Rectus Sheath, Fascia Transversalis & Pre-Peritoneal Fat/ Fascia during .... Contemporary issues of human anatomy related to the posterior rectus sheath, ...
A Study of Laparoscopic Surgical Anatomy of Infraumbilical Posterior Rectus Sheath, Fascia Transversalis & Pre-Peritoneal Fat/ Fascia during TEPP Mesh Hernioplasty for Inguinal Hernia
A Thesis Submitted for the award of the Degree of DOCTOR OF PHILOSOPHY In SURGERY By DR. MAULANA MOHAMMED ANSARI MBBS, MS (Surgery) Department of Surgery Faculty of Medicine, Jawaharlal Nehru Medical College Aligarh Muslim University, Aligarh – 202002, UP, INDIA
May, 2016
Chapter I - Introduction
M. M. Ansari
Chapter - 1
Introduction
CHAPTER – I INTRODUCTION, CONTEMPORARY ISSUES & PRESENT STRATEGY It is humbling to realize that even today basic anatomy may not be known or all understood. (Patrick C Walsh, 1998)
1.1. INTRODUCTION “The study of anatomy has changed enormously in the last few decades. No longer do medical students have to spend long hours in the dissecting room searching fruitlessly for the otic ganglion or tracing the small arteries that form the anastomosis round the elbow joint. They now need to know only the basic essentials of anatomy with particular emphasis on their clinical relevance, and this is a change that was long overdue” (Faiz and Moffat, 2011). “Familiarity with fascia and its specialized arrangements is a very great help to the surgeon in any field, but especially in operations in the inguinal region. … the surgeon trained in conventional transinguinal exploration (for hernia repair) may find himself unfamiliar with the fascial appearances encountered in the use of this alternative (preperitoneal) route” (Fowler, 1975). Contrary to the general belief, extraperitoneal anatomy of the groin is reported to be complex (Arregui, 1997; Lange, 2002), and is not properly understood by the majority of the practicing surgeons (Arregui, 1997; Colborn and Skandalakis, 1998; Lange et al, 2002; Faure et al; 2006), leading to difficulties in performing the 1
M. M. Ansari
Chapter - 1
Introduction
laparoscopic preperitoneal repair of the inguinal hernia, with a long learning curve (Liem et al, 1996; Faure et al, 2006), and leading to its lack of popularity despite the obvious advantages and better results (Lange et al, 2002). Inadequate understanding & improper dissection of the pre-peritoneal anatomy is now regarded as the main cause of difficulties during TEPP hernioplasty, especially in presence of the wide anatomic variations which received little/no attention of the anatomists & the practicing surgeons alike. In the light of such a multifarious scenario, the present study was undertaken with the hope to develop a clear understanding of the anatomy of groin and its adjacent areas, and to help in the creation of an easy surgical road-map towards the straightforward laparoscopic hernioplasty for the inguinal hernia.
1.2. HISTORICAL BACKGROUND & CONTEMPORARY ISSUES The conventional picture describes an incomplete posterior rectus sheath in the lower half of the abdomen with the existence of a sharp, concave downwards, lower border (known as Arcuate line of Douglas) due to shifting of the aponeuroses from the posterior to the anterior rectus sheath somewhere between the umbilicus and the pubic symphysis (Williams & Warwick, 1980; Moore, 1985; Last, 1985; Romanes, 1987; Moffat, 1987; Mwachaka et al, 2009) A sharp well-defined Arcuate line can appear only if all the fibres of posterior rectus sheath shift suddenly at a definite level but often the transition is gradual, incomplete or even totally lacking (Rizk, 1991). Way back in 1940, McVay & Anson wrote that "Descriptions of the rectus sheath contained in our textbooks of anatomy are singularly alike; they are stereotyped and oversimplified; when these accounts recognise structural variation at all, it is only in connection with the position of the linea semicircularis.", and since then it seems that little has changed (Monkhouse and Khalique, 1986). However, a footnote in the 35th edition of Gray's Anatomy (Warwick & Williams, 1973) did mention the different opinions of several investigators (Walmslay, 1937; McVay & Anson, 1940) that the general textbook description of the rectus sheath formation is not a common arrangement. This comment was incorporated into the main text in the later editions of the Gray’s Anatomy including the 40th edition (Standring, 2008). A bi-laminar concept of each of the three aponeuroses of the anterior abdominal wall was endorsed in its 41st edition (Standring, 2016), based on the earlier work of Rizk (1980), but the reference to the variation in the rectus sheath formation was simply deleted, although variation in the arcuate line was added. Current laparoscopic approach for hernioplasty demands precise knowledge of the posterior anatomy of the anterior abdominal wall, especially in the inguinal region. Gross preperitoneal 2
M. M. Ansari
Chapter - 1
Introduction
anatomy from the laparoscopic perspective is rarely reported (Quinn et al, 1995), and so is the case of the living surgical anatomy of the posterior rectus sheath and preperitoneal fascial tissues. Even after advent of the laparoscopic era, only one study, to the best of our knowledge, is reported in the English literature by Maurice E. Arregui (1997) who lamented that there remains not only little understanding but also little interest in the laparoscopic surgical anatomy of the inguinal region among the practicing surgeons. Moreover, occurrence of wide anatomic variations recently emphasized (Rizk, 1991; Mwachaka et al, 2009) may add to the misery of difficulties to the laparoscopic hernia surgeon if he/she is not familiar with the various anatomical features. Contemporary issues of human anatomy related to the posterior rectus sheath, arcuate line, transversalis fascia, pre-peritoneal fat and pre-peritoneal fascia in the inguino-pelvic region are briefly highlighted individually in the following paragraphs:
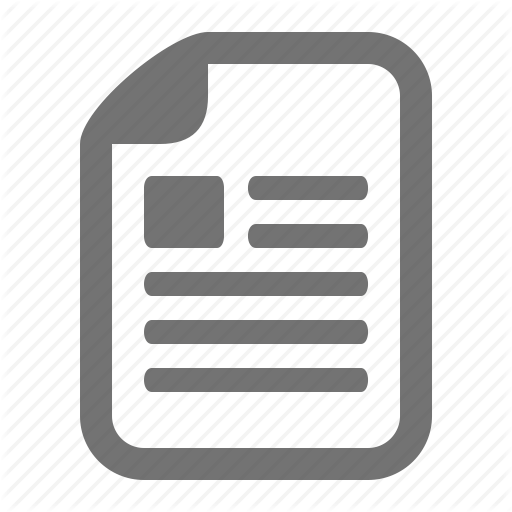
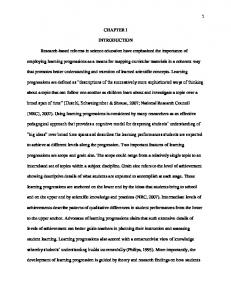
1.2.1. Variations in Posterior Rectus Sheath Considerable variations in the formation of the rectus sheath have been reported by several investigators from time to time since long (Schaefer & Dancer, 1894; Warwick & Williams, 1973; Rizk, 1980; Monkhouse and Khalique, 1986; Rizk, 1991; Standring, 2008) although the conventional anatomy of the rectus sheath is still taught regularly in the anatomy classrooms based on the apparent accord in the textbooks. Hence, the young upcoming laparoscopic surgeons with mindset of the stereotyped anatomy of the inguinal region are unable to appreciate the complex preperitoneal anatomy, landing into surgical difficulties with a long learning curve (Lange et al, 2002). Standring (2008) provided a totally new insight/concept about the bi-laminar nature of each of the three anterior abdominal wall muscle aponeuroses - external oblique, internal oblique & transversus abdominis, based on the classical work of Rizk in 1980 (Figure 1.1). Mwachaka et al (2009) and Monkhouse and Khalique (1986) documented both aponeurotic and musculoaponeurotic natures of the posterior rectus sheath while Rao et al (2009) reported an occurrence of the musculoaponeurotic anterior rectus sheath. Complete posterior rectus extending upto the pubic symphysis has been reported that may be tendinous or grossly attenuated (Anson et al, 1960; Rizk, 1991; Arregui, 1997; Ansari, 2014). Mwachaka et al (2010) also reported gender variation in the incidence of the complete posterior rectus sheath.
3
M. M. Ansari
Chapter - 1
Introduction
Fig. 1.1: Showing the bi-laminar nature of the external oblique, internal oblique and transversus abdominis aponeuroses (modified from Gray’s Anatomy, 40th Edition, 2008)
1.2.2. Variations of Arcuate Line Wide variations have been documented in the level, number and morphology of the arcuate line of Douglas. Arcuate line is reported to vary from half way to 1/4th down the umbilicus to the symphysis pubis (Woodburne, Woodburne, 1961; 1961 Cunningham et al, 2004; Loukas et al, 2008 2008; Mwachaka et al, 2010; Ansari, 2013). The arcuate rcuate line may sometimes be totally absent (Rizk, (Rizk, 1991 1991; Mwachaka et al, 2010; Ansari, 2013 & 2014), ), indistinct (Schaefer & Dancer, 1894) or double (Lung (Lung-Chin, 1965) or even multiple (Woodburne Woodburne and Burkel, 1988; 1988 McVay & Anson, 1940). ). Monkhouse and Khalique (1986) observed that the shape and position of the arcuate line were neither symmetrical nor constant. Gender variation has recently been reported by Mwachaka et al (2010). In the opinion of some anatomists (Moffat, ( 1989; Rizk, 1991), the arcuate rcuate line seen in the dissecting room is artificially created usually during dissection dissection by removing the lower part of the attenuated posterior rectus sheath (PRS), considering it to be merely transversalis fascia.
1.2.3. Controversies in Transversalis Fascia There is lack of agreement among the anatomists and surgeons alike about the definit definition, nature, layers, extent, attachments or function of the transversalis transversalis fascia ever since it was described by Sir Astley Cooper in 1804 and so named by him in 1844; and the controversies exist even today (Memon et al, 1999). Original bi-laminar bi description of transversalis ransversalis fascia by Cooper was supported by Mackay (1889), Lytle (1945), and Read & John (1994) but was not universally accepted by other investigators including McVay and Anson (1940), Condon (1995), Arregui (1997), and Colborn and Skandalakis (1998). ( The transversalis ransversalis fascia has also been described as a 4
M. M. Ansari
Chapter - 1
Introduction
direct extension of the transversus aponeurosis in select cases by Pierpont et al (1969) that added a new confusion. Petros Mirilas (2012) categorically affirmed that the concept of ‘bilaminar transversalis fascia’ is outdated. Bendavid (2001) and Ansari (2015a) documented the transversalis fascia as a single-layer structure but of diaphanous nature in the inguinal region.
Textbooks of anatomy do not describe the so-called posterior lamina of the transversalis fascia described by Cooper (Williams and Warwick, 1980; Williams et al, 1989; Moore, 1992; Woodburne and Burkel, 1994; Rosse and Rosse-Gaddum, 1997), and the Nomina Anatomica (12th International Congress of Anatomists, 1989) also does not mention this term as well (Memon et al, 1999). Most of the contemporary textbooks of anatomy including the Gray’s Anatomy (Standring, 2008 and 2016) also do not mention the posterior lamina during discussion of the transversalis fascia.
1.2.4. Significance of Pre-Peritoneal Fat The preperitoneal fat has up till now been regarded as an inconsequential structure, but some recent reports emphasized its possible significance not only with respect to aetiology of the inguinal hernia but also with respect to its surgical repair. The extraperitoneal fat usually protrudes into the inguinal canal in varying amounts, and often produces the so-called lipoma of the cord (Nyhus et al, 1991; Fawcett and Rooney, 1997). In the opinion of Lilly and Arregui (2002), the preperitoneal fat insinuates itself through the internal ring and over time dilates it, and this might then predispose to the formation of an indirect hernia. The herniating preperitoneal fat or cord lipoma has been reported to cause similar symptoms even in absence of a true inguinal hernia (Gersin et al, 1999; Lilly and Arregui, 2002), or may be a cause of recurrence of symptoms after inguinal hernia repair (Felix et al, 1998).
1.2.5. Existence of Pre-Peritoneal Fascia Although contemporary textbooks of anatomy do not mention the pre-peritoneal fascia as a separate entity, but in addition to the transversalis fascia, a variably organized and possibly thickened layer of pre-peritoneal fascia has been described in many reference texts (Memon et al, 1999). Attachments of the posterior lamina in the original description of Cooper (1804, 1844) seem to be identical to those of the pre-peritoneal fascia described later by several investigators (Read and John, 1994). Way back in 1975, Fowler reported that “the preperitoneal fascia of the groin is distinct from the transversalis fascia, although often mistaken for it”, which was later supported by Arregui (1997) and Ansari (2015b). Fowler (1975) also documented the presence of a preperitoneal
5
M. M. Ansari
Chapter - 1
Introduction
fascial ring or secondary internal ring, which appears to have been confused in the past with the transversalis fascial opening or internal ring proper.
1.2.6. Need of Present study Recent interest in the laparoscopic preperitoneal approach for the posterior hernia repair in patients with the groin hernia, for which the surgeon works in the preperitoneal fascial planes, has created an acute need for the thorough study of the preperitoneal anatomy that is not described well in the current literature, especially from the laparoscopic perspective (Arregui, 1997). Moreover, almost all the published literature is based on the gross anatomic studies during autopsy and dissection of the human cadavers, and very little information is available regarding the live surgical anatomy of posterior rectus sheath and extraperitoneal tissues/ fascias of the inguino-pelvic region. Laparoscopic hernia surgery warrants a sound knowledge of the preperitoneal anatomy, more precise identification of structures and more careful dissection as compared to the open surgery (Rosser, 1994), especially during the total extraperitoneal pre-peritoneal (TEPP) approach where all the surgical work is carried out in a limited closed space. There is sufficient published anecdotal experience to indicate that the relationships of structures near the internal ring are not generally known to the most practicing surgeons (Brick et al, 1995). The anatomy of the anterior approach to the abdominal wall, as is the standard protocol followed in the dissection hall with resultant mindset of the medical students from the very beginning, cannot necessarily be directly applied to the posterior approach of the laparoscopy (Marks et al, 1996). The surgeon with the stereotyped knowledge of the classical anatomy only of the posterior rectus and extraperitoneal tissues/fascias, often lands up in difficulties during the laparoscopic inguinal hernioplasty and is often lost in the multi-fascial structures of the inguino-pelvic region, especially near the internal inguinal ring for no obvious reason, possibly not due to the lack of skill/experience or the presence of the inflammatory adhesions but due to the technical error of inappropriate surgical dissection secondary to the lack of knowledge and appreciation of the considerable anatomical variations as has been rightly emphasized by Arregui (1997). Moreover, the continued role of anatomic research cannot be overemphasized even if the anatomic structures are well known because new surgical approaches provide new vision of structures known for centuries, and at the same time, new dangers arise from the newer techniques (Avisse et al, 2000).
6
M. M. Ansari
Chapter - 1
Introduction
1.3. PRESENT RESEARCH STRATEGY Present research was planned in terms of well-defined problem definition, aims and objectives, research methodology, scope of this research, completion of the present research and plan of chapters. The details are briefly described in the following paragraphs.
1.3.1. Problem Definition There is no doubt that the TEPP (total extra-peritoneal preperitoneal) hernioplasty for the inguinal hernia is now a well-recognized technique with proven efficacy, reduced post-operative pain and low failure rate, in addition to the early return to the activity and work (Faure et al, 2006). However, the operator often finds difficulties in execution of the TEPP for no apparent reason/cause, which are almost always, attributed to the lack of his/her surgical skills or presence of adhesions. It is now also increasingly recognized that despite the merits of the laparoscopic hernioplasty, the extraperitoneal anatomy & dissection in the groin is poorly understood by the most practising surgeons (Arregui, 1997; Colborn and Skandalakis, 1998; Lange et al, 2002; Faure et al, 2006). Moreover, the inadequate poor understanding of the extraperitoneal anatomy resulting into the improper surgical dissection of the tissue planes is now regarded as the main cause of difficulties in the execution of the laparoscopic hernioplasty for the inguinal hernia with a long learning curve required for the laparoscopic total extra-peritoneal preperitoneal (TEPP) repair (Brick et al, 1995; Liem et al, 1996; Lange et al, 2002; Vidovic et al, 2007), leading to its lack of popularity among the surgical fraternity despite its obvious merits and better surgical outcomes (Lange et al, 2002). The reportedly complex inguinal anatomy (Arregui, 1997; Lange, 2002) becomes more kaleidoscopic and even psychedelic in presence of the anatomic variations which have been documented by several investigators over the last several decades but which received little attention of the anatomists and the practising surgeons alike.
1.3.2. Objectives of the Present Research The objective of the present work was to perform and establish the laparoscopic inguinal hernioplasty through the total extra-peritoneal preperitoneal (TEPP) approach at our institution and to carry out a laparoscopic study of the live surgical human anatomy of the abdomino-inguinal region in these patients with the inguinal hernia under the preperitoneal laparoscopy which provides 7
M. M. Ansari
Chapter - 1
Introduction
an excellent interparietal-cum-posterior perspective, very good lighting and clear magnified definition of the various anatomical planes, along with instant documentation and video-recording.
1.3.3. Aims of the Present Research The main aim of the present research was to study the morphology of the following structures below the umbilicus during the TEPP (total extra-peritoneal preperitoneal) laparoscopic hernioplasty for the inguinal hernia: 1) Posterior Rectus Sheath 2) Arcuate line Douglas 3) Pre-Peritoneal Fat/Fascia 4) Transversalis Fascia
1.3.4. Research Methodology Adopted The research methodology adopted in the present work is detailed in the Chapter II. However, the various parameters for the patient’s selection, technique and software used for the proposed research are listed below: 1) Selection Criteria for the Study 2) Inclusion Criteria for the Study 3) Exclusion Criteria for the Study 4) Approval by Ethical and Scientific Committee of the University 5) Admission of Patients to the Hospital 6) Patients’ Written Informed Consent 7) Standard 3-midline-port Technique of Laparoscopic TEPP Surgery for Inguinal Hernia 8) Instant Data Collection & Documentation 9) Follow Up after Discharge from the Hospital 10) Statistical Analysis (SPSS v. 21)
1.3.5. Scope of this research “Inguinal hernia repair is the most frequent operation in general and visceral surgery worldwide” (Bittner et al, 2011) and this was ratified by Berger (2016). With increase in the anatomic knowledge, the evolution of the laparoscopic procedures has paralleled that of the open surgery (Mirilas et al, 2005). Therefore, adequate and proper understanding of the inguinal anatomy by the surgeons, especially the upcoming young surgeons, will go a long way for the safe, smooth and rapid execution of the hernioplasty, especially by the newer surgical techniques to improve the quality of the patient care to the masses at an affordable cost. 8
M. M. Ansari
Chapter - 1
Introduction
This study assumes more importance in the current trend of the fast urbanization with rapid adoption of the newer technological approaches of the hernia surgery even in the developing countries including India, especially the laparoscopic method of hernioplasty, with particular reference to the familiarity and timely recognition of the anatomic variations in the inguinal region in order to be able to perform the precise surgical dissection, a prerequisite for prevention of the frequently reported complications of the disabling chronic inguinal pain and the recurrence of hernia which leads to not only the additional cost but also the loss of man-hour. The study may prove even more fruitful in the ill-defined subset of population with the higher risk of developing these complications. James Rosser (1994) declared categorically that the ultimate responsibility lies with the surgeon who must be equipped with the ‘crisp, precise anatomical knowledge’, and the knowledge of the precise preperitoneal anatomy leads to a safer surgical dissection as rightly emphasized by Kraus (1994).
1.3.6. Completion of the Present Research The present study was completed in about five years’ time and recruited a total of sixty three adult patients with uncomplicated primary inguinal hernia who were posted for the laparoscopic total extra-peritoneal pre-peritoneal (TEPP) mesh hernioplasty at our institution - Jawaharlal Nehru Medical College Hospital, Aligarh Muslim University, Aligarh, India.
1.3.7. Plan of Chapters The present work has been distributed and discussed in the following plan of the chapters:
Chapter – I: Introduction, Contemporary Issues & Present Strategy Chapter – II: Review of Literature Chapter – III: Clinical Research Methodology Chapter – IV: Observations & Results Chapter – V: Discussion Chapter – VI: Summary of the Thesis Chapter – VII: Outlook & Scope for Future Research REFERENCES ANNEXURES: o Annexure I: Ethical Clearance & CASR Approval o Annexure II: Informed Consent Form o Annexure III: Proforma for Data Collection o Annexure IV: List of Working Papers o Annexure V: Published Papers (List & Full Texts) o Annexure VI: Profile of the Candidate o Annexure VII: Soft/Digital Material (List, Videos, & PDFs):
Video Clips (Eleven in Number) Complete Thesis (PDF) Publications (PDFs) Bio-Data of the Candidate (PDF)
9
M. M. Ansari
Chapter - 1
Introduction
1.4. CONCLUSION Despite the wide anatomic variations reported from time to time over the last several decades, the traditional description of the inguinal anatomy is still taught in our anatomy classrooms, leading to a fixed mindset that often proves counterproductive for instant recognition and precise dissection of the anatomical structures required during the laparoscopic surgery, especially by the upcoming young surgeons. Research in the live surgical anatomy of the preperitoneal tissues of the inguinal area cannot be overemphasized for the acute need of its sound understanding warranted for smooth safe execution of the laparoscopic total extra-peritoneal pre-peritoneal (TEPP) repair of the inguinal hernia. The present study of the live surgical anatomy during the excellent perspective, lighting and magnification of the preperitoneal laparoscopy was designed and conducted to address the controversies in the anatomic descriptions and the interpretations of the different preperitoneal layers of the inguinal and supra-inguinal regions, and to develop an easy surgical road map for the TEPP hernioplasty to establish the procedure at our institution.
--- End of Introduction ---
10