Making Data Collection in Low-resource Contexts Intuitive, Fun, and Interactive Greg Wenner, Martin Marino, Eric Obeysekare, Khanjan Mehta
Humanitarian Engineering & Social Entrepreneurship (HESE) Program The Pennsylvania State University University Park, PA Correspondence:
[email protected] Abstract—Community health data can be used to track diseases, facilitate efficient deployment of medical resources, or reduce clinic wait times in fledgling healthcare systems in developing countries. Despite these potential benefits, many electronic data collection, aggregation and digitization projects fail within a few years of launching. Over a three-year span, Community Health Workers (CHWs) operating our telemedicine venture in East Africa retrogressed from using laptops and netbooks, to smartphones and basic cell phones, to pen and paper. The reasons for these technology downgrades can be attributed to diverse contextual, business-related, communication, coordination, and technological challenges that compromise the collection of data. To address this health data collection challenge, our team has designed intuitive, fun, powerefficient, and rugged devices that draw on principles of tangible computing, user-centered design, and interaction design. By incorporating lights, sounds, and instant feedback, these devices are designed to become a natural part of CHW-client interactions rather than cumbersome, intrusive distractions. This article describes the design of three interactive prototypes to gamify the health data collection process and preliminary test results from their deployment in Kenya.
The use of data to improve health and healthcare delivery is particularly important in the developing world, where life expectancies are much lower and healthcare systems are still rudimentary. Medical data can be used to track diseases, monitor immunization programs, improve clinic wait times, facilitate the efficient deployment of medical resources, and train healthcare personnel. However, there are numerous challenges that hinder the collection of health data in resource constrained communities [6]. These challenges can be classified as contextual, business-related, communication and coordination, or technological. Contextual issues, such as infrastructure limitations, are specific to where data is collected. Business challenges, like employee turnover, must be considered as ventures collecting these data need to fund their efforts. Communication and coordination challenges, like language differences and potentially inaccurate data, can affect the usability of collected data. Finally, technological challenges, the category of challenges most often thought of, can cause loss of data or failure of equipment used by a venture. Collectively, these challenges prevent many projects from obtaining, aggregating, and digitizing data.
Keywords—Data collection, Community Health Workers (CHWs), gamification, tangible computing, Fun Theory
Community Health Workers (CHWs) are unpaid government-trained health workers who provide very basic health services in their communities. CHWs can combat the lack of trained physicians in low-resource environments [7]. CHW programs are becoming more popular in the developing world. In 2011, the World Health Organization estimated that there are more than 1.3 million CHWs worldwide [8]. These CHWs are essential to data collection efforts because they are on the ground in communities and thus have the ability to reach many individual patients. Because of their positions and locations in the community, CHWs must deal with many of the challenges to medical data collection [6]. Successful data collection ventures can leverage CHWs and provide them with products that incentivize and empower them to collect data needed to improve health systems.
I. INTRODUCTION Governments and NGOs operating in low-resource contexts are realizing the need for data to support and guide their development efforts. The Population Council, when looking at the demand for data in developing countries, found that data is crucial for development [1]. Access to reliable data enables policy makers to make better decisions regarding resources and interventions. Recognizing the need for these data, development organizations such as the Canadian Department of Foreign Affairs, Trade, and Development (DFATD) and the United States Agency for International Development (USAID), sponsor programs that are searching for ways to use data for development [2], [3]. Private sector organizations also acknowledge the importance of data. For example, Orange, a large telecommunications provider, conducted the Data for Development (D4D) Challenge. D4D provided a large set of telecommunications data taken from Cote d’Ivoire during a six month period to teams of researchers, challenging them “to help address society development questions in novel ways” [4]. Teams used these data to optimize public transport, look at communication patterns, and even do health-related analyses like tracking disease outbreaks [5]. 978-1-4799-7193-0/14/$31.00 ©2014 IEEE
CHWs of the Mashavu mHealth venture, operating in Nyeri, Kenya were given such a device for testing and evaluation. Mashavu is a flagship mHealth venture of the Penn State Humanitarian Engineering and Social Entrepreneurship (HESE) program that aims to increase basic knowledge of health among community members. The device was designed by the HESE data collection team with Mashavu CHWs in mind. This device must integrate with existing CHW practices and be intuitive, rugged, and power-efficient to succeed. Data collected through the device will be aggregated to a central 49
IEEE 2014 Global Humanitarian Technology Conference
location where it can be harnessed for the development of these communities. This article will describe the design of the data collection device and explore how this device can be integrated into Mashavu. After examining related work that justifies the approach, this article will describe current Mashavu operations and challenges faced by its CHWs. Next, the design of the device will be described in-depth with explanation of the design choices made. Finally, two alternative designs are presented along with a deployment and evaluation plan for field work to be conducted in Kenya and Sierra Leone. This article is written from the perspective of a mobile healthcare venture that has the goal of collecting data about community members in its operating regions. Data collection device design is relevant to researchers and other ventures interested in collecting data in low-resource environments, especially those that are health-focused. II. RELATED WORK The gamification of data collection is an emerging field. While other attempts have been made at collecting health data (and other types of data) in resource constrained environments, there is a lack of literature detailing gamified, interactive approaches. Gamification is the incorporation of game-like mechanics in real world settings. The goal is to turn a boring task into an exciting one, at the same time speeding it up [9]. A study in which gamification was included into a classes’ curriculum showed varying results. Points were rewarded for assignments that were completed resulting in higher reported motivation to complete work [9]. A device can also be gamified by tracking and recording data. Presenting data over time to a user can be rewarding and motivate them to set higher goals [10]. Nike+ does this by tracking how far the user runs and logging achievements. [11]. Other techniques can be combined with gamification to add an element of fun to a task. The Fun Theory is a concept built around making jobs or actions fun. This theory uses sensory feedback to motivate the user. For example, the World’s Deepest Bin is used to encourage more people to throw their trash into a garbage can instead of onto the ground. Throwing trash into the can triggers a fun, cartoon-like sound [12]. This instantaneous reward for performing a civic duty resulted in increased garbage can usage. In order for the Fun Theory to be successfully implemented, tangible and ubiquitous computing should be used to improve how physical objects are interacted with. Tangible computing is the interaction and manipulation of physical objects in order to augment how we view a virtual space. It is natural for humans to want to use their hands when performing tasks. Tangible user interfaces can also enhance face-to-face interactions by having users focus on physical objects and use their hands rather than focusing solely on a screen [13]. For example, using physical inputs to modify virtual settings, makes a system more interactive [14]. After an extensive search for literature regarding ventures in health data collection, none have utilized tangible computing. There have been some approaches to data collection in lowresource environments. A literature review of other attempts
found a lack of information in this area and proposed a mobile phone based solution [15]. The USAID-AMPATH (Academic Model Providing Access to Healthcare) provided pre-primary healthcare via home visits to people in Western Kenya [16]. CHWs were able to collect basic health information using PDAs and smartphones. Using PDAs was easier than recording data on paper, but the small screen and keyboard size made entering and reading data difficult. Another example is an Integrated eHealth Center (eHC). The setup uses a local server that allows it to send and receive clinical health data. This requires a reliable power source and maintenance [17]. Another example is an eMedical Record system in Haiti that uses a checklist to collect clinical patient data. This venture had difficulties relating to Internet latency, correct identification of patients, and accuracy of collected data [18]. In Umlazi, South Africa, two dozen women were hired as CHW’s to collect health data by using mobile phones to survey over 35,000 homes in four months. Mobile phones allow for real-time tracking of data and identification of generated data [19]. The Mosoriot Medical Record System (MMRS) is an electronic medical record system (eMR) in rural Kenya. This system allows a patient to electronically register with the MMRS where they are given an identification card to carry. This system facilitates patient data entry and identification [20]. Media Lab Asia has developed a Health Information Management System (HIMS) for CHWs to collect health data using mobile devices. This system is used in 20 different locations [21]. DoctorMe is a web/mobile application in Thailand that uses gamification to identify trending symptoms searched by users. It should soon be able to collect patient health data and is one of the most popular applications in the health and fitness category of applications in Thailand [22]. Tangible computing devices are more intuitive to use. This is important when trying to collect data in areas that have low computer literacy. Using gamification and Fun Theory can also motivate the tedious process of data collection and make it more enjoyable. Combining these concepts provides a promising new direction for health data collection. III. MASHAVU CASE STUDY Mashavu is a mobile health (mHealth) program that offers affordable services to community members [23]. Community Health Workers (CHWs) are provided a backpack that contains the medical equipment required for Masahvu work. The CHWs travel to rural areas and provide a ‘Know Your Numbers’ service that includes data such as height, weight, age, blood pressure, and BMI. These services generate income for the CHW and empower the community with personal health information. Following the interaction, the CHW records all of the collected data in a carbon-copy receipt book and gives a copy to the client. CHWs keep a copy of the receipt from each consultation. A. Past Data Collection Efforts Mashavu initially provided CHWs with laptops at stationary kiosks on which to enter data. This method was laborious, and was phased out when Mashavu became a mobile venture [24]. In 2012, Mashavu provided CHWs with smartphones to collect data via a web form. Although the
CHWs were able to quickly enter the data during the consultations, issues including network unreliability, fear of theft, and users forgetting their passwords forced Mashavu to revert to using receipt books [6], [25]. Data collection on receipt books does not allow for efficient data digitization and analysis. Optical character recognition (OCR) was tested on receipts from consultations, but the CHWs’ hand writing was inconsistent and yielded incorrect or missing data. B. Data Digitization Challenges Completed receipt books also introduce privacy issues when they are transported or stored in an insecure manner. 1) Lack of Incentives Lack of incentives has been a large issue in previous iterations of this project. The CHWs expressed that entering the data was “silly” and unnecessary. Even after explaining the potential benefits of this data collection, the CHWs were still unwilling to do it. For a short time, monetary rewards were given to the CHWs for their digital data collection efforts, but that proved to be an insufficient incentive. By providing efficiency, sensory feedback, and ease of use, it is possible to indirectly incentivize the use of the device. Potential clients may be dissuaded from using the service if they know that their data is being digitized. Previously, frequent news stories in Kenya of citizens being falsely registered to rival political parties prevented many people from using Mashavu’s service [25]. 2) Data Reliability Eliminating user error is essential for providing reliable data. For example, a common error during the initial Mashavu pilot was incorrect height data, mostly due to the omission of a decimal point. Incorporating a maximum height enforced by the web form prevented the error from propagating through the system [6]. When designing information collection systems, it is important to restrict low-level details so that only valid data can be entered. Implementation of new technologies should not hinder CHWs regular work patterns. For example, if CHWs were paid per set of data entered, they would be inclined to enter as many records as possible. This could involve expediting the consultations or fabricating records to enter. Both of these outcomes result in data inconsistency. 3) Education Technology education is not as widespread in developing countries as it is in developed ones. Although most individuals have cellphones, other personal technologies are sparse. CHWs were unfamiliar with the smartphone and laptop platforms, and even after training found them tedious. When considering technologies to integrate, it is important to leverage the formats and platforms that the people are already familiar with, or that are easy to learn. In addition to hands-on training with the technology, customized literature should be provided in the native language [25]. 4) Contextual Challenges Normal wear and tear on technology is amplified in low-resource environments. Protection from the elements can be challenging in developing countries. Data collection devices
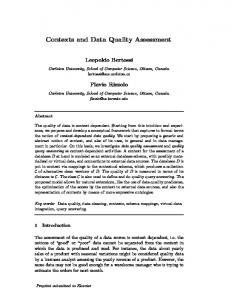
must be mobile; this increases the chance of damage. Moisture, dust, and heat are other serious factors that affect the longevity of technology. Establishing a reliable and accurate system to manage the flow of data is challenging because of resource constraints. Auxiliary collection methods and backups are essential when working in conditions where technology often fails. For example, when Mashavu’s smartphones experienced network connectivity issues, the consultations took longer than usual, or the data was not entered. Additionally, the price of data transfer can be significantly higher in developing countries [25]. Some countries also have laws and restrictions regarding the collection and storage of patient health data. IV. SYSTEM DESIGN Smartphones and laptops proved improper for data collection in previous iterations of Mashavu, leading to the design of a radically new data collection system tailored to the end-users, CHWs. This system aims to decouple the physical data collection systems from the data transfer and analysis functions. When the CHWs were using smartphones, they were responsible for connecting to the network and loading the web form. The addition of a new device has eliminated this extra step. Upon the entry of the client health data, the device will transmit the information to an idle Android application on the CHW’s smartphone via Bluetooth. This device implements a “store and forward” system, which stores the data in the cell phone until it has a reliable connection to the cellular network. It then forwards the data to the database in the cloud. The user need not enter data on complicated, multifunctional devices and the device allows for data entry even when a mobile data connection is not available. Fig. 1 shows the data collection device and other devices used by the CHW during a consultation. V. DEVICE DESIGN Fun, intuitiveness, and familiarity have been emphasized in conceptualization of these designs in an effort to gamify the process of data collection. Engaging the user’s senses increases the usability and readability of technology, making it more efficient and enjoyable to operate. This new approach stems from the concept of user-centered design and draws from many business innovations in the developed world. The team took several crucial preliminary design steps before coming to the three final designs. First, the team compiled an extensive list of potential attributes that could be included in the device. After analyzing how each one contributes, they were rated and the team used the most logical combination of features to decide on three designs. The following section outlines the primary design, the logic behind design decisions, and alternatives considered. A. Prototyping The team underwent rapid prototyping to create three preliminary designs of the data collection device. These devices were tested with CHWs to determine the best attributes for the final device. Fig. 2 shows one of the completed prototypes that was used for testing and validation.
Fig. 1. Systems Diagram
introduced from closely clustered controls. Clients are also better able to see their data being entered onto the device, allowing more engagement and reducing potential error.
Fig. 2. Prototype Device
B. Design Choices Ideally, this new approach and design would address several challenges including, but not limited to cost, ruggedness, and reliability. Unfortunately, these factors sometimes conflict with one another and require compromise. For example, a conveniently sized device may not be the most durable. The final design finds a comfortable balance between the aforementioned goals while prioritizing the end-user experience. Fig. 3 shows a mockup of the final device design. 1) Platform The decision to use a tablet design was based around its simplicity and readability. Smaller devices like watches and phones are more expensive, difficult to ruggedize, and can be easily misplaced. A tablet-sized device offered a larger canvas for tangible inputs (e.g. lights and sounds) that engage the user’s senses and gamify the data entry process. Devices formatted to mimic phones or watches do not allow for the physical controls that are conducive to straightforward data entry. Larger surface area also helps to mitigate user error
Convenience and usability may be enhanced in a number of ways. The goal of wearable technology is to incorporate it into the user’s life; remaining unobtrusive while improving quality [26]. To do this, it must be efficient and comfortable to wear. Watches are a simple example of how wearable devices can be efficient without being a nuisance. This becomes significantly more difficult when the device in question must be low cost, specialized, and mobile. Wearing the technology also reduces the chances of the device being stolen. There are many ways to implement wearable technology, but two have proven to be the most effective. A necklace attachment has been added to the design that connects at the bottom of the device, so that it hangs freely near the abdomen while not in use. The user may then use both hands for other tasks, and not have to set the device down. Another considered design modification is a band connected to the back of the device to wrap around the forearm, allowing the device to be worn like a watch. The user would then operate the device with the opposite hand. The necklace attachment would allow for full use of both hands. If preferred, both of these attachments can be removed easily. The device will be powered by an Arduino microcontroller. Microcontrollers are small, relatively cheap computing units that can be easily programmed for use with custom devices and applications. The Arduino will handle all data processing on the device as well as send the data over Bluetooth. Arduino was chosen for its simplicity and versatility.
Fig. 3. Mockup of Device
2) Power Availability, cost, maintenance, failure modes, and the environmental repercussions must be assessed when considering powering methods. Non-rechargeable batteries introduce materials that are not biodegradable or environmentally sustainable. CHWs are required to replace the depleted batteries on a regular basis, decreasing the appeal of the device. However, non-rechargeable batteries can easily be replaced if they die, and are abundant and relatively low-cost in these environments [27]. Additionally, electricity required to charge reusable batteries may be difficult to come by and may introduce additional costs to the workers, lowering their bottom line. Rechargeable batteries also degrade slowly over time and have a limited lifetime. Replaceable batteries will provide a more linear, spread out cost pattern than the one-time purchase of a rechargeable battery or solar device.
International Telecommunications Union estimates that in 2013 there were 63 mobile phone subscriptions per 100 people in Africa [28]. An even higher percentage of individuals have access to cellphones, making the keypad a familiar tool. This will be a fast method of data entry, especially for data points with large value ranges, but possibly not as engaging as other data entry methods. Keypads are more susceptible to environmental conditions than many other data entry devices because of the many moving parts. Usually, a keypad consists of twelve buttons, allowing for twelve separate failure points. This provides a cheap and familiar medium on which to enter data. They are the simplest form of data entry, performing only one function. Unlike keypads that provide many failure points, the button has only one with a small range of motion. This combined with its simplicity, prompts its use wherever the data allows.
Nontraditional power methods like solar are also being considered for future designs of this device. Cost, failure modes, upkeep, and environmental issues are all factors that will influence the adoption of alternate technologies.
Switches, like sliders, provide an inexpensive and intuitive data input method. Like dials, they do not provide support for data points with large ranges because of their small size. These are best utilized for data that require only two to three possibilities like gender. Their small size and limited movement range make them one of the more durable data input methods.
3) Data Input Data entry methods have been a focus throughout the design process. Incorporating tangible data entry methods like sliders, dials, keypads, buttons, and switches will facilitate better client interaction. The client can easily view what the CHW is doing, verify their actions, and be a part of the data entry process. The size and format of each data input is important because it directly affects which data values they can most efficiently collect. Physical inputs allow for discrete entry of each desired value. This enhances the CHW’s ability to learn, remember, and eventually assimilate the device into their everyday routine. Sliders and dials are two options of tangible data input components. Keypads are moderately inexpensive and easy to understand because of their ubiquitous nature. The
4) Data Output Data output methods in low-resource environments must be power efficient and easy to maintain and repair. The user must be able to view the entered data to verify the input is set to the proper value. Seven-segment displays, a block that uses a combination of seven line segments to construct any digit, is the most efficient method for simple numerical data and will be used on the device. These blocks are easy to install, program, and are extremely power efficient when compared to LCD screens. They are more readable than LCD screens and do not require a backlight, offering superior durability and longevity.
To deliver the data to the client, CHWs currently record data on paper receipts and give a copy to the client at the end of their interaction. Research has proven that clients enjoy and benefit from receiving these receipts [6]. Adding a receipt book to the front panel of the device would make it more efficient by allowing the CHW to simultaneously enter the device data and fill out the paper receipt. The two activities can be synchronized by aligning the data readouts with corresponding blank fields on the receipts. Adding a pen holder on the device would also be convenient. A notepad was not included in the first design because of unforeseen logistical challenges. Research into portable or attached printer options yields options that are too costly, bulky, or unreliable in these environments. Adding printers would also add maintenance requirements to the device. Even for inkless printers, the required specialized paper is costly and sparse in the target areas. Procuring, storing, and transporting such materials adds unnecessary responsibility for the CHWs. To transfer the data to the database, a small Bluetooth adapter can be used to transmit the entered data to the user’s smartphone. This is a low-cost, space-efficient, and relatively simple method of transferring the data to a device that can forward it to other locations. Bluetooth requires a one-time exchange of the connected device’s PINs before use. All that this feature requires of the CHW is to ensure that the application that is receiving the data is active. Although this method allows for the use of a separate device to collect the data, it does create a layer of complexity and add failure points when compared to the previous data collection systems. However, because this device uses a store and forward system, issues with connecting to the network during the consultations do not effect data collection. In the event Bluetooth fails, code in the microcontroller logs all entries to a memory card in the device that can be exported manually at a later time. 5) Ruggedization Constructing a rugged device requires an understanding of the frequency of use and misuse, as well as the climate-related conditions that the device will endure. A portable device requires design elements that minimize inevitable stress. Ensuring the device’s components are sealed inside casing is important to reduce damage, and exposure to dust, dirt, humidity, and water. Soft rubber corners offer impact protection to the device. These come at a fairly low cost and drastically increase the durability of the device. A hard plastic cover that flips open to reveal the data inputs (sliders, buttons, etc.) offers increased protection while the device is not in use. These components are the most likely failure modes for these devices. Thus, emphasis should be placed on keeping them safe. The cover should have a latch that keeps it closed so that it does not accidentally open during transportation. The cover could also be used as a writing surface. A hard case or sleeve to enclose the entire device is an option, but would be a nuisance to keep track of, and would pose a risk if the case were to be misplaced. 6) Gamification Adding elements that stimulate senses increases readability and usability while indirectly promoting the program with an engaging and high-tech experience. After familiarizing
themselves with the device, CHWs become more efficient by multitasking with their senses, possibly using some for data entry and some for conversing with the client. When passersby see the unique device in use, they may be interested or inquire, and potentially become clients. Fun elements help to convey messages across any language, and are therefore applicable to any location. The disadvantage of these elements is that they draw power. Lights complement the data being displayed so that all components act as one cohesive entity. For example, when a user slides the height input upward, the lights running parallel to it will follow the slider up while the digital readout of the numbers appear at the top of the device. Lights also provide an low-cost, attractive, and seemingly sophisticated means to indirectly advertise to potential clients. An audio speaker will engage the user’s sense of hearing. The device will emit an audible signal to indicate that the user switching the device on or off,. It can also provide the user with audio feedback upon data entry. Small digital speakers are inexpensive and easy to install. Descriptive images provide universal readability of data inputs. For example, the slider for height could display a tall person at the top of the scale and a short person at the bottom. This small element makes it easy for anyone viewing the process to see what data is being entered. The images also make it faster for the CHW to locate the correct input. Descriptive images will not be used on the prototype due to space limitations. 7) Two Additional Designs The team has prioritized the development of the above device, but has conceptualized two additional devices with slightly different layouts. The user interface of the first additional design will be similar in size to the design above, but instead of utilizing sliders, it will use large dials. These dials offer a different approach, but a similar concept to that of the sliders. A notepad attachment and pen holder will also be added to this device. The other design is significantly smaller in size than the other two, using a small, calculator-like keypad for data entry. The keypad will be an effective data input method because the CHWs are already familiar with this platform. An optional armband attachment will be fixed to the backside. This device will also utilize solar power instead of conventional batteries. VI. DEPLOYMENT & EVALUATION The deployment and evaluation of the devices requires the utilization of the knowledge gained from previous attempts at data collection. The goal is to better understand technology implementation and provide hard evidence toward attributes that work in these low-resource environments. A. Observations During two weeks of fieldwork in Nyeri, Kenya in May 2014, the team was able to test the device with CHWs working with the Mashavu venture. Team members accompanied the Mashavu CHWs during their work days, observing their interactions with customers in order to determine how to best integrate data collection into their workflow. Multiple
customer interactions were often happening simultaneously, adding an additional challenge to individual record collection. Some customers paid to only receive some of the services provided by the Mashavu workers, making many records incomplete. The team modified the device to be able to accept incomplete records and is considering splitting the device into different functions, one for height and weight, and one for blood pressure. During testing, team members showed the device to customers to get their opinions on it. The customers were very interested, but did have some trouble using the device themselves. It was concluded that this was because they have minimal experience using computers. During this time, several errors were found in how the data was transferred to the cell phone via Bluetooth, but were quickly rectified. One Mashavu worker quickly learned how to use the various inputs and was able to enter data while working with customers after several interactions with the device. Soon, the CHW was commenting on how easy it was to enter and read data. The Mashavu workers will be trained how to use of the device and will be able to explain how it works to customers in their local language. B. Issues While conducting testing with CHWs, issues including ruggedness, sustainability, manufacturability, and usability were encountered. 1) Ruggedness Devices that are used in low-resource contexts must be able to withstand harsh environmental conditions not present in other areas including dust, rain, and vibration. To prevent dust from entering the device and causing the failure of moving parts, like the sliders, future iterations of the device will include a rubber coating around all externally exposed parts. This will also protect the internal components from moisture. However, during filed testing, it was discovered that the CHWs do not work when it is raining, alleviating some concerns about rain. The device was also modified to ensure the internal components do not move around, especially during transportation over bumpy roads. A cloth bag for the device was also procured to decrease the likelihood of dropping the device and make it more accessible to the CHWs while working. 2) Sustainability Economic and environmental sustainability are important to the success of this device. By selling the data to interested parties, the cost of the device will be offset and additional profits can be distributed to CHWs and future research. Disposal and maintenance of the device will be conducted at a local youth empowerment center’s electronics lab. Workers in this lab will be trained in the maintenance of the device and will recycle parts from broken devices. The proper disposal of batteries is an issue worldwide and is something that must be carefully considered in low-resource contexts. 3) Manufacturability Ideally, any data collection devices would be manufactured in the same areas where they would be used, reducing transportation costs. Preliminary results have not yielded any
local manufacturing locations, however the previously mentioned youth center is a possibility that will be explored further. 4) Usability After conducting testing with the CHWs, it was found that some of the input parameters needed to be slightly adjusted in order for the device to record accurate information. In its current prototype form, the device is quite bulky. Adding a large device to the set of things a CHW needs to use may prevent adoption of the device. This is one reason that a bag was obtained for the device. Future iterations will include efforts to slim-down the overall size of the device. Making the device wearable may also make it easier to carry. During preliminary testing, it was found that the battery life of the device was rather limited. Future designs must take power efficiency into account so the device can be used for an extended period of time. VII. CONCLUSION CHWs are a valuable resource that can be used to collect data in low resource contexts but to do so must be empowered with tools that facilitate this collection. Rather than attempt to shape an existing device, like a smartphone or tablet, to be used for this task, custom devices can be designed and will be more effective. These devices can incorporate gamification and Fun Theory mechanics to increase the motivation of those using the devices. A prototype health data collection device was positively received by CHWs working in rural Kenya. These CHWs also provided specific feedback about the device and how future iterations of the design can be better. By utilizing concepts from tangible computing, the amount of technical literacy needed to understand a device is lowered, an important aspect in low-resource contexts. The device and future prototypes will continue to be tested in both Kenya and Sierra Leone. The success of data collection devices like this will have many benefits for development organizations and will result in improved healthcare systems. VIII. REFERENCES [1] W. Baldwin, "Demographic Data For Development: Overview Report," Population Council, 2011. [2] Foreign Affairs, Trade, and Development Canada, "Open Data for Development Challenge," Foreign Affairs, Trade, and Development Canada, 15 January 2014. [Online]. Available: http://www.acdicida.gc.ca/acdi-cida/acdi-cida.nsf/eng/DEN1223131242-PCZ. [Accessed 10 April 2014]. [3] United States Agency for International Development, "Data & Analytics for Development," United States Agency for International Development, [Online]. Available: http://www.usaid.gov/what-we-do/sciencetechnolog-and-innovation/data-analytics-development. [Accessed 10 April 2014]. [4] France Telecom-Orange, "Data For Development Challenge," France Telecom-Orange, [Online]. Available: http://www.d4d.orange.com/home.
[Accessed 10 April 2014]. [5] J. Poole, "Winning Research from the Data for Development Challenge," United Nations Global Pulse, 6 May 2013. [Online]. Available: http://www.unglobalpulse.org/D4D-Winning-Research. [Accessed 10 April 2014]. [6] A. Shovlin, M. Ghen, P. Simpson and K. Mehta, "Challenges Facing Data Digitazation in Low-resource Contexts," in IEEE 2013 Global Humanitarian Technology Conference, San Jose, 2013. [7] S. M. Swider, "Outcome Effectiveness of Community Health Workers: An Integrative Literature Review," Public Health Nursing, vol. 19, no. 1, pp. 11-20, 2002. [8] World Health Organization, "World Health Statistics 2011," World Health Organization, Geneva, 2011. [9] W. Huang and S. Dilip, "A Practitioners Guide to Gamification of Education," Rotman School of Management, Toronto, 2013. [10] J. Simoes, "Four Approaches to Collecting Data in Gamified Systems," Gamifeye, 18 February 2013. [Online]. Available: http://www.gamifeye.com/2013/02/18/four-approachesto-collecting-data-in-gamified-systems/. [Accessed 9 May 2014]. [11] Nike, Inc., "Nike+ Fuelband SE," Nike, Inc., [Online]. Available: http://www.nike.com/us/en_us/c/nikeplusfuelband. [Accessed 7 May 2014]. [12] The Fun Theory, "The World's Deepest Bin," Volkswagen, 21 September 2009. [Online]. Available: http://www.thefuntheory.com/worlds-deepest-bin. [Accessed 27 April 2014]. [13] M. Billinghurst, K. Hirokazu and I. Poupyrev, "Collaboration with Tangible and Augmented Reality Interfaces," HCI International, vol. 1, pp. 5-10, 2001. [14] D. G. Caicedo, "What are Tangible User Interfaces?," 16 May 2010. [Online]. Available: http://www.bluehair.co/2010/05/what-are-tangible-userinterfaces-2/. [Accessed 20 Apil 2014]. [15] D. Shao, "A Proposal of Mobile Health Data Collection and Reporting System for the Developing World," Malmö University, 2012. [16] Z. A. Rajput, S. Mbugua and D. Amadi, "Evolution of an Android Based Telemedicine mHealth System for Population Survailence in eveloping Countires," Journal of the American Medical Informatics Association, vol. 19, no. 4, pp. 655-659, 2012. [17] A. Agrawal, J. Bhattacharya and N. Baranwal, "Integrating Halthcare Delivvery and Data Collection in Rural India using a Rapidly Deployable EHealth Center," PLoS Medicine, vol. 10, no. 6, 2013. [18] H. Fraser, "An Information System and Medical Record to Support HIV Treatment in Rural Haiti," BMJ, vol. 329, no. 7475, pp. 1142-1146, 2004.
[19] M. Tomlinson, W. Solomon and Y. Singh, "The Use of Mobile Phones as a Data Collection Tool: A Report from a Household Survey in Africa," BMC Medical Informatics and Decision Making, vol. 9, no. 51, 2009. [20] J. Rotich, "Installing and Implementing a Computerbased Patient Record System in Sub-Saharan Africa: The Mosoriot Meical Record System," Journal of the American Medical Informatics Association, vol. 10, no. 4, pp. 295-303, 2003. [21] Media Lab Asia, "Healthcare," Media Lab Asia, 6 April 2011. [Online]. Available: http://www.medialabasia.in/index.php/research/projects/ healthcare. [Accessed 20 April 2014]. [22] P. Susumpow, P. Patcharapom, S. Nathalie and A. Crawley, "Participatory Disease Detection through Digital Volunteerism: How the DoctorMe Application Aims to Capture Data for Faster Disease Detection in Thailand," in WWW Companion 14, Geneva, 2014. [23] R. Qin, R. Dzombak, R. Amin and K. Mehta, "Reliability of a Telemedicine System Designed for Rural Kenya," Journal of Primary Care and Community Health, vol. 4, no. 3, pp. 177-181, 2013. [24] S. Suffian, J. Lackey, R. Dzombak and K. Mehta, Telemedicine for Preventative Healthcare: Lessons from a Pilot Study in Rural Kenya, to be published. [25] P. Sundin, J. Callan and K. Mehta, "Why do Entrepreneurial mHealth Ventures in the Developing World Fail to Scale?," to be published. [26] F. Gemperle, C. Kasabach, J. Stivoric, M. Bauer and R. Martin, "Design For Wearability," in Wearable Computers, 1998. Digest of Papers. Second International Symposium on, Pittsburgh, 1998. [27] P. Maher, N. Smith and A. A. Williams, "Assesment of Pico Hydration as an Option for Off-grid Electrification in Kenya," Journal of Renewable Energy, vol. 28, no. 9, pp. 1357-1369, 2003. [28] B. Sanou, "The World in 2013: ICT Facts and Figures," International Telecommunications Union, Geneva, 2013.