danny was murdered last year" or "My baby brother..." So many people had real stories about violence. That felt so good; they wrote their name or they wrote some little slogan on the sheet. They did that for one day through five lunch hours, and the sheet was just covered. Teachers, many teachers, came and wrote things that whole Week Without Violence. One teacher said, "I've been here for X number of years, and I've lost 14 kids." It's a very sad story. But the kids felt so good that they did something about it; then the banner was hung on the commons. The banner hung on the commons--it was just a real source of pride and acknowledgement.
Community Health Education Programs Offered and Four Video Productions The TCN worked with Provena Mercy Center and a number of community partners to present health-education programs on the themes of personal safety, peacemaking and nonviolence, and effective parenting over the course of the 18month LSTA grant project. The first program offered to the general public featured J. J. Bittenbinder, a former Chicago police detective, on the topic "Street Smarts: Personal Safety Techniques" on the evening of May 4, 1998. In June 1998, 20,000 brochures on the June 19-20, 1998, program offering, "Building the Peaceable Community, School, and Family" were distributed to teachers, students, churches, and community agencies. Dr. Phillip Jacobson, a local Aurora pediatrician with Dreyer Medical Clinic, and Jim and Kathy McGinnis, peace educators with the Institute for Peace and Justice, presented to 90 program participants information about effective parenting, resiliency in children, and techniques for
206 breaking the cycle of violence and creating circles of peace within our homes and communities. In conjunction with the peacemaking program, the Clothesline Project was featured in the Provena Mercy Center atrium during Father's Day week, June 1521, 1998. One hundred t-shirts lined the atrium walkways and visually told the stories of victims of violence and the reactions of family members to the murders of some domestic violence. Several TCN partners and the project director worked closely with the YWCA in planning and implementation of the Week Without Violence in October 1998 and October 1999. "Peace Begins at Home" ribbons, created by Mutual Ground, an Aurora domestic violence shelter and prevention agency, were distributed to all employees at Provena Mercy Center in October 1998. The "Peace Sheets Activity" and "Hands Across Aurora" were two other important events in 1998 and 1999 that provided teens and parents with opportunities to demonstrate their commitment to nonviolence and unity in Aurora. The East Aurora High School Honors Drama Class performed the play "Once Upon a Crime" to over 1,200 middle-school and elementary-school students in 1998 with an important message and unforgettable chant--"Stop the violence, begin today." And on October 19, 1999, the Institute for Peace and Justice presented two parenting-for-peace programs to 20 new teen mothers and to 30 Aurora community members and parents. During Spring 1999, a number of community education programs were offered by the TCN to heighten awareness of nonviolence and peacemaking issues. On March 14, 1999, Brothers Bill Tomes and Jim Fogarty, leaders of the Brothers and Sisters of Love in Chicago, Illinois, discussed their work with Chicago street gangs in reducing killings in the Cabrini Green housing project. "In the Line of Fire" had over 30 Aurora community members present, with a number of Catholic and Protestant clergy
207 in attendance. On April 11, 1999, the TCN sponsored a performance of the Health Works Theatre's play, "silence.com." Forty adults and children attended the 45-minute play, which presented vignettes on substance abuse, spouse abuse, and psychological abuse. Dr. Thomas Phelan, noted licensed clinical psychologist and author, presented "Surviving Your Adolescents" on May 1, 1999, at Provena Mercy Center. Thirty adults and teens were in attendance to enhance their communication skills and problem-solving techniques. Dr. Phelan compared major and minor issues and possible solutions for parents of teens. Rene Souba, a licensed clinical social worker with Provena Mercy Center, offered advice to over 40 parents and teachers at St. Joseph School in Aurora on May 18, 1999. Rene highlighted creation of mission statements and family goals based on the ideas of Steven Covey (1997) about the habits of effective families. As project director, I discussed the TCN's Family Pledge of Nonviolence and the importance of family conferences and "togetherness activities" for the parents and teachers at St. Joseph School. During National Library Week, April 4-17, 1999, the TCN sponsored the "Ask-A-Librarian for Health Information" promotion. TCN school, public, and special librarians advertised the TCN website (www.aurora.il.us/teencare) and reference services so that teen and parent health-information questions could be answered via the website electronic gateway. An overnight conference for middle-school students was held on a Saturday and Sunday, June 5-6, 1999. Safe Night USA drew over 60 middle-school students. The MWAH! (Messages Which Are Hopeful!) drama troupe performed a series of skills that showed the dynamics of abusive relationships and the dangers of drunk
208 driving to the young audience. TCN sponsored a booth at Project Unity's Back to School Fair in 1998 and 1999. Held in mid-August, the Back to School Fair has drawn 1,700 low-income families each year. Free school supplies, free health screenings, and information about social services available in the Aurora community have been provided to families in preparation for the coming school year. TCN partners and Provena Mercy Center Library staff and friends distributed partnership bookmarks, membership brochures, refrigerator magnets, and newsletters to fair participants. In evaluating the attendance at TCN community health education programs, Lynn Elam, programming director with the DLS, offered this advice on what she considered to be a disappointing community attendance level: In watching the programming that went on with this particular project--how do you get people out of their houses to come to the program? Because there was very good programming, and the attendance struck me as being disappointing in that you wanted to go knocking on doors and say, "Hey! You need to be here. This is really good!" You wonder what's going on--how do you get to the people, how do you get them out there motivated? It's not enough to issue press releases to the local newspaper--it's definitely not. That is very limiting. You can think about cable TV. How many watch their local TV channel? I think we have to become better at figuring out how to get the message to the people. Maybe the best thing you're ever going to get . . . is something on the TV or radio. So maybe we need to be thinking along those lines, thinking about broadcasting. This library consultant's media outreach advice was acted upon in the second year of the grant. To reach more community members with the peacemaking and nonviolence message from the June 1998 peacemaking conference, the TCN project director supplied two edited video programs produced by Video Perfections, "Building the Peaceable Community, School, and Family" and "Kids Count, Too: Nurturing Peacemakers," to Aurora Community Cable Channel 6 and Sugar Grove Channel 17. These programs were broadcast in April 1999 during
209 National Library Week. Edited video programs were also produced of the Brother Bill Tomes program, "In the Line of Fire," and the DLS Teleconference on the TCN services in 1999.
Safe Night USA in Aurora Darnae Scales with Breaking Free, Inc., commented favorably on the middleschool student conference that promoted Character Counts! six core values of trustworthiness, respect, responsibility, fairness, caring, and citizenship-I think that Safe Night was definitely a success. One, it was the way it was planned. It was really a Safe Night for the kids staying over because I know other communities nearby; [theirs] ended at 12 o'clock. The kids didn't get to sleep over like they did at Aurora's Safe Night. And I thought we had a good program. The program content gave enough variety to hold the kids' interest with the motivational speaker [a former college football player now a stockbroker], and the MWAH! drama troupe, and the speakers on different topics like drug abuse prevention. The TCN's "Pledge of Nonviolence" was discussed with the middle-school students during this all-night conference and an Aurora Safe Night "Peace Sheet" was available for the teens to sign.
Marketing, Public Relations, and "Media Blitz" The TCN employed direct marketing, paid newspaper advertising, free community press coverage, radio, and cable television as formal channels of communication for increasing awareness of the partnership and the website. Two Fox Valley Today interview shows were taped with Pam Nelson at Plano TV-30 in 1998 and 1999, a show which is seen in the Aurora viewing area. The local Aurora and Chicago newspapers (Beacon News, Chicago Tribune, Chicago Sun Times, Daily Herald, and Kane County Chronicle) were issued press releases routinely when the
210 two LSTA grants were awarded or community health-education programs were scheduled. Provena Mercy Center Public Relations Department provided consulting in the preparation of news releases. Direct mailings of program flyers, membership brochures, and newsletters were distributed to local churches, health-care providers, social service agencies, schools, government officials, libraries, businesses, and individual community members. The TCN developed an internal mailing list of over 1,110 agencies and individuals in the Aurora area with many names and addresses contributed by partner members. The following products and "give-aways" were developed over the course of the LSTA grant project to reach teens and parents: (a) refrigerator magnets (100), (b) bookmarks (15,000), (c) hats (30), (d) umbrellas (10), (e) membership brochures (2,000), (f) three issues of a printed newsletter (4,000-11,000 copies), (g) posters (100), (h) computer signs with website address (50), and (i) TCN buttons with website address (200). Copies of books explaining the "Family Pledge of Nonviolence" from the Institute for Peace and Justice, McGinnis et al.'s 1996) Families Creating a Circle of Peace: A Guide for Living the Family Pledge of Nonviolence, and presenting meditations on the Pledge by McGinnis (1998) were bought in bulk by the partnership to distribute at public programs and to partner agencies. Brochures were also purchased in quantity from the American Academy of Pediatrics (1995) on Raising Children to Resist Violence: What You Can Do and from the AMA (1996) on Media Use Suggestions for Parents for distribution to partners and the general public. The importance of marketing to the TCN for program awareness is best summarized by Olive Poliks, East Aurora High School guidance counselor, in her exit interview:
211 If we had more resources, I would put a lot in[to] marketing. I would get our name out there more. I had talked with one of our members about doing a press release every time we have a meeting. . . . I think we need somebody to do some aggressive marketing. I think more people are trying to get involved and either do something regarding publicity or pushing the programs with their staff as well as with the clientele that they reach.
Fundraising Activities The TCN partnership received two LSTA Grants from the Illinois State Library in 1998-1999 for a total of $106,890. According to Lynn Elam, DLS programming director, it was unusual for the Illinois State Library to provide a second year of funding for a grant project: Typically with LSTA or state library funds, grants are given as seed money to begin programs. But the fact that the Teen CARE Network received as much money as it did--I think once under LSCA and twice under LSTA is absolutely phenomenal. It [the TCN] definitely identified a need and met the need under terms of both programs. Amy Kellerstraus, LSTA consultant with the Illinois State Library, explained why the TCN project was funded under LSTA two times: I knew there was a sense of cooperation here [in Aurora]. And I knew there was a definite sense in that community and that area about the teens. And I thought, "This is a logical progression of where that group's going. They've got the base--now they're trying some other things." That's what I saw in Aurora. Here was this outreach to teens and, by gosh, guess what? Out of that came a real need for help. Not just information, not just outreach to teens, but health information. There was a focus here, and they were looking at what were the possibilities. Especially using some new innovations--the Web. You were looking at doing some things that were actually wanted. This is an area where a lot of libraries don't think about doing some research first. So that was the uniqueness that came through. It wasn't just a continuation [grant project]. It wasn't just, "Now fund us forever!" It [the grant proposal] was saying, "We have several activities, some good context to know ourselves. We're starting to talk about things, but we still feel this is something that needs to be addressed, that we haven't been able to address doing our activities that we now consider part of our everyday [library] things that we do." We weren't looking at a library; we were looking at a group of libraries that talked. That's critical. Provena Mercy Center also provided matching funds of approximately 10%-
212 15% of the grant total. This match was used to support partnership marketing and was offered to the TCN by the vice president of Marketing and Public Relations at Provena Mercy Center. Other TCN partners joined the fundraising bandwagon. The MLA awarded a Research, Development, and Development Project Grant to the TCN project director in 1998 in support of the Youth Risk Behaviors needs assessment research. Dreyer Foundation contributed a $500 grant to the East Aurora High School Honors Drama Class for costumes used in their "Once Upon a Crime" play for the YWCA Week Without Violence in 1998. During 1999, the Exchange Club awarded East Aurora High School a $500 grant in support of Week Without Violence activities. Breaking Free, Inc., offered $5,000 in grant funds from the Illinois Department of Human Services for 1999-2000 programming after the LSTA funding ended. West Aurora High School Library received one "Ask an Expert" grant for a series of 10 brown-bag teacher healtheducation training lunches from the Illinois State Library, totaling $3,300. Individual contributions were matched by Nicor Gas for a total grant of $200. And DLS awarded the TCN and Provena Mercy Center Library the 1999 Millennium Award for excellence in library services and programming with a certificate and $1,000 check in October 1999. Although a number of these supporting community groups did not become TCN partners, their financial support was a clear sign of the value placed on developing Aurora youth and providing quality health information for teens and parents.
Perceived Partnership Barriers or Obstacles The TCN LSTA grant project and partnering experience was seen by many of
213 the partners to be a positive experience, as revealed in the exit interviews conducted and Partnering Behaviors Survey responses. Yet there were some barriers that partners thought needed to be overcome. Specifically, Martha Kieffer, community liaison with Provena Mercy Center, believed TCN was too library-focused and needed to involve other sectors of the community as well as teens more directly in program planning and implementation: I guess one of the disadvantages is that it [the partnership] was so library-focused. It was a library grant, so it's understandable that it had to be. But, perhaps, drawing a little more resources from the social service sector --and we did have some social service agencies. People from [agencies such as Breaking Free] getting involved, working with kids--I know a couple of times church members came, and that's good. Somehow, if we could get teens involved, that's what I really would like to see--get the teens involved. At one of the conferences I attended, they said if you're at these partnership meetings, look under the table. If all you see are wing-tips and pumps, you've got the wrong people. Because, you should see SAS, see Nikes, see sandals, and you should see all different kinds of shoes under the table to get a true community partnership. So, that it's not just the professionals trying to fix them, us fixing them. It's everybody involved in making our communities healthier. Nancy Webb, RN, from Dreyer Medical Clinic believed that the peacemaking and nonviolence focus of the grant moved the project away from the general healthcare issues and concerns for wellness that were of primary importance to her employer: I think the clinic would appreciate a little more focus on what we could do to keep teens healthier, keep them nonpregnant--sexuality education and sexual transmission of diseases--things like that. I thing there was a point where it got to more the violence and the guns and the abuse, which is also important. But I think maybe we got away from where I was representing the clinic. I think we could integrate those two concepts better--social and health. Sean Waite, vice president at Provena Mercy Center, noted that the scope of the project and diverse partners involved made "boundary setting" difficult at times: Probably one of the biggest things is you want to be everything to everybody. It's a big challenge to take on such a project and, with limited funding, living within the grant. We [the hospital] did put in some matching--you have to balance the good works for the community along with the business needs, and that got difficult at times. When you get a great idea, you have to step back and say
214 that potentially, "We can't do that." It would have been nice to have funding longer than two years to really secure what the future of this [partnership] will look like. I think it was great work that was done in two years. It was a lot to get done and meet all those needs and now try to continue it for the future. The inherent difficulties of the "boundary spanning" role assumed by the project director is clearly reflected in observations made by Sean Waite. At times, it was a juggling act for the project director to accomplish the multiple tasks involved and to satisfy the needs of the multiple partner stakeholders with varying needs and keep the project within budget and on schedule. In contrast to the "boundary setting" perspective of Provena's administration, DLS programming director, Lynn Elam, perceived a need to further expand the project. Two shortcomings of the TCN grant project related to (a) the small number of committed partners and (b) the city of Aurora focus: One of the things I found really interesting about this particular project was the large amount of participants. Sometimes I think that can become unwieldy. I think that people derive more benefits than what they give. There were probably five or six people in the project that you could really point to and say, "Yes, they really pulled their weight." Where the others--they just got the goods! One of the things that I would like to have seen in this project was as the partnership grew, not an emphasis on Aurora so much, but more of a countywide or regional-wide perspective. Those are all the things to learn for the next time. But Aurora is a large city. So it was large enough that it could support this kind of program by itself. Martha Kieffer, community liaison with Provena Mercy Center, believed that time was a critical barrier for the TCN partnership and in community agency coordination efforts in general: Time is always an obstacle--having enough time. The resources of time, staff, being able to attend all the meetings is a problem--just being able to pull people together. That's always an obstacle as far as I'm concerned--getting people's schedules to coordinate and that kind of thing. Kim McLevain with the Kane County ROE saw both publicity and conflicting schedules as restraining the TCN:
215 Anyone that's putting on an event, the more publicity you can get, the better. I know we all try and help each other out, but we just need to publicize everything more. I'm sure you did an excellent job publicizing it. And I tried to help you out any chance I could. Another obstacle is the conflicting schedules of different agency representatives. We're all "meeting-ed" out, so getting people in one place at the same time is one of them. In responding to an open-ended question about partnership improvements, Darnae Scales with Breaking Free, Inc., recommended some improvements in the newsletter: "Give the Teen CARE Network more up-front publicity. For example, spell out Teen CARE Network on the front page of your newsletter and give your activities front page and your partners the remainder (except your highlights column)." Holly Cherry with Kane County INFO/Crisis Line also agreed that the conflicting schedules of partners was a barrier to communication and involvement: One thing I felt I would have liked to have seen was more repeat attendees at the [steering committee] meetings. I would like to have seen more people stay more "plugged in" and help determine more things. For instance, talking about the programs and details that we were able to put together. And I know I haven't been able to attend all of them [the meetings] either, but I felt like I would have liked to have seen more of the same faces. And I think the problem with that is people's busy work lives. Darnae Scales with Breaking Free, Inc., agreed that the effectiveness of the organization could be enhanced if partners attended meetings more frequently or sent an agency representative in their place: I notice that some of the members, that are listed as members, if they would consistently send a representative at least once during the year. Sending a representative if you can't make a meeting because, I think, one, you miss out on so much because that member isn't abreast of what's going on except if they have to wait for the newsletter. And second, we miss out on what that agency or organization is doing because they're not at the table. So I think it's important that [members attend]. I don't look at that as a barrier, but I look at it as--as great potential. Nancy Webb, RN with Dreyer Medical Clinic, conceded that technology was only part of the picture when delivering health-care information to the community. Openness to teen needs and health concerns is the key to bonding between teens and
216 youth service professionals: Wow, we really have this technology! It's really neat, but it is still the people who bridge that gap and bring the child, the adolescent, the teen, to that resource. That's the key. It's not having that technology. It's this open, warm, friendly person that brings it. The barriers, obstacles, and challenges described by these steering committee partners can be summarized as follows for the TCN partnership: • Insufficient budget to meet programming and marketing demands of a partnership program representing a diverse membership base; • Trying to be all things to all people--a strain between the lead agency medical librarian role and that of a "boundary spanner" project director; • The difficulty of coordinating time, resources, and people from different agencies; varying levels of commitment among the agency members influenced attendance and knowledge of programs and services and required formal communications to keep partners "connected;" • Public relations and marketing efforts requiring both on an informal and formal basis; • Differences in professional perspectives due to the group's diversity-negotiation and clarification between health care, education, social services, and religious communities; • A loss of focus on general teen health-information needs; and • Tension between technological solutions to youth problems versus human resource solutions.
The Future Vision for the Partnership Darnae Scales with Breaking Free, Inc., stressed the resource network, the
217 website, and more direct teen involvement in planning and decision making as keys to the future of the partnership: I see the Teen CARE Network continuing to maintain the resources that they provide to and through their libraries. I think that's the value--and the website. And if possible, do some interactive things on the website. You know, where you put questions out there to teens. I think that every avenue that we have for planning, we can have at least one or two teens involved. That would make sense and would be consistent with the mission of the Teen CARE Network. The need for direct involvement by teens also appeared in responses to openended questions in the Partnering Behaviors Survey. This recurring theme is reflected in these partners' comments: "I would like to see more direct interaction with teens;" "I believe for the next year we need to bring more teens to the table and get their input on `teen care' issues in our community." Lynn Elam, DLS programming director, thought that a permanent "home" with a tax-supported agency would ensure that the website and program continue into the future: What I would really like to see happen here is, I would like another agency or a city or a county or somebody to come in and say, "This is a great program. Let's incorporate in into what we do," and keep it alive and living that way. . . . Ultimately, I think I would like to see the program, not absorbed, but incorporated within a larger tax-funded agency so that it can continue. Sister Margaret Mary Knittel, Provena Mercy Foundation grants writer, offered this insight on finding a "home" for the partnership after the Provena Mercy Center launch: This [the partnership], to me, is a kind of thing that would better succeed, in my opinion, with some kind of "home" as you call it. Who owns the [digital] cameras? I think that's an important question. I'm not going to dismiss that, but whether it just fizzles because it's person-driven and not project-driven. Maybe they [the TCN agencies] should hire somebody half-time or one-third time? Maybe East Aurora High School would give one of their faculty members two periods a day release time and fund it that way. It seems different to me than other examples in my head. Especially because of the technology. You've got to dust it [the website] off; you can't just promote it.
218
The issue of future funding for the TCN is a critical issue faced by the organization. In an exit interview, Darnae Scales with Breaking Free, Inc., encouraged the TCN leadership to seek new funding sources and share the responsibility for grant writing among a number of the partners: Continue to research to find other sources of funding together so it's not burdensome on any one person. Take the grant application and proposal and say, "Okay, I'll do this piece. You do that piece." Allocate responsibility or delegate responsibility and seek new funding streams. Olive Poliks, East Aurora High School guidance counselor, stressed the positive mission and commitment of the partners in building a better Aurora community: I think my vision is to be totally open, to just believe that good things are going to happen. It has to be good things . . . because every single person involved is committed to making our community better for teens. It truly is a perfect name--Teen CARE. These are people who care about teens and want to make a difference in their lives, and I'm really proud to be a part of it. Kim McLevain, social worker with Kane County ROE, agreed with the need for open communication and indicated that the more experience with collaboration, the better the results obtained: I would say, keep communication open, try not to come in with a closed mind, be as open as possible to new experiences, new suggestions, new opportunities for whatever the other partner might be bringing in. Follow-up on anything you're supposed to, make sure you do everything you're supposed to, and remember that everybody's human. We will make mistakes. And every time we collaborate, we get better as we go along! Amy Kellerstraus, the LSTA Grant consultant, offered two pieces of advice on the future of the TCN in an exit interview: improve and maintain the website and continue to meet as a partnership and network: I think there would be two things I would want them [the partners] to try to do. One is maintain or improve the website . . . keeping it up and making sure it's current. In other words, continuing to be aware of what should be added or subtracted and being forward enough to say, "We should take this off, we should put something else on," and being willing to give the time or the effort to basically
219 develop that. The second thing is, I hope they continue to meet. Because I think if they continue to talk, they're going to find out that there's more beyond the TCN that they can also do. It's communication--even if you met only four times a year--but the primary purpose was to review what we should continue to do on the Teen CARE Network, but also what areas should we [the partner agencies] get into? Based on these exit interview excerpts and Partnering Behaviors Survey comments, the future promise of the TCN can be summarized as follows: • Research new funding sources for teen health, wellness, and prevention projects; • Locate a permanent "home" for the partnership to house programs, services, and resources acquired; • Directly involve teens in the operation and decision-making of the partnership; • Expand public relations and marketing to increase awareness of the partnership to Aurora teens, parents, and the community at large; • Maintain commitment, communication, and openness to new opportunities that are identified through regular partnership meetings; encourage risk-taking; • Maintain and expand the website based on teen health concerns and interests and obtain feedback through an interactive survey on the website; and • Continue to add to the health-information resource base and technology base at partner libraries. Summary of Overall Effectiveness and Partnership Impact From the responses of 20 partners to the Partnering Behaviors Survey, there was consensus that the partnership was effective in these areas: 1. Commitment: 100.0% of the respondents either strongly agreed or agreed
220 that commitment to partnering was shared among the members and that members believed they could "make a difference" in providing health information to Aurora teens and parents. 2. Environment of openness and trust: 95.0% of the respondents strongly agreed or agreed with the statement, "We created an environment of openness and trust for all involved." 3. Clear vision of what we wanted to accomplish: 90.0% of the respondents strongly agreed or agreed with the statement, "We shared a clear vision of what we wanted to accomplish." 4. Active listening: Of those responding, 85.0% strongly agreed or agreed with the statement, "We listened actively to one another's viewpoints." 5. Sharing of information, skills, authority and resources: Of those responding, 85.0% strongly agreed or agreed with the statement, "We shared information, skills, authority, and resources." 6. Empowerment and opportunity-seeking: Of those responding, 85.0% of strongly agreed or agreed with the statement, "We found opportunities and empowered others." 7. Communication: Of those responding, 65.0% of the partners responding to the survey strongly agreed with the statement, "We kept one another informed throughout via scheduled meeting times, regular mailings, e-mail, and telephone." 8. Marketing to clients and the community: Of those responding, 65.0% strongly agreed or agreed with the statement, "We shared information about the partnership with those we served and actively marketed TCN services." 9. Recognition of contributions and celebrating successes: 95.0% of the respondents strongly agreed or agreed with the statement, "We recognized and
221 celebrated our successes." 10. Participatory decision-making and change: 75.0% of the respondents strongly agreed and agreed with the statement, "We mutually agreed to any changes that needed to be made." 11. Opportunities for creative problem-solving: 80.0% of the respondents strongly agreed or agreed with the statement, "We solved problems creatively and sought opportunities and encouraged others to do so." 12. Honest about strengths and weaknesses/effective interaction with one another: 90.0% of the respondents strongly agreed or agreed with the statement, "We were honest about our strengths and weaknesses and interacted effectively with one another." The responses of partners to the Partnering Behaviors Survey also point to these areas for improvement in partnership operations and partnering behaviors: 1. Conflict management and disagreements managed: Only 55.0% of the respondents strongly agreed or agreed with the statement, "We managed disagreements and conflicts appropriately." 2. Risks taken: 65.0% of the respondents strongly agreed or agreed with the statement, "We took necessary risks." 3. Fulfilled agreed-on responsibilities: 65.0% of the respondents strongly agreed or agreed with the statement, "We fulfilled all agreed-on responsibilities." 4. Checkpoints established to monitor our progress: 65.0% of the respondents strongly agreed or agreed with the statement, "We established checkpoints to monitor our progress."
Summary of Partner Views on Success and Impact
222 These exit interview comments from the partners in different community sectors offer insight into the critical success factors at work in the TCN.
Health-Care Viewpoints I think it was very successful and one of the biggest initiatives we've ever taken on. Even if we hadn't accomplished all the positive goals we've achieved, just to bring those groups together, get them to work together, was a positive. It [the partnership] is one of the finest examples . . . of a community linkage through health education . . . that I have seen. I've never seen a finer example in a short period of time, accomplishing as much as this particular grant accomplished with the outreach. And the focus that this particular project took and what the results of the needs assessment showed would be to focus on violence and prevention with families and children. Did it [the grant project] bring a new patient into the door? That's how the hospital thinks. Whether it's a direct implementation of its mission, that's the debatable point. I think it was very successful in establishing that ability, the use, that measuring. How is it being used? Are the kids really using it [the web site] and getting something out of it? I think it was wonderful. It did what is was supposed to do.
Library Consultant Viewpoints I think it was very successful in terms of broadening a network of awareness. I think that everybody who was involved now has a better sense of what these other agencies do, just the discovery that these people are out there working in these particular types of areas. The contact information alone, I think, is very, very valuable. It's a long history of success [in Aurora]. Because of that history of success, there's a sense of, "Oh, that's the area of DuPage Library System that has a good track record."
Community Agency Viewpoints I think that anything that lasts longer than a few months has to be doing some good. And I think that these connections and the statistics you shared with me about
223 the hits on the site is outstanding. . . . It's obvious that kids or people are accessing it [the website] for some pretty definite reasons. In other words, people know it's out there, they know how to access it, they're going there. I measure it [success] by the simple fact that when I read the minutes, I see more people involved. The more people you have as a resource, the better off the organization's going to be. Sustaining the Partnership: TCN Leadership Structure and Programs, 1999-2000 In June 1999 as the LSTA grant project was drawing to a close, a new leadership team structure went into effect with the nomination and selection of two cochairs, a program chair, a Web master, a public relations chair, and a recording secretary. Figure 8 depicts the new partnership leadership structure approved by the steering committee. The co-leaders renamed the steering committee into a "Leadership Team," and planning meetings were held throughout the summer of 1999 to implement programs for the 1999-2000 school year for teens and parents. The outgoing TCN project director worked with Provena Mercy Center's administration and the TCN partners to ensure a structure was in place, using increased volunteer involvement as the key mechanism beyond the LSTA grant project. A boost came to the TCN from Breaking Free, Inc., in the form of a minigrant. Darnae Scales, community mobilization specialist with Breaking Free, Inc., applied for $5,000 in grant funds from the Illinois Department of Human Services to support TCN programming for the 1999-2000 school year. The grant also allowed for the acquisition of additional library resources for TCN partners, marketing of the TCN website on t-shirts, and provided funds for speakers at community health education programs. A series of five programs were planned for the 1999-2000 school year: (1) "Making Winners Out of Would-Be Losers," a presentation on cultural diversity and
224 academic achievement by Dr. Samuel Betances on September 13, 1999, at East Aurora High School; (2) "Starting Out Right: Nurturing Young Children as Peacemakers" on October 19, 1999, for the YWCA Truancy Alternative Program (TAP) and YWCA Week Without Violence presented by Jim and Kathy McGinnis with the Institute for Peace and Justice; (3) "Parenting for Peace and Justice" on
225
Figure 8: TCN Leadership Role Structure, September 1999
226 October 19, 1999, for families, presented by the Institute for Peace and Justice at the Copley Theatre, Aurora; (4) "Open Line: Where Parents and Teens Connect," on February 15, 2000, at East Aurora High School; and (5) "Is It Too Late? How to Recognize Signs of Substance Abuse in Teens," on April 27, 2000, at West Aurora High School. Olive Poliks, newly elected co-leader of TCN, summed up the future direction of the partnership in terms of proactive leadership and democratic participation: I think the real thing is leadership; I think that is absolutely key, that we have to have people in place who are willing to push, really push. I feel I'm willing to do that, and I feel I have the personality--I'm a very pushy person. I think it's going to take that. I don't think we can sit around and be passive and say, "Well what do you want to do?" "I don't know, what do you want to do?" People are willing to do it if you tell them what you want them to do. People absolutely want to have input, it has to be some kind of democratic process and some kind of sharing of materials, but there has to be a pushy person behind it. Future projects for which funds are available include the development of public service TV announcements (in 1999-2000 school year), written and produced by students and edited in cooperation with Video Perfections, about nonsmoking and the TCN website; and distribution of the TCN t-shirts (250) to promote the website and logo. Enhanced advocacy efforts at the state, county, and local government levels on teen health issues are also anticipated in the coming years. Evaluation of the TCN Partnership Using Two Models Table 16 summarizes the four key dimensions for evaluating partnerships as presented by Alter and Hage (1993) and contains columns that show the strengths and weaknesses of the TCN in relationship to the four evaluation dimensions.
227 Table 16 Partnership Effectiveness Matrix Strengths Goals
Five goals
Weaknesses Meeting attendance inconsistent
Increase from 15 to 40 members Marketing Website developed, 9/98 Media coverage increased Products and programs System resources
Materials acquired = 850+
Future funding uncertain
Total funding = $130,000+
501 (c) (3) status needed
Bibliography of materials on website Internal processes
Absence of conflict
Vision often unchallenged
Diversity of partners Constituencies
Responses reflected high personal satisfaction Group continues to meet Different agencies attend monthly meetings
Source: Adapted from Alter & Hage, 1993.
Administrative support uncertain at top levels of partner agencies
228 These four dimensions of the TCN partnership, which will be briefly analyzed in this section, are (1) goals, (2) system resources, (3) internal processes, and (4) constitutencies.
Goals The goals achieved over the 18-month grant lifecycle are taken from the TCN Phase II: Final Report (Howrey, 1999c). The TCN accomplishments are summarized as follows: Goal 1:Build and expand the partnership from its current membership to 25 active partners The partnership now numbers 40 members and this growth exceeded our expectations. The increase from 15 to 40 members over an 18-month time period is a 167% increase in membership. The diversity and geographical location of member agencies has also expanded over time. We have agencies representing Black and Hispanic youth and several partner agencies are located in northern Kane County and DuPage County. The Teen CARE Network partnership holds monthly Leadership Team meetings which serve as a communication forum about youth services in the greater Aurora area. Attendance at these monthly meetings has averaged between 1012 youth services professionals and librarians. Goal 2:Continue to develop an Aurora Teen Health and Wellness Internet website The Teen CARE Network website has met its major goals for free access to health information and updating the Healthy Teens Handbook in a cost-effective manner. The website usage has averaged 376 user sessions and 1,162 search engine hits per month. WebTrends data indicates that public and school library patrons are the primary users of the Teen CARE Network website. Approximately one third of website users are returning users. Goal 3:Collaborate with local news media and heighten the visibility of the Teen CARE Network The visibility of the Teen CARE Network has increased over time, but the Leadership Team believes there is significant room for improvement in the marketing of the program to the community and recognition of the TCN mission by our local news media. The projected Public Service Announcement on cable television and press releases to local newspapers on programs and meetings will support the continuing visibility of the partnership in Aurora. The
229 membership brochure and Teen CARE Network website bookmarks developed for Phase II outreach programs have enhanced our ability to spread the Teen CARE Network mission along with the "Pledge of Nonviolence," adapted from the Institute for Peace and Justice and FAVAN, on our website at www.aurora.il.us/teencare. Goal 4:Acquire materials in a variety of formats in both English and Spanish to be shared and housed among TCN partners The Annotated Bibliography of Materials Added [see Appendix H] reflects the variety of health topics and formats selected by the Teen CARE Network library partners. A continuing effort by the Teen CARE Network librarians is important to keep health education and prevention materials current for teens and parents. Goal 5:Develop mentoring behaviors critical to violence prevention and peacemaking for teens, parents, and TCN partners The Teen CARE Network has linked with other agencies that have strong mentoring programs in place--Communities in Schools, West Aurora School District, and East Aurora School District. Programs and publications from the Institute for Peace and Justice define mentoring behaviors in terms of the "Family Pledge of Nonviolence" and the "School Pledge of Nonviolence." Breaking Free, a Teen CARE Network partner, is working with the schools to train teachers in the use of the "Character Counts!" curriculum with elementary and middleschool students. The "Character Counts!" program emphasizes six core or pillar values--trustworthiness, respect, responsibility, fairness, caring, and citizenship. (pp. 11-12)
System Resources System resources were added through the grant in the areas of human resources, learning resources, and technological resources. With 40 TCN partners, we have been able to tap into the expertise and skills of involved members. Aurora University has provided technical assistance with MS Frontpage `98 and publication of the TCN website on the Aurora Online Community Network Web server. Over 800 learning resource titles were added to the collections of the nine library partners. Additional resources for individuals on peacemaking, parenting, and general teen health issues have been distributed at community health-education
230 programs. A centralized bibliography of resources for loan from partner libraries is accessible on the TCN website. After a dispute with Ebsco Information Services over the licensing of the Health Source Plus, the free health information on the TCN is now OCLC's First Search. Each member library has its own free account, so the First Search product eliminates any concerns over security of account numbers or passwords for "free" access to health information. The Leadership Team is involving more partners in task forces and grant writing and delegating responsibility for the actual operations of the TCN. Without a paid project director, the partners are helping with these tasks to sustain the organization and involve teens and teachers in health-information delivery.
Internal Processes The TCN website and the monthly Leadership Team meetings serve as the primary means of communication for the partnership. One policy is in place for the loan of the digital cameras acquired with LSTA funds. The printed newsletter was replaced by an electronic edition on the TCN website to reduce printing costs. Minutes continue to be issued and mailed monthly to partners, along with the announcement of the next meeting. The Leadership Team meetings are facilitated by a guidance counselor and a school librarian. East Aurora High School currently maintains the financial records for the TCN because the partnership itself is not yet a 501 (c) (3) organization and cannot accept grant funds directly. Teens have begun to attend Leadership Team meetings and present health-education projects that are of interest to the membership.
Multiple Constituencies
231 Based on the responses of 50.0% of the partners to the Partnering Behaviors Survey and the willingness of partners to allocate time for 30-minute exit interviews, it can be concluded that a high level of commitment and satisfaction with the partnership exists. Leadership meetings continue on a monthly basis with an average of 10-12 professionals attending, and there is sharing of resources, program offerings, and career opportunities. A total of 70 agencies receive minutes and notification of the meetings each month. TCN Leadership Team meetings contribute to the personal satisfaction of the professionals who attend. An atmosphere of openness and trust exists during the TCN Leadership meetings, and the group facilitation style is one of active listening, encouragement, participation, and mentoring. The professionals represented at TCN meetings provide direct services to youth and are not the key administrators of the partner agencies. As a result, the opportunity for the partnership to receive direct financial contributions or to develop direct services for youth are unlikely given the present membership mix and volunteer coordination of the TCN.
Partnership Success Factors Table 17 presents the 19 success factors identified by Mattessich and Monsey (1992). This model is applied to the TCN partnership case to assess the factors contributing to the effectiveness of the partnership. Two columns have been added to this table: one column represents areas of strength demonstrated by the TCN in relationship to the success factors, and the second column identifies areas for improvement based on partner feedback received by the primary investigator through the exit interviews, written comments, meeting interactions with partners, and informal telephone conversations.
232 This success factor matrix illustrates why the TCN partnership has contin-
233 Table 17 Nineteen Partnership Success Factors Applied to TCN (Mattessich & Monsey, 1992)
Strength
Needs to be Improved?
X
No
Weak
Yes
X
Aurora mayor + ACMAB
Environmental Factors 1. History of collaboration or cooperation in the community 2. Collaborative group seen as leader in the community 3. Political/social climate favorable Membership 3. Mutual respect, understanding, and trust***
X
4. Appropriate cross-section of members***
X
5. Members see collaboration as in their self-interest
X
6. Ability to compromise
Untested
Bus/Minority
Raise issues
Process and Structure 7. Members share a stake in both process and outcome
X
8. Multiple layers of decision making
X
Group process
9. Flexibility
X
Funding??
10. Development of clear roles and policy guidelines 11. Adaptability
Informal group X
New leaders/ writing grants
12. Open and frequent communications**
X
More informal
13. Established information and formal communication links
X
Meetings, web
14. Concrete, attainable goals and objectives
X
Better timeline
15. Shared vision
X
Project-driven
16. Unique purpose
X
Yes, teen health info
Communication
Purpose
(continued on following page)
234 Table 17 (continued) Resources 17. Sufficient funds**
X
18-months + new grants
18. Skilled convener*
X
Continues with new leadership
* High consensus ** Moderately high consensus *** Very high research consensus
ued to sustain itself beyond the 18-month grant period. The crucial factors at work in this case study were (a) the previous history of collaboration among the commit-ted agencies in health-information service delivery; (b) the favorable climate in the Aurora community toward partnerships and cooperation; (c) the frequent communications, both formal and informal, among the membership; (d) the diversity and heterogeneity of the agencies represented at the table; (e) the development of feelings of trust, respect, and understanding of the partners toward one another; (f) sufficient funds; and (g) a skilled convener. Ultimately, the TCN is bridging educators, teachers, and youth services professionals in providing a "learning organization" to the two public school districts and several private high schools. The TCN community health education programming and "cutting-edge" website offers a new electronic and just-in-time delivery mechanism for improved health information to Aurora teens and parents.
CHAPTER 6 CONCLUSION
This chapter summarizes the key findings gathered on the development, growth, and effectiveness of the TCN library/community agency partnership. The chapter also highlights the significance of the research findings for both the academic and practice communities and the main benefits of the partnership for library and youth services practitioners. The strengths and limitations of the case study and AR methods employed are identified, and recommendations for future AR projects are outlined specifically for the Aurora, Illinois, community and in general for researchers interested in implementing change in their own local communities.
Research Questions The research questions answered in this research investigation cover these partnership development issues: 1. What are the phases and processes involved in the formation and implementation of a CHI network partnership/alliance? 2. What are important coordinating structures in developing effective library/community agency partnerships? 3. What are barriers to collaboration that partners perceive may limit the effectiveness and growth of a partnership? 4. How do the partners define successful outcomes in evaluating the partnership in addressing a mutually defined problem and seeking community-level solutions? How are successful partnering practices and collaborative behaviors
236 defined by the partner agencies involved in the network? 5. How is the partnership sustained over time? The Process and Phases of Partnership Development Library/community agency partnerships such as the TCN form to address a community problem that the partners believe need to be resolved. The partners arrive at a common vision, which requires collaborative planning and deliberation on the particular methods to be employed. For the TCN, a website, newsletters, monthly steering committee meetings, and community health-education programming were important methods employed to communicate to teens, parents, and interested professionals about available health and social services (Kane County INFO, 1994) and free health-information resources in Kane County and on the Internet. As a result of these communications about the partnership's nonviolence and peacemaking mission and available health-information resources (i.e., benefits), more youth service agencies joined the partnership over the 18-month grant period; the partnership grew from 15 agencies to 40 agencies. The grant application process required that each partner agency write a letter to Provena Mercy Center Hospital committing staff time to network participation and involvement in programming. Formalizing this process contributed to the legitimacy of TCN and its institutionalization within DLS and the receipt of Illinois State Library LSTA grant funding in 1998 and 1999. The implementation of the partnership required that a project director navigate the differing needs of the lead agency, Provena Mercy Center, and the key stakeholders in the library/community partnership--schools, social service agencies, health-care
237 providers, public libraries, school libraries, and government agencies. As the convener of TCN, I was able to build on my 20 years of professional and volunteer experience in the Fox Valley area. I discovered that my networking and marketing skills, honed as a support group leader for the Greater Chicago Area Chapter of the Alzheimer's Association over a 10-year period (1981-1991), prepared me well for my role as convener of TCN. My library organizational skills ensured that the grant project goals were implemented despite the tight schedule of website development, health education programming, and library collection development activities. The collaborative approach to collection development and website development motivated both myself and others involved in the partnership building process. Gray's (1989) model of the collaborative process served as a tool that guided the exceptional performance of TCN. The partnering behaviors demonstrated by the steering committee members were a key part of the effectiveness of the partnership. The partners served as mentors for each other and established an "environment of openness and trust;" engaged in active listening; were willing to share information, skills, authority, and resources; and found opportunities to empower one another. Despite differences in contributions to the group, 100.0% of the partners responding to the Partnering Behaviors Survey agreed that there was a high level of commitment to partnering shared among the TCN members. A clear vision was evident to the partners as well--90.0% of the partners agreed that a clear vision of what needed to be accomplished was present among the TCN's partner agencies. Coordinating Structures for Library/Community Agency Partnerships
238 The coordinating structures that were put into place for the TCN contributed to its effectiveness over the 18-month grant period: project director, steering committee with monthly meetings, mission statement and goal-setting, minutes of meetings, marketing and newsletter, the allocation of funds for library partner collection development and ordering procedures, website, and routine follow-up with partners by the project director. The literature review on effective partnerships, both theoretical and research-based, pointed out the need for these structures to be in place.
Perceived Barriers to Collaboration The results of exit interviews and my observations as project director suggest that partners perceived several barriers to collaboration. These barriers were identified as (a) an insufficient budget to meet programming and marketing of the partnership; (b) a strain between the local library resource needs of the hospital as lead agency and the community-oriented needs of diverse agencies; (c) a small core group of committed partners among the 40 partner agencies composing the partnership; (d) uneven participation in programming activities among the local school districts (e.g., Aurora YRBS survey results that drew heavily from West Aurora School District #129 and were not representative of the total Aurora high school population risk behaviors); (e) lack of a paid employee to exclusively work with partnership marketing and media relationships; (f) a loss of focus on health-information dissemination versus nonviolence and peacemaking; (g) a lack of direct teen involvement and leadership in TCN program planning and implementation activities; and (h) tension over the role of technology versus people in disseminating health information.
239 Successful Outcomes The barriers to partnership collaboration identified above did not seriously impact the effectiveness of the TCN in accomplishing its goals, programming objectives, and the building of a community information network to deliver quality health information to Aurora teens and their parents. Written comments received from the partners reflected a high level of personal satisfaction by partner representatives as a result of their involvement in the professional networking group. In addition, statistical data on the use of the website showed an average of 376 user sessions per month in 1999. WIC collections were added to all nine library partners, and a bibliography of the health resources added can be searched on the TCN website. The printed newsletter, Teens CARE About... Newsletter, was converted to an electronic publication that is accessible to any teen or parent with an Internet connection.
Sustaining Partnerships: Success Breeds Success The grant-writing process that gave birth to TCN in January 1998 has continued under the present Leadership Team in 1999-2000 and resulted in a grant application to the City of Aurora Funders' Consortium for "Target: Tobacco-Free Youth," a smoking prevention program in 2000-2001. The proposed grant project uses a peer-counseling and role-modeling approach to encourage a tobacco-free lifestyle for teens and elementary students. Grant writing is seen by the TCN Leadership Team as an important way of obtaining the funds necessary to sustain innovative health education programs. TCN continues to communicate routinely and to meet monthly under the revised Leadership Team structure. The website continues to be maintained, and an electronic newsletter has been added to the website in place of the more costly printed
240 newsletter. All these coordinating structures established are consistent with the critical success factors considered important by Alter and Hage (1993) and Mattessich and Monsey (1992) to ensure the partnership sustains itself into the future. Marketing of the TCN is an important and continuous part of the change process. The Leadership Team remains in contact with the local newspapers and cable television producers about programs and services offered to teens, parents, and youth services professionals through the TCN. Many of the active partners believe that the partnership would be more effective if high-school and middle-school students were recruited into leadership roles, directly involved in planning, and encouraged to communicate to peers about the implications of the Aurora Schools youth risk behaviors survey results for their school district. The partners believe the teens desire a voice in setting the direction and operating tone of an organization that cares about their health, social, spiritual, and intellectual needs. From what the partners reported in the exit interviews, TCN is governed by a living and breathing "ethic of care" that governs their interactions with partners, colleagues, and clients.
Significance of the Research TCN is an example of a "symbiotic network" in which organizations from different niches in the community banded together to achieve a common set of goals (Alter & Hage, 1993). As TCN partners learned through the relationship to do things better and make continuous improvements in their partnership activities, the active partners created mutual rewards that were self-reinforcing. This process generated mutual dependency and interdependency. In this manner, reciprocity was established, and the relationship within the partnership deepened as learning continued, and adaptiveness was speeded up. TCN in essence took on the features of both a learning
241 organization and an informal, professional networking group (Ramsey, 1997; Rowley, 1997; Watkins & Marsick, 1993). As the grant project evolved, it became apparent to me in the role of project director that TCN took on the features of a "learning organization" and an informal, professional networking group. The representatives from partner agencies involved in the steering committee sought out new ideas, new problems, and new opportunities for learning from each other with the intent of gaining "competitive advantage" in serving their clients (Rowley, 1997). For TCN members, the competitive advantage was gained through technology with the creation and maintenance of the website, a gateway for electronic communication between agencies and clients with e-mail capability on the website, and a formal Mailman listserv. Dixon (1994) defined organizational learning as "the intentional use of learning processes at the individual, group, and system level to continuously transform the organization in a direction that is increasingly satisfying to its stakeholders" (p. 5). A key part of this definition focuses on the fact that the organization changes in a direction that satisfies the stakeholders involved in an organization. Based on the partner agency feedback from the Partnering Behaviors survey and exit interviews, it is clear that organizational learning occurred and was valued. A second definition of a learning organization was provided by DiBella and Nevis (1998). Organizational learning is viewed by these authors as "the capacity or processes within an organization to maintain or improve performance based on experience" (p. 28). This second definition highlights the continuous improvements that result from the type of experience and learning that occurred in this case study. Learning organizations are characterized by three processes: (1) knowledge creation or acquisition, (2) knowledge dissemination, and (3) knowledge use. All
242 three processes are required for organizational learning. And the TCN's library and community agency partners believed these processes were basic to its mission of improving health-information delivery to Aurora teens and their parents. In addition to the technology benefits of the TCN partnership, the committee members involved in the LSTA grant preparation also believed the human element crucial to long-term success and results. Professional networking was a benefit of the partnership that served as the foundation for collaborative service improvements (Howrey, 1998b). As defined by Ramsey (1997), "A network is an extended group of people with similar interests or concerns who interact and remain in informal contact for mutual assistance and support" (p. 9). The benefit of an effective network of professional contacts is that it allows the professional to be part of an invisible team, even when you're working solo. A professional network provides a safety net and a personal "think tank" to help get one's job done. Networks are effective "because they are flexible and comfortable and they truly help people do a better job" (p. 12). As discovered through the 18 exit interviews conducted as a part of this AR project, the mutual benefits of innovative web-based technology for health-information dissemination and professional networking were important to the TCN partners in their daily work with teens and parents. The resource dependency model introduced in the review of the literature is applicable to the TCN partnership experience. Many of the organizations that joined the TCN anticipated direct benefits from the TCN website, the books, the audiovisual materials acquired, and the equipment (WICs and digital cameras) added for direct access by partners through the LSTA grant. This case study points to the importance of taking a holistic approach to
243 developing health information and community education programs for teens. Youth development hinges on opportunities for real-life problem solving before crisis situations occur. The Aurora Schools YRBS results indicated that teens typically do not seek out health information and lack experience in locating needed health and social services. Thus, the health-education curriculum designers at the middle-school and high-school levels are encouraged to routinely incorporate critical-thinking skills, cooperative learning, role plays, case studies, and information-gathering strategies for teen "real-world readiness." And the health-education curriculum needs to actively recruit health-care professionals and social service professionals as mentors and role models for teens to understand and actively seek out healthy lifestyles. This perspective on a holistic approach to health education is consistent with current health promotion models. As Millstein, Nightingale, Petersen, Mortimer, and Hamburg (1993) argued, many different perspectives need to be integrated into effective adolescent health promotion programs: As society has changed, our perceptions of health and health promotion have also undergone major change. From a strictly biological model, we have broadened our perspectives to include psychological and social/environmental aspects of health. This biopsychosocial model considers health in terms of personal experiences of general well-being, the capacity to perform expected roles and tasks, and the fulfilling of one's health potential. Responding to the challenge of promoting adolescent health in the 21st century will require integrating knowledge bases from a variety of sources. Effective health promotion . . . requires a broad-based strategy that includes participation of the many individuals and institutions that have contact with or otherwise affect the lives of adolescents. (p. 1413) Community outreach and partnerships bring clients to the forefront of healthinformation services and break down the artificial barriers between professionals committed to the same goals and ideals. Kanter and Eccles (1992) noted there is a continuing gulf in bringing what is known about partnerships and interorganizational networks from the academic world
244 to bear on the world of practice. This AR project was designed specifically to bridge this gulf. The integration of analysis and action, theory and practice, and the ideal and real worlds is a goal of AR. Action researchers recognize that knowledge is socially constructed, open to change, negotiation, and reconstruction. Creating collaborative learning organizations, action researchers unite the best ideas with strategic actions to make change and process improvements happen. The methodologies employed in this case study to analyze and make continuous process improvements in the functioning of the TCN partnership are tools that can be employed by other health-care and library practitioners to improve professional practice and health-information services to customers. The findings of this case study contribute to the knowledge base for managers on how to build and deploy networks strategically for the delivery of quality health-information services. The various agencies and organizations that joined the TCN in 1997-1999 continue to share a common vision and commitment to improving access to health information for teens and their parents. This shared vision evolved over time and began with the cooperative THINK LSCA project in 1994-1995. The realization among a group of libraries and community agencies that a "second generation" of Aurora youth required health information was the basis for renewed dialogue in Aurora and DLS (Howrey, 1998b). These prospective members of the new partnership perceived a "performance gap" in delivering authoritative health information to teens and parents in a timely manner, and the brainchild that arose, the TCN, was a vehicle to change and fix the problem. In preparing the grant, Provena Mercy Center and the partnership members developed plans for health-information delivery system change and improvement through the creation of a website, materials
245 acquisition by library partners, WICs in area libraries, community health-education programs targeted specifically to teens and parents, and professional networking among youth service professionals. Strengths of the Case-Study Approach, AR Methods, and Theoretical Constructs Employed The primary strength of the TCN case-study research resides in the creation of a new "professional networking" organization for agencies serving youth in the Aurora area. The TCN steering committee meetings were a regular forum for agencies to share information about their programs and learn from other agencies. A "learning community" was formed when the TCN steering committee brought together youth services professionals. Several partners interviewed in 30-minute exit interviews indicated they were amazed at the clear direction and "working group" nature of the steering committee. The TCN steering committee did not just talk--it saw a need, reflected on the need, and took decisive action--an unusual trait for a young organization. The multiple data sources and triangulation strategy employed in the case study--comparing meeting minutes, informal observations, partnering behaviors survey, program evaluation surveys, and exit interviews--supported the conclusions drawn about the benefits of the partnership to involved member agencies. A second strength of the research project was the rapid expansion of the partnership through community outreach activities. Open systems theory was quite effective when put into operation. The sheer increase in members from 15 to 40 (167.0%) and the greater diversity of partner agencies (including the Urban League; Breaking Free, Inc.; Aunt Martha's Youth Services; Aurora Township Youth Services; Communities in Schools; Fox Valley Girl Scouts; and several churches) recruited over
246 a short time period are strong indicators of the impact of the project in the greater Aurora area. The partnership expanded geographically from Aurora proper into Batavia, northern Kane County, Kendall County, and DuPage County. The current Leadership Team is preparing several grants for funding of TCN programs during the 2000-2001 school year, knowing that such grant-writing activities and networking will sustain the partnership into the future. Personal communication and monthly meeting attendance for partner agencies are key sources of energic input for the partnership as an open system. The scope of information products developed by the TCN partnership is a third indicator of the impact and overall strength of the project. Membership brochures, bookmarks with the TCN website address (http://www.aurora.il.us/ teencare) and "Pledge of Nonviolence," the Teens CARE About... Newsletter, the "Annotated Bibliography of Materials Added" found on the website, and the updating and electronic publication of the Healthy Teens Handbook (Kane County INFO, 1994), available just in time for teens and parents on the website, reflect the variety of materials selected by the library partners and developed for use by teens and parents. These products clearly reflect on the benefits of the partnership to teens, parents, and professionals serving youth in improving access to commun-ity health-information resources. New knowledge was created when the Aurora Schools YRBS was completed in June 1998. This information was compiled by the project director with input from the steering committee and published electronically on the TCN website for community-wide distribution. As a result of using the standardized YRBS in Aurora from the Centers for Disease and Control, other communities can directly compare their youth risk behavior results as a community with the 1998 Aurora results. The
247 TCN is seen by the member agencies, which include DLS and the Illinois State Library, as a model program for other communities to adopt and adapt to meet local needs. The community education programming is a fourth strength of the TCN partnership. As the quality of all the programs offered was rated high by those in attendance, it is accurate to report that the community education programming on teen health concerns was a strength of the project in spite of "low numbers." TCN was envisioned as a way of increasing access to health information for teens and parents, and the programs offered were selected to accomplish this important goal. Several of the programs are now available on video so interested teens, parents, and professionals have access to violence prevention strategies and effective parenting methods. The "media blitz" resulted in multiple channels of communication over the 18-month grant to fill the gap in access to community health information. A fifth program strength was the development of the TCN website and the "free" health-information services provided on the site. The Webmaster received several confidential teen health questions via e-mail, and these questions were referred to the appropriate health-care professionals or agencies. The website statistics for hits on the homepage show that there were over 1,400 visitors to the homepage from Fall 1998 to Fall 1999. This represents nearly 110 visitors to the homepage each month. Using data provided by the Aurora Online Community Network (AOCN) as a comparison, the project director, through triangulation, found that these homepage "hit" statistics did not depict the entire TCN website usage. In the peak months of library research, the total numbers were significant. In October 1998, there were 303 user sessions, 783 page views, and 1,148 hits via search engines for the TCN site. And in March 1999, there were 610 user sessions, 1,491
248 page views, and 3,433 hits for the entire site. The AOCN WebTrends reports demonstrate a much higher level of use than the hit counter on the TCN homepage shows. And about one third of users return to the TCN site. Users were getting some real benefits from the free health-information sources made available through the website--resource dependency theory fits the observations drawn. The presence of free health-information databases on the TCN website was a definite plus for stimulating traffic. Tables 14 and 15 illustrate that visitors to the TCN's website were using both the Health Reference Center and Ebsco's Health Source Plus. A future direction suggested by this website usage data for the TCN is having the Leadership Team seek out grant funding for a citywide license for Ebsco's Health Source Plus full-text database. A sixth TCN program strength was the collection development activities made possible with grant funds at the individual libraries. The TCN partner librarians reported that individual students and classes were using the materials acquired with LSTA funds. High in-house library use was reported in contrast to the actual checkout of materials. Teens desire their privacy, and the TCN librarians expressed the importance of confidentiality in handling questions from teens for health information. This pattern of in-house library use was reported by both school and public librarians. School librarians reported that health education, health occupations, and psychology classes were using the LSTA materials added extensively. Social exchange and resource dependency theory suggest that the librarians will continue to be involved in the partnership with significant benefits gained for students, teachers, and library collections and services. Marilyn Wolf, Jefferson Middle School librarian, reported that her circulation figures doubled for the month of October 1998 as a result of adding the TCN books to
249 her collection. She stated, "Students have a sixth sense when new books are available. The books purchased have circulated extremely well. Students need to have this type of `help book' available, and students need to know others have the same problem as they do." A health education teacher from Jefferson Middle School also wrote, It's [video] a very useful and valuable supplement to our human sexuality curriculum. Parent input, when we were redesigning our eighth-grade curriculum, wanted more abstinence ideas and promotion. This one video was an important part of that change. Thanks so much for the necessary resources and support that brought this video for use in the classroom. Students are beginning to believe that abstinence is an important part of their value system and behavior. To provide a total picture of the partnering behaviors demonstrated within the TCN partnership, a structured checklist with open-ended questions was mailed to over 40 professionals involved in the partnership. The structured checklist, "How Well Did We Partner?", was adapted from Sujansky (1991) and proved to be a useful tool for evaluation of the partnership's operations and partnering behaviors. The semistructured exit interviews also provided an opportunity for reflection on the partnership's strengths and weaknesses and areas for future improvement. This case study provided a good opportunity to experiment with the Sujansky (1991) partnership tool for operating a partnership, interacting with member agencies, and assessing overall effectiveness. This tool proved to be invaluable and can be adapted to other partnerships for assessment purposes. The Partnering Behaviors survey captured some of the "networking" dynamics of the relationships that evolved in the collaborative, library/community agency partnership. The survey measured observations about overall "willingness to collaborate" and "adaptive efficiency," key theoretical constructs that apply to all partnerships.
250
Limitations of the Research Project The weaknesses of the TCN partnership are identified as follows: 1. TCN needed a professional marketing firm to help the partnership systematically approach the local media. The TCN project director was unable to build rapport with the media because her role in the grant was a "jack-of-all-trades." As a result, participant turnout for education programs was lower than expected. More attention needed to be paid to informal, "word-of-mouth" advertising versus the more formal marketing channels employed. Peacemaking and nonviolence programs require a more personalized and persuasive marketing approach than print media are able to produce. 2. TCN media visibility was low in general with the news media and the community at large. As an example, we discovered that the mission was unclear from the name. One parent at the 1998 Project Unity Back-to-School Fair commented that she thought the group was a "babysitting service." 3. Public libraries needed encouragement to link community education programs to TCN resources. For example, Dreyer Medical Clinic staff were interested in linking physicians with public libraries to present health programs, but few direct contacts were made between the public library partners and Dreyer Medical Clinic's key contact person. Free advice from local physicians would have been appreciated by both teens and parents. 4. The "grassroots collegial approach" employed in the grant failed to generate interest among Aurora's "influentials" to become directly involved in the TCN partnership and contribute resources to ensure its future operations. Administrative support from the agency executives was questionable at times.
251 5. Digital imaging technologies did not become a "comfortable" part of the website development project. Because no internal expert on digital imaging surfaced from within the partnership, as project director, I relied on external consultants to provide training and technical advice on hardware and software to add web-based multimedia components. We learned scanning and still digital photography, but newness of digital video technology caused us to miss a few needed pieces (specifically an internal video editing board) that would allow us to edit images taken with the Canon ZR camera purchased. It was a frustrating and humbling experience for both myself as project director and the external consultants. As a result, TCN has not yet incorporated video clips into its website due to a shortage of operating funds. 6. For the TCN partners who did not regularly attend steering committee meetings, communication and connection strongly hinged on mailings and formal communications (e.g., newletters). Several partners noted in exit interviews that they needed to "renew" their relationship to the group as a result of nonattendance. One partner indicated she needed to attend meetings to be "more involved in building and sustaining valued partnerships." The connection of some of the partners to the "working group" was uncertain and fragile. 7. The TCN needs to focus more on advocacy and a proactive stance on health policy issues of importance to the group--gun control legislation, media violence, smoking prevention, abstinence, and substance abuse--and become involved in advocacy through such events as the Million Moms March on Mother's Day 2000 (http://www.millionmommarch.com). 8. The TCN partners need to investigate and evaluate whether applying for 501 (c) (3) not-for-profit status is a sound financial strategy. Currently, the partnership cannot accept contributions on its own.
252 9. The involvement of classroom physical education and health education teachers is needed across the city of Aurora to increase awareness of the website and resources available for teens and parents.
The Future of Health Promotion in the Greater Aurora Community The amount of direct involvement with the YWCA (October 1998 and October 1999), Fox Valley Park District (June 1999), Aurora Township Youth Services (January 1999+), and Breaking Free, Inc. (January 1999+) was an unanticipated consequence of the excitement created by the TCN partnership in the greater Aurora community. The grant activities moved from a hospital-based project to a stronger community-wide health-information network with a focus on youth violence prevention and safety concerns. The Kane County Health Department became more involved in Winter 199899, as our TCN steering committee discussed adolescent pregnancy programming, women's health, and suicide prevention. The Kane County Health Department was awarded a Women's Health grant from the Illinois Department of Public Health, and the TCN plans to participate in Health Department programs offered to female students in the Aurora schools served. A joint Provena Mercy Center and Rush-Copley (1998) PRC Aurora Community Health Assessment confirmed that fitness, nutrition, and violent crime have a significant impact on the community's overall health and well-being, so the TCN needs assessment was validated through this larger assessment effort by the hospitals with adult community members. The PRC Aurora Community Health Assessment also noted that the Aurora area continues to compare unfavorably to the
253 U.S. overall for murder, rape, and aggravated assault/battery rates. Both the povertystricken and Hispanic communities in particular suffer from high levels of crime in the Aurora area (Provena Mercy Center & Copley-Rush, 1998). Provena Mercy Center is hoping to address the needs of the Hispanic community with the development of a parish nursing program at St. Nicholas Church Aurora's east side during 1998 and in other Catholic and Protestant churches in 1999 and 2000. A total of nine parish nurses will be hired by the Provena Mercy Center program for local Aurora parishes. After three years of operation, the TCN partnership has conducted an evaluation of its 1999-2000 program activities and has implemented strategic planning for the coming 2000-2001 school year. The partnership has several new members on its Leadership Team that wrote grants to support prevention activities with at-risk youth in Kane, Kendall, and DuPage counties. The partnership now totals 41 members, and the strategic focus for program activities in 2000-2001 is "Tobacco-Free Youth" and a week devoted to teen mentors working with middle and elementary schools to discuss the health risks associated with tobacco smoking. Dreyer Medical Clinic, the American Cancer Society, and Provena Mercy Center are supporting this collaborative initiative with students attending public and private schools. From the viewpoint of the primary investigator, suggestions for future AR and action learning projects for the review and consideration of the TCN Leadership Team and professionals serving teens in the Aurora schools include: 1. Administering the YRBS to seniors in 2000-2001 who were freshmen in 1997-1998; 2. Having high-school students in the health occupations classes work with the available data to analyze Aurora youth risk behaviors and present their findings to the Boards of Education;
254 3. Initiating a study circle on the spirituality and practice of active nonviolence (Butigan, 1999); 4. Identifying and networking with other successful community network partnerships identified by the American Library Association to profile and document effective programs and services supporting community change and improvement (Bajjaly, 1999).
AR and the Quest for Safe Communities This case study and the AR methods employed have helped local Aurora professionals reflect on their practice, collect data about youth risk behaviors and potential services, and create alternative ways to improve health-information delivery and practice. This AR project was concerned with continuous improvement, youth development, professional self-renewal, and planned community change (Schmuck, 1997). The primary investigator used triangulation and multiple data sources to establish the credibility of the case report for the audiences in the academic and practice communities we hoped to reach. The TCN, as an AR study, examined a problem of local significance. Yet the problem of community violence and effective school safety responses are a pressing national concern. As I complete writing the case-study results reported here, the first anniversary of the Columbine High School tragedy reminds me of the importance of this "learning organization" experience. The lessons learned by our partners and "model partnership" have both practical and moral implications for other American communities. Building circles of peace, hope, and justice is an important community undertaking. It is hoped that the research methods employed and partnership
255 evaluation models introduced in this study will have value for community mobilization efforts across America. A visit to the TCN website at http://www.aurora.il. us/teencare is a first step in the right direction. Visitors take notice: it was a group of librarians and libraries, joining hands in leadership and unity with other committed health and social service agencies, that built a "Utopian Health-Information Network" here in Aurora. We believe that the TCN will continue to contribute to a safer Aurora community and the healthy and productive futures of all our citizens.
POSTSCRIPT Confronting Helplessness in the Face of Violence Through Action and Hope Three years after six-year-old Nico Contreras was shot to death on November 10, 1996, the case remains unsolved. Nico was sleeping when a gunman outside riddled the back wall and window of the boy's grandparents' wood-frame home on Aurora's near east side. At the time, the crime grabbed headlines and jostled parts of the community into action. Prayers were said, candlelight vigils were held, and antiviolence groups were formed. It has caused a 30year-old mother to fear for her children's lives in her parents' home. It has left an emptiness for Sandi, Nico's mother, as well as her parents, Mike and Maria Saltijeral, all of whom can no longer enjoy a rambunctious youngster who loved going to church. And it has caused all of them, frustrated over the fact that no one has been charged with the killing, to keep asking, "Who killed Nico?" (Chase, 1999, p. 1) Nico's death came at a time when Aurora already was dealing with two high-profile murders. Two years earlier, 19-year-old College of DuPage student Armando Mendez was beaten and fatally shot after his car ran out of gas. A few months later, Moshe Rogers, a 17-year-old Aurora Central Catholic High School basketball and track star, was fatally shot as he drove home from school after a basketball game. (Chase, 1999, p. 1) Reverend Dan Haas, pastor of Aurora Community Church and a long-time antiviolence advocate, said the three cases focused attention on Aurora's difficulties and spurred community action. "These were all young people looking forward to the best years of their lives and it got the community mobilized," Haas said. "These crimes highlighted a degree of vulnerability. We realized we're all susceptible to violence." (Chase, 1999, p. 1) In the years following Nico's death, Aurora has indeed made strides to stop the violence. Since the record year of 1996, the murder rate in Aurora has dropped by more than half. Eleven murders were reported in 1998, and through Friday, this year's [1999] total was eight. Much of the credit has gone to community groups. Some goes to the public schools, which have numerous antigang programs. "The number of people who now get involved [in antiviolence efforts] has increased greatly," Aurora police spokesman Dan Ferrelli said. (Chase, 1999, p. 1)
A Parting Reflection on Peacemaking
257 and Nonviolence from Gandhi We have to make truth and nonviolence not matters for mere individual practice but for practice by groups and communities and nations. That at any rate is my dream. I shall live and die in trying to realize it. My faith helps me to discover new truths every day. (Gandhi, 1982, p. 71)
REFERENCES Aldrich, H. E., & Pfeffer, J. (1979). Environments of organizations. In M. ZeyFerrell (Ed.), Readings on dimensions of organizations: Environment, context, structure, process and performance (pp. 3-27). Santa Monica, CA: Goodyear Publishing. Alexander, E. R. (1995). How organizations act together: Interorganizational coordination in theory and practice. Amsterdam, Australia: Gordon and Breach. Allen, B. (1992). Librarians and patrons: Partnerships for the '90s. Illinois Libraries, 74(1), 6-10. Alter, C., & Hage, J. (1993). Organizations working together. Newbury Park, CA: Sage Publications. American Academy of Pediatrics & American Psychological Association. (1995). Raising children to resist violence: What you can do. Elk Grove Village, IL: American Academy of Pediatrics. American Medical Association [AMA]. (1993, October). Advocacy brief: The impact of violence. Chicago, IL: AMA Division of Policy Communication, Group on Health Policy. American Medical Association [AMA]. (1996, August). Media use suggestions for parents. Chicago: AMA, Department of Mental Health. Appleby, J. (1995). Creating healthier communities: 25 pioneering models. Healthcare Form, 8(3), 43-54. Bajjaly, S. T. (1999). The community networking handbook. Chicago, IL: American Library Association. Baker, S. B., & Roberts, D. M. (1989). The factor structure of the problemsolving inventory: Measuring perceptions of personal problem solving. Measurement and Evaluation in Counseling and Development, 21(4), 157-164. Baniak, P. (1995, February 21). A community grieves: As loss of star youth sinks in, difficult task of healing begins. Chicago Tribune, Metro Southwest, p. 1. Barton, W. H., Watkins, M., & Jarjoura R. (1997). Youth and communities: Toward comprehensive strategies for youth development. Social Work, 42(5), 483493. Bazzoli, G. J., Stein, R., Alexander, J. A., Conrad, D. A., Sofaer, S., & Shortell, S. M. (1997). Pubic-private collaboration in health and human service delivery:
259 Evidence from community partnerships. Milbank Quarterly, 75(4), 533-561. Beaupre, B. (1998, May 5). Murders spark increase in Illinois' teen death rate. Chicago Sun-Times, p. 16. Bils, J. (1996a, November 13). Aurora again plans vigil for slain youth. Chicago Tribune, Metro DuPage Section, p. 1. Bils, J. (1996b, May 12). Aurora "Peace Summit" aims to fight gangs; Community to plan anti-crime strategy. Chicago Tribune, Metro DuPage Section, p. 1. Blau, P. M. (1970). Exchange theory. In O. Grusky & G. A. Miller (Eds.), The sociology of organizations: Basic studies (pp. 127-147). New York: Free Press. Blum, R. W., & Rinehart, P. M. (1997). Reducing the risk: Connections that make a difference in the lives of youth. Minneapolis, MN: University of Minnesota, Division of General Pediatrics and Adolescent Health. Bolland, J. M., & Wilson, J. V. (1994). Three faces of integrative coordination: A model of interorganizational relations in community-based health and human services. Health Services Research, 29(3), 341-366. Booth, B. (1999, January 4). Alliance ready for partnership with AMA against violence. American Medical News, 42(1), p. 1. Boyatzis, R. E. (1998). Transforming qualitative information: Thematic analysis and code development. Thousand Oaks, CA: Sage Publications. Bradshaw, L. K. (1998a). Interagency collaboration [online]. Greenville, NC: East Carolina University, Department of Educational Leadership. Available: http://150.216.8.1/leed/6801e.html Bradshaw, L. K. (1998b). Interagency collaboration: Preconditions, progress, and pressures [online]. Greenville, NC: East Carolina University, Department of Educational Leadership. Available: http://150.216.8.1/schofed/ leed/Interage.html Brener, N. D., Collins, J. L., Kann, L., Warren, C. W., & Williams, B. I. (1995). Reliability of the Youth Behavior Survey questionnaire. American Journal of Epidemiology 141(6), 575-580. Bryant, B. K. (1982). An index of empathy for children and adolescents. Child Development 53, 413-425. Buchanan, A. (1997, April 21). Grief finds a place on gym's wall: Portraits of slain students unveiled. Chicago Tribune, Metro Chicago, p. 1. Butigan, K. (1999). From violence to wholeness: A 10-part program in the spirituality and practice of active nonviolence. Las Vegas, NV: Pace e Bene Franciscan Nonviolence Center.
260 Butterfoss, F. D., Goodman, R. M., & Wandersman, A. (1993). Community coalitions for prevention and health promotion. Health Education Research, 8(3), 315330. Calloway, M., & Morrissey, J. P. (1993). Accuracy and reliability of selfreported data in interorganizational networks. Social Networks, 15(4), 377-398. Carr, W., & Kemmis, S. (1986). Becoming critical: Education, knowledge and action research. London: Falmer Press. Chase, J. (1999, November 15). Death's chill lingers; family lacks answers three years after boy's slaying. Chicago Tribune, Trib West, p. 1. Chavis, D. M. (1995). Building community capacity to prevent violence through coalitions and partnerships. Journal of Health for the Poor and Underserved, 6(2), 234-245. Cheadle, A., Wagner, E., Anderman, C., Walls, M., McBride, C., Bell, M. A., Catalano, R. F., & Pettigrew, E. (1998). Measuring community mobilization in the Seattle minority youth health project [online]. Evaluation Review, 22(6), 699-716. Available: http://ehostweb8.global.epnet.com/fulltext.asp Christian, S. E. (1998, July 26). New Rx from the nation's top doc. Chicago Tribune, 2-1, 2-3. Collins, B. W., & Sasser, A. B. (1997, April/May/June). Creating partnerships for the distribution of consumer health information. Virginia Libraries, 43, 4-6. Consumers go online for health care. (1999). CyberAtlas: The Web marketer's Guide to Online Facts [online]. Available: http://cyberatlas.internet.com/ markets/professional/article/0,1323,5971_153181,00.html Covey, S. R. (1997). The seven habits of highly effective families. New York: Golden Books. Crowl, T. K. (1993). Fundamentals of educational research. Madison, WI: WCB Brown & Benchmark. Dahlen, K. H. (1993). The status of health information delivery in the United States: The role of libraries in the complex health care environment. Library Trends 42(1), 152-179. Dardick, H. (1994, October 29). Aurora student slain near home. Chicago Tribune, News, p. 5. Dardick, H. (1995, February 27). Unity campaign aims to lift veil of racism. Chicago Tribune, Metro DuPage, p. 1. Dardick, H. (1997, October 28). Crosses help bear heavy burden of violence;
261 Murder victim's son-in-law teams with community in remembrances. Chicago Tribune, Metro Lake, p. 6. Dardick, H. (1998, June 19). School supplies program honored. Chicago Tribune, Metro DuPage, p. 3. Dardick, H. (1999, April 16). Aurora counts itself with cities in program to build character. Chicago Tribune, Trib West, p. 11. Deering, M. J. (1996). Partnerships for network health information for the public: Introduction (Symposium). Bulletin of the Medical Library Association, 84(2), 205-236. Deering, M. J., & Harris, J. (1996). Consumer health information demand and delivery: Implications for libraries. Bulletin of the Medical Library Association, 84(2), 209-216. Deye, D. L., Kahn, G., Jimison, H. B., Renner, J. H., Wenner, A. R., & Gabello, W. J. (1997). How computers enrich patient education. Patient Care 31(3), 88-99. DiBella, A. J., & Nevis, E. C. (1998). How organizations learn: An integrated strategy for building learning capacity. San Francisco, CA: Jossey-Bass. Dixon, N. (1994). The organizational learning cycle: How we can learn collectively. London: McGraw-Hill Book Company. Dolcini, M. M., Adler, N. E., & Ginsberg, D. (1996). Factors influencing agreement between self-reports and biological measures of smoking among adolescents. Journal of Research on Adolescence, 6(4), 515-542. Doz, Y. L., & Hamel, G. (1998). Alliance advantage: The art of creating value through partnering. Boston, MA: Harvard Business School Press. Dreyer Medical Clinic. (2000, Winter). Talk to a nurse one-on-one. The Pulse, 10(1), 4. Dryfoos, J. G. (1994). Full-service schools: A revolution in health and social services for children, youth and families. San Francisco, CA: Jossey-Bass. Dryfoos, J. G. (1998). Safe passage: Making it through adolescence in a risky society--what parents, schools, and communities can do. New York: Oxford University Press. Dwyer, K. P. (1998, June 28). Beyond the legal issues surrounding kids who kill is the moral dilemma of: How to prevent the next school massacre. USA Weekend, 17. East Aurora Schools District #131. (1998). 1998 school report card. Aurora, IL: East Aurora High School.
262 Elliott, D. S., Hamburg, B. A., & Williams, K. R. (1998). Violence in American schools: A new perspective. Cambridge, England: Cambridge University Press. Falcon, P. (1996, November 11). Boy, 6, shot while sleeping. Copley News Service, 1. Falcon, P., & Nelson, M. (1998, January 2). Aurorans join to stop violence at its source. Beacon News, A1, A4. Feinberg, S., & Feldman, S. (1996). Serving families and children through partnerships: A how-to-do-it manual. New York: Neal-Schuman Publishers. Fisher, M. (1992). Parents' views of adolescent health issues. Pediatrics, 90(3), 335-341. Galaskiewicz, J. (1985). Interorganizational relations. Annual Review of Sociology, 11, 281-304. Gall, C. F., & Miller, E. G. (1997). Strategic planning with multitype libraries in the community: A model with extra funding as the main goal. Bulletin of the Medical Library Association, 85(3), 252-259. Gamm, L. D. (1998). Advancing community health through community health partnerships. Journal of Healthcare Management, 43(1), 51-67. Gandhi, M. (1958). All men are brothers: Autobiographical reflections. New York: Continuum Publishing Company. Gandhi, M. (1982). The words of Gandhi. New York: Newmarket Press. Gardner, M. L. (1991). Business-school partnerships. Executive Excellence, 8(9), 11-12. Giloth, B., & Jellen, B. C. (1989). Improving adolescent health through community partnerships: Program manager's guide [KIT]. Chicago, IL: American Hospital Association. Gottlieb, N. H., Brink, S. B., & Gingiss, P. L. (1993). Correlates of coalition effectiveness: The smoke-free class of 2000 program. Health Education Research 8(3), 375-384. Grady, K. E., & Wallston, B. S. (1988). Research in health care settings. Newbury Park, CA: Sage. Gray, B. (1989). Collaborating: Finding common ground for multiparty problems. San Francisco, CA: Jossey-Bass. Greene, D. L. (1998, July 9). Clinton backs stalled bill aimed at keeping guns
263 from children. Baltimore Sun, 3A. Greenwood, D. J., & Levin, M. (1998). Introduction to action research: Social research for social change. Thousand Oaks, CA: Sage Publications. Gross, K. (1998). Baby TALK: Still growing a decade later. Illinois Libraries, 80(3), 124-128. Hall, R. H. (1999). Organizations: Structures, processes and outcomes (7th ed.). Upper Saddle River, NJ: Prentice-Hall. Hall, S. (1996). Reflexivity in emancipatory action research: Illustrating the researcher's constitutiveness. In O. Zuber-Skerritt (Ed.), New directions in action research (pp. 28-48). London: Falmer Press. Hamburg, M. A. (1998). Youth violence is a public health concern. In D. S. Elliott, B. A. Hamburg, & K. R. Williams (Eds.), Violence in American schools: A new perspective (pp. 31-54). Cambridge, England: Cambridge University Press. Handy, L. (1992). Serving youth through cooperative efforts. Illinois Libraries, 74(1), 24-25. Hannigan, G. G. (1997). Action research: Methods that make sense. Medical Reference Services Quarterly 16(1), 53-58. Hart, E., & Bond, M. (1995). Action research for health and social care: A guide to practice. Buckingham, England: Open University Press. Heppner, P. P. (1988). The problem-solving inventory: Manual. Palo Alto, CA: Consulting Psychologists Press. Hill, S. C. (1997). School-related violence: A secondary analysis of the Youth Risk Behavior Survey data (1993 and 1995). (Doctoral dissertation, Southern Illinois University, Carbondale, 1997). Dissertation Abstracts Internationl, 58-09A, 3434. (University Microfilms No. 9808823) Hord, S. M. (1985, January). Collaboration or cooperation: Comparisions and contracts, dilemmas, and decisions. Paper presented at the Meadow Brook Symposium on Collaborative Action Research in Education, Oakland University. (ERIC Document Reproduction Service No. ED 258 356) Howrey, M. M. (1994, March 21). THINK: Teen Health Information Network: An Aurora area partnership of public libraries, schools, and community agencies (unpublished LSCA grant proposal to the Illinois State Library). Aurora, IL: Mercy Center for Health Care Services and Aurora Public Library. Howrey, M. M. (1998a, August). Featured partner: The Aurora Police Department Juvenile Division. Teens CARE About... Newsletter, 1(1), 3.
264 Howrey, M. M. (1998b, January 23). Teen CARE Network: An Aurora partnership committed to action, respect, and excellence (unpublished LSTA grant proposal to the Illinois State Library). Aurora, IL: Provena Mercy Center. Howrey, M. M. (1998c, April). Teen CARE Network website [online]. Aurora, IL: Provena Mercy Center. Available: http://www.aurora.il.us/teencare Howrey, M. M. (1998d, November 24). Teen CARE Network Phase I: Final narrative report and final financial report. Aurora, IL: Provena Mercy Center. Howrey, M. M. (1999a, April/June). Featured partner program: Aurora Township Youth Services. Teens CARE About... Newsletter, 1(3), 3. Howrey, M. M. (1999b, February/March). Featured partner program: Character Counts! in Aurora. Teens CARE About... Newsletter, 1(2), 3. Howrey, M. M. (1999c, September 30). Teen CARE Network Phase II: Final report. Aurora, IL: Provena Mercy Center. Hughes, I. (1997). Action research electronic reader: Introduction [online]. Available: http://www.beh.cchs.usyd.edu.au/~arow/Reader/rintro.htm Humphries, A. W., & Kochi, J. K. (1994). Providing consumer health information through institutional collaboration. Bulletin of the Medical Library Association, 82(1), 52-56. Illinois Attorney General, Advisory Group on School Safety and Firearms. (1998, July). Safe 2 learn: School safety and firearms—Proposed initiatives. Springfield, IL: Office of the Attorney General. Illinois State Library. (1998). Long range plan for the use of library services and technology act (LSTA) funds--1997-2002 [online]. Springfield, IL: Illinois State Library. Available: http://www.library.sos.state.il.us/news/lstalrp. html Illinois Violence Prevention Authority. (1998). Building a safe Illinois: A state plan for violence prevention. Chicago: The Authority. Intel, health care leaders explore "Internet gap" between doctors and patients. (1999, October 12). Business Wire [online]. Available: http://finance. individual.com/display_news.asp?doc_id=BW19991012BW1328] Jick, T. D. (1979). Mixing qualitative and quantitative methods: Triangulation in action. Administrative Science Quarterly, 24, 602-611. Joint Commission on the Accreditation of Healthcare Organizations. (1998). 1998 hospital accreditation standards. Oakbrook Terrace, IL: The Commission.
Kaluzny, A. D., Zuckerman, H. S., & Ricketts, T. C. (Eds.). (1995). Partners
265 for the dance: Forming strategic alliances in health care. Ann Arbor, MI: Health Administration Press. Kane County Health Department. (1997). Violence prevention/control services of Kane County. Geneva, IL: Health Department. Kane County INFO. (1976). Senior handbook. Aurora, IL: Author. Kane County INFO. (1994). Healthy teens handbook (1st ed.). Geneva, IL: Community Contacts. Kane County INFO. (1996). Directory of human services for Kane County (6th ed.). Aurora, IL: Author. Kann, L., Kinchen, S. A., Williams, B. I., Ross, J. G., Lowry, R., Hill, C. V., Grunbaum, J., Blumson, P. S., Collins, J. L., & Kolbe, L. J. (1998). Youth risk behavior surveillance--United States, 1997. MMWR, 47(SS-3), 1-92. Kanter, R. M., & Eccles, R. G. (1992). Making network research relevant to practice. In N. Nohria & R. G. Eccles (Eds.), Networks and organizations: Structure, form, and action (pp. 521-527). Boston, MA: Harvard Business School Press. Kappeli, S. (1995). Interprofessional cooperation: Why partnership is so difficult. Patient Education and Counseling, 26, 251-256. Katz, D., & Kahn, R. L. (1978). The social psychology of organizations (2nd ed.). New York: John Wiley & Sons. Kerka, S. (1997). Developing collaborative partnerships [online]. Columbus, OH: ERIC Clearinghouse on Adult, Care, and Vocational Education, Ohio State University. Available: http://www.ericacve.org/docs/collab.htm Kock, N. F., Jr., McQueen, R. J., & Scott, J. L. (1997). Can action research be made more rigorous in a positivist sense? The contribution of an iterative approach [online]. Journal of Systems and Information Technology, 1(1), 1-24. Available: http://www.parnet.org/PARchive/bibliodetail.cfm?id=453 Kolar, C. (1999, June 5). About the Aurora Online Community Network [online]. Aurora, IL: Aurora University. Available: http://www.aurora.il.us/ about.html Kolbe, L. J., Kann, L., & Collins, J. L. (1993). Overview of the Youth Risk Behavior Surveillance System. Public Health Reports, 108(Supplement 1), 2-10. Kuzel, J., & Erickson, S. (1995). Teen Health Information Network (THINK). Illinois Libraries, 77(4), 157-182. Lantieri, L., & Patti, J. (1996). Waging peace in our schools. Boston, MA: Beacon Press.
266 Lash, S. (1998, July 1). Gun-control group asks health-care workers to teach firearm safety. Houston Chronicle, A-12. Lasley, T. J. (1994). Teaching peace: Toward cultural selflessness. Westport, CT: Bergin & Garvey. Lester, W. (2000, April 21). Locking up triggers: Poll finds many Americans want stricter gun enforcement. Beacon News, A-12. Lipman-Blumen, J., & Leavitt, H. J. (1999). Hot groups: Seeding them, feeding them, and using them to ignite your organization. New York: Oxford University Press. Longe, M. E., & Thomas, K. (1998). Consumer health resource centers: A guide to successful planning and implementation. Chicago: American Hospital Publishing. Maack, M. N. (1997). Toward a new model of the information professions: Embracing empowerment. Journal of Education for Library and Information Science, 38(4), 283-302. Mager, R. F., & Pipe, P. (1984). Analyzing performance problems, or you really oughta wanna (2nd ed.). Belmont, CA: Lake Publishing Company. Mattessich, P. W., & Monsey, B. R. (1992). Collaboration: What makes it work; A review of research literature on factors influencing successful collaboration. St. Paul, MN: Amherst H. Wilder Foundation. Maxwell, J. A. (1998). Designing a qualitative study. In L. Bickman & D. J. Rog (Eds.), Handbook of applied social research methods (pp. 69-100). Thousand Oaks, CA: Sage. Mays, G. P., Halverson, P. K., & Kaluzny, A. D. (1998). Collaboration to improve community health: Trends and alternative models. Joint Commission Journal on Quality Improvement, 24(10), 518-540. McCain, W. J., & Stratton, B. F. (1994). Planning and partnering for healthier communities. Journal of Health Care Marketing, 14(4), 8-9. McGill, I., & Beaty, L. (1995). Action learning (2nd ed.). London: Kogan Page. McGinnis, J. (1993). Educating for peace and justice: Religious dimensions, grades 7-12. St. Louis, MO: Institute for Peace and Justice. McGinnis, J. (1998). A call to peace: 52 meditations on the Family Pledge of Nonviolence. Liguori, MO: Liguori Publications. McGinnis, J., Lovingood, K., Lovingood, G., & Vogt, J. (1996). Families
267 creating a circle of peace: A guide for living the Family Pledge of Nonviolence. St. Louis, MO: The Institute for Peace and Justice. McGinnis, J., & McGinnis, K. (1998, June 19-20). Building the peaceable community, school, and family [video]. Aurora, IL: Video Perfection. McTaggart, R. (1991). Principles for participatory action research. Adult Education Quarterly, 41(3), 168-187. Medical Library Association. (1996a). The crisis of violence in America: Challenges for health sciences librarians to respond to the need for interdisciplinary collaboration to address violence (cassette recording No. 05-1149-96). Alexandria, VA: Audio Manuscripts. Medical Library Association. (1996b). The librarian's role in the provision of consumer health information and patient education. Policy statement of the Medical Library Association and the Consumer and Patient Health Information Section (CAPHIS/MLA). Bulletin of the Medical Library Association, 84(2), 238-239. Merriam, S. B. (1998). Qualitative research and case study applications in education. San Francisco, CA: Jossey-Bass. Miles, M. B., & Huberman, A. M. (1984). Qualitative data analysis: A sourcebook of new methods. Beverly Hills, CA: Sage. Millard, S. K. (1999). How Delaware education and policy leaders define a successful university/state K-12 education partnership: A state K-12/university library online. Newark, DE: University of Delaware. Millstein, S. G., Nightingale, E. O., Petersen, A. C., Mortimer, A. M., & Hamburg, D. A. (1993). Promoting the healthy development of adolescents. JAMA, 269(11), 1413-1415. Nagle, E. (1996). The new knowledge environment: Quality initiatives in health sciences libraries. Library Trends, 44(3), 657-674. National Education Goals Panel. (1995). The national education goals report: Building a nation of learners, 1995 [online]. Washington, DC: National Education Goals Panel. Available: www.negp.gov/negp/ Newbold, P. A. (1998). Improving community health status. Healthcare Executive, 13(1), 48-49. Noddings, N. (1984). Caring: A feminine approach to ethics and moral education. Berkeley, CA: University of California Press. Noddings, N. (1992). The challenge to care in schools: An alternative approach to education. New York: Teachers College Press. Noddings, N. (1996). The caring professional. In S. Gordon, P. Benner, & N.
268 Noddings (Eds.), Caregiving: Readings in knowledge, practice, ethics, and politics (pp. 160-172). Philadelphia, PA: University of Pennsylvania Press. Nohria, N. (1992). Is a network perspective a useful way of studying organizations? In N. Nohria & R. G. Eccles (Eds.), Networks and organizations: Structure, form, and action (pp. 1-22). Boston, MA: Harvard Business School Press. Oliver, C. (1990). Determinants of interorganizational relationships. Academy of Management Review, 15(2), 241-265. Osborn, R. N., & Hagedoorn, J. (1997). The institutionalization and evolutionary dynamics of interorganizational alliances and networks. Academy of Management Journal, 40(2), 261-278. Pelton, T. (1994, November 21). 750 make joyful noise for peace. Chicago Tribune, Chicagoland, p. 1. Pennbridge, J. N. (1988). Interorganizational relations: An ethnographic assessment of the resource dependency model. Unpublished doctoral dissertation, University of California, Los Angeles. Plaut, T., & Landis, S. (1992). Enhancing participatory research with the community oriented primary care model: A case study in community mobilization. American Sociologist, 23(4), 56-70. Potts, C. (1999, June 28). Keep our kids safe. American Medical News, 42(24), 22-23. Prothrow-Stith, D. (1996). Violence: A public health crisis. Healthcare Forum Journal, 39(5), 17-21. Prothrow-Stith, D. (1997). A stitch in time (Harvard School of Public Health Assistant Dean Deborah Prothrow-Stith discusses violence prevention). Hospitals & Health Networks, 71(4), 16. Provan, K. G., & Brinton, M. H. (1995). A preliminary theory of interorganizational network effectiveness: A comparative study of four community mental health systems. Administrative Science Quarterly, 40(1), 1-33. Provena Mercy Center & Rush-Copley Medical Center. (1998). PRC Community health assessment. Omaha, NE: Professional Research Consultants. Provena Mercy Center Library. (1998a, March 13). Teen CARE Network minutes. Unpublished proceedings. Provena Mercy Center Library. (1998b, July 20). Teen CARE Network minutes. Unpublished proceedings. Provena Mercy Center Library. (1998c, September 14). Teen CARE Network
269 minutes. Unpublished proceedings. Provena Mercy Center Library. (1999, April 5). Teen CARE Network minutes. Unpublished proceedings. Putting the information infrastructure to work: Health care and the national information infrastructure. (1994). Bethesda, MD: Agency for Health Care Policy and Research. Ramsey, R. D. (1997). Networking in the '90s: Another survival tool for supervisors. Supervisor, 58(5), 9-12. Reason, P. (1994). Three approaches to participative inquiry. In N. K. Denzin & Y. S. Lincoln (Eds.), Handbook of qualitative research (pp. 324-339). Thousand Oaks, CA: Sage. Recardo, R., Molloy, K., & Pellegrino, J. (1995). How the learning organization manages change. National Productivity Review, 15(1), 7-13. Rees, A. M. (1991). Managing consumer health information services. Phoenix, AZ: Oryx Press. Rees, A. M. (1995). Consumer health USA: Essential information from the federal health network. Phoenix, AZ: Oryx Press. Rees, A. M. (1998). Consumer health information source book (5th ed). Phoenix: Oryx Press. Resnick, M. D., Bearman, P. S., Blum, R. W., Bauman, K. E., Harris, K. M., Jones, J., Tabor, J., Beuhring, T., Sieving, R. E., Shew, M., Ireland, M., Bearinger, L. H., & Udry, J. R. (1997). Protecting adolescents from harm: Findings from the National Longitudinal Study on Adolescent Health. JAMA, 278(10), 823-832. Ring, P. S., & Van de Ven, A. H. (1994). Developmental processes of cooperative interorganizational relationships. Academy of Management Review, 19(1), 90-118. Rolls, J. (1995). The transformational leader: The wellspring of the learning organization. In S. Chawla & J. Renesch (Eds.), Learning organizations: Developing cultures for tomorrow's workplace (pp. 101-108). Portland, OR: Productivity Press. Roth, A. (1997, December 28). Offering prayers for peace. Beacon News, A3. Roth, A. (1998, November 7). Message of hope: Bright future class strives to help teens see possibilities. Beacon News, A3. Rowley, J. (1997). The library as a learning organization. Library Management, 18(2), 88-91.
270 Saltiel, I. M. (1998). Defining collaborative partnerships. New Directions for Adult and Continuing Education, 79, 5-12. Sarason, S. B., & Lorentz, E. M. (1998). Crossing boundaries: Collaboration, coordination, and the redefinition of resources. San Francisco, CA: Jossey-Bass Publishers. Savenye, W. C., & Robinson, R. S. (1996). Qualitative research issues and methods: Introduction for educational technologists. In D. H. Johnassen (Ed.), Handbook of research for educational communications and technology (pp. 11711195). New York: Simon & Schuster Macmillan. Scherer, M. J., & McKee, B. G. (1993, April 12-16). Participatory action research (PAR): What it is, what is isn't, how it's done, what you get. Paper presented at the Annual Meeting of the American Educational Research Association, Atlanta, GA. (ERIC Document Reproduction Service No. ED 359 224) Schmuck, R. A. (1997). Practical action research for change. Arlington Heights, IL: IRI/Skylight Training and Publishing. Schön, D. A. (1983). The reflective practitioner: How professionals think in action. New York: Basic Books. Scott, C. M., & Thurston, W. E. (1997). A framework for the development of community health agency partnerships. Canadian Journal of Public Health, 88(6), 416420. Sgroi, A., & Saltiel, I. M. (1998). Human connections. New Directions for Adult and Continuing Education, 79, 87-92. Sherlock, B. (1995, August 14). School fair puts kids on equal footing. Chicago Tribune, Metro DuPage, 3. Smith, S. E. (1997). Deepening participatory action research. In S. E. Smith, D. G. Willms, & N. A. Johnson (Eds.), Nurtured by knowledge: Learning to do participatory action-research (pp. 173-263). New York: Apex Press. Stake, R. E. (1994). Case studies. In N. Denzin & Y. S. Lincoln (Eds.), Handbook of qualitative research (pp. 236-247). Thousand Oaks, CA: Sage. Stake, R. E. (1995). The art of case study research. Thousand Oaks, CA: Sage. Stapleton, S. (1999, January 25). Cities take aim at gun industry. American Medical News, 41(2), 1, 30.
Stiffman, A. R., Earls, F., Dore, P., Cunningham, R., & Farber, S. (1996). Adolescent violence. In R. J. DiClemente, W. D. Hansen, & L. E. Ponton (Eds.),
271 Handbook of adolescent health risk behavior (pp. 289-312). New York: Plenum Press. Stolovitch, H. D., & Keeps, E. J. (Eds.) (1992). Handbook of human performance technology: A comprehensive guide for analyzing and solving performance problems in organizations. San Francisco, CA: Jossey-Bass Publishers. Strauss, A., & Corbin, J. (1990). Basics of qualitative research: Grounded theory, procedures, and techniques. Newbury Park, CA: Sage Publications. Stringer. E. T. (1996). Action research: A handbook for practitioners. Thousand Oaks, CA: Sage. Sujansky, J. G. (1991). The power of partnering: Vision, commitment, and action. San Diego, CA: Pfeiffer & Company. Sullivan, T. J. (1998). Collaboration: A health care imperative. New York: McGraw-Hill. Survey shows propensity for youth violence, Part 1. (1999, July). Nation's Health, 29(6), 16. Teens CARE about... Newsletter. (1998/99). Aurora, IL: Provena Mercy Center. Top 50 websites of September 1999 (1999, November 10). Cyberatlas: The big picture: Traffic patterns [online]. Available: http://cyberatlas.internet.com/ big_picture_traffic_patterns/article/0,1323,5931_219781,00.html Tremblay-McGaw, R. (1999). Part of the solution: Librarians work to stop gun violence. American Libraries 30(8), 56-58. United States Public Health Service. (1995). Healthy people 2000: National health promotion and disease prevention objectives--Midcourse review and 1995 revisions. Washington, DC: U.S. Department of Health and Human Services, Public Health Service. United Way of the Aurora Area. (1995, January 1). An assessment of Aurora area needs. Aurora, IL: United Way. United Way of the Aurora Area. (1996, August). 1996 Needs assessment survey. Aurora, IL: United Way. Van de Ven, A. H., & Ferry, D. L. (1980). Measuring and assessing organizations. New York: John Wiley & Sons.
Wang, M. C., Haertel, G. D., & Walberg, H. J. (1993). School-linked services: A research synthesis. Philadelphia, PA: National Education Center on Education in the Inner Cities. (ERIC Document Reproduction Service No. ED 399 314)
272 Watkins, K. E., & Marsick, V. J. (1993). Sculpting the learning organization: Lessons in the art and science of systemic change. San Francisco, CA: Jossey-Bass. Weick, K. E. (1979). The social psychology of organizing (2nd ed.). New York: McGraw-Hill. Weick, K. E. (1995). Sensemaking in organizations. Thousand Oaks, CA: Sage. Weiler, R. M., Sliepcevich, E. M., & Sarvela, P. D. (1993). Development of the adolescent health concerns inventory. Health Education Quarterly, 20(4), 569-583. West Aurora Schools District #129. (1998, October). West High School 1998 report card. Aurora, IL: West Aurora Schools. Whyte, W. F. (1991). Participatory action research. Newbury Park, CA: Sage. Wiley, D. C., James, G., Furney, S., & Jordan-Belver, C. (1997). Using the Youth Risk Behavior Survey to compare risk behaviors of Texas high school and college students. Journal of School Health, 67(2), 45-49. Wilson, A. M. (1990). Interorganizational networking as a community-based approach to adolescent pregnancy and teen parenting: A case study. New York: City University of New York. Winter, R. (1996). Some principles and procedures for the conduct of action research. In O. Zuber-Skerritt (Ed.), New directions in action research (pp. 13-27). London: Falmer Press. Womack, S. T. (1997). What action research is: A review of the literature [online]. Available: http://firstsearch.oclc.org/:next+NEXTCM (ERIC Document Reproduction Service No. 414 255) Yin, R. K. (1994). Case study research: Design and methods (2nd ed.). Thousand Oaks, CA: Sage. Young, L. (1996, March 7). Witness recounts slaying of Rogers. Chicago Tribune, Metro DuPage, 1. Young Women's Christian Association [YWCA]. (1999). YWCA week without violence: Steering committee meeting minutes. Aurora, IL: Author. Yuchtman, E., & Seashore, S. E. (1979). A system resource approach to organizational effectiveness. In M. Zey-Ferrell (Ed.), Readings on dimensions of organizations: Environment, context, structure, process, and performance (pp. 291307). Santa Monica, CA: Goodyear Publishing. Zammuto, R. F. (1984). A comparison of multiple constituency models of
273 organizational effectiveness. Academy of Management Review, 9(4), 606-616. Zuber-Skerrit, O. (1996). Emancipatory action research for organisational change and management development. In O. Zuber-Skerritt (Ed.), New directions in action research (pp. 83-105). London: Falmer Press.
APPENDICES
APPENDIX A AURORA SCHOOLS YOUTH RISK BEHAVIOR SURVEY (YRBS); LETTER TO BUILDING PRINCIPAL; TEST ADMINISTRATION INSTRUCTIONS; AND QUESTIONNAIRE, MAY 1998
276 April 30, 1998
Dear Aurora Building Principal: The Teen CARE Network, which evolved from the Teen Health Information Network (THINK) partnership of libraries and social service, health and educational agencies in 1994-95, has been meeting since November 1997. The partnership is committed to gathering information about teen health concerns and developing programs for improved access to health information for teens and their parents. On April 13th, George H. Ryan, Secretary of State, announced that Provena Mercy Center Medical Library and theTeen CARE Network library partnership were awarded a Library Services and Technology Act (LSTA) grant from the Illinois State Library. To fulfill our important mission of improved access to health information for the Aurora community, we are seeking your assistance and cooperation in gathering information about the current health status of Aurora teens. A Youth Risk Behavior Survey (YRBS), originally developed by the Centers for Disease Control, has been reviewed and modified by the Teen CARE Network Steering Committee for Aurora schools. The modified Aurora YRBS assesses teen health risk-taking and problem-solving. A copy of the Aurora Schools YRBS survey is enclosed for your review and for possible future review by interested school personnel and parents. We are asking that health education teachers and/or physical education teachers administer the YRBS to freshmen students during a regularly scheduled class period. We hope to have over 1700 Aurora freshmen participate in the YRBS, but a signed parent consent form is required to be on file with the classroom teachers for teens prior to the day of YRBS administration (see the enclosed consent form). We anticipate that the YRBS survey will take approximately 30 minutes of class time. Students absent on the day of administration will not be able to complete the survey later. Copies of the parent consent form,YRBS, NIU scantron forms, and pencils will be provided in sufficient quantities for classroom teachers administering the survey. It is important that teachers inform individual students about the need for privacy and confidentiality of their YRBS responses. All completed consent forms, scantron forms and YRBS surveys will be placed in a brown envelope and sealed by the classroom teacher. Sealed envelopes are to be returned to: Mary Howrey, Project Director, Teen CARE Network, Provena Mercy Center Medical Library, 1325 N. Highland Avenue, Aurora, Illinois, 60506. We look forward to working with you and your teachers in assessing teen health behaviors and in developing health information resources in the Aurora community for teens and their parents. Sincerely,
Mary M. Howrey Medical Librarian 630-801-2686 630-801-2687 (FAX) E-Mail:
[email protected]
277 yrbsscov.doc
278 Aurora Schools Youth Risk Behavior Survey (YRBS) Administrator Instructions, May 1998 Page 1 1.Assign a class period for administration of the YRBS to the students in your class. The estimated time for completion of the YRBS is 30 minutes. 2.Explain the benefits to your high school and the student body by having students answer the 100 questions about their health behaviors, learning style and learning media preferences. 3.Each student is required to have his/her parent complete and sign a Parent Consent form. Instruct your students to write in the test date and date by which the Parent Consent form is to be returned to you at school. 4.IMPORTANT: Only students with a signed consent form indicating parent approval of participation may complete the YRBS. There is NO penalty to the student for non-participation in the survey. However, you may award students extra credit for completing the YRBS. 5.Check to be sure that sufficient copies of the YRBS questionnaire, NIU answer sheets and Number 2 pencils are available for your students. 6.READ ALOUD these instructions to your students about the YRBS questions. a.Your school is precoded in the Miscellaneous Section on the front of the form. b.Record your answers to the 100 questions on the back of the answer sheet. The YRBS questions are numbered 101-200 and match with the numbers and responses found on this side of the NIU Testing Service answer sheet. c. Do NOT write your answers on the questionnaire itself. d. Use the Number 2 pencil provided by your teacher. e.Blacken the circle on the answer sheet that matches the number of the question. f. Erase all marks and corrected answers completely. g.Answer all questions on the survey with the one response that best describes your behavior or attitude toward the health issue. h.Do NOT code your name on the front side or sign your name on the second page of the answer sheet. This will guarantee that your responses are kept confidential.
Aurora Schools Youth Risk Behavior Survey (YRBS)
279 Administrator Instructions, May 1998 Page 2 7.READ ALOUD to your students the YRBS test instructions found on the front page of the survey. Stress the CONFIDENTIAL nature of each student's responses to the survey. IMPORTANT INSTRUCTIONS TO FOLLOW-This survey is about health behavior. It has been developed so you can tell us what you do that may affect your health. The information you give will be used to develop better health education for young people like yourself. DO NOT write your name on this survey. The answers you give will be kept private. No one will know what you write. Answer the questions based on what you really do. Completing the survey is voluntary. Whether or not you answer the questions will not affect your grade in this class. The questions that ask about your background will only be used to describe the types of students completing this survey. The information will not be used to find out your name. No names will ever be reported. Make sure you answer every question. Fill in the ovals completely on the answer sheet provided. When you are finished, follow the instructions of the person giving you the survey. 8.Have the students return the completed answer sheets and surveys to you. Place all these forms in the brown envelope provided. Seal the envelope and return the envelope to your school librarian. Any questions about the survey can be directed to: Mary M. Howrey, Medical Librarian, Provena Mercy Center Medical Library, 1325 N. Highland Avenue, Aurora, Illinois, 60506, Phone: 630-801-2686. 9.The Number 2 pencils are a gift from the Teen CARE Network partnership supported with a LSTA grant from the Illinois State Library.
Yrbsadmi.doc/5/03/98
280 Youth Risk Behavior Survey
281
282
283
284
285
286
287
APPENDIX B INFORMED CONSENT FORMS FOR YOUTH RISK BEHAVIOR SURVEY AND EXIT INTERVIEWS
289 Teen CARE Network YRBS Survey CONSENT FORM Northern Illinois University LEPS/LEIT Department, DeKalb, Illinois, 60115 Dear Aurora Parent, Your teen is invited to participate in a survey project being conducted by the Teen CARE Network, a partnership of 15 Aurora educational, health and social service agencies. Mary Howrey, Medical Librarian, is the Project Director and a graduate student at Northern Illinois University. The purpose of the Teen CARE Network is to improve access to health information for all teens and their parents in Aurora. Your teen will be asked to answer the Aurora Schools Youth Risk Behavior Survey (YRBS), a series of 100 questions originally developed by the Centers for Disease Control to determine possible teen health risks including nutrition, tobacco use, alcohol and other drug use, physical activity and fitness, injuries, sexual behavior, STDs and pregnancy. The Youth Risk Behavior Survey (YRBS) has the approval of state and local officials and has received the support of many national organizations including the National PTA and the National Catholic Educational Association. A copy of the YRBS is available in your school principal's office and district office for your review prior to the date of theYRBS administration. There are no risks to your teen in answering the questions anonymously. Your teen and classmates will benefit from improvements in health education classes at your high school, in the development of an Aurora Teen CARE Network Internet site, and by the addition of new learning materials added to Aurora libraries. These improvements are possible as a result of an Illinois State Library (LSTA) grant to our local Aurora public, school, college and medical libraries. To gain the most benefit from what we learn in Aurora, Teen CARE Network success stories will be shared with librarians at professional meetings throughout the state of Illinois. Any information shared will guarantee the privacy of your teen and classmates. It is very important that all selected students participate. However, the decision to participate is voluntary. Your decision and that of your teen to participate in the project will not affect you or your teen. Your teen will be asked to indicate his/her willingness to participate on the day of survey administration without penality and can decline to answer questions at that time. **Please sign and date this form and have your teen return this signed form to his/her school by this date: ________________. The survey will be conducted on: ______________________. If you would like further details about the project, contact: Mary Howrey, Teen CARE Network Project Director, Provena Mercy Center Medical Library, 1325 N. Highland Avenue, Aurora, Illinois, 60506, Phone: 630-801-2686. Thank you for promptly completing and returning this consent form to your teen's school.
YES, I agree to allow my teen to participate in the Teen CARE Network research project and acknowledge that I have received a copy of this consent form. ________________________________________________ ___________________ Signature of Parent/Guardian Date NO, I do not wish my teen to participate in this Teen CARE Network research project. ________________________________________________ __________________ Signature of Parent/Guardian Date
290
291 Teen CARE Network Program Evaluation Partner Release Form As a member of the Teen CARE Network partnership, I grant Mary Howrey, Project Director of the Teen CARE Network LSTA Project, permission to utilize partnership evaluation data gathered during a face-to-face interview with me. This data will be used in completing her Ed.D. doctoral research at Northern Illinois University, Department of Instructional Technology. I understand that any information provided will be analyzed to ensure the anonymity of my responses to interview questions and the confidentiality of the information I provide about the partnership. I also will be given an opportunity to review transcripts of the interview session and final manuscript to validate the content and findings communicated to the academic and professional community. As a partner in the Teen CARE Network, I have voluntarily chosen to participate in the final evaluation phase of the project, plan to discuss the preliminary project results generated at a future Teen CARE Network Steering Committee meeting, and anticipate receiving a final summary of the evaluation results from the Teen CARE Network Project Director.
____________________________________________ _______________ Participant Signature Date ____________________________________________ Participant Name _____________________________________________________________ Partner Agency Any questions about this release form can be directed to either Mary Howrey, Information Specialist at Nicor Gas Corporate Library, 630-983-8676, x. 2190, or Dr. Rhonda Robinson, Professor at Northern Illinois University, LEIT Department, DeKalb, IL, 60115, 815-753-9323. tcnreleaseform.doc 7/10/99
APPENDIX C EXIT INTERVIEW QUESTIONS, JULY-SEPTEMBER 1999
293 Interview Questions for Teen CARE Network Program Exit Evaluation Sessions In June and July 1999, a structured survey was distributed to the 39 partner agencies involved in the Teen CARE Network. The cover letter notified the partners of a change in leadership and requested that the survey form and Interview Release Form be returned to Provena Mercy Center Library. As of September 10, 18 partners returned the "How Well Did We Partner?" survey. A total of 18 Teen CARE Network Program Evaluation Partner Release Forms were returned to indicate that a number of partners were willing to spend a minimum of one-half hour discussing their involvement in and perspectives of the effectiveness of the partnership. During July, August and September 1999, 18 interviews were conducted that varied in length from 25 minutes to 1-1/2 hours. The average length of an interview was 35 minutes. The first two interviews were conducted in an "unstructured" manner. The interviewer covered the concepts identified in the structured, mailed survey but did not use specific questions in advance to guide the interview. After the investigator transcribed the first interview session, it became apparent that it was necessary to ask a series of general questions so that a comparative analysis could be made between the partners interviewed. The questions that guided 16 of the later interviews are: 1.What is the function or purpose of your agency? 2.Why did your agency become a partner in the Teen CARE Network? 3.What benefits do you perceive your agency gained from the partnership? 4.In your opinion, what obstacles did the partnership experience in fulfilling its mission? 5.How successful was the Teen CARE Network Partnership partnership in
294 accomplishing its primary mission? 6.
What is your vision for the partnership in the next year?
7.What advice do you have for other groups wanting to form a partnership?
APPENDIX D GRAY'S PARTNERSHIP DEVELOPMENT MODEL: TEEN CARE NETWORK PARTNERSHIP TIMELINE, 1997-2000
296 Phase One: Problem Setting October 1997 Discussions with Lynn Elam of DuPage Library System, Mary Hauge, WAHS and Ginny Koch, Provena Mercy Center Focus Group Meeting at West Aurora High School with librarians, teachers, guidance counselors, school nurse and social worker (Survey results) November 1997 Youth Needs Focus Group Meeting, West Aurora High School (Minutes) Literature review conducted on teen risk behaviors and health information needs December 1997 Teen CARE Network is named Letters solicited from community agencies, health care providers, libraries and schools for LSTA grant application Community needs assessments obtained from United Way, Kane County Health Department and Crisis Line/INFO Phase Two: Direction Setting January 1998 Letters of support received from 15 partners Teen CARE Network Steering Committee holds first meeting Meeting with Provena Mercy Center Administrative Team to finalize grant application and obtain final approval Illinois State Library grant submitted February 1998 MS FrontPage '98 selected as Web Site development package of choice based on Aurora University recommendations and Waubonsee Community College training available March 1998 Illinois State Library awards $64,800 grant to Provena Mercy Center for Teen CARE Network partnership April 1998 Teen CARE Network Web site development begins on Aurora University Web server May 1998 Street Smarts: Straight Talk for Kids, Teens and Parents presented by J.J. Bittenbinder, on May 4 at Provena Mercy Center (N=400) YRBS assessment conducted at Aurora high schools (East Aurora, Rosary High School and West Aurora High School)
297 Phase Three: Implementation June 1998 Fox Valley Today interview about Teen CARE Network, June 6, TV 30, Plano Building the Peaceable Community, School and Family Program Clothesline Project on display at Provena Mercy Center, Social Work MSW Intern assists with Healthy Teen Handbook input on Web site Health Reference Center subscription begins for Teen CARE Network Web site July 1998 FAVAN meeting held at Provena Mercy Center Library, July 13 Membership database and mailing list developed with codes, July 2 August 1998 Project Unity Back-to-School Fair, August 15 (N=1600) Grant application made to Illinois State Library for Phase II Illinois Council for Violence Prevention Holds Quarterly Meeting at Provena Mercy Center, August 13, 1998 Teens CARE AboutNewsletter, Volume 1, Number 1, August 1998 Wellness Information Units Shipped to Partner Libraries for 1998-1999 School Year September 1998 Teen CARE Network has 23 partners Teen CARE Network Web site operational (www.aurora.il.us/teencare) for 1998-99 School Year Teen CARE Network has a booth at the Urban League's "Do the Right Thing", September 19 Parenting Teens: From Rebellion to Responsibility, September 28 - October 19 October 1998 Community Resource Fair Booth, Aurora Community Center, October 3 Digital Camera Meeting, DLS and ITS, Inc., at Provena Mercy Center Library, October 16 YWCA Week Without Violence, October 18 -24 ILA Poster Session on the Teen CARE Network, October 26 "Peace Sheets" distributed to interested Aurora high schools and middle schools as a YWCA Week Without Violence activity "Once Upon a Crime East" Aurora High School Honors Drama Class presentations, October 19-23, to elementary students and Aurora Community Study Circles reaches nearly 1100 Aurora east side students and community members Community Resource Team Resource Fair Booth, October 31 November 1998 Teen CARE Network has 25 partners Teen CARE Network Phase II awarded $40,000 LSTA grant Teens CARE AboutNewsletter distributed to health librarians at HSLI Conference, November 6
298 December 1998 IAEC Session on the Teen CARE Network, December 11 Bibliography of Materials Acquired loaded onto Web site, December 23 (N=400) January 1999 Teen CARE Network has 30 partners Internet training session at DLS on Internet Consumer Health Resources, January 6, for librarians Seven Habits of Highly Effective Families presented at Kane County Prevention Council's Parent University, January 30, by Jonathan Switzer, Youth Minister with Aurora Community Church (N=35) February 1999 Teen CARE Network has 32 partners Teens CARE AboutNewsletter, Volume 1, Number 2, February/March 1999 issued Teen CARE Network booth at DuPage/Kane Teacher Institute Day, February 26 Teen CARE Network receives "Organizing Award" from the Institute of Peace and Justice, St. Louis, MO, February 27 Digital Camera Loan Policy Draft, February 8, at TCN Steering Committee Meeting March 1999 Cartoon Contest Announced in Beacon News on March 8 Chicago Tribune, Trib West article on Teen CARE Network, March 12 Brother Bill Tomes program on Gang Violence Prevention, March 14 Statewide Teleconference on the Teen CARE Network, March 17 Teens CARE AboutNewsletter, Volume 1, Number 3 mailed to 9500 Aurora homes with teens Illinois State Library places Teen CARE Network grant on their web site under "Grants You Wish You Thought of" Teen CARE Network has 37 partners "Peace Sheets" exhibit available for loan to interested organizations April 1999 Teen CARE Network Partners interviewed on Fox Valley Today TV 30, Plano, 4/6 Chicago Tribune article on HealthWorks Theatre production, 4/8 Healthworks Theatre Production of "silence.com" on 4/11 (during National Library Week) (N=40) Kids Count, Too!! (Broadcast on 4/12 and 4/16), video of Dr. Phillip Jacobson's 1/2 hour presentation about effective parenting and resilient children Cartoon Contest receives 60 cartoon submissions Building the Peaceable Community, School and Family on Aurora Cable Channel 6 on April 14 (National Library Week) Moms and Dads: Let's Talk, Provena Mercy Center, April 26, for parents of middle school girls on physical and emotional changes of puberty Ebsco Health Source Plus to Replace Health Reference Center, April 26, TCN Steering Committee Meeting TCN Membership Brochures (N=2000) and Bookmarks (N=10,000) Produced May 1999 Dr. Thomas Phelan presents "Surviving Your Adolescents" on 5/1 (N=30)
299 Seven Habits of Highly Effective Families presented by Renee Souba, LCSW, at St. Joseph School to 40 parents and teachers on 5/18 (N=40) June 1999 Starting Out Right workshop for teen moms and dads canceled and rescheduled for 10/99 Safe Night USA and "MWAH!" for Aurora middle school students, June 5-6, Fox Valley Park District (N=60) TCN ListServ set up on Aurora University web server, June 14 Materials orders due, June 30 TCN elects officers, June 28, at TCN Steering Committee meeting TCN Mailing List=1100, June 28 July 1999 Teen CARE Network has 39 partners August 1999 Teens CARE AboutNewsletter, Volume 2, Number 1, August 1999 is produced online at www.aurora.il.us/ teencare Project Unity Back to School Fair, August 14 (N=1700) September 1999 Teen CARE Network and Breaking Free presents Dr. Samuel Betances on "Making Winners Out of Would be Losers," at East Aurora High School, September 13 (N=65) Teen CARE Network has 40 partners Parenting Teens: From Rebellion to Responsibility, 9/27/99- 10/18/99, Provena Mercy Center LSTA grant project ends, September 30 October 1999 Jim and Kathy McGinnis present "Starting Out Right: Nurturing Young Children as Peacemakers" on October 19 at the YWCA Teen Adolescent Program (TAP) Parenting for Peace and Justice presented at Copley Theatre, October 19 (N=25) Teen CARE Network Recognized by DuPage Library System with the 1999 Millennium Service Award ($1000), October 21 Safe Night II, 10/23/99, 5 p.m. - Midnight, Fox Valley Park District (N=60) February 2000 American Cancer Society joins Teen CARE Network (N=41) Parenting Teens: From Rebellion to Responsibility, 2/7/2000 - 2/28/2000, Provena Mercy Center Open Line: When Parents and Teens Connect, 2/15/2000, East Aurora High School May 2000 Is It Too Late? How to Recognize Signs of Substance Abuse in Teens, 4/27/2000, East Aurora High School Under Development Cable Public Service Announcement--Teen CARE Network Services West Aurora High School 30-60 second PSA
300 Fundraising to Date $500 Grant from Dreyer Medical Clinic (to East Aurora HS for Peace Play expenses) (10/98) $500 Grant from Exchange Club (8/99) $5000 Grant from Breaking Free from Illinois Department of Human Services/Criminal Justice Grant for Prevention of Juvenile Delinquency (7/99) $200 Matching Grant from Nicor Gas Employee (Provena Mercy Center Foundation) 8/99 Ask-an-Expert Grants (2) (West Aurora High School Library) on health education themes Funders' Consortium grant application, 1/21/2000,
APPENDIX E TEEN HEALTH CONCERNS INVENTORY
APPENDIX F PARTNERING BEHAVIORS SURVEY, JUNE-JULY 1999
303 Partner Agency________________________________________ Date__________ How Well Did We Partner? Assess the effectiveness of Teen CARE Network partnering practices by circling one of these responses, 1=Strongly Agree 2=Agree 3=Neutral, 4=Disagree 5=Strongly disagree, or NA=Does not apply or Don't know, to each of the following questions. Return the survey to: Provena Mercy Center Library, 1325 N. Highland Avenue, Aurora, IL, 60506, by July 20, 1999. Part 1: Use of the Partnering Operating Model Vision 12345
NA
We shared a clear vision of what we wanted to accomplish.
12345
NAWe understood how our activities fit into the big picture of prevention and health information needs in the Aurora area.
Commitment 12345
NA
We shared a commitment to our TCN mission and goals.
12345
NAWe believed in making a difference in providing health information to Aurora area teens and their parents.
Action 12345
NA
We set clear goals for the TCN partnership.
12345
NAWe defined our roles and responsibilities as contributing partners.
12345
NA
We established realistic time lines to accomplish our tasks.
12345
NA
We determined diagnostic methods to use.
12345
NA
We communicated throughout the process.
12345
NA
We determined the resources needed to accomplish our goals.
12345
NA
We defined the evaluation process.
12345
NA
We specified our agreements and policies in writing.
Diagnosing 12345
NAWe used a variety of diagnostic techniques (focus groups, checklists, interviews, needs assessments).
12345
NA
We collected and analyzed Aurora teen risk behaviors data.
304 Making Decisions 12345
NA
We summarized the information gathered in diagnosis.
12345
NAWe recommended various courses of action for the partnership.
12345
NA
We provided written documentation of the recommendations.
12345
NA
We outlined specific plans and time lines for all involved.
12345
NA
We established checkpoints to monitor our progress.
12345
NAWe evaluated the results we achieved in our services and programs offered.
12345
NAWe established a plan for health information service improvements.
Implementing
Part 2: Use of Partnering Behaviors 12345
NA
We assessed our willingness to partner.
12345
NAWe were honest about our strengths and weaknesses and interacted effectively with one another.
12345
NAWe discussed our preferred working styles and contributions to the partnership.
12345
NAWe chose partners who contributed knowledge, talents and resources.
12345
NAWe involved others in health information service improvements.
12345
NAWe created an environment of openness and trust for all involved.
12345
NA
We challenged one another.
12345
NA
We took necessary risks.
12345
NA
We shared information, skills, authority and resources.
12345
NA
We found opportunities and empowered others.
12345
NAWe solved problems creatively and sought opportunities and encouraged others to do so.
12345
NAWe managed the unique and different contributions of partners.
305 12345
NA
We listened actively to one another's viewpoints.
12345
NA
We managed disagreements and conflicts appropriately.
12345
NAWe kept one another informed throughout via scheduled meeting times, regular mailings, e-mail and telephone.
12345
NA
12345
NAWe shared information about the partnership with those we served and actively marketed TCN services.
12345
NA
12345
NAWe evaluated the partnering relationship throughout the project.
12345
NA
We mutually agreed to any changes that needed to be made.
We fulfilled all agreed-on responsibilities.
We recognized and celebrated our successes.
306 Part 3: Use of Partnering and the Partnership Model (1)What am I doing well in practicing partnering? What are my greatest strengths?
(2)Where would I choose to make modifications and/or improvements in my partnering practices?
(3)What am I doing well in developing partnerships? What are my greatest strengths?
(4)
Where could I choose to make modifications and/or improvements?
(5)How has my agency and I benefited from Teen CARE Network partnering project activities?
(6)What should be the continuing vision of the TCN partnership over the course of the next year?
(7)What resources and programs are needed to accomplish your suggested vision for the Teen CARE Network over the course of the next year?
APPENDIX G PROGRAM EVALUATION FORMS
309
310
APPENDIX H TEEN CARE NETWORK WEBSITE HOMEPAGE AND BIBLIOGRAPHY OF MATERIALS (SAMPLE PAGES) ADDED BY TEEN CARE NETWORK MEMBER LIBRARIES FOUND ON WEBSITE
311
312
313
314
315
316
317
318 Pamphlet Inventory Life Skills Education (Publisher) Selected titles include Abstinence. 1997 Abusive Women. 1997 Access to Better Health. 1997 Adolescent Sexuality. 1996 Adult Children of Alcoholics. 1997 AIDS and the Heterosexual Community. 1997 AIDS and Minorities. 1997 AIDS: The Social Impact. 1997 AIDS: Understanding the Epidemic. 1997 Alcohol at Work. 1997 Alcohol and How It Affects Driving. 1997 Alcohol And Seniors. 1997 Alcohol and the Student Athlete. 1997 Alcohol and the Teenage Drinker.1997 An Alcoholic in your Life. 1997 Alcoholism and the Family.1997 Anger. 1996 Anorexia. 1996 Assertiveness. 1997 Attention Deficit Disorder. 1997 Birth Control. 1995 Breaking Up. 1997 Bulimia. 1996 Caffeine. 1997 Cancer. 1996 Caring. 1997 Child Abuse. 1996 Child Neglect. 1997 Childhood Stress. 1996 Cocaine. 1997 Codependency. 1996 The Computerized Job search. 1997 Coping with Family Stress. 1997 Coping with Unemployment. 1997 Crack. 1997 The Cycle of Life. 1996 Dating. 1995 Date Rape. 1996 Dating Violence.1996 Deciding About Sex. 1995 Depression. 1995 Domestic Abuse. 1996 Drinking Myths. 1997 Drugs and the Student Athlete. 1997 Effective Goal Setting. 1997 Ending an Addiction. 1997
319 Facing A Drug Problem. 1996 Feeling Lonely. 1996 Fetal Alcohol Syndrome. 1997 Food... for Thought. 1997 Gambling. 1997 Getting Along. 1995 Getting Over a Violent Relationship. 1997 Going It Alone. 1997 Growing Self- Esteem. 1997 Herpes. 1995 HIV Testing. 1997 How Alcohol Affects your Body. 1997 How to Assess Your Drinking. 1997 How to Choose Your Doctor. 1997 How to Get a Good Night's Sleep. 1996 How to Handle Peer Pressure. 1995 How to Say No. 1997 How not to Quit Smoking. 1997 Hypertension. 1996 Incest. 1996 Inhalants. 1997 The Interview. 1997 An Introduction to Asthma. 1997 An Introduction to Arthritis. 1997 An Introduction to Diabetes. 1996 An Introduction to Infertility. 1997 An Introduction to Stress. 1996 About the Jobs. 1997 Juvenile Delinquency. 1996 Living with AIDS. 1997 Living with an Alcoholic Parent. 1997 Living with Your Teenager. 1995 Looking Back, Moving Forward. 1997 Lowering Your Cholesterol. 1995 LSD. 1997 Making Friends. 1997 Managing Your Worries. 1997 Marijuana: An Introduction to the Facts. 1997 Marijuana: The Personal Effects. 1997 Marijuana And Driving. 1997 Marijuana and Your Health. 1997 The Mature Resume. 1997 Medical Tests.1996 Mental Illness.1996 Mixing Alcohol with Drugs. 1997 Narcotics. 1997 New Kid on the Block. 1997 Obesity. 1996 Over the Counter Drugs. 1997 Parents, Families, and Child Abuse. 1996
320 PCP. 1997 Positively. 1996 Pregnant Too Soon. 1995 Pre-Natal Care. 1996 Problem Drinking. 1997 Prejudice. 1996 Prescription Drug Abuse. 1997 Preventing Elder Abuse and Neglect. 1997 Puberty. 1995 Puberty for Girls. 1995 Questions Teens Ask ... About Sex. 1996 Rape. 1996 The Recovering Alcoholic. 1997 Rules of the Road. 1995 Safer Sex. 1997 Secondhand Smoke. 1997 Sexual Abuse of Children. 1996 Sexual Harassment: It's Not Part of the Job! 1997 Sexual Harassment: One of the Lessons You Learn in School? 1997 Smoking and Your Kids. 1997 Step-Parenting. 1997 Steroids. 1997 Straight Talk about Drugs. 1997 Street Smarts. 1996 Tanning. 1995 Talking with Children. 1996 Teenagers and AIDS. 1997 Teen Gangs. 1996 The Teenage Alcoholic. 1997 Teenage Marriage. 1996 Teaching Values. 1996 Tobacco. 1997 Understanding Alzheimer's Disease. 1995 Understanding Fetal Alcohol Syndrome. 1997 Understanding Homosexuality. 1996 Understanding Suicide. 1995 Unwed Fathers. 1995 Uppers And Downers. 1997 VD and STD's. 1995 Violence in America. 1996 Violent Kids, Violent Schools. 1996 The Way Out for Abused Women. 1997 What is Addiction? 1997 When You Love an Alcoholic. 1997 Witness to Violence. 1997 Women and Aids. 1997 Women and Alcohol. 1997 Your Child's Behavior and You. 1997 You and Your Heart. 1996 You and Your Phobias. 1996
321 You and Your Self-Image. 1995 You and Your Values. 1996 The Young Drinking Driver. 1997 Youth and Suicide. 1995 Krames Communications (Publisher) Examen Papanicolaou. (Pap smear). 1993 Having a Baby. 1997 Las Primeras Semanas De Su Bebe. (Baby's First Weeks). 1996 Tener un Bebe. (Having a baby). 1997 Your Baby's First Weeks. 1996 Your Pap Exam. 1997 Breastfeeding Your Baby. 1996 Healthy Mom, Healthy Baby. 1996 Is Smoking Worth It? 1996 Librese Del Estres. (Emotional Stress). 1991 Vale la pena fumar? (Teens Say No to Smoking). 1996 Waiting for the Right Time. 1996
APPENDIX I TEEN CARE NETWORK PARTNER AGENCIES, SEPTEMBER 1999
323
Teen CARE Network Partner Agencies (N=40) September 1999 1.
Aunt Martha's Youth Services
2.
Aurora Area Interfaith Food Pantry
3.
Aurora Central Catholic High School
4.
Aurora East School District #131
5.
Aurora Police Department
6.
Aurora Public Library
7.
Aurora Township Youth Services
8.
Aurora University
9.
Aurora West School District #129
10.
Batavia High School
11.
Batavia Public Library
12.
Breaking Free/Family Support Center
13.
Communities in Schools
14.
Crisis Line of the Fox Valley/INFO, A Program of the Association for Individual Development
15.
Dreyer Medical Clinic
16.
DuPage Library System
17.
Family Counseling Service
18.
First Presbyterian Church
19.
Fox Valley Girl Scout Council
20.
Fox Valley Park District
21.
Greater Dupage MYM
22.
Holy Angels Church & School
23.
Illinois Dept. of Human Services/Teen Services
324
24.
Kane County Health Department
25.
Kane County Region Office of Education
26.
Kane County SHOCAP
27.
KDK Training, Employment & Business Services
28.
Marmion Academy
29.
Messenger Public Library of North Aurora
30.
New England Congregational Church
31.
Northern Illinois University
32.
Our Lady of Good Counsel Church & School
33.
Parents Anonymous
34.
Provena Mercy Center
35.
Quad County Urban League
36.
Rosary High School
37.
Sugar Grove Public Library
38.
Visiting Nurse Association of Fox Valley
39.
Wesley United Methodist Church
40.
YWCA
Note: These schools are accessing the TCN Web site for health information based on inquiries received, but are not formally involved as "partners"-Glenbard East High School Streamwood High School Wheaton Central High School
APPENDIX J TEEN CARE NETWORK DIGITAL CAMERA POLICY AND LOAN AGREEMENT FORM
326 Teen CARE Network (TCN) Policy Statement 1999 - 2000
To encourage use of the digital imaging equipment added under the 1998 LSTA Teen CARE Network project, the following guidelines have been adopted regarding the loan of digital cameras and maintenance of equipment to Teen Care Network partner members: 1.Provena Mercy Center houses, maintains and lends the three Sony Mavica FD7 digital cameras and the Canon ZR digital video camera. The regular loan period for digital cameras acquired under the LSTA grant is one week. This loan period may be extended with permission of Provena Mercy Center Library staff. Provena Mercy Center staff provide training to TCN partner members on the basic use of the still digital cameras. Partners provide their own 3-1/2 inch disk for use in the digital cameras (either IBM-format or MacIntosh format). One camera is always available on-site at Provena Mercy Center. 2.A twenty-five-dollar refundable deposit is required for loan of digital cameras. The preferred payment method is a check. The refundable deposit is returned to the patron when the camera is returned, inspected by a Library staff member, and the staff member confirms that the camera is in excellent working condition. 3.Borrowers of the digital still cameras or digital video camera sign a Digital Camera Loan agreement form that specifies the responsibilities of the borrower and TCN. This agreement remains in effect for one year from the date which appears on the agreement form.
327 Teen CARE Network (TCN) Digital Camera Loan Agreement Form: Borrower & TCN Responsibilities ----------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------This agreement applies for a period of one year between the Teen CARE Network (TCN), owner of the still digital camera or digital video camera, and the individual borrower of this TCN equipment ______________________________________________________________________. (Name of the Borrower) (DLS Member Library or TCN Partner) The digital cameras are the property of the Teen CARE Network as acquired under the 1998 Library Services and Technology Act (LSTA) grant with funds provided by the Illinois State Library, a division of the Office of the Secretary of State. (1)The borrower of the digital camera agrees to accept responsibility for safe return and/or replacement of digital camera equipment to TCN responsible parties. (2)The borrower agrees to return the equipment by the agreed upon return date. A fine of $2 per day will be charged for late return of equipment to the loaning agency (Provena Mercy Center). (3)The loan period is one week from the receipt of the equipment. However, the loan period may be extended with permission of TCN responsible parties at Provena Mercy Center Library. (4)The borrower agrees to supply TCN responsible parties with a $25 personal or agency check which is refundable upon the safe return of the equipment. The check is refunded when a responsible TCN party determines the equipment is in excellent working condition. (5)TCN responsible parties will provide training on the basic use of the digital cameras. TCN will inspect the cameras prior to loan and upon their return to determine that the cameras are in excellent operating condition. Borrowers are requested to report any malfunctions in equipment to TCN responsible parties. (6)The borrower will provide the IBM- or MacIntosh-formated disk upon which digital images are recorded. TCN will have available for purchase digital video cassettes for recording of full motion video images. Agreed to by:______________________________________________________ (Signature of Borrower) Printed Name of Borrower) TCN Partner Organization__________________________________________ Work Address______________________________ Work Phone____________ Home Phone___________________________ Today's Date________________ Approved by:_________________________________ (Provena Mercy Center)
On the reverse side, please identify the anticipated uses or applications of the camera for your library or TCN partner agency: