■ Feature Article
Does Adding Computed Tomography Change the Diagnosis and Treatment of Tillaux and Triplane Pediatric Ankle Fractures? FRANK A. LIPORACE, MD; RICHARD S. YOON, MD; ERIK N. KUBIAK, MD; DEBRA M. PARISI, MD; KENNETH J. KOVAL, MD; DAVID S. FELDMAN, MD; KENNETH A. EGOL, MD
abstract Full article available online at ORTHOSuperSite.com. Search: 20120123-11 Computed tomography (CT) has been deemed a necessary part of management for Tillaux and triplane pediatric ankle fractures. However, no previously published study has attempted to quantify its usefulness in changing management. Six third-party, blinded orthopedic surgeons (F.A.L., E.N.K., D.M.P., K.J.K., D.S.F., K.A.E.) were randomly assigned to evaluate 24 pediatric Tillaux or triplane fractures with plain radiographs; after 6 months, they were again randomly assigned to evaluate the 24 radiographs plus CT scans, totaling 144 third-party, blinded evaluations. Intra- and interobserver agreements were assessed via correlation coefficient analysis. Evaluation of CT scans changed the original diagnosis of fracture type from Tillaux to triplane fracture in 7 (4.9%) of 144 evaluations. Inter- and intraobserver agreements regarding primary treatment plans did not significantly differ between radiographs and radiographs plus CT scans (0.5 vs 0.4, respectively; P⬎.05). The addition of CT did not significantly change the impression of the amount of displacement per case. By adding CT, more patients who were assigned nonoperative management were reassigned to operative treatment (P⫽.033). Adding CT, although it may influence the decision to operate on Tillaux and triplane fractures, may not be as useful as previously thought.
A
B
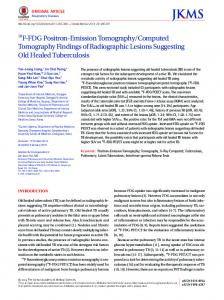
Figure: Anteroposterior (A) and lateral (B) radiographs of a pediatric, intra-articular distal tibia fracture.
Dr Liporace is from the Division of Orthopaedic Trauma, Department of Orthopaedic Surgery, UMDNJ – New Jersey Medical School, Newark, New Jersey; Drs Yoon and Egol are from the Division of Orthopaedic Trauma and Dr Feldman is from the Division of Pediatric Orthopaedic Surgery, Department of Orthopaedic Surgery, NYU Hospital for Joint Diseases, New York, New York; Dr Kubiak is from the Division of Orthopaedic Trauma, Department of Orthopaedic Surgery, The University of Utah, Salt Lake City, Utah; Dr Parisi is from the Department of Orthopaedic Surgery, Beth Israel Orthopaedics and Sports Medicine, New York, New York; and Dr Koval is from the Division of Orthopaedic Trauma, Department of Orthopaedic Surgery, Orland Regional Medical Center, Orlando, Florida. Drs Liporace, Yoon, Kubiak, Parisi, Koval, Feldman, and Egol have no relevant financial relationships to disclose. Correspondence should be addressed to: Frank A. Liporace, MD, Division of Orthopaedic Trauma, Department of Orthopaedic Surgery, UMDNJ – New Jersey Medical School, 90 Bergen St, Ste 1200, Newark, NJ 07101 (
[email protected]). doi: 10.3928/01477447-20120123-11
e208
ORTHOPEDICS | ORTHOSuperSite.com
USEFULNESS OF CT IN TREATING PEDIATRIC ANKLE FRACTURES | LIPORACE ET AL
D
istal tibial fractures account for approximately 5% of pediatric fractures and 15% of physeal injuries and are twice as common in boys (Figure 1).1-3 When treating children with ankle fractures, 2 important goals exist: (1) achieving a satisfactory reduction; and (2) avoiding physeal arrest to minimize the risks of angular deformity, early arthrosis, leg-length inequality, and joint stiffness.4 The fusion pattern of the distal tibia’s epiphysis explains the configuration of the fragments in triplane and Tillaux ankle fractures. These patterns of injury result from a supination–eversion or external rotation force, typically in patients with a mean age of 13.5 years.5,6 Although plain radiography has been cited as the mainstay in the diagnosis of pediatric ankle fractures, computed tomography (CT) has been cited as a useful adjunct for the evaluation of intra-articular pediatric ankle fractures.7-9 The spatial re-
lation of major fracture fragments may be appreciated by examining the axial, sagittal, and coronal plane reconstructions, in addition to offering important information regarding articular splits and depressions, along with fracture comminution and alignment (Figure 2).6,10,11 To our knowledge, although previous retrospective series have reported that CT is a necessary adjunct in treating Tillaux and triplane ankle fractures, no previously published study has quantitatively assessed CT as a useful adjunct to plain radiographs in this setting.9,12 The current study outlines the influence of adding CT to plain radiographs compared with radiographs alone in the diagnosis, decisionmaking process, and treatment of Tillaux and triplane ankle fractures. Based on previous literature, our null hypothesis for this study was that CT provides a useful adjunct in the decision-making process in the treatment of Tillaux and triplane pediatric ankle fractures. Thus, using intra- and interobserver agreements, our hypothesis was that there should be an increase in agreement when CT is added to plain radiographs.
MATERIALS AND METHODS
1A
1B
Figure 1: Anteroposterior (A) and lateral (B) radiographs of a pediatric, intra-articular distal tibia fracture.
Between January 2001 and January 2003, an initial diagnostic code search for a diagnosis of Tillaux or triplane fracture was performed. Inclusion criteria were cases with complete plain radiographic and CT series to create the radiographic library for analysis and cases that were not
2 Figure 2: Axial computed tomography scan of intra-articular distal tibia fracture.
FEBRUARY 2012 | Volume 35 • Number 2
treated by any of the 6 third-party, blinded evaluators (F.A.L., E.N.K., D.M.P., K.J.K., D.S.F., K.A.E.). A total of 24 cases met the criteria for inclusion. Cases without a CT scan and those that went immediately to the operating room were excluded. Evaluation, assessment, and data collection were performed by 6 blinded, thirdparty orthopedic surgeons in a test/retest experimental design. Cases were assigned in a randomized fashion. Radiographic review was performed on 2 separate occasions with a 6-month interval between. Plain radiographs alone were assessed on the first occasion, and, on the second occasion, plain radiographs plus CT were assessed, totaling 144 evaluations. Following each plain radiograph review, a questionnaire was administered asking the reviewer to determine diagnosis (Tillaux versus triplane), amount of displacement, treatment plan (closed reduction with casting, closed reduction with percutaneous pinning [CRPP], or open reduction and internal fixation [ORIF]). The treatment plan was kept more general to avoid further subgroups of treatment. For example, CRPP was deemed those managed via Kirschner wires or via cannulated screws, and ORIF was deemed any open reduction combined with any type of fixation. Keeping the groups general provided for a more consistent and less confusing analysis, avoiding bias and removing surgeon preference as a variable. Following each plain radiograph plus CT review, a questionnaire was administered to determine changes in diagnosis, perceived displacement, and treatment plan. All radiographs provided were de-identified, and questionnaires were completed within 30 minutes of film review as a study requirement. Statistical analysis was performed with SPSS version 18.0 software (IBM, Inc, Armonk, New York). Inter- and intraobserver agreement were analyzed via intraclass correlation coefficient (ICC), interpreted as follows: poor (0-0.2), fair (0.3-0.4), moderate (0.5-0.6), strong (0.7-
e209
■ Feature Article
0.8), and almost perfect (⬎0.8) (Table 1).13 Categorical data were analyzed via Fisher’s exact test. Significance was set at P⬍.05.
RESULTS In 7 (4.8%) of 144 evaluations, CT scan changed the original diagnosis of fracture type from Tillaux to triplane. Using an ICC to evaluate patients with plan radiographs vs plain radiographs plus CT, inter- and intraobserver agreement for classifying fracture type were 0.73 and 0.43, indicating strong and fair-to-moderate agreement, respectively; no significant difference was observed between agreements (P⫽.05). When comparing treatment chosen with and without the addition of CT scan to plain radiographs, inter- and intraobserver agreements were 0.5 and 0.4, indicating moderate and fair agreement, respectively; no significant difference was observed between agreements (P⬎.05). After reviewing CT scans, an additional 19 (13%) of 144 evaluations (P⫽.033) that were initially assigned nonoperative management were reassigned to operative management (6 to CRPP; 13 to ORIF) (Table 2; Figure 3). In the operative group, when CT scans were added to plain radiographs, no significant increase was seen in the proportion of cases assigned ORIF vs CRPP (P⬍1.0) (Figure 4).
Plain radiographic evaluation was the study most frequently cited as having the greatest influence on treatment (68%), followed by axial CT (11%), coronal CT (8%), and sagittal reconstruction (6%). The addition of CT scan to radiographic evaluation did not significantly change the impression of the quantity of displacement per case (Table 3).
formity.18 Ertl et al12 reported that malreduction of the articular surface of ⬎2 mm has been correlated with poor long-term out-
Table 1
Intraclass Correlation Coefficient Interpretation Values Strength of Agreement
DISCUSSION
Agreement Value
Almost perfect ⬎0.8 Typically occurring in patients aged Strong 0.7-0.8 approximately 12 to 14 years, Tillaux Moderate 0.5-0.6 fractures (Salter III fractures of the anterolateral portion of the tibia) and triplane Fair 0.3-0.4 fractures (Salter IV fractures that have Poor 0-0.2 components in the sagittal, coronal, and transverse planes) can be a diagnostic challenge.12,14-16 Table 2 Articular displaceTreatment Plan Based on Radiographic Evaluation ment of ⬎2 mm is generally consid% ered an indication Plain Plain Radiographs Radiographs⫹CT P for reduction of the articular surface.11,17 Nonoperative 52 39 .033 Misdiagnosis and Operative 48 61 treatment that does CRPP 15 19 not produce anatomic ORIF 33 42 reduction can result Abbreviations: CRPP, closed reduction with percutaneous in premature physeal pinning; CT, computed tomography; ORIF, open reduction internal fixation. closure and the aforementioned risks of de-
3
4
Figure 3: Following the addition of computed tomography (CT) scans to radio- Figure 4: The addition of computed tomography (CT) to radiographs (Xray) did graphs (Xray), a significant increase in change from nonoperative (cast) to opera- not significantly change the type of operative treatment; no significant change tive management was observed (P⬍.05). was observed in closed reduction with percutaneous pinning (CRPP) vs open reduction internal fixation (ORIF) with the addition of computed tomography, but a significant shift occurred toward operative management as definitive treatment.
e210
ORTHOPEDICS | ORTHOSuperSite.com
USEFULNESS OF CT IN TREATING PEDIATRIC ANKLE FRACTURES | LIPORACE ET AL
Table 3
Average Impression of Fracture Displacement by Surgeon mm Surgeon No. 1
Plain Radiographs
Plain Radiographs⫹CT
Changea
1.7⫾2.1
1.2⫾2.0
⫺0.5
2
3.4⫾3.2
3.5⫾2.3
0.1
3
1.6⫾1.1
2.1⫾1.8
0.5
4
1.5⫾0.9
1.6⫾1.1
0.1
5
2.4⫾2.5
1.9⫾1.5
⫺0.5
6
2.7⫾2.3
2.1⫾0.7
⫺0.6
CONCLUSION
Abbreviation: CT, computed tomography. a No significant differences were observed.
comes, with 7 of 15 patients having residual symptoms after 3 to 13 years of follow-up. Rapariz et al9 noted similar conclusions, reporting that CT was a mandated necessary step of management in this fracture cohort. Accepted modes of treatment include casting, percutaneous reduction with wire or screw fixation, and ORIF.19-21 Our data show that when presented with the same plain radiographic workup, reviewers generally agreed on the classification of the fracture. However, the addition of CT scans had the potential to change the reviewers’ original classification. Provided with more information, agreements fell from a strong agreement (0.73) to a fair-to-moderate (0.43) rating. Rejecting our null hypothesis, agreement fell instead of increasing when adding CT. A recent study reported that plain radiographs and CT were accurate within 1 mm in depicting fracture displacement approximately 50% of the time.11 Computed tomography was more sensitive than plain radiographs in detecting fractures with ⬎2 mm of displacement.11 However, we found that a reviewer’s impression of the amount of fracture displacement was not significantly altered by the addition of CT scan, regardless of displacement. Despite lack of agreement, the addition of CT scans to plain radiographs significantly changed the treatment plan from nonoperative to operative management
FEBRUARY 2012 | Volume 35 • Number 2
change to operative management. One of the major findings in our study, specific reasons (ie, location of fracture lines relative to the weight-bearing surface, newly recognized fractures lines on CT, rotational aspect) would have offered insight into the significant change from a nonoperative to operative treatment plan. Furthermore, more pointed reasons, such as avoiding the risk of future complications in this pediatric complication as a reason for surgery, may have also proved helpful.
in 19 (13%) of 144 evaluations. Provided with CT, the decision to operate, whether via CRPP or ORIF, significantly increased despite our data indicating lack of agreement, minimal diagnostic change, and an insignificant, low rate of patients moving from the nonoperative to operative groups. Past literature deemed CT scans a necessary part of the workup for Tillaux and triplane pediatric ankle fractures.9,12,22,23 However, some studies have reported that not all surgeons have been following this pattern, as a postal survey of surgeons revealed that only 38% always request CT scans before treating triplane fractures.7 Furthermore, our data do not fully support CT as a useful adjunct, exhibiting evidence against our original null hypothesis. Furthermore, despite lower agreement and nonsignificant changes in additional information with the addition of CT, a significant increase in change in operative management with the addition of CT was a contradictory finding. However, when concerning the pediatric population, this finding may be contributed to today’s litigious society, with the benefits of avoiding future arthritis and decreased function outweighing the risks of an operation and potential complications of nonoperative treatment. The major limitation of the current study was our lack of specificity in regard to surgeons’ assessment in initial treatment plan and what prompted a subsequent
Despite the established literature reporting CT scan as a necessary adjunct to the treatment of Tillaux and triplane pediatric ankle fractures, no prior study quantifies its usefulness. Data from our correlation study rejected our null hypothesis, exhibiting little benefit to CT as a necessary adjunct in this fracture cohort. However, although a blinded, third-party evaluative, test/retest experimental design offers valuable information, a prospective, randomized trial may offer a more definitive look at the true usefulness of CT in assessing pediatric ankle fractures.
REFERENCES 1. Mizuta T, Benson WM, Foster BK, Paterson DC, Morris LL. Statistical analysis of the incidence of physeal injuries. J Pediatr Orthop. 1987; 7(5):518-523. 2. Peterson CA, Peterson HA. Analysis of the incidence of injuries to the epiphyseal growth plate. J Trauma. 1972; 12(4):275-281. 3. Worlock P, Stower M. Fracture patterns in Nottingham children. J Pediatr Orthop. 1986; 6(6):656-660. 4. Kay RM, Matthys GA. Pediatric ankle fractures: evaluation and treatment. J Am Acad Orthop Surg. 2001; 9(4):268-278. 5. Dailiana ZH, Malizos KN, Zacharis K, Mavrodontidis AN, Shiamishis GA, Soucacos PN. Distal tibial epiphyseal fractures in adolescents. Am J Orthop (Belle Mead NJ). 1999; 28(5):309-312. 6. Kärrholm J, Hansson LI, Laurin S. Computed tomography of intraarticular supination– eversion fractures of the ankle in adolescents. J Pediatr Orthop. 1981; 1(2):181-187. 7. Jones S, Phillips N, Ali F, Fernandes JA, Flowers MJ, Smith TW. Triplane fractures of the distal tibia requiring open reduction
e211
■ Feature Article
and internal fixation. Pre-operative planning using computed tomography. Injury. 2003; 34(4):293-298.
13. Portney L, Watkins M. Foundations of Clinical Research Applications to Practice. Upper Saddle River, NJ: Prentice Hall; 2000.
19. Kling TF Jr. Operative treatment of ankle fractures in children. Orthop Clin North Am. 1990; 21(2):381-392.
8. Vanhoenacker FM, Bernaerts A, Gielen J, Schepens E, De Schepper AM. Trauma of the pediatric ankle and foot. JBR-BTR. 2002; 85(4):212-218.
14. Dias LS, Giegerich CR. Fractures of the distal tibial epiphysis in adolescence. J Bone Joint Surg Am. 1983; 65(4):438-444.
20. Manderson EL, Ollivierre CO. Closed anatomic reduction of a juvenile tillaux fracture by dorsiflexion of the ankle. A case report. Clin Orthop Relat Res. 1992; (276):262-266.
9. Rapariz JM, Ocete G, González-Herranz P, et al. Distal tibial triplane fractures: longterm follow-up. J Pediatr Orthop. 1996; 16(1):113-118. 10. Feldman F, Singson RD, Rosenberg ZS, Berdon WE, Amodio J, Abramson SJ. Distal tibial triplane fractures: diagnosis with CT. Radiology. 1987; 164(2):429-435. 11. Horn BD, Crisci K, Krug M, Pizzutillo PD, MacEwen GD. Radiologic evaluation of juvenile tillaux fractures of the distal tibia. J Pediatr Orthop. 2001; 21(2):162-164. 12. Ertl JP, Barrack RL, Alexander AH, VanBuecken K. Triplane fracture of the distal tibial epiphysis. Long-term follow-up. J Bone Joint Surg Am. 1988; 70(7):967-976.
e212
15. Spiegel PG, Cooperman DR, Laros GS. Epiphyseal fractures of the distal ends of the tibia and fibula. A retrospective study of two hundred and thirty-seven cases in children. J Bone Joint Surg Am. 1978; 60(8):10461050. 16. Cooperman DR, Spiegel PG, Laros GS. Tibial fractures involving the ankle in children. The so-called triplane epiphyseal fracture. J Bone Joint Surg Am. 1978; 60(8):1040-1046. 17. Koury SI, Stone CK, Harrell G, La Charité DD. Recognition and management of Tillaux fractures in adolescents. Pediatr Emerg Care. 1999; 15(1):37-39. 18. Barmada A, Gaynor T, Mubarak SJ. Premature physeal closure following distal tibia physeal fractures: a new radiographic predictor. J Pediatr Orthop. 2003; 23(6):733-739.
21. Schlesinger I, Wedge JH. Percutaneous reduction and fixation of displaced juvenile Tillaux fractures: a new surgical technique. J Pediatr Orthop. 1993; 13(3):389-391. 22. Cutler L, Molloy A, Dhukuram V, Bass A. Do CT scans aid assessment of distal tibial physeal fractures? J Bone Joint Surg Br. 2004; 86(2):239-243. 23. Shin AY, Moran ME, Wenger DR. Intramalleolar triplane fractures of the distal tibial epiphysis. J Pediatr Orthop. 1997; 17(3):352-355. 24. Kim JR, Song KH, Song KJ, Lee HS. Treatment outcomes of triplane and Tillaux fractures of the ankle in adolescence [published online ahead of print February 4, 2010]. Clin Orthop Surg. 2010; 2(1):34-38.
ORTHOPEDICS | ORTHOSuperSite.com





































![usa.siemens.com/computed-tomography [PDF]](https://m.moam.info/img/260x300/usasiemenscom-computed-tomography-pdf_6479f808098a9ec7448b4651.jpg)







