the Oscar O¨flund Foundation, Hel- sinki; and the Helsinki University .... Haines JL, Hauser MA, Schmidt S etal. (2005): Complement factor H variant increases ...
Acta Ophthalmologica 2008
Complement factor H Y402H polymorphism and characteristics of exudative age-related macular degeneration lesions Sanna Seitsonen,1 Irma Ja¨rvela¨,2 Seppo Meri,3 Petri Tommila,1 Pa¨ivi Ranta1 and Ilkka Immonen1 1
Department of Ophthalmology, Helsinki University Central Hospital, Helsinki, Finland 2 Department of Medical Genetics, University of Helsinki, Helsinki, Finland 3 Department of Bacteriology and Immunology, Haartman Institute, University of Helsinki, Helsinki, Finland
ABSTRACT. Purpose: The Y402H polymorphism of the complement factor H (CFH) gene is associated with age-related macular degeneration (AMD) in many populations. The reported genotype)phenotype correlations in the CFH Y402H polymorphism have not been pronounced and no studies on the effect of the polymorphism on the subgroups within wet AMD have been performed. In this study, we wanted to evaluate whether the CFH Y402H polymorphism has an effect on clinical variables in recent exudative AMD lesions. Methods: The study included 172 patients with exudative AMD. The size of AMD lesions and the presence and area of other AMD lesion variables were recorded in fluorescein angiography (FA) and analysed in relation to the Y402H genotypes. Results: The median lesion size (classic + occult choroidal neovascularization [CNV] + serous pigment epithelium detachment [PED] + haemorrhage, if present) was 8.15 mm2 in patients homozygous for the CFH risk allele (CC), 7.50 mm2 in heterozygous patients (CT), and 7.05 mm2 in those with the normal genotype (TT) (p = 0.599). Areas of classic and occult CNV, combined, without serous PED or haemorrhage were 6.37 mm2, 5.00 mm2 and 5.18 mm2, respectively (p = 0.407). There was a trend for CC patients to have more frequently minimally classic and less frequently predominantly classic lesion composition than CT or TT subjects. Conclusions: We detected no clear impact of the CFH Y402H polymorphism on recent exudative AMD lesion characteristics. Although the complement cascade is implicated in CNV formation and scarring processes in the retina, the Y402H polymorphism appears relatively neutral in these functions. Key words: age-related macular degeneration – choroidal neovascularization – complement factor H – polymorphism
Acta Ophthalmol. 2008: 86: 390–394 Copyright ª Acta Ophthalmol Scand 2007.
doi: 10.1111/j.1600-0420.2007.01050.x
390
Introduction Age-related macular degeneration (AMD) is the leading cause of visual handicap in developed countries. Findings in eyes with AMD lesions can be divided into precursor lesions, such as drusen or pigmentary abnormalities, and later lesions, such as central geographic atrophy and exudative AMD and its sequelae (Bird et al. 1995). The exudative form of AMD is responsible for the majority of visual handicap caused by the disease, and the development of this type of lesion is heralded by a loss of central vision occurring within 6–12 months (Bressler 2001). The Y402H polymorphism in the complement factor H (CFH) gene has been identified as a major risk factor for AMD (Edwards et al. 2005; Hageman et al. 2005; Haines et al. 2005; Klein et al. 2005). Relative risk for AMD has been reported as 1.86)4.6 for patients with one risk allele and 3.3)9.26 for patients with two risk alleles (Haines et al. 2005; Klein et al. 2005; Souied et al. 2005; Baird et al. 2006). Although the wet form of AMD is virtually always connected with a decrease in central visual acuity (VA) and scarring of the macula, considerable variation exists in the characteristics of acute and chronic lesions and in the level of final VA (Riusala et al. 2005).
Acta Ophthalmologica 2008
Although several haplotypes and polymorphisms in different genes have been associated with AMD (Hageman et al. 2005; DeWan et al. 2006; Gold et al. 2006; Hughes et al. 2006; Li et al. 2006; Maller et al. 2006; Yang et al. 2006), the CFH Y402H polymorphism is the most thoroughly studied and appears to involve a highly significant risk for AMD in several ethnic groups (Conley et al. 2005; Edwards et al. 2005; Hageman et al. 2005; Haines et al. 2005; Klein et al. 2005; Souied et al. 2005; Baird et al. 2006; Magnusson et al. 2006; Seitsonen et al. 2006). As the complement system has been reported to be involved in the growth of choroidal neovascularization (CNV) (Bora et al. 2005) and other processes occurring in tissue response and scarring, we wanted to analyse whether a connection exists between the CFH Y402H polymorphism and the variation in AMD lesion characteristics in eyes with recent exudative AMD.
Materials and Methods Patient material
The patient material consisted of 172 patients who attended the retina clinic at the Department of Ophthalmology, Helsinki University Central Hospital for exudative AMD between 1999 and 2005. Written informed consent was obtained from all subjects after explanation of the nature and possible consequences of the study. The study was approved by the Ethics Committee of the Helsinki University Eye and Ear Hospital and performed in accordance with the Declaration of Helsinki. Ophthalmologic investigations
Visual acuity assessment, biomicroscopy of the anterior and posterior parts of the eye and fluorescein angiography (FA) were performed in all patients. The angiograms were recorded using either the Topcon Imagenet (Topcon Inc., Tokyo, Japan) or Heidelberg retinal angiograph (Heidelberg Engineering, Heidelberg, Germany) systems. The area measurements were performed with the software within the respective imaging systems. Blood samples for genotyping were obtained from all patients. Angiograms were reviewed later by a retina specialist (I.I.). The angiograms
were evaluated without knowledge of patient identity and genotype. The following parameters were recorded: total lesion area, including occult and classic CNV lesion components, serous pigment epithelial detachment (PED) and any haemorrhage dense enough to cover underlying fluorescence, and CNV lesion area, including classic and occult lesion components but excluding serous PED and haemorrhage. The presence and size of a serous PED and the presence of a retinal-angiomatous proliferation (RAP) were also recorded. Only one eye in each subject was analysed, except for data presented on fellow eyes. In patients with bilateral wet AMD, the eye which had been evaluated for the first time for recent wet AMD at the date closest to 31st March 2003 was selected as the study eye. Polymerase chain reaction sequencing
DNA was extracted from 10 ml of peripheral blood using the phenol– chloroform method. The DNA of the study subjects was amplified by polymerase chain reaction (PCR) and sequenced using primers forward 5¢-ctttgttagtaactttagttcg-3¢ and reverse 5¢-ttagaaagacatgaacatgctagg-3¢ to determine the T1277C genotypes. Sequencing was performed using cycle sequencing with the Big Dye Terminator kit (version 3.1) (Applied Biosystems Inc., Foster City, CA, USA), and reactions were run on an ABI 3730 capillary sequencer according to the manufacturer’s instructions. Statistical analysis
All analyses were performed using SPSS Release 13.0, 2005 (SPSS Inc., Chicago, IL, USA) statistical software. Differences between groups were evaluated using the Kruskal– Wallis H-test (continuous variables) and the chi-square test. The median and the 25% and 75% quartiles are given as descriptive statistics. The level of significance was set at p < 0.05. The power of the study was estimated by using the PS (version 2.1.31, 2004) software in http://biostat. mc.vanderbilt.edu/twiki/bin/view/Main/ PowerSampleSize. The calculations were performed for a 2 · 2 table, assuming grouping of patients was based on the frequency of a clinical variable. For example, when patients
were divided into four quartiles according to the total CNV lesion size, the proportion of the CC genotype in the three smaller quartiles (n = 123) was 0.36. In this setting, a proportion of > 0.56 or < 0.15 would have been detected with a power of 0.8 and p-value of 0.05 in the largest quartile of lesions corresponding to about ± 20% unit difference between the groups.
Results Of the 172 eyes enrolled, eight were excluded because > 50% of the total lesion area consisted of subretinal haemorrhage. In the remaining 164 eyes, the mean age (standard deviation [SD]) of the patients was 75.0 years (6.6). The median lesion sizes in patients (n = 164) with the normal genotype (TT, n = 26), and in patients who were heterozygous (CT, n = 80) and homozygous (CC, n = 58) for the Y402H polymorphism were 7.05 mm2, 7.50 mm2 and 8.15 mm2, respectively (p = 0.599, Kruskal–Wallis H-test). The corresponding medians of CNV lesion areas were 5.18 mm2, 5.00 mm2 and 6.37 mm2, respectively (p = 0.407) (Table 1). Patients were further divided into four quartiles according to total lesion size. When the smallest or largest quartile was compared with the remaining three quartiles, no difference existed between the genotypes. (Table 2). The CNV category was analysed in lesions where the CNV lesion was ‡ 50% of the total lesion area (n = 144) (Fig. 1). These lesions were classified as predominantly classic, minimally classic, or occult according to the Treatment of Age-related Macular Degeneration with Photodynamic Therapy (TAP) Study guidelines (TAP Study Group 1999). In these analyses there was a tendency for minimally classic lesions to be more prevalent in patients with the CC genotype and RAP lesions in patients with the TT genotype, but the difference did not reach statistical significance. There was no difference between the genotypes studied in the proportion of patients with a serous PED (Table 1). We also analysed whether the age of onset of exudative AMD varied between genotypes. In total, 87
391
Acta Ophthalmologica 2008
Table 1. Characteristics of choroidal neovascularization lesions in the different genotypes of the complement factor H gene Y402H (T1277C) polymorphism. CFH genotype (T1277C) Characteristics Age Mean (SD) Total lesion area (mm2) Median (Q25%– Q75%) CNV lesion area (mm2) Median (Q25%– Q75%) Presence of PED (%) Presence of RAP (%)
CC (n = 58)
CT (n = 80)
TT (n = 26)
CT or CC (n = 138)
74.9 (6.9)
74.9 (6.7)
75.8 (5.9)
74.9 (6.7)
p-value
8.15 (4.64–12.6)
7.50 (3.08–13.4)
7.05 (3.20–10.8)
8.00 (3.43–13.0)
0.599*
6.37 (1.84–10.1) 13.8 10.3
5.00 (2.08–10.5) 10.0 17.5
5.18 (0.468–8.76) 15.4 23.1
5.81 (2.05–10.1) 11.6 14.5
0.407* 0.528 0.257
* Kruskal–Wallis H-test. Fisher’s exact test, TT compared with CT or CC. CFH = complement factor H; CC = patients homozygous for the CFH risk allele; CT = patients heterozygous for the CFH risk allele; TT = patients with the normal genotype; SD = standard deviation; Q25% = 25% quartile; Q75% = 75% quartile; CNV = choroidal neovascularization; PED = pigment epithelium detachment; RAP = retinal-angiomatous proliferation.
Table 2. Total lesion size: largest and smallest quartiles (n = 41) compared with the remaining lesions (n =123). CFH genotype (T1277C) n (%)
Largest quartile Three smallest quartiles Smallest quartile Three largest quartiles
CC
CT
TT
p-value
14 44 13 45
21 59 22 58
6 20 6 20
0.916* 0.805 0.946* 0.805
(34%) (36%) (32%) (37%)
(51%) (48%) (54%) (47%)
(15%) (16%) (14%) (16%)
Comparisons between the complement factor H (T1277C) CC and TT genotypes and between CT or CC and TT genotypes. * Chi-square test, TT compared with CC. Chi-square test, TT compared with CT or CC. CFH = complement factor H; CC = patients homozygous for the CFH risk allele; CT = patients heterozygous for the CFH risk allele; TT = patients with the normal genotype.
patients had unilateral exudative AMD, 63 had bilateral exudative AMD, and the status of the other eye was unknown in 14 patients. The date of onset in the first eye was unknown in nine cases of bilateral late AMD. The age at onset of AMD in the first eye was fairly similar for the different genotypes (Table 3).
Discussion Although the prognosis for central VA is generally poor in all eyes with exudative AMD, some variation in the level of final VA is evident in these patients (Riusala et al. 2005). In addition, the extent and configuration of end-stage disciform scarring are variable. A previous report has suggested that the size of the late disciform lesion can be partially predicted from baseline angiographic findings (Riusala & Immonen 2004).
392
A small, baseline lesion may predict a smaller-than-average lesion at the end-stage. This was considered to indicate that, in eyes with a milder stimulus for angiogenesis, both the baseline and end-stage lesions would be smaller. By contrast, in eyes with a ‘larger pathogenetic burden’, a large baseline lesion would lead to major scarring (Riusala & Immonen 2004). As there is relatively rapid growth in CNV lesions at the early stage, the size of lesion at a given time-point is probably a function of both the duration of the early CNV process and the dimensions of the area with an angiographic stimulus. As the time between the initiation of CNV and the diagnostic FA probably varies independently of the genotype, we considered that the lesion size could be used as a surrogate measure of CNV lesion activity in this setting. In eyes with AMD the inflammatory component is most pronounced
in acute exudative lesions (Grossniklaus et al. 2002). Complement factor H has a central role in regulating many aspects of the inflammatory process and the complement system has a vital role in innate immunity (Rodrı´ guez de Co´rdoba et al. 2004). Components of the complement system, including C3, factor H and membrane attack complex (MAC), have been found in drusen from human donor eyes (Hageman et al. 2005) and C3 and MAC were deposited in experimental murine laser-induced CNV (Bora et al. 2005). Moreover, the complement system was found to be central to the expression of vascular endothelial growth factor (VEGF), transforming growth factor-b2 (TGF-b2) and b-fibroblast growth factor (b-FGF) in experimental CNV lesions (Bora et al. 2005). Thus, we expected that the presence of a CFH polymorphism would be a factor favouring a more aggressive phenotype with larger baseline lesions in exudative AMD. It was, therefore, somewhat surprising that we were unable to detect a clear impact of the Y402H polymorphism on exudative AMD lesion characteristics. This is the first study to attempt to find a connection between the CFH Y402H genotype and the phenotype of exudative AMD lesions. In previous studies, Magnusson et al. (2006) reported similar frequencies of the CFH Y402H risk allele in AMD patients with drusen (odds ratio [OR] 2.52) and those with more advanced lesions (OR 2.39). Later studies, however, found higher prevalences of the
Acta Ophthalmologica 2008
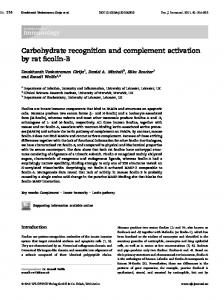
(A)
case, the genotype)phenotype correlations in AMD are not strong. Our results are in line with the hypothesis that the CHF Y402H polymorphism affects a very specific function, possibly related to drusen formation, but other aspects of the role of the complement cascade in subretinal CNV and scarring are unaffected.
Minimally classic (percent within genotype), p = 0.105, TT versus CT or CC
60% 50% 40% 30% 20% 10% 0%
(B) 60%
CC, n = 18
TT, n = 3
CT, n = 21
CT or CC, n = 39
Predominantly classic lesion (percent within genotype), p = 0.883, TT versus CT or CC
Acknowledgments The study was presented in part at the Association for Research in Vision and Ophthalmology Annual Meeting, May 2006. We thank the patients for their participation in the study and Marja Ikonen for collecting the patient samples. We acknowledge the financial support of grants from the Pa¨ivikki and Sakari Sohlberg Foundation, Helsinki; the Mary and Georg Ehrnrooth Foundation, Helsinki; the Eye and Tissue Bank Foundation, Helsinki; the Eye Foundation, Helsinki; the Evald and Hilda Nissi Foundation, Vaasa; the Oscar O¨flund Foundation, Helsinki; and the Helsinki University Central Hospital Research Funds (TYH5117, TYH6233), Helsinki, Finland.
50% 40% 30% 20% 10% 0% CC, n = 10
(C)
CT, n = 29
TT, n = 7
CT or CC, n = 39
Occult no classic lesion (percent within genotype), p = 0.170, TT versus CT or CC
60% 50% 40% 30% 20% 10% 0%
CC, n = 22
CT, n = 23
TT, n = 11
CT or CC, n = 45
Fig. 1. Prevalence of choroidal neovascularization (CNV) subtype categories in the different genotypes of the complement factor H (CFH) gene Y402H (T1277C) polymorphism: percentages within each genotype. Only patients with neovascular lesion ‡ 50% of the total lesions are included. (A) Minimally classic lesions. (B) Predominantly classic lesions. (C) Occult lesions. CC = patients homozygous for the CFH risk allele; CT = patients heterozygous for the CFH risk allele; TT = patients with the normal genotype.
Table 3. Age at onset of exudative age-related macular degeneration. Unilateral late AMD at presentation
Bilateral late AMD at presentation
Genotype (T1277C)
Age at presentation of the first eye (years)
Age at presentation of the first eye (years)
Age at presentation of the second eye (years)
CC CT TT CT or CC p-value
74.8 (7.0); 73.1 (6.9); 74.8 (6.0); 73.9 (6.9); 0.517*
73.3 (7.3); 74.9 (6.5); 73.0 (6.3); 74.2 (6.8); 0.295*
75.5 (6.7); 77.8 (5.7); 76.2 (5.7); 76.9 (6.2); 0.364*
32 40 15 72
20 27 7 47
22 32 9 54
Values are expressed in mean (standard deviation); n. *Kruskal–Wallis H-test.
CFH Y402H polymorphism in late lesions (ORs 11.02, 12.43, respectively) compared with those with predisposing lesions (ORs 2.00, 6.52, respec-
tively) (Despriet et al. 2006; Baird et al. 2006). These differences may in part be explained by differences in the classification of early lesions. In any
References Baird PN, Islam FM, Richardson AJ, Cain M, Hunt N & Guymer R (2006): Analysis of the Y402H variant of the complement factor H gene in age-related macular degeneration. Invest Ophthalmol Vis Sci 47: 4194–4198. Bird AC, Bressler NM, Bressler SB et al. (1995): An international classification and grading system for age-related maculopathy and age-related macular degeneration. Surv Ophthalmol 39: 367–374. Bora PS, Sohn JH, Cruz JM et al. (2005): Role of complement and complement membrane attack complex in laser-induced choroidal neovascularization. J Immunol 174: 491–497. Bressler NM, Treatment of Age-related Macular Degeneration with Photodynamic Therapy (TAP) Study Group (2001): Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: 2-year results of two randomized clinical trials. TAP Report 2. Arch Ophthalmol 119: 198– 207. Conley YP, Thalamuthu A, Jakobsdottir J, Weeks DE, Mah T, Ferrell RE & Gorin MB (2005): Candidate gene analysis suggests a role for fatty acid biosynthesis and
393
Acta Ophthalmologica 2008
regulation of the complement system in the aetiology of age-related maculopathy. Hum Mol Genet 14: 1991–2002. Despriet DD, Klaver CC, Witteman JC et al. (2006): Complement factor H polymorphism, complement activators, and risk of age-related macular degeneration. JAMA 296: 301–309. DeWan A, Liu M, Hartman S et al. (2006): HTRA1 promoter polymorphism in wet age-related macular degeneration. Science 314: 989–992. Edwards AO, Ritter R III, Abel KJ, Manning A, Panhuysen C & Farrer LA (2005): Complement factor H polymorphism and age-related macular degeneration. Science 308: 421–424. Gold B, Merriam JE, Zernant J et al. (2006): Variation in factor B (BF) and complement component 2 (C2) genes is associated with age-related macular degeneration. Nat Genet 38: 458–462. Grossniklaus HE, Ling JX, Wallace TM et al. (2002): Macrophage and retinal pigment epithelium expression of angiogenic cytokines in choroidal neovascularization. Mol Vis 8: 119–126. Hageman GS, Anderson DH, Johnson LV et al. (2005): A common haplotype in the complement regulatory gene factor H (HF1 ⁄ CFH) predisposes individuals to agerelated macular degeneration. Proc Natl Acad Sci U S A 102: 7227–7232. Haines JL, Hauser MA, Schmidt S et al. (2005): Complement factor H variant increases the risk of age-related macular degeneration. Science 308: 419–421. Hughes AE, Orr N, Esfandiary H, DiazTorres M, Goodship T & Chakravarthy U (2006): A common CFH haplotype, with
394
deletion of CFHR1 and CFHR3, is associated with lower risk of age-related macular degeneration. Nat Genet 38: 1173–1177. Klein RJ, Zeiss C, Chew EY et al. (2005): Complement factor H polymorphism in age-related macular degeneration. Science 308: 385–389. Li M, Atmaca-Sonmez P, Othman M et al. (2006): CFH haplotypes without the Y402H coding variant show strong association with susceptibility to age-related macular degeneration. Nat Genet 38: 1049– 1054. Magnusson KP, Duan S, Sigurdsson H et al. (2006): CFH Y402H confers similar risk of soft drusen and both forms of advanced AMD. PLoS Med 3: e5. Maller J, George S, Purcell S, Fagerness J, Altshuler D, Daly MJ & Seddon JM (2006): Common variation in three genes, including a non-coding variant in CFH, strongly influences risk of age-related macular degeneration. Nat Genet 38: 1055–1059. Riusala AM & Immonen IJ (2004): Predictors of structural findings in old disciform lesions. Am J Ophthalmol 138: 245–253. Riusala A, Sarna S & Immonen I (2005): Visual acuity and structural findings in old age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol 243: 947–950. Rodrı´ guez de Co´rdoba S, Esparza-Gordillo J, Goicoechea de Jorge E, Lopez-Trascasa M & Sanchez-Corral P (2004): The human complement factor H: functional roles, genetic variations and disease associations. Mol Immunol 41: 355–367. Seitsonen S, Lemmela¨ S, Holopainen J et al. (2006): Analysis of variants in the complement factor H (CFH), the elongation of very long chain fatty acids-like 4
(ELOVL4) and the hemicentin 1 (HMCN1) genes of age-related macular degeneration (AMD) in the Finnish population. Mol Vis 12: 796–801. Souied EH, Leveziel N, Richard F, DragonDurey MA, Coscas G, Soubrane G, Benlian P & Fremeaux-Bacchi V (2005): Y402H complement factor H polymorphism associated with exudative age-related macular degeneration in the French population. Mol Vis 11: 1135–1140. Treatment of Age-related Macular Degeneration with Photodynamic Therapy (TAP) Study Group (1999): Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: 1-year results of two randomized clinical trials. TAP Report 1. Arch Ophthalmol 117: 1329–1345. Yang Z, Camp NJ, Sun H et al. (2006): A variant of the HTRA1 gene increases susceptibility to age-related macular degeneration. Science 314: 992–993.
Received on January 29th, 2007. Accepted on August 1st, 2007. Correspondence: Sanna Seitsonen MD Department of Ophthalmology Helsinki University Central Hospital University of Helsinki Box 220 00029 Helsinki Finland Tel: + 358 50 562 3680 Fax: + 358 9 4717 5100 Email: sanna.seitsonen@hus.fi