reference material 470 (CRM 470) in the United. States. Clin Chem Lab Med ... Christenson RH, Duh SH, Apple FS, Bodor GS,. Bunk DM, Panteghini M, et al.
Clinical Chemistry 54:8 1349–1355 (2008)
General Clinical Chemistry
Commutable Calibrator with Value Assigned by the IFCC Reference Procedure to Harmonize Serum Lactate Dehydrogenase Activity Results Measured by 2 Different Methods Giampaolo Cattozzo,1* Elena Guerra,2 Ferruccio Ceriotti,2 and Carlo Franzini,3 on behalf of the Enzyme Working Group of the Italian Society of Clinical Biochemistry and Clinical Molecular Biology (SIBioC)
BACKGROUND: The availability of commutable calibrator materials may ease considerably the task of harmonizing assay results and ensuring their traceability to reference procedures. We sought to verify the commutability of potential calibrator materials and evaluate their effectiveness in harmonizing LDH results by 2 measurement methods. METHODS:
We measured LDH in 109 serum samples and 31 materials, including frozen serum pools (with either normal or abnormal isoenzyme patterns), commercial stabilized materials, and the ERM-AD453/ IFCC reference material. We assayed LDH activity with the IFCC reference procedure and with 2 commercial methods, 1 using the lactate-to-pyruvate (LP) reaction, and the other the pyruvate-to-lactate (PL) reaction. We selected a commutable material, with LDH value assigned by the reference procedure, as a calibrator for recalculating the results for patient sera by both LP and PL, thereby making them traceable to the IFCC reference procedure.
RESULTS: Original values for patient sera (n ⫽ 109) by the 2 commercial methods showed a mean (SD) PL/LP ratio of 1.97 (0.03); this ratio changed to 1.06 (0.02) after recalculation of results. Linear regression of PL vs LP recalibrated values gave y ⫽ 1.108x – 9.7. At the clinically important concentration of 250 U/L (upper reference limit), the systematic difference between methods was 6.8%, which met our proposed quality specifications for inaccuracy and total error. CONCLUSIONS: By properly selecting the calibrator, the results of serum LDH measurement by 2 different
1
A. O. Ospedale di Circolo e Fondazione Macchi, Varese, Italy; 2 Diagnostica e Ricerca S. Raffaele SpA, IRCCS S. Raffaele, Milano, Italy; 3 Universita` di Milano, Milano, Italy. * Address correspondence to this author at: Laboratorio di Analisi Ospedale F. Del Ponte, A. O. Ospedale di Circolo e Fondazione Macchi, Via F. Del Ponte n. 19, 21100 Varese, Italy. Fax ⫹390332299408; e-mail giampaolo.cattozzo@
methods may be harmonized and made traceable to the selected highest (reference) metrological level. © 2008 American Association for Clinical Chemistry
Lactate dehydrogenase (LDH)4 (L-lactate: NAD⫹ oxidoreductase, EC 1.1.1.27) is present in all cells of the human body and in human blood serum. Increases in its serum concentration are observed in a variety of pathological events and have long been considered relevant to appropriate patient management (1 ). The importance of serum LDH measurement has been underscored in different conditions including malignancies (2, 3 ), neuroblastoma (4 ), cutaneous melanoma (5 ), hemolytic anemia (6 ), severe acute respiratory syndrome (7 ), and chronic lymphocytic leukemia (8 ). The potential medical utility of measuring LDH in other biological fluids has also been reported (9 ). Such a pattern of utilization across various clinical settings provides a rationale for harmonization of LDH measurement results in practice. Using the same principle (UV spectrometric monitoring of pyridine coenzyme oxidation), LDH activity can be measured by either the lactate-to-pyruvate reaction (LP, forward reaction) or the pyruvate-to-lactate reaction (PL, backward reaction). As early as 1974, the forward reaction was recommended (10 ), and in 2002 the IFCC recommended a reference procedure for the measurement of LDH at 37 °C based on the forward reaction under optimized conditions (11, 12 ). With this IFCC reference procedure, a reference material was certified for LDH activity concentration (13 ), and pre-
gmail.com. Received November 6, 2007; accepted May 1, 2008. Previously published online at DOI: 10.1373/clinchem.2007.100081 4 Nonstandard abbreviations: LDH, lactate dehydrogenase; LP, lactate to pyruvate; PL, pyruvate to lactate; EQA, external quality assessment; ISO, International Standards Organization.
1349
liminary upper reference limits were established in hospitalized subjects (14 ). Despite agreement on a reference method (12 ) and the availability of a comprehensive approach (15 ) for establishing traceability of routine measurement results to the highest metrological level (reference method), satisfactory LDH assay harmonization has not yet been achieved. In a number of regional and national external quality assessment (EQA) schemes in Italy, covering about one half of the country, only 10% to 20% of the laboratories presently use the forward reaction, although this percentage is slowly increasing. Each laboratory reports its measurement results using its method-specific calibration, a process that yields a PL/LP results ratio close to 2. In other European countries, the situation also appears to be unsatisfactory (16 ). In international EQA schemes (17 ), the overall percentage of laboratories using the forward reaction is about 75%, but there are strong geographical differences, with some countries still using the backward reaction in nearly 100% of their laboratories. It is generally agreed that assuring the traceability of everyday measurement results to the highest accepted/available metrological order, by establishing a comprehensive reference measurement system, is the way to achieve definitive harmonization of results, but implementing the whole process is not easy (15, 16 ). One critical point of the overall process is the quality of the materials used as calibrator, with special reference to a quality characteristic of the materials referred to as commutability. Different comprehensive definitions have been given for this characteristic (18, 19 ), but the original one (commutability refers to “the ability of an enzyme material to show interassay activity changes comparable to those of the same enzyme in human serum”) (20 ) is still valid and applies in this context. Lack of commutability is frequently observed in stabilized (control and calibration) materials (21 ), especially in enzyme materials (22, 23 ), making them unsuitable for direct trueness-transfer processes (16, 24–26 ). The aim of the present work was to check the possible practical implementation of the traceability principle to achieve uniform results in routine, automatic measurement of serum LDH activity, independently of the reaction direction (forward or backward). To this end, the experimental work focused on the verification of commutability of stabilized materials and on the comparability of results by different methods after recalibration with commutable materials. Materials and Methods We assayed 109 anonymized fresh patient serum samples and 31 other materials. Patient sera, covering a 1350 Clinical Chemistry 54:8 (2008)
wide interval of activity concentration values, were obtained from blood samples collected in plain tubes and allowed to clot at room temperature. We selected sera to include in this study based only on the LDH activity concentration; several of these samples were subsequently submitted for isoenzyme analysis and pooled. The materials were grouped into the following categories: a) 5 frozen pools of fresh sera with normal isoenzyme patterns; b) 4 frozen serum pools with abnormal isoenzyme patterns (increase of isoenzyme 1, isoenzyme 3, isoenzyme 4, and isoenzyme 5); and c) 22 commercial stabilized materials, either calibrators or controls, from Bio-Rad Laboratories, Olympus Diagnostica, Roche Diagnostics, and Siemens Medical Solutions Diagnostics. In this last category we also included the ERM-AD453/IFCC reference material, supplied by the Institute for Reference Materials and Measurements and certified by this institute and the IFCC. This material is intended to be used as a reference material for manufacturers of reagents, to control the performance of enzyme measurements, and to verify the comparability of results from different laboratories. Total LDH activity concentrations in the materials, as measured by the IFCC reference procedure, spanned the following intervals: a) 90 – 473 U/L; b) 475–954 U/L; c) 25–580 U/L. We performed LDH measurements according to the IFCC reference procedure (12 ), using N-methylglucamine from Merck; NAD free acid, grade I, and NAD crystal lithium salt from Roche; and lithium Llactate from Sigma. The in-cuvette temperature was checked with a thermal probe calibrated against a certified thermometer; wavelength and absorbance accuracy were checked against international standards. All the materials, but not the patient sera, were assayed with this reference procedure. LDH activity concentrations in the patient sera and in the materials were also measured by means of 2 commercial methods implemented on an AU640 automatic analyzer (Olympus Diagnostica) at 37 °C, based on the forward (LP) and the backward (PL) method, respectively. According to the manufacturer’s claims, the former method was calibrated to give results traceable to those of the IFCC reference procedure, the latter to a proprietary master calibrator. All the materials were assayed in triplicate, all the patient sera in duplicate; mean values from replicates were used for further calculations. Analytical imprecision (in percent CV) of the reference procedure spanned the interval 0.23%–2.46% for enzyme activity concentrations ranging from 25 to 954 U/L: the highest imprecision values were seen at both limits of the concentration interval. For the LP and the PL methods, the analytical imprecision was 0.00%–2.28% and 0.00%– 4,17%, respectively, with highest imprecision seen at low concentration values.
IFCC-Traceable Calibration Harmonizes LDH Values
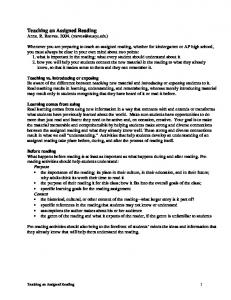
Normalized residual
50 40 30 20 10 0 –10 0
300
600
900
1200
Lactate dehydrogenase (U/L) Fig. 1. Commutability (displayed as normalized residuals vs enzyme activity concentration) of 31 materials with patient sera, in the pair of methods PL and LP. The materials included 5 serum pools with normal isoenzyme pattern (䡬), 4 serum pools with abnormal isoenzyme pattern ( ), 21 commercial materials (Œ), and the ERM-AD453/IFCC reference material ( ). Dotted lines show the ⫾3 limits.
We determined the isoenzyme pattern by means of agarose gel electrophoresis, followed by incubation with NAD and nitroblue tetrazolium salt (Interlab), and measured the relative amount of each isoenzyme by densitometric scanning of the gel. Serum pools were stored in a frozen state at ⫺80 °C for no longer than 1 month. Additional data were made available from the EQA scheme of the Regione Lombardia. Within this scheme, in the years 2005 and 2006, 24 control sera were analyzed by almost 250 participants, with a variety of instruments. The results obtained with either the LP or the PL methods were pooled, regardless of the instrument and of the calibration approach, and mean and SD were calculated. In the assay of the 24 control sera, 208 –220 laboratories used the PL method and 23–27 used the LP method. To assess the commutability of the materials with patient sera, we assayed materials and sera with the PL and LP methods and graphically compared the intermethod differences observed in the assay of the materials with those of patient sera. We assessed the intermethod relationship in the assay of sera statistically by nonparametric linear regression (27 ), calculated the distance of each single point from the regression line along the vertical axis (residual), and computed the SD of the residuals (residual SD) as a measure of the dispersion around the line. For each material, the residual was then computed and divided by the residual SD of patient sera to yield the normalized residual. We took
the normalized residual of each material as the measure of its degree of commutability (21, 28, 29 ); normalized residuals outside the ⫾3 interval were considered to indicate lack of commutability. For serum pools with abnormal isoenzyme pattern and for stabilized materials, we assessed commutability with the normal frozen pools in 2 pairs of methods including the reference procedure (either LP vs IFCC or PL vs IFCC) following the same experimental/statistical approach. To estimate the effect of recalibration with commutable material on the comparability of results by the LP and PL methods, we recalculated the results for all patient sera by both LP and PL methods, taking as calibrator a commutable material with value assigned by the IFCC reference procedure. The intermethod differences and ratios before and after recalibration were computed, and the relationship between the results by the 2 recalibrated methods was assessed by nonparametric linear regression and correlation analysis (30 ). Results The normalized residuals observed for the materials against patient sera, in the PL/LP pair of methods, are plotted against enzyme activity in Fig. 1; materials having a normalized residual outside the ⫾3 interval were considered noncommutable with patient sera in the relevant pair of methods. The materials and the pools spanned across similar activity concentration intervals, with the main exception of 1 pool with an abnormal Clinical Chemistry 54:8 (2008) 1351
Normalized residual
15
10
5
0
–5 0
250
500
750
1000
Lactate dehydrogenase (U/L) Fig. 2. Commutability with normal isoenzyme pattern serum pools of 26 materials (4 serum pools with abnormal isoenzyme pattern and 21 commercial materials), in 2 pairs of methods: LP vs IFCC reference procedure (●) and PL vs IFCC reference procedure (‚). The and the refer to the ERM-AD453/IFCC reference material in the LP/IFCC pair and the PL/IFCC pair, respectively.
isoenzyme pattern. In Fig. 2, the commutability of the different categories of materials with the normal frozen pools, in the pair of methods LP/IFCC or PL/IFCC, is similarly shown. The overall observed frequency of commutability, in different combinations of pairs of samples and of methods, is shown in Table 1. When the PL method was compared with the LP method, all the frozen pools with normal isoenzyme pattern were found commutable with patient sera, whereas 20 of 26 (77%) other materials (abnormal pools and commercial materials) were not. All the tested materials were found commutable with the normal frozen pools in the LP/IFCC pair of methods, whereas the commutability rate was 19 of 26 (73%) in the PL/IFCC pair. All the materials found commutable with patient sera in the PL/LP pair of methods also were commutable in the LP/IFCC and PL/IFCC pairs. The ERM-AD453/IFCC reference material was found noncommutable in the
PL/LP and PL/IFCC pairs. From graphical presentation of results (Figs. 1 and 2), there appears to be a relationship between degree of noncommutability and enzyme activity concentration, with materials at low concentrations more frequently found commutable. This pattern has been described and hypothetically attributed to an effect of the kind of enzyme in the material rather than to the material matrix (21 ). In recalibrating the 2 routine methods, all results were recalculated, taking one of the stabilized materials included in the study as a common calibrator. The selected material showed commutability with serum pools with normal isoenzyme pattern and with patient sera, exhibiting normalized residuals 0.1, 0.3, and ⫺0.1 for the methods’ pairs LP/IFCC, PL/IFCC, and PL/LP, respectively. Moreover, the value was assigned to the selected material by means of the IFCC reference procedure. In this way, the results from the routine meth-
Table 1. Frequency of commutability observed in this study. Comparison Pair of methods
PL vs LP
a b
Frequency of commutability
Pair of sample categories
Materials vs patient sera
Frozen poolsa (n ⴝ 5)
Stabilized materials (n ⴝ 26)
5
6
LP vs IFCC
a
Stabilized materials vs frozen pools
NA
26
PL vs IFCC
Stabilized materials vs frozen poolsa
NA
19
With normal isoenzyme pattern. NA, not applicable.
1352 Clinical Chemistry 54:8 (2008)
b
IFCC-Traceable Calibration Harmonizes LDH Values
Lactate dehydrogenase (difference PL – LP) (U/L)
1200
900
600
300
0 100
400
700
1000
1300
1600
Lactate dehydrogenase (mean) (U/L) Fig. 3. Intermethod differences (PL-LP) vs activity concentration for patient sera before (●) and after (‚) recalibration with a commutable calibrator.
ods were made traceable to the IFCC procedure. Fig. 3 shows the large improvement in agreement of methods after recalibration. As shown in Table 2, before calibration we observed (for 109 patient sera) a PL/LP mean ratio equal to 1.97 (0.03), in acceptable agreement with the mean value of 2.21 (0.12) obtained for 24 samples in the EQA scheme, with a variety of instruments and calibration processes. After recalibration, the mean PL/LP ratio value dropped to 1.06 (0.02); recalibrated values from the EQA scheme were not available. Result of linear regression and correlation analysis of recalibrated values (PL vs LP methods, 109 patient sera) gave intercept ⫽ ⫺9.7 U/L (CI ⫺11.4 to ⫺8.3), significantly different from 0; intercept ⫽ 1.108 (CI 1.101–1.116), significantly different from 1; nonparametric Spearman correlation coefficient r ⫽ 0.999.
Table 2. Ratios of LDH activities measured with 2 methods (PL and LP), before and after recalibration of both methods traceable to the IFCC procedure.a PL/LP ratios
Samples
Patient serab EQAS materialsc a
n
Before recalibration
After recalibration
109
1.97 (0.03)
1.06 (0.02)
24
2.21 (0.12)
—
Data are mean (SD). EQAS, external quality assessment scheme. Our laboratory, same instrument. Various instruments from 208 –220 laboratories (PL method) and 23–27 laboratories (LP method) participating in the scheme; recalibrated results not available.
b c
Discussion From a general point of view, given the variety of existing analytical methods and the heterogeneity of many molecules in biological specimens, reaching complete harmonization among measurements is a difficult task. The simple approach of using a single material as a common calibrator, not a part of a comprehensive measurement system, may produce misleading results (21, 24, 25, 31, 32 ). The lack of commutability of the calibrator is the main cause for this. A possible alternative is based on the impractical approach of using fresh patient sera as calibrators (33 ). The most effective solution currently recommended for trueness transfer is the implementation of a comprehensive reference measurement system (15, 34 ), including a hierarchy of measurement procedures and calibration materials. Even in this case, however, the commutability of materials must be considered, as it is recommended in projects aiming at pursuing or checking results harmonization (35, 36 ). In the case of serum LDH, all the parts (materials and methods) of a comprehensive measurement system are available. Despite the fact that uniform analytical procedures (e.g., based on the forward reaction) are more likely to produce results traceable to a reference procedure based on the same principle, achievement of such uniformity in measuring LDH across laboratories and manufacturers has been difficult to accomplish. In the work reported herein, we have verified the feasibility of making everyday measurements by different methods traceable to the highest metrological level. We gained confidence in the reliability of our Clinical Chemistry 54:8 (2008) 1353
trueness-transfer process by checking the commutability of different materials with different methods and assigning the calibration value using the reference procedure. The low reliability of results of either calibration or trueness assessment with noncommutable materials has already been discussed (24, 25 ). The commutability of the serum pools with the patient sera, as recommended for cholesterol secondary reference materials (37 ), was not verified; the pool was assumed to reproduce the mean behavior of the sera used in the preparation of the pool itself (36 ). A material exhibiting commutability characteristics as described above was then selected and used to recalibrate by calculation the results obtained by the 2 working methods (PL and LP) in the assay of 109 serum samples. Before recalibration, the mean (SD) PL/LP ratio was 1.97 (0.03), a figure in acceptable agreement with that observed in the EQA scheme [2.21 (0.12)]; after recalibration, the PL/LP ratio dropped to 1.06 (0.02), a figure indicating about 6% systematic proportional overestimation by PL method, and very significant improvement of intermethod agreement. Clinically, the comparison of results from 2 different methods may be particularly important at certain concentrations. One of these concentrations is the upper reference limit; the upper reference limit for the IFCC method has been set close to 250 U/L (247 U/L for females and 248 U/L for males) (14 ). From the linear regression equation of the PL (y) vs the LP (x) recalibrated values (y ⫽ 1.108x – 9.7; r ⫽ 0.999), at the critical value of x ⫽ 250 U/L, the corresponding y ⫽ 267 U/L gives a systematic difference of 6.8%. Although the observed bias is proportional, and the absolute mean bias, in U/L, is higher at higher activity concentration values, at lower activity concentration values the proportional bias is partly compensated by the statistically significant negative intercept. This last calculated bias value of 6.8% compares favorably with the mean value found for the PL/LP ratio (1.06) (Table 2); it is higher than the analytical goal for bias (4.3%) derived from biological variation (38 ) but is within the
limit (7.8%) proposed as an interim quality specification for inaccuracy (39 ). An even more favorable comparison is obtained if our experimental systematic bias (6.8%) is compared with the biological variation– based quality specification for total error (11.4 at P ⬍ 0.05) (38 ). In our experimental design, we have followed the principles described in International Standards Organization (ISO) document 17511 (19 ), but the transferability chain was different from that described in the ISO document. Our modified approach was chosen in an attempt to reduce uncertainty related to the length of the chain (40 ). Moreover, we preferred an approach including use of the IFCC reference measurement procedure over the direct use of an already existing reference material for calibration because we believed that verification of commutability was an important step of the overall process. In conclusion, our data show the feasibility of harmonizing the results of serum LDH measurements obtained by 2 different methods by use of a common commutable calibrator, with value assigned by means of the reference IFCC procedure. Our data also demonstrate the importance of verifying the commutability of reference materials for each measurement procedure for which they will be used. We have considered 2 current methods, differing in the reaction direction. In vitro diagnostic companies make available 2 families of analytical systems based on reaction direction, each including a different combination of instrument, reagents, and calibrators. The traceability of the results for each analytical system should be verified. We found the residual bias of 1 PL method to be clinically acceptable with reference to current biological variation– based quality specifications. Further improvement in harmonization across methods is likely to be obtained with the common adoption of a uniform method principle based on the forward reaction direction. Grant/Funding Support: None declared. Financial Disclosures: None declared.
References 1. Panteghini M, Bais R, van Solinge WW. Enzymes. In: Burtis CA, Ashwood ER, Bruns DE, eds. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics, 4th ed. St. Louis: Elsevier, 2006;601–3. 2. Sturgeon C. Practice guidelines for tumor marker use in the clinic. Clin Chem 2002;48:1151–9. 3. Suh SY, Ahn HY. Lactate dehydrogenase as a prognostic factor for survival time of terminally ill cancer patients: a preliminary study. Eur J Cancer 2007;43:1051–9. 4. Riley RD, Heney D, Jones RD, Sutton AJ, Lambert PC, Abrams KR, et al. A systematic review of molecular and biological tumor markers in neuroblastoma. Clin Cancer Res 2004;10:4 –12.
1354 Clinical Chemistry 54:8 (2008)
5. Balch CM, Soong SJ, Atkins MB, Buzaid AC, Cascinelli N, Coit DG, et al. An evidence-based staging system for cutaneous melanoma [Review]. CA Cancer J Clin 2004;54:131– 49. 6. Dhaliwai G, Cornett PA, Tierney LM. Hemolytic anemia. Am Fam Physician 2004;69:2599 – 606. 7. Hui DS, Chan MC, Wu AK, Ng PC. Severe acute respiratory syndrome (SARS): epidemiology and clinical features. Postgrad Med J 2004;80:373– 81. 8. Montillo M, Hamblin T, Hallek M, Montserrat E, Morra E. Chronic lymphocytic leukemia: novel prognostic factors and their relevance for riskadapted therapeutic strategies. Haematologica 2005;90:391–9.
9. Ernam D, Atalay F, Hasanoglu HC, Kaplan O. Role of biochemical tests in the diagnosis of exudative pleural effusions. Clin Biochem 2005;38:19 –23. 10. Demetriou JA, Drewers PA, Gin JB. Enzymes. In: Henry RJ, Cannon DC, Winkelman JW. Clinical Chemistry: Principles and Techniques, 2nd ed. New York: Harper & Row, 1974;919 –32. 11. Siekmann L, Bonora R, Burtis CA, Ceriotti F, Clerc-Renaud P, Fe´rard G, et al. IFCC primary reference procedures for the measurement of catalytic activity concentrations of enzymes at 37 °C. Part 1. The concept of reference procedure for the measurement of catalytic activity concentrations of enzymes. Clin Chem Lab Med 2002;40:631– 4.
IFCC-Traceable Calibration Harmonizes LDH Values
12. Schumann G, Bonora R, Ceriotti F, Clerc-Renaud P, Ferrero CA, Fe´rard G, et al. IFCC primary reference procedures for the measurement of catalytic activity concentrations of enzymes at 37 °C. Part 3. Reference procedure for the measurement of catalytic concentration of lactate dehydrogenase. Clin Chem Lab Med 2002;40:643– 8. 13. Siekmann L, Bonora R, Burtis CA, Ceriotti F, Clerc-Renaud P, Fe´rard G, et al. IFCC primary reference procedures for the measurement of catalytic activity concentrations of enzymes at 37 °C. Part 7. Certification of four reference materials for the determination of enzymatic activity of ␥-glutamyltransferase, lactate dehydrogenase, alanine aminotransferase and creatine kinase according to IFCC reference procedures at 37 °C. Clin Chem Lab Med 2002;40:739 – 45. 14. Schumann G, Klauke R. New IFCC reference procedures for the determination of catalytic activity concentration of five enzymes in serum: preliminary upper reference limits obtained in hospitalized subjects. Clin Chim Acta 2003;327:69 –79. 15. Panteghini M, Ceriotti F, Schumann G, Siekmann L. Establishing a reference system in clinical enzymology. Clin Chem Lab Med 2001;39:795– 800. 16. Jansen R, Schumann G, Baadenhuijsen H, Franck P, Franzini C, Kruse R, et al. Trueness verification and traceability assessment of results from commercial systems for measurement of six enzyme activities in serum: an international study in the EC4 framework of Calibration 2000 project. Clin Chim Acta 2006;368:160 –7. 17. QCNet. http://sde.qcnet.com/sde/reports/unity WWReports.aspx (Accessed February 2008). 18. Dybkaer R. Vocabulary for use in measurement procedures and description of reference materials in laboratory medicine. Eur J Clin Chem Clin Biochem 1997;35:141–73. 19. International Standards Organization. In vitro diagnostic medical devices: measurement of quantities in biological samples—metrological traceability of values assigned to calibrators and control materials. ISO/FDIS 17511, 2002. 20. Fasce CF Jr, Rej R, Copeland WH, Vanderlinde RE. A discussion of enzyme reference materials: ap-
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
plications and specifications. Clin Chem 1973;19: 5–9. Franzini C. Commutability of reference materials in clinical chemistry. J Int Fed Clin Chem 1993;5: 169 –73. Rej R. Accurate enzyme activity measurements: two decades of development in the commutability of enzyme quality control materials. Arch Pathol Lab Med 1993;117:352– 64. Brion E, Lessinger JM, Gould N, Leyendecker J, Fe´rard J. Evaluation of commutability of control materials. Clin Chem Lab Med 2002;40:625–30. Franzini C, Ceriotti F. Impact of reference materials on accuracy in clinical chemistry. Clin Biochem 1998;31:449 –57. Miller WG. Specimen materials, target values and commutability for external quality assessment (proficiency testing) schemes. Clin Chim Acta 2003;327:25–37. Cattozzo G, Franzini C, Melzi d’Eril G. Commutability of calibration and control materials for serum lipase. Clin Chem 2001;47:2108 –13. Passing H, Bablok W. A new biometrical procedure for testing the equality of measurements from two different analytical methods: applications of linear regression procedures for method comparison studies in clinical chemistry. J Clin Chem Clin Biochem 1983;21:709 –20. van Helden WC, Visser RW, Van den Bergh FA, Souverijn JH. Comparison of intermethod analytical variability of patient sera and commercial quality control sera. Clin Chim Acta 1979;93: 335– 47. Middle JG, Libeer JC, Malakhov V, Penttila I. Characterisation and evaluation of external quality assessment scheme serum. Clin Chem Lab Med 1998;36:119 –30. Cattozzo G, Franzini C, Melzi d’Eril GV. Myoglobin and creatine kinase MB mass assays: intermethod variability of patient sera and commercially available control materials. Clin Chim Acta 2001;303:55– 60. Ledue TB, Johnson AM. Commutability of serum protein values: persisting bias among manufacturers using values assigned from the certified
32. 33.
34.
35.
36.
37.
38.
39.
40.
reference material 470 (CRM 470) in the United States. Clin Chem Lab Med 2001;39:1129 –33. Miller WG, Myers GL, Rej R. Why commutability matters [Editorial]. Clin Chem 2006;52:553– 4. Franck PF, Steen G, Lombarts AJ, Souverijn JH, van Wermeskerken RK. Multicenter harmonization of common enzyme results by fresh patientpool sera. Clin Chem 1998;44:614 –21. Muller MM. Implementation of reference systems in laboratory medicine. Clin Chem 2000;46: 1907–9. Baadenhuijsen H, Kuypers A, Weykamp C, Cobbaert C, Jansen R. External quality assessment in The Netherlands: time to introduce commutable survey specimens. Lessons from the Dutch “Calibration 2000” project. Clin Chem Lab Med 2005; 43:304 –7. Christenson RH, Duh SH, Apple FS, Bodor GS, Bunk DM, Panteghini M, et al. Towards standardization of cardiac troponin I measurement. Part II: assessing commutability of candidate reference materials and harmonization of cardiac troponin I assays. Clin Chem 2006;52:1685–92. Myers GL, Eckfeldt JH, Greenberg N, Levine JB, Miller WG, Wiebe DA. Preparation and validation of commutable frozen human serum pools as secondary reference materials for cholesterol measurement procedures; approved guideline. NCCLS C37-A, 1999. Rico`s C, Alvarez V, Cava F, Garcı`a-Lario JV, Herna`ndez A, Jime´nez CV, et al. Current databases on biological variation: pros, cons and progress. Scand J Clin Lab Invest 1999;59:491–500. Westgard QC. Clinical quality requirements: European biologic goals and calculated biologic allowable total errors. http://www.westgard.com/ europe.htm (Accessed August 2007). International Standards Organization. In vitro diagnostic medical devices: measurement of quantities in samples of biological origin— metrological traceability of values for catalytic concentration of enzymes assigned to calibrators and control materials. ISO/FDIS 18153, 2003.
Clinical Chemistry 54:8 (2008) 1355