the societal perspective, which includes work-loss costs as well as medical costs, ... Permanente Pediatric Vaccine Study Center, Oakland, ..... Advice nurse call.
Cost-effectiveness of a Routine Varicella Vaccination Program for US Children Tracy A. Lieu, MD, MPH; Stephen L. Cochi, MD; Steven B. Black, MD; M. Elizabeth Halloran, MD, DSc; Henry R. Shinefield, MD; Sandra J. Holmes, PhD; Melinda Wharton, MD; A. Eugene Washington, MD, MSc
Objective.\p=m-\Toevaluate the economic consequences of a routine varicella vaccination program that targets healthy children. Methods.\p=m-\Decisionanalysis was used to compare the costs, outcomes, and cost-effectiveness of a routine vaccination program with no intervention. Clinical outcomes were based on a mathematical model of vaccine efficacy that relied on published and unpublished data and on expert opinion. Medical utilization rates and costs were collected from multiple sources, including the Kaiser Permanente Medical Care Program and the California Hospital Discharge Database. Results.\p=m-\Aroutine varicella vaccination program for healthy children would prevent 94% of all potential cases of chickenpox, provided the vaccination coverage rate is 97% at school entry. It would cost approximately $162 million annually if one dose of vaccine per child were recommended at a cost of $35 per dose. From the societal perspective, which includes work-loss costs as well as medical costs, the program would save more than $5 for every dollar invested in vaccination. However, from the health care payer's perspective (medical costs only), the program would cost approximately $2 per chickenpox case prevented, or $2500 per life-year saved. The medical cost of disease prevention was sensitive to the vaccination coverage rate and vaccine price but was relatively insensitive to assumptions about vaccine efficacy within plausible ranges. An additional program for catch-up vaccination of 12-year-olds would have high incremental costs if the vaccination coverage rate of children of preschool age were 97%, but would result in net savings at a coverage rate of 50%. Conclusions.\p=m-\Aroutine varicella vaccination program for healthy children would result in net savings from the societal perspective, which includes work-loss costs as well as medical costs. Compared with other prevention programs, it would also be relatively cost-effective from the health care payer's perspective. (JAMA. 1994;271:375-381)
VARICELLA virus causes an estimated 3.7 million cases of chickenpox and 9000 hospitalizations in the United States an¬ nually.1 A routine varicella vaccination program targeting healthy children could prevent most of this morbidity From the Robert Wood Johnson Clinical Scholars Program and Division of General Pediatrics, Department of Pediatrics, University of California, San Francisco (Dr Lieu); Division of Research, The Permanente Medical
Group, Oakland, Calif (Dr Lieu); Surveillance, Investigations, and Research Branch, National Immunization Program, Centers for Disease Control and Prevention, Atlanta, Ga (Drs Cochi, Holmes, and Wharton); Kaiser Permanente Pediatric Vaccine Study Center, Oakland, Calif (Drs Black and Shinefield); Division of Biostatistics, Emory University School of Public Health, Atlanta, Ga (Dr Halloran); and MEDTEP Research Center on Minority Populations, Institute for Health Policy Studies, and Department of Obstetrics, Gynecology, and Reproductive Science, University of California, San Francisco (Dr
Washington).
Reprint requests to Division of Research, The Permanente Medical Group, 3451 Piedmont Ave, Oakland, CA 94611 (Dr Lieu).
and mortality (M.E.H., S.L.C., M.W., and L. Fehrs, MD, unpublished data, 1993), but would it be worth the cost? A cost-benefit analysis in 1985 sug¬ gested that a varicella vaccine that pro¬ vided lifelong immunity would save $7 in costs to society for every dollar in¬ vested in vaccination.2 If only medical costs were considered, varicella vacci¬ nation would cost money; however, sav¬ ings could accrue depending on the cost of the vaccine. Since the previous analy¬ sis, further data about vaccine efficacy have become available. A mathematical model of vaccine efficacy has been de¬ veloped that takes into account the in¬ direct effects of vaccination on disease transmission and the resultant age shifts in the epidemiology of disease.3 In ad¬ dition, empirical data on the medical uti¬ lization and costs of work loss due to chickenpox have now been collected.4,5
Policy decisions about new health pro¬ grams today ideally should be based not only on clinical effectiveness but also on cost-effectiveness. We performed an up¬ dated cost-effectiveness analysis of a rou¬
tine varicella vaccination program for preschool-age children, who are cur¬ rently being considered by policymak¬ ers as the primary target group for vac¬ cination. The present analysis is unique because it takes into account (1) current evidence about vaccine efficacy, (2) the effects of expected changes in the age distribution of disease, and (3) empirical data on the costs of medical utilization and work loss from varicella.
METHODS Decision Analysis Model We constructed a decision tree (Fig 1) to compare two major options for vari¬ cella. Under "No Vaccination," a person's probability of contracting chickenpox re¬ flects the current absence of a vaccina¬ tion program. Chickenpox may cause no
complications, major complications,
or
death (Fig 2). It also may cause medical utilization includingtelephone advice, out¬ patient visits, emergency department vis¬ its, and hospitalization. Major complications were defined as those requiring hospitalization, includ¬ ing but not limited to pneumonia and encephalitis. Patients with major com¬ plications could go on to have no longterm
sequelae, long-term disability, or
death. The possibility that a vaccination program could cause changes in the prevalence of zoster was not included; the expert panel indicated that no longterm data exist on this question.6 Under the "Vaccination" option, a per¬ son may or may not be vaccinated, de¬ pending on the extent of vaccination coverage in the population. Because the vaccine is less than 100% effective, vac¬ cinated as well as unvaccinated indi¬ viduals may contract chickenpox and subsequently use medical services or de¬
velop major complications.
Under both the "No Vaccination" and "Vaccination" options, there is a sec¬ ondary decision of whether to use acy-
Downloaded from jama.ama-assn.org at University of California - San Francisco on February 21, 2012
-Acyclovir -
Varicella -
r
Q -
No Varicella -
Decide
Q
Varicella —
Vaccinated —
Q
Q -
No Varicella Vaccination
Q
-
Varicella -
-Not Vaccinated
No -
-c
No Vaccination
Medical Care Within First 24 h
Q
No Medical Care Within First 24 h Medical Care Within First 24 h No Medical Care Within First 24 h
-Acyclovir
Medical Care Within First 24 h
No -
C -
No Varicella
Acyclovir
No Medical Care Within First 24 h
Acyclovir
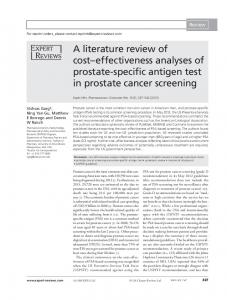
Fig 1.—Decision tree representing strategies for reducing varicella morbidity in the general population. Squares represent decisions by the clinician or policymaker; circles represent chance events. There are two basic options: No Vaccination or Vaccination (of all healthy children). Under the vaccination strategy, some children may not be vaccinated, and some of those vaccinated may develop varicella. Among unvaccinated children who develop varicella and present within the first 24 hours of symptoms, the clinician or policymaker also must decide whether the use of acyclovir is warranted.
Fig 2.—Varicella subtree outlining outcomes and associated utilization in persons with primary varicella In¬ fection. Minor complications include impetigo and cellulitis, which can be treated on an outpatient basis. The dashed lines refer to utilization outcomes that are not mutually exclusive. Major complications refer to out¬ comes serious enough to require hospitalization, including pneumonia and encephalitis. clovir for unvaccinated persons who seek medical care within the first 24 hours of the onset of chickenpox. Since chickenpox occurring in vaccinated persons is generally milder than chickenpox in un¬ vaccinated persons, we assumed that vaccinated persons with chickenpox would not receive acyclovir. The analysis was conducted from both the health care payer's perspective (pri¬ marily health insurers and parents, in¬ cluding medical costs only) and the so¬ cietal perspective (medical and workloss costs) for a 30-year period following the introduction of a routine varicella vaccination program. The model assumes an annual birth cohort of 4 million and
programmed on an Excel spread¬ sheet (Microsoft Corp; Redmond, Wash).
was
Data and Assumptions The probabilities of events in the de¬ cision tree (Table 1) were derived from
(1) published studies; (2) unpublished data from local, state, and national sources; (3) the mathematical model of expected health outcomes of a vaccination program3; and (4) consultation provided by a con¬ sensus panel ofnational varicella and vac¬ cine experts convened to provide esti¬ mates about selected assumptions for which empirical data were sparse or lack¬ ing.6 When estimates or assumptions were equivocal, we chose the one that would bias the results against vaccination. Probabilities of Chickenpox, Com¬ plications, and Utilization.—The agespecific probabilities of chickenpox, sub¬ sequent major complications, and death were derived from data collected in the National Health Interview Survey and Michigan Inpatient Database.1 The prob¬ ability of long-term disability after en¬ cephalitis was based on published stud¬ ies and on the opinion of an expert panel.69 The probabilities of emergency
department visits, outpatient urgent
care visits, and calls for a nurse's advice for children with chickenpox were based on utilization data collected in 1991 and 1992 from the Kaiser Permanente Medi¬ cal Care Program (KPMCP) of North¬ ern California.5 Probabilities of utiliza¬ tion for adults with chickenpox were extrapolated from estimates for children, adjusted in proportion to the relative age-specific rates of major complications. Vaccine Efficacy.—The projected numbers of chickenpox cases with no vs a universal vaccination program were based on a nonlinear mathematical model of va¬ ricella transmission and vaccine efficacy in an age-structured population, which has been described in detail.3 This model pre¬ dicted the shifts in the age distribution of chickenpox expected after widespread use of varicella vaccine in young children. Es¬ timates of vaccine efficacy (Table 1) were based on published studies and on the opinion of an expert panel.6·10"13 These in¬ cluded the estimates that given equiva¬ lent exposures, a vaccinated person with partial protection would be 12% as likely as an un vaccinated person to develop dis¬ ease. Of those initially completely pro¬ tected from disease, 15% would have ex¬ perienced partial waning of immunity by the time of death if there were no boost¬ ing by natural reinfection. Vaccine Complications.—Complica¬ tions after varicella vaccination are un¬ common but may include pain at the injection site and rash.14·15 We assumed that 2% of vaccinated persons would re¬ quire a follow-up outpatient visit for mi¬ nor complications. Serious complications due to the vaccine have not been re¬ ported in immunocompetent children. Chickenpox in Vaccinated Persons.— Chickenpox in vaccinated persons is usu¬ ally much milder than in unvaccinated persons.11·16"18 Our base case scenario as¬ sumed that a vaccinated person who sub¬
sequently developed chickenpox was only as likely to transmit the wild-type virus, compared with an unvaccinated person with chickenpox.6·16 In addition, a vaccinated person who subsequently de¬ veloped chickenpox was assumed to be only 1% as likely as an unvaccinated per¬ son with chickenpox to develop major complications requiring hospitalization.6 40%
However, it was assumed that a vacci¬ nated person with chickenpox was as likely as an unvaccinated person with chickenpox to make a physician visit or to seek advice by telephone. Vaccination Program and Catch-up Program.—The vaccination program we modeled assumed one varicella vaccina¬ tion would be routinely recommended for each child under the age of 6 years. Each scenario assumed that vaccination coverage would increase over the first 5
Downloaded from jama.ama-assn.org at University of California - San Francisco on February 21, 2012
years of the program and would reach stable coverage rates during the sixth year. The base case scenario assumed that vaccination coverage levels of chil¬ dren at school entry (aged 5 to 6 years) would be 97% by the sixth year of the vaccination program, based on experi¬ ence with other routine childhood vac¬ cines in states with school laws.18 When any new childhood vaccination program is introduced, policymakers must decide whether those persons who are older than the recommended age should be vaccinated in a supplemen¬ tary catch-up program.19 The base case analysis assumed no catch-up program. The incremental costs and benefits of a catch-up program were assessed in a sensitivity analysis. Under this program, any 12-year-old who neither had been vaccinated nor had a history of chick¬ enpox would receive varicella vaccina¬ tion. This program was assumed to be¬ gin 1 year after introduction of routine vaccination of preschoolers and to con¬ tinue for 11 years. It was assumed that 100% of susceptible 12-year-olds would be vaccinated. Also, it was assumed that no serological testing would be per¬ formed and that the medical history would reliably identify children who were already immune and not in need of varicella vaccination. However, this is a simplification of the actual situation.20 Acyclovir Treatment.—For the branches of the decision tree that lead to acyclovir treatment, it was assumed that acyclovir would be prescribed to all patients who made either an emergency department visit or an urgent care clinic visit within the first 24 hours of rash onset. The proportion of all patients who made visits to physicians within the first 24 hours was calculated based on esti¬ mated rates of visits to physicians (11% to 81%, varying by age) and on a survey finding that 43% of KPMCP parents who had made physician visits or calls for a nurse's advice did so within the first 24 hours of illness.6 It was assumed that acyclovir would not be prescribed without a physician encounter. Further, it was assumed that the availability of acyclovir would not change the probability of physician vis¬ its, a conservative assumption that tends to limit the effects, both costs and ben¬ efits, of an acyclovir strategy. Based on available data and our expert panel opin¬
ion, acyclovir was assumed not to change the rate of major complications requir¬
ing hospitalization after chickenpox.6·2123
Costs Costs were collected from a variety of published and unpublished sources and are summarized in Table 2. All costs were estimated in 1990 dollars.
Table 1.—Varicella-Related Probabilities and Varicella Vaccine
Efficacy
Base Case Estimate
Variable
Parameters Worst and Best Case Estimates
Chickenpox 9-year-olds Varicella sequelae (rate per chickenpox case) Major complications requiring hospitalization* Pneumonia
0.0015
Wharton et al'
0.00014
Wharton et al1
0.0000082
Wharton et al1 Wharton et al1
0.03
Expert Panel6
Encephalitis Death
Long-term disability after encephalitis Chickenpox-related utilization (rate per chickenpox case) Emergency department visit* Outpatient urgent care visit* Advice
nurse
call
Probability of physician visit within 24 h of onset of Being vaccinated by age of 6 y Minor vaccine complication requiring follow-up visit Vaccine efficacy parameters Complete protection 6 wk after vaccination Immunity is only partial by age at death Relative susceptibility to chickenpoxt Relative infectiousnesst Relative probability of major Work loss reduction For persons or parents of children treated with
Lieu et al5 0.118
Lieu et al5
0.88
Lieu at al5
rash
sequelaet
acyclovir
For persons or parents of children with chickenpox after vaccination
(Direct Costs)
Medical Care for Varicella.—The age-specific costs of varicella-re¬ lated hospitalization (Table 2) were de¬ rived by analyzing 1990 hospital dis¬ charge data from the California Office of Statewide Health Planning and Devel¬ opment, a database of all hospitalizations in California.24 Patients with im¬ munodeficiency, cancer, and trauma were excluded from this analysis. It was not possible to separate costs caused by varicella from costs attributable to in¬ tercurrent illness; thus, the figures may overestimate the costs of illness caused by varicella. To derive estimates of ac¬ tual costs, the mean charges for varicellarelated hospitalization were adjusted by the aggregate ratio of costs to charges for all hospitals in the state (0.53:1). The costs of emergency department visits and outpatient urgent care clinic visits were based on consultations with KPMCP administrators. The costs of nonprescription medications for chick¬ enpox were retail costs and were pro¬ rated based on the average use of the medications in the survey of KPMCP parents. The cost of a therapeutic course of acyclovir was taken from the Drug Topics Blue Book and was calculated based on the age-appropriate formula¬ tion and amount. We are unaware of any published em¬ pirical data on the cost of long-term care mean
0.50, 0.97
0.97
Lieu et al5 Cutts et al1'
0.02
0.83, 0.95 0.30, 0.05 Q.16, 0.05
0.90
Panel6 Panel6 Panel6 Panel6 Panel6
0.01
Expert Expert Expert Expert Expert
0.20
Dunkle et al2'
0.20
Expert Panel6
*Estlmate varies by age. Ellipses indicate estimates were not used tVaccinated person compared with an unvaccinated person.
Medical Costs
Source Wharton et al'
9156
rate per 100 000* 5- to
in
sensitivity analysis.
for persons with
long-term disability af¬
ter varicella complicated by encephalitis. These cases were assumed to incur medi¬ cal costs of $10 000 each year until death.
Vaccination Program Costs.—There available data for vaccine price. Based on informal discussions with the only US manufacturer, we estimated a private sector vaccine price of $35. The base case analysis herein assumes that all vaccine would be delivered at this price. The cost of vaccine administration has previously been estimated at $10.25 For toddlers, the cost of the labor and over¬ head to administer varicella vaccine was prorated to $5 since at least one other vaccination would be given at the visit. For 12-year-olds, we assumed that the varicella vaccine would require the full $10 cost for vaccine administration. are no
Work-Loss Costs (Indirect Costs) The value of work loss was used as a proxy for the time costs of varicella. The $201 cost of work parents miss when their children have chickenpox was based on a survey of 179 KPMCP parents who made physician visits or calls for a nurse's advice for chickenpox.5 The cost of work loss by adults who contract chickenpox was based on two sources. The number of days lost was based on analysis of Na¬ tional Health Interview Survey data. The age-specific cost of each day of work loss was derived from mean annual earnings tables for US persons in 1990 (D. Rice,
Downloaded from jama.ama-assn.org at University of California - San Francisco on February 21, 2012
at a rate of 5% per year before averaging.
Table 2.—Costs of Varicella-Related Events In 1990 Dollars*
Cost, $
Cost-effectiveness ratios were calcu¬ lated as discounted medical costs per
Source
Medical Costs
Hospitalization for varicella complicationst Emergency department visit Outpatient urgent care clinic visit
7482
OSHPD2' KPMCP administration:): KPMCP administration^ KPMCP administration^ Lieu et al5
42
Advice call
Nonprescription
medications
16 35
Vaccine dose
Vaccine administration To child 5 y old or less To child 12 y old in
Grabowsky and Markowitz25 Grabowsky and Markowitz25
10
catch-up program Long-term care for disability from varicella encephalitis, per year
Cochi et al33 Work-Loss Costs
Work loss of
of
child with
chickenpox Work loss of an adult with chickenpox§ Work loss of a person with death or long-term disability due to varicella encephalitist parents
a
201
Lieu et al5
749
NHIS, Rlceli
422 340
Ricell
*OSHPD indicates Office of Statewide Health Planning and Development; KPMCP, Kaiser Permanente Medical Program; and NHIS, National Health Interview Survey. tEstimate varies by age. Estimate shown is for 5- to 9-year-olds. ¿Estimate was based on consultation with administrators of the KPMCP. varies by age. Estimate shown is for 30- to 34-year-olds. ||D. Rice, PhD, written communication, March 1993.
Care
¿Estimate
Table 3.—Average Annual Varicella-Related Health Outcomes and Costs With and Without a Vaccination Program*
Projected US
Disease Cases No Health Outcomes
Chickenpox cases Major sequelae
Prevented
Vaccination 3 953 000
by
Vaccination
Vaccination
240 000
3 713 000
9930
610
Pneumonia
1000
62
938
Encephalitis
650
40
610
Cases of
long-term disability from encephalitis
Deaths
Discounted Costs
($
in
millions)
20
18
56
52
No Vaccination
Vaccination
Net Cost (Savings) of Vaccination vs No Vaccination
Medical costsf Vaccine and administration Varicella disease costs Total Medical Costs
Work-loss costs
(savings)
Total medical
work-loss varicella-related
costs
+
(savings)
10
90
529
(80)
98 48
(392)
146
(384)
"Figures are averages over the first 30 years of a vaccination program. Costs are determined at 5% per year; health
outcomes
are undiscounted. care
payer's perspective includes medical costs only. Ratio is the reduction in medical costs divided by the cost of the vaccination program. Societal perspective includes medical and work-loss costs. Ratio is the reduction in medical and work-loss costs divided by the cost of the vaccination program. tHealth
PhD, written communication, March 1993).
The discounted cost of future work loss for individuals who die or who have longterm disability from varicella encephalitis was estimated from a table of the present value of expected future lifetime earnings (D. Rice, PhD, written communication, March 1993). Costs of Vaccinated and
Acyclovir-Treated Cases For vaccinated persons who contracted
chickenpox, we assumed that the costs of physician visits, calls for a nurse's ad¬ vice, and hospitalizations were equal to those of unvaccinated persons with chick¬ enpox. For both vaccinated and acyclovir-
treated cases, it was assumed that work loss would be reduced by 20% for either the parent of a child with chickenpox or an adult with chickenpox.6 Cost-effectiveness Calculations Results of the analysis are presented as annual averages for the first 30 years of a routine varicella vaccination program. Vaccine cost-effectiveness traditionally has been analyzed using a single birth cohort. In the current analysis, we chose to average disease burden over 30 years to reduce variability from expected shifts in disease epidemiology due to the vac¬ cination program. Costs occurring in the future were discounted to present value
chickenpox case, as major complication death prevented, and as dollars per life-year saved. Incremental cost-effec¬ or
tiveness ratios were calculated to evalu¬ ate the additional cost for the additional benefit gained by the catch-up vaccina¬ tion program relative to the routine vac¬ cination program without catch-up. Ben¬ efit-cost ratios were the reduction in disease costs divided by the cost of the vaccination program. In all analyses, costs are discounted at a rate of 5% per year. There is con¬ troversy about whether health outcomes should be discounted. We have presented the main results with health outcomes undiscounted and discounted at 5%. The sensitivity analyses are presented with health outcomes undiscounted.
Sensitivity Analysis Considerable uncertainty exists about several of the key assumptions in this model. For example, estimating the wan¬ ing of protection from varicella vaccine over a lifetime is difficult since experi¬ ence with the vaccine spans only two decades. Sensitivity analysis was per¬ formed for three key assumptions: (1) vaccination coverage rates of school-age children were varied from the base case of 97% to 70% and 50%; (2) vaccine ef¬ ficacy was varied using the ranges sug¬ gested by our varicella vaccine expert panel6; and (3) vaccine price and vaccine administration strategies were varied over plausible ranges. Additional sensitivity analyses were performed and may be obtained from the authors and include (1) a two-dose vacci¬ nation strategy; (2) use of a measles-
mumps-rubella-varicella vaccine; (3) un¬ discounted costs; (4) discounting health outcomes at 5% for all analyses; (5) vary¬ ing the discount rate from 3% to 8% for
costs alone and for costs and health out¬ comes; and (6) crediting health benefits occurring in years 31 through 70 after vaccination to the first 30 years of the program. Two- and three-way sensitivity
analyses are also available.
RESULTS The projected results of the first 30 years of a routine varicella vaccination program are expressed as yearly aver¬ ages in Table 3. With no vaccination, 3.9 million chickenpox cases, 9900 major com¬ plications, and 56 deaths would be ex¬ pected annually. Each year, varicella-re¬ lated disease was predicted to cause $90 million in discounted medical and $439 million in discounted work-loss costs. A varicella vaccination program is pre¬ dicted to prevent 3.7 million (94%) of the
Downloaded from jama.ama-assn.org at University of California - San Francisco on February 21, 2012
chickenpox cases that would bet xpected without vaccination (Table 3), 9J00 hos¬ pitalizations, and 52 deaths annually. The vaccination program, including vaccine and administration, is projected to cost $88 million a year in discounted costs. However, vaccination saves an aver¬ age of $80 million annually in discounted medical costs. The bulk of the savings results from reduction in use of nonprescription medications (35%), hospitaliza¬ tion (34%), and urgent care clinic visits (20%). Thus, from the health care pay¬ er's perspective, the discounted net cost of the program is $8 million per year. The cost of the work loss saved by preventing varicella is estimated at $392 million per year, far greater than the cost of the vaccination program. Of the work-loss savings, 83% is from par¬ ents not missing work to care for chil¬ dren who would have chickenpox, 13% is from adults who no longer miss work due to chickenpox, 3.2% is from deaths averted, and 1.0% is from long-term dis¬ ability cases averted. When savings from averted work loss are incorporated into the total, a varicella vaccination pro¬ gram is expected to have a net savings of $384 million per year in discounted costs from the societal perspective. Although this analysis was conducted using discounted costs, policymakers may find undiscounted costs useful when comparing varicella vaccination with other programs. In undiscounted aver¬ age costs, the vaccination program would cost $162 million annually. Cost-effectiveness and Benefit-Cost Ratios From the health care payer's perspec¬ tive, using a varicella vaccination pro¬
$2.10 per case of chickenpox prevented (Table 4), $840 per major com¬ plication prevented, and $2500 per lifegram cost
year saved when future health outcomes were not discounted. When future health outcomes were discounted, the vaccina¬ tion program's cost appeared greater at $4.20 per chickenpox case prevented, $1650 per major sequela prevented, and $16 000 per life-year saved. From the health care payer's perspec¬ tive, a varicella vaccination program was projected to save 90 cents in discounted costs for each dollar spent on a vacci¬ nation program, ie, it would not save money. From the societal perspective, a varicella vaccination program was pro¬ jected to save $5.40 for every dollar in¬ vested in the program.
Sensitivity Analysis Vaccination Coverage.—The results were very sensitive to assumptions about the level of vaccination coverage in the target population reached by the
10000 ó O
50%
S g 6000
Base Case
5 k 4000
70%
20 40
50 60 Vaccination
70
80
90
100
100
Fig 4.—Cost per chickenpox case prevented vs vaccine price for 97% coverage (solid line) and best and 50% and 70% coverage (dashed lines).
5
'··.— Worst Case
suggested by our expert panel. At the 97% coverage level, the health benefits, costs, and cost-effectiveness ratios were insensitive to varying assumptions about vaccine efficacy. If vaccination coverage were assumed to be 50%, the results were only slightly more sensitive to assump¬
4-
o
40 60 80 Vaccine Price, $
Coverage Rate, %
6
œ
Coverage
Best Case
2000
O
Coverage ..-f? Coverage -yf/ 97%
-Worst Case
8000
\-Base Case
3
Best Case
2
O
40
50
60
Vaccination
V=^r^ 70
80
90
100
Coverage Rate, %
Fig 3.—Cost per health benefit gained vs vaccina¬ tion coverage rate for base case vaccine assump¬ tions (solid line) and best and worst case vaccine assumptions (dashed lines). Top, Cost per life-year saved. Bottom, Cost per chickenpox case pre¬ vented. Best case vaccine has 95% complete pro¬ tection 6 weeks after vaccination, 5% of vaccinées with only partial immunity by age at death, 5% rela¬ tive susceptibility, and 0% relative infectiousness. Worst case vaccine has 83% complete protection 6 weeks after vaccination, 30% of vaccinées with only partial immunity by age at death, 16% relative sus¬ ceptibility, and 95% relative infectiousness. age of 6 years. The higher the coverage more disease prevented and the less the medical cost per year of life saved. For example, a year of life saved cost $2500 at the 97% coverage level, $2900 at the 70% coverage level, and $7400 at the 50% coverage level (Fig 3, top, solid line). In terms of medical cost per chickenpox case prevented, the 70% coverage level was marginally more costeffective than the 97% level (Fig 3, bot¬ tom, solid line). Preventing a case of chickenpox cost $2.10 at the 97% cover¬ age level, $1.90 at the 70% coverage level, and $4.20 at the 50% coverage level. The differing patterns of the curves in Fig 3, top and bottom, reflect the fact that a 97% coverage level prevents 94% ofchick¬ enpox cases and 94% of deaths, while a 70% coverage level prevents 70% of chick¬ enpox cases but only 45% of deaths. Vaccine Efficacy.—As Fig 3 shows, the cost-effectiveness of the vaccination program was much more sensitive to the vaccination coverage rate than to vaccine efficacy assumptions within the ranges
level, the
tions about vaccine efficacy. Vaccine Price.—As expected, the pro¬ gram's cost-effectiveness was highly sen¬ sitive to vaccine price (Fig 4). At a 97% coverage level, the net medical cost per chickenpox case prevented increased lin¬ early by approximately 58 cents and the cost per life-year saved increased lin¬ early by $683 for every dollar that the vaccine price increased. The threshold price below which vac¬ cine began to save money from the health care payer's perspective was $31 under base case assumptions. The threshold was relatively insensitive to assumptions about vaccine efficacy and vaccination coverage: it varied from $26 (worst case
efficacy, 50% coverage) to $31 (best case efficacy, 97% coverage).
Incremental Cost of Catch-up Pro¬ gram.—When vaccination coverage of children at school entry was assumed to be 97%, the incremental benefit of the
program for catch-up vaccination of 12was minimal because trans¬ mission of varicella had already been interrupted by the routine vaccination program. In this scenario, the catch-up program prevented only 1% more of the potential disease cases than routine vac¬ cination alone. The catch-up program's incremental cost per chickenpox case prevented was $315, more than 100 times the basic cost of disease prevention. The catch-up vaccination program for 12-year-olds was more effective and costeffective at lower vaccination coverage rates of children at school entry. When coverage of school-age children was 70%, the catch-up program prevented an ex¬ tra 10% of all potential chickenpox cases at an incremental cost of $7.30 per chick¬ enpox case prevented. When vaccina-
year-olds
Downloaded from jama.ama-assn.org at University of California - San Francisco on February 21, 2012
Table 4.—Cost-effectiveness and Benefit-Cost Ratios for Routine Varicella Vaccination of US Children Costs
Discounted;
Health Benefits
Costs Discounted; Health Benefits
Undiscounted*
Discounted!
Cost-effectiveness Ratios Medical cost in dollars per
2.10
Chickenpox case prevented Major sequelae prevented Long-term disability prevented Death prevented Life-year saved
4.20
840
1650
150 000
294 000
2500
16 000
Benefit-Cost Ratios Dollars saved per dollar invested in vaccination
program, health
care
payer's perspective}:
Dollars saved per dollar invested in vaccination program, societal perspective}
*Costs
tCosts
0.9
0.9
5.4
5.4
discounted at a rate of 5% per year. and health benefits are discounted at a rate of 5% per year.
are
^Health care payer's perspective includes medical costs alone. Societal perspective includes medical and work-
loss costs.
Table 5.—Cost-effectiveness and Cost-Benefit Ratios of a Routine Varicella Vaccination With Other Vaccination and Preventive Programs*
Program Compared
Cost per
Year of Life
Intervention
Hepatitis Smoking
vaccination of Infants cessation for
Source
Saved,$
Cost-effectiveness Ratios (Health Care Payer's Costs discounted at 5%; health outcomes undiscounted Varicella vaccination of children, 1 dose 2500
Perspective) Current analysis Bloom et aP
3200
Oster et aP
middle-aged men elderly
Pneumococcal vaccination of
Sisk and
9000
Costs and health outcomes discounted at 5% Varicella vaccination of children, 1 dose of
Hypertension screening middle-aged Hepatitis vaccination of infants Colorectal cancer screening of elderly Cholesterol reduction using cholestyramine
Riegelman2'
Current
analysis Littenberg et al2s
21 300
men
41 000
Bloom et al2'
45 000
Wagner et al31
resin
Kinosian and
Intervention
Ratio
Eisenberg31
Source
Cost-Benefit Ratios
Health care payer's perspective! Varicella vaccination of children, 1 dose
Pertussis, 1987 price
Haemophilus influenzae type
vaccination of children
0.9
Current
1.1
Office of
analysis Technology Assessment report, 13532 Cochi et al,33 Hay and Daum34
1.3-3.4
Measles, mumps, rubella vaccination Pertussis, 1984 price
3.0
White et al3i
Hinman and
Kaplan3'
Societal
perspective! Haemophilus influenzae vaccination
of children
Hay and Daum34 analysis
2.8
Varicella vaccination of children, 1 dose Measles, mumps, rubella vaccination
Current 14.4
White et al3i
*AII estimates administration.
are adjusted to 1990 dollars. Price for one dose of varicella vaccine is $35, not including cost of tHealth care payer's perspective includes medical costs only. Ratio is the reduction in medical costs divided by the cost of the vaccination program. Societal perspective includes medical and work-loss costs. Ratio is the reduction
in medical and work-loss costs divided
by the
cost of the vaccination program.
tion coverage was assumed to be 50%, the catch-up program saved money com¬ pared with routine vaccination alone.
Acyclovir Options If there were no vaccination program, the use of acyclovir for persons who sought in-person physician consultation within the first 24 hours of symptoms would lead to a projected net savings of $300 000 per year from the societal per¬ spective. If there were a vaccination pro-
gram, acyclovir use for unvaccinated pa¬ tients presenting within the first 24 hours was still predicted to result in a small net savings. Medical costs would increase by $833 000 per year, but workloss costs would be reduced by $856 000 per year, for a projected total savings of $23 000 per year. Whether acyclovir use
predicted to save money depended greatly on the estimated value of work lost by parents when children had chick¬ was
enpox. With
or
without
a
vaccination
acyclovir use was no longer predicted to result in savings when the value of work loss was reduced by less than 10% to $185 per chickenpox case. progran,
COMMENT This analysis shows that the desir¬ ability of a routine varicella vaccination program depends on whose
perspective
is taken. At a vaccine price of $35, an effective vaccination program for pre¬ school-age children would not save money from the health care payer's per¬ spective, which includes only the medi¬ cal costs. However, it would save almost $400 million annually from the societal perspective, which includes the costs of lost work as well as medical care. The analysis also underscores the importance of vaccine pricing and vaccination cov¬ erage in determining cost-effectiveness. The current analysis is compared with studies of other vaccination and preven¬ tive health programs in Table 5.26~36 The program appears more cost-effective than many other prevention programs studied.Varicella vaccination appears less cost-effective than previous vaccination programs from the health care payer's perspective, but comparable from the so¬ cietal perspective. From the societal per¬ spective, the vaccination program would save money even when the costs of work loss were assumed to be less than one tenth of those in the base case analysis. This analysis found that for serious varicella complications, including death, the higher the vaccination coverage rate, the lower the cost per health benefit achieved. Compared with a coverage rate of 50%, a vaccination coverage rate of 97% would have roughly half the cost per life-year saved. In addition, the desir¬ ability of a catch-up program for 12-yearolds depends on the coverage of children at school entry. A catch-up program would not be very effective or cost-ef¬ fective if there were 97% coverage of 6-year-olds, but it would have incremen¬ tal costs similar to the basic program costs if coverage rates were 70% or lower. These findings are in basic agreement with a previous analysis of varicella vac¬ cination,2·37 which found benefit-cost ra¬ tios of 0.3 from the health care payer's perspective and 6.9 from the societal perspective. The current study, how¬ ever, differed in several respects. Most important, it took into account the shifts in the age distribution of disease ex¬ pected when most of the population has been vaccinated.3 It incorporated recent data on vaccine efficacy and varicella epidemiology1 and found that the costeffectiveness of routine vaccination was relatively insensitive to estimates of vac¬ cine efficacy parameters over the ranges
suggested by an expert panel.
Downloaded from jama.ama-assn.org at University of California - San Francisco on February 21, 2012
The current analysis included several assumptions that biased its results against a varicella vaccination program. It assumed that chickenpox that oc¬
curred in vaccinated persons would cause 80% of the work loss of chickenpox in unvaccinated persons, but the duration of chickenpox in vaccinated persons is most likely even shorter. Also, health benefits that occurred after the first 30 years were not attributed to those years of the vaccination program, even when they occurred in individuals who were vaccinated in years 1 through 30. These results should be evaluated in light of several limitations. We did not attempt to include the potential benefits or costs of future cases of zoster. Zoster may be clinically milder in vaccinated healthy persons than in unvaccinated per¬ sons,38 but there are, at best, limited data on the long-term incidence of zoster in vaccinated persons.39"11 We also did not include any assumptions regarding the effects of vaccination on congenital vari¬ cella
syndrome. By convention, recent analyses of adult
health programs express their results in cost per year oflife saved. In this analysis, we have presented costs per life-year saved to allow comparisons with other programs. However, the main goal of a routine varicella vaccination program is to prevent suffering from chickenpox or from major complications rather than to save lives. Since varicella causes very few deaths despite many chickenpox cases, a mortality-based outcome measure may underrepresent the program's cost-effective¬ ness. We have not attempted to place a value on the intangible costs of pain and suffering from varicella or to convert the costs of morbidity from chickenpox and nonfatal complications into quality-ad¬ justed life-years. Instead, the results al¬ low the reader to explicitly evaluate these goals of a varicella vaccination program. We conclude that, at a cost of $35 for each vaccine dose, a routine varicella vaccination program for preschool-age children will not save money from the health care payer's perspective, but would still be desirable and would save money from the societal perspective. It
has an acceptable cost per life-year saved compared with other established health interventions. Policymakers will need to base decisions not only on the results of this cost-effectiveness analysis, but also on qualitative judgments, including the relative value of preventing mor¬ bidity and mortality from varicella com¬ pared with that of other diseases. If a program of routine varicella vaccination is adopted, we recommend reevaluating the cost-effectiveness of the interven¬ tion as new data become available. We are grateful to the members of the expert panel on varicella vaccination: Ann Arvin, MD, Philip Branell, MD, Kathryn Edwards, MD, Anne Gershon, MD, Carolyn Bréese Hall, MD, and Sam¬ uel L. Katz, MD. We appreciate the assistance of Edwin M. Lewis, MPH, Paula Ray, MPH, and the many Kaiser Permanente Medical Care Program nurses, research assistants, and patients who con¬ tributed data for this study. We are indebted to Deborah Rennie and Harold
Luft, PhD, and to the California Office of Statewide Planning and Development for help with the Cali¬ fornia Hospital Discharge Database. We acknowl¬ edge Dorothy Rice, PhD, for advice and data on the costs of work loss. We thank Lyn Wender for ed¬ iting. This study is dedicated to the memory of Stephen Preblud, MD.
References 1. Wharton M, Fehrs LJ, Cochi SL, Stroup NE. Health impact of varicella in the 1980s. Read before the 30th Interscience Conference on Antimicrobial Agents and Chemotherapy; October 24, 1990; Atlanta, Ga. Abstract. 2. Preblud SR, Orenstein WA, Koplan JP, Bart KJ, Hinman AR. A benefit-cost analysis of a childhood varicella vaccination programme. Postgrad Med.
1985;61:17-22.
3. Halloran ME, Struchiner CJ, Watelet L. Epidemiologic effects of vaccines with complex direct effects in an age-structured population. Math Biosci. In press. 4. Sullivan-Bolyai JZ, Yin EK, Cox P, et al. Impact of chickenpox on households of healthy children. Pediatr Infect Dis J. 1987;6:33-35. 5. Lieu TA, Black SB, Rieser N, Ray P, Lewis N, Shinefield HR. The cost of chickenpox: parents' perspective. Pediatr Infect Dis J. In press. 6. Expert Panel Conference. Cost-effectiveness of varicella vaccine and acyclovir use. Atlanta, Ga: Centers for Disease Control and Prevention; January 12, 1993. 7. Fleisher G, Henry W, McSorley M, Arbeter A, Plotkin S. Life-threatening complications of varicella. AJDC. 1981;135:896-899. 8. Guess HA, Broughton DD, Melton LJ, Kurland LT. Chickenpox hospitalizations among residents of Olmsted County, Minnesota, 1962 through 1981. AJDC. 1984;138:1055-1057. 9. Jackson MA, Burry VF, Olson LC. Complications of varicella requiring hospitalization in previously healthy children. Pediatr Infect Dis J. 1992; 11:441-v 5. 10. Weibel RE, Neff BJ, Kuter BJ, et al. Live attenuated varicella virus vaccine: efficacy trial in healthy children. N Engl JMed. 1984;310:1409-1415. 11. Kuter BJ, Weibel RE, Guess HA, et al. Oka/ Merck varicella vaccine in healthy children: final report of a 2-year efficacy study and 7-year follow\x=req-\ up studies. Vaccine. 1991;9:643-647. 12. Asano Y, Nagai T, Miyata T, et al. Long-term protective immunity of recipients of the OKA strain of live varicella vaccine. Pediatrics. 1985;75:667-671. 13. Johnson CD, Kumar ML, Rome LP, Fattlar DC, Stancin T. Varicella antibody persistence and reinfections six years post-vaccination. Pediatr Res. 1992;31(No. 4, pt 2):165. Abstract.
14. White CJ, Kuter BJ, Ngai A, et al. Modified of chickenpox after varicella vaccination: correlation of protection with antibody response. Pediatr Infect Dis J. 1992;11:19-23. 15. Arbeter AM, Starr SE, Plotkin SA. Varicella vaccine studies in healthy children and adults. Pediatrics. 1986;78:748-756. 16. Watson BM, Piercy SA, Plotkin SA, Starr SE. Modified chickenpox in children immunized with the Oka/Merck varicella vaccine. Pediatrics. 1993; 91:17-22. 17. White CJ, Kuter BJ, Hildebrand CS, et al. Varicella vaccine (VARIVAX) in healthy children and adolescents: results from clinical trials, 1987 to 1989. Pediatrics. 1991;87:604-610. 18. Cutts FT, Zell ER, Mason D, Bernier RH, Dini EF, Orenstein WA. Monitoring progress toward US preschool immunization goals. JAMA. 1992;267: 1952-1955. 19. Cochi SL, Preblud SR, Orenstein WA. Perspectives on the relative resurgence of mumps in the United States. AJDC. 1988;142:499-507. 20. Kelley PW, Petruccelli BP, Stehr-Green P, Erickson RL, Mason CJ. The susceptibility of young adult Americans to vaccine-preventable infections. JAMA. 1991;266:2724-2729. 21. Dunkle LM, Arvin AM, Whitley RJ, et al. A controlled trial of acyclovir for chickenpox in normal children. N Engl J Med. 1991;325:1539-1544. 22. Balfour HH, Kelly JM, Suarez CS, et al. Acyclovir treatment of varicella in otherwise healthy children. J Pediatr. 1990;116:633-639. 23. Balfour HH, Rotbart HA, Feldman S. Acyclovir treatment of varicella in otherwise healthy adolescents. J Pediatr. 1992;120:627-633. 24. Office of Statewide Health Planning and Development. 1990 Discharge Data. Sacramento: California Dept of Health Services; 1992. 25. Grabowsky M, Markowitz L. Serologic screening, mass immunization, and implications for immunization program. J Infect Dis. 1991;164:1237-1238. 26. Bloom BS, Hillman AL, Fendrick AM, Schwartz JS. A reappraisal of hepatitis B virus vaccination strategies using cost-effectiveness analysis. Ann Intern Med. 1993;118:298-306. 27. Oster G, Huse M, Delea T, et al. Cost-effectiveness of nicotine gum as an adjunct to physician advice against cigarette smoking. JAMA. 1986;256:1315-1318. cases
28. Sisk JE, Riegelman RK. Cost-effectiveness of vaccination against pneumococcal pneumonia: an update. Ann Intern Med. 1986;104:79-86. 29. Littenberg B, Garber AM, Sox HC. Screening for hypertension. Ann Intern Med. 1990;112:192-202. 30. Kinosian BP, Eisenberg JM. Cutting into cholesterol: cost-effective alternatives for treating hypercholesterolemia. JAMA. 1988;259:2249-2254. 31. Wagner JL, Herdman RC, Wadhwa S. Cost\x=req-\ effectiveness of colorectal cancer screening in the elderly. Ann Intern Med. 1991;115:807-817. 32. Healthy Children: Investing in the Future. Washington, DC: US Congress, Office of Technology Assessment; 1988. Publication OTA-H-345. 33. Cochi SL, Broome CV, Hightower AW. Immunization of US children with Hemophilus influenzae type b polysaccharide vaccine. JAMA. 1985; 253:521-529. 34. Hay JW, Daum RS. Cost-benefit analysis of Haemophilus influenzae type b prevention: conjugate vaccination at eighteen months of age. Pediatr Infect Dis J. 1990;9:246-252. 35. White CC, Koplan JP, Orenstein WA. Benefits, risks and costs of immunization for measles, mumps and rubella. Am J Public Health. 1985;75:739-744. 36. Hinman AR, Kaplan JP. Pertussis and pertussis vaccine. JAMA. 1984;251:3109-3113. 37. Preblud SR. Varicella: complications and costs. Pediatrics. 1986;78(suppl):738-735. 38. Plotkin SA, Starr SE, Connor K, Morton D. Zoster in normal children after varicella vaccine. J Infect Dis. 1989;159:1000-1001. 39. Hardy I, Gershon AA, Steinberg SP, LaRussa P, and the Varicella Vaccine Collaborative Study Group. The incidence of zoster after immunization with live attenuated varicella vaccine. N Engl J Med. 1991;325:1545-1550. 40. Brunell PA, Taylor-Wiedeman J, Geiser CF, Frierson L, Lydick E. Risk of herpes zoster in children with leukemia: varicella vaccine compared with history of chickenpox. Pediatrics. 1986;77:53-56. 41. Lawrence R, Gershon AA, Holzman R, Steinberg SP, and the NIAID Varicella Vaccine Collaborative Study Group. The risk of zoster after varicella vaccination in children with leukemia. N Engl J Med. 1988;318:543-548.
Downloaded from jama.ama-assn.org at University of California - San Francisco on February 21, 2012