Environment International 77 (2015) 42–47
Contents lists available at ScienceDirect
Environment International journal homepage: www.elsevier.com/locate/envint
Male fertility following occupational exposure to dichlorodiphenyltrichloroethane (DDT) Marcello Campagna, Giannina Satta, Domenica Fadda, Sergio Pili, Pierluigi Cocco ⁎ Department of Public Health, Clinical and Molecular Medicine, Occupational Health Section, University of Cagliari, Asse Didattico E ss 554, km 4,500, 09042 Monserrato, Cagliari, Italy
a r t i c l e
i n f o
Article history: Received 20 August 2014 Received in revised form 8 January 2015 Accepted 18 January 2015 Available online 30 January 2015 Keywords: Male fertility Time to pregnancy DDT Occupational exposure
a b s t r a c t Background: The inconsistent epidemiological results of the endocrine disrupting effects of DDT fuel a harsh debate on its global ban. Objectives: We tested the hypothesis that occupational exposure to dichloro-diphenyl-trichloroethane (DDT) causes impairment in male fertility in a cohort of DDT exposed workers, in Sardinia, Italy. Methods: We accessed official records on date of marriage and date of birth of the first child to estimate time to pregnancy (TTP) in the spouses of 1223 workers employed in a 1946–1950 anti-malarial campaign. The TTP calculation was censored at the 13th month after date of marriage. We used a modified Cox's proportional hazard model to calculate the fecundability ratio (FR) by job, by cumulative exposure to DDT, and by time window in relation to the anti-malarial operations, adjusting by paternal age at marriage. Results: Among the spouses of DDT applicators, fecundability did not vary during DDT use (FR = 1.22, 95% CI 0.84–1.77) nor in the following decade (FR = 1.01, 95% CI 0.67–1.50) with reference to the prior years. A significant increase occurred among the unexposed and the less exposed sub-cohorts, which generated a nonsignificantly reduced FR among the DDT applicator sub-cohort with reference to the unexposed following exposure. Conclusion: We did not find evidence of an impairment in male fertility following heavy occupational exposure to DDT. However, although fecundability was highest among the spouses of the DDT applicators in the years prior to the anti-malarial campaign, we cannot exclude that DDT exposure prevented an increase parallel to that observed among the unexposed and the less exposed sub-cohorts. © 2015 Elsevier Ltd. All rights reserved.
1. Introduction In 2001, the World Health Organization (WHO) Stockholm convention on persistent organic pollutants (POPs) made an exception to the worldwide ban for dichloro-diphenyl-trichloroethane (DDT) production and use “…in accordance with the WHO recommendations and guidelines on the use of DDT and when locally safe, effective and affordable alternatives are not available… [that] … pose less risk to human health and the environment …” (UNEP, 2002). Ten years after, WHO was still supporting the use of DDT in indoor residual spraying for countries where malaria is endemic (WHO, 2011). Its low cost, the long persistence of DDT in the environment, and its continuing effectiveness against malaria vectors keep it in the list of valuable insecticidal resources to fight malaria (van den Berg, 2009). The WHO Stockholm convention report lists the endocrine disruption potential of DDT among its adverse health outcomes. Endocrine disruptive effects were extensively studied in wildlife (Vos et al., 2000) ⁎ Corresponding author. E-mail addresses:
[email protected] (M. Campagna),
[email protected] (G. Satta),
[email protected] (D. Fadda),
[email protected] (S. Pili),
[email protected] (P. Cocco).
http://dx.doi.org/10.1016/j.envint.2015.01.010 0160-4120/© 2015 Elsevier Ltd. All rights reserved.
and in humans (Martenies and Perry, 2013). As it concerns human studies, several reports described a decrease in sperm count in relation to DDE body burden (Ayotte et al., 2001; Dalvie et al., 2004a; De Jager et al., 2006; Martenies and Perry, 2013). On the other hand, exposure in utero to the anti-androgen DDT derivative para,para′-DDE (p,p′-DDE) was not related to reduced androgen action in vivo, as reflected by anogenital distance or penile dimensions at birth (Longnecker et al., 2007); duration of lactation was not shortened (Cupul-Uicab et al., 2008); and evidence of a correlation between hormone function and DDT derivatives body burden was inconsistent (Ayotte et al., 2001; Martin et al., 2002; Cocco et al., 2004). Previous studies, including one by our group, did not provide convincing evidence of an impairment in male fertility following occupational and environmental exposure to DDT and its derivatives (Cocco et al., 2005b; Axmon et al., 2006; Harley et al., 2008). Nonetheless, the positive reports on male reproductive effects have captured greater attention (Eskenazi et al., 2009; Bouwman et al., 2013) in forensic trials and by environmental agencies. Currently, the global use of DDT for vector control around the world ranges 4–5000 metric tons per year, and several countries are reintroducing its production and use (van den Berg, 2009). Besides, computer models of how diseases spread, compared with what is known about global warming, predict a northward spreading of malaria
M. Campagna et al. / Environment International 77 (2015) 42–47
(Parham and Michael, 2010). Therefore, due to a foreseeable rehearsal and spreading of malaria, Public Health Agencies, Environmental Agencies, and policy makers worldwide need further reliable information on DDT health effects before taking balanced and responsible decisions about the most effective and safe strategy to fight malaria. To further test the hypothesis of adverse effects of DDT on male fertility, we extended our previous study to comprise a larger proportion of participants to one of the first attempts to eradicate malaria with extensive use of DDT, which was conducted in the Italian island of Sardinia in 1946–50. 2. Methods 2.1. Study setting Details on the anti-malarial campaign, conducted in Sardinia from 1 November 1946 to 31 May 1950 within the post-war reconstruction plan known as “Marshall plan”, with support from the Rockefeller Foundation, the United Nations, and the Italian Government, can be found elsewhere (Logan, 1953; Cocco et al., 2005a). Briefly, a pest control agency named Ente Regionale per la Lotta Anti-Anofelica in Sardegna (Regional Agency for the anti-anopheles fight in Sardinia, ERLAAS) was specifically created to conduct the anti-malarial operations. In 43 months, ERLAAS sprayed 267 metric tons of DDT over the whole Sardinian territory (Logan, 1953), corresponding to 10.6 mg/m2 or about 190 g per resident. Apart from a limited use of chlordane for residual and anti-larval purposes in selected areas, DDT was the only chemical used in the anti-malarial operations, thus creating a quasiexperimental setting. 2.2. Study population and exposure assessment Among the cohort of 4552 ERLAAS employees, we identified 1462 men who were born, had been lifetime resident in Sardinia, and got married by 31 December 1979. After excluding 153 subjects, for whom ERLAAS registers did not include information about the job title, 40 subjects we were unable to trace, and 46 subjects whose first child was born less than nine months after the date of marriage, we divided the remaining 1223 study subjects by job into three sub-cohorts: DDT applicators (N = 466), who prepared and applied daily the pesticide solution in diesel fuel; bystanders, including mainly warehouse workers and drivers, whose occupational exposure to DDT was mainly indirect, and inspectors, whose exposure was mainly by contact when re-entering the area after treatment to verify that the application had been conducted properly (N = 399); and occupationally unexposed (N = 358), including mainly laboratory, and administrative and managerial staff. This last sub-cohort had only background exposure at the general population level; we will define it as unexposed throughout the paper. When the same subject had held multiple jobs in different periods within the anti-malarial campaign, we retained the job involving the highest exposure. Cumulative DDT exposure during the antimalarial operations was estimated retrospectively for each individual, based on the exact dates of starting and ceasing each job, the task performed, and the concentration of DDT in the insecticide preparation, based on published information (Logan, 1953), as previously described (Cocco et al., 2005a). Based on these estimates, cumulative exposure to DDT in our study population ranged 8.6 mg–32.4 g (median 4.06 g) among applicators, and 0.1 mg–3.1 g (median 17.6 mg) among bystanders and inspectors. Over the whole study population the bounds defining tertiles of the distribution of cumulative DDT exposure were 33.1 mg, and 2.104 g. 2.3. Study outcomes We followed up fecundability among the spouses of cohort members. We expressed fecundability as time to pregnancy (TTP), i.e. the
43
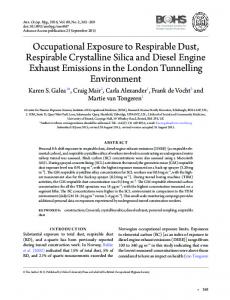
time in months required by each couple to achieve the first successful pregnancy. We calculated the time lag between the date of marriage and the ninth month before the birth date of the first child, assuming it as a reasonable estimate of TTP in a traditionally observant Catholic population. We excluded couples whose first child was born less than nine months after the date of marriage, and we considered date of marriage in the remaining couples as a reasonable surrogate for date of starting unprotected intercourses. We censored follow-up and TTP calculation at the 13th month, based upon the WHO definition of infertility (http://www.who.int/reproductivehealth/topics/infertility/definitions/ en/, accessed 30 June 2014). Date of marriage and date of birth of the first child were available at the Population Registrar of the communes of residence. We estimated the effect of the husband's exposure to DDT on his spouse fecundability for dates of marriage occurring within four time windows, defined in relation to the dates of the anti-malarial operations (before 1 November 1946; between 1 November 1946 and 31 May 1950; between 1 June 1950 and 31 December 1960; from 1 January 1961 to 31 December 1979), within each job sub-cohort with reference to the years prior to the use of DDT. We also compared fecundability among the spouses of the DDT exposed sub-cohorts and among the categories of cumulative DDT exposure with reference to the unexposed sub-cohort, within each of the above mentioned time windows. 2.4. Statistical methods As the measure of effect, we calculated the fecundability ratio (FR) and the respective 95% confidence interval (CI) associated with the husband's job, or with the husband's cumulative exposure to DDT by time windows within each sub-cohort with reference to the years prior the beginning of the anti-malarial operations, and by job or by tertiles of cumulative exposure to DDT within each time window with reference to the unexposed sub-cohort, using a modified Cox's proportional hazard model for discrete time-censored data, with SPSS®. We adjusted the FRs by paternal age at marriage. A FR lower than unity would imply a reduced fecundability associated with an impaired male fertility resulting from DDT exposure. We used the likelihood ratio test (Breslow and Day, 1980) to assess the interaction between DDT exposure, as related to the job or to the estimated cumulative exposure, and the period of marriage, whether during the antimalarial operations, or in the following decade, or afterwards, with reference to the years prior to their onset. 2.5. Ethical issues The use of official records was made according to the prescription of the Italian Authority for the Protection of personal data N. 85 of March 1, 2012, published on the Gazzetta Ufficiale della Repubblica N. 72 of March 26, 2012, authorizing the treatment of personal data for scientific research purposes. The authors performed the research in accordance with the principles of the Declaration of Helsinki. 3. Results Table 1 summarizes the size of the sub-cohorts and the total cohort. About 25% of study subjects got married during the anti-malarial campaign, and 58.2% afterwards. DDT applicators prevailed in our study population, accounting for 38.1% of the total study subjects, with bystanders and inspectors representing 32.6%, and the unexposed subcohort 29.2%. Over the whole study population, infertility rate, i.e. the proportion of subjects who did not conceive within 12 months after marriage or never conceived over the total who got married within the same time period, did not vary with time, showing a tendency towards improvement, if anything. Table 2 and Fig. 1 show the FR and the respective fecundability curves for each sub-cohort by time window with reference to the
44
M. Campagna et al. / Environment International 77 (2015) 42–47
Table 1 Study sub-cohorts of participants to the 1946–50 anti-malarial campaign in Sardinia, Italy by year of marriage and reproductive outcome. Date of marriage
N (%)
b01/11/1946 01/11/1946–31/10/1950 01/11/1950–31/12/1960 01/01/1961–31/12/1979 Total
233 (19.1) 278 (22.7) 528 (43.2) 184 (15.0) 1223 (100.0)
a b
Age at marriage
Successful conceptiona
Mean
sd
Yes ≤12 months
Yes N12 months
Never conceived
24.3 27.9 32.4 41.3 31.0
2.81 3.23 4.21 5.96 6.80
126 (54.1) 170 (61.1) 330 (62.5) 102 (55.4) 728 (59.5)
93 (39.9) 84 (30.2) 144 (27.3) 37 (20.1) 358 (29.3)
14 (6.0) 24 (8.6) 54 (10.2) 45 (24.5) 137 (11.2)
Infertility rate (se)
χ2 (p value)b
0.46 (0.04) 0.39 (0.04) 0.37 (0.03) 0.45 (0.05) 0.40 (0.02)
Reference 1.51 (0.22) 2.86 (0.09) 0.04 (0.84)
Percent rates are calculated over the total in the correspondent row. With reference to the time period before initiating DDT exposure in the anti-malarial operations (before 01/11/1946).
years prior to the onset of the anti-malarial campaign. Due to the long persistence of DDT in the adipose tissue (Baird and Cann, 2008), when occupational exposure had ceased, DDT body burden had presumably reached its highest level. When considering marriages occurring in the first years following the end of the anti-malarial operations, with reference to the years prior to the beginning of the operations, the FR among DDT applicators was 1.01 (95% CI 0.67–1.50), and it was 1.62 (95% CI 1.06–2.50) among bystanders and inspectors, and 2.19 (95% CI 1.30–3.69) among the unexposed sub-cohort. Within the same time window, heterogeneity across sub-cohorts was of borderline significance (Q = 5.84, degrees of freedom = 2, p = 0.054). We did not detect heterogeneity by sub-cohort for marriages in 1946–1950, during the operations, or in 1961–79, more than 10 years after the end of the anti-malarial operations. Our results indicate that, while among the spouses of DDT applicators fecundability did not vary with time in relation to the husband's occupational exposure to DDT, a significant increase in fecundability was observed among the spouses of bystanders and inspectors, and more clearly so among the spouses of the unexposed, during the anti-malarial campaign and in the following decade. Table 3 and Fig. 2 show the FR and the respective fecundability curves by job and by tertiles of cumulative exposure to DDT with reference to the unexposed sub-cohort within each of the four time windows, as previously defined. Before the onset of the anti-malarial campaign, spouses of DDT applicators, who had been the most severely exposed to DDT, and spouses of bystanders and inspectors had a higher FR compared to the unexposed sub-cohort (respectively 1.49, 95% CI 0.89 to 2.48; and 1.64, 95% CI 1.00 to 2.69). Immediately after the end of the anti-malarial operations, as an effect of the increasing fecundability among the spouses of the unexposed sub-cohort, the FR was reversed among the spouses of DDT applicators (FR = 0.82, 95% CI 0.63 to 1.07), and in the medium tertile of cumulative exposure to DDT (FR = 0.81, 95% CI 0.61 to 1.10), and, although less pronounced, in the upper tertile. We did not detect heterogeneity in the FR across study sub-cohorts within any of the time windows, including the decade following the anti-malarial campaign (by job: Q = 5.11, degrees of freedom = 3, p = 0.16; by cumulative exposure to DDT: Q = 1.54, degrees of freedom = 2, p = 0.46). The likelihood ratio test did not suggest an interaction between exposure to DDT, as defined by job or by the estimated cumulative exposure, and period of marriage (p = 0.394, and p = 0.433, respectively). Results did not change when using the median or the tertile of cumulative exposure as cut points between categories,
Table 2 Fecundability ratio by time windows in relation to the 1946–1950 anti-malarial campaign in Sardinia, Italy, by job title. Time period
Unexposed N
FR
≤1946 52 1.0 1947–1950 71 1.95 1951–1960 173 2.19 1961–1979 61 2.04
95% CI
Bystanders and inspectors
DDT applicators
N
N
FR
– 96 1.0 1.15–3.30 82 1.26 1.30–3.69 172 1.62 0.95–4.40 48 1.85
95% CI
FR
95% CI
– 83 1.0 – 0.84–1.90 124 1.22 0.84–1.77 1.06–2.50 183 1.01 0.67–1.50 0.84–4.05 74 0.91 0.49–1.71
or when using the central year for each time window, or when considering non-categorical covariates. 4. Discussion TTP is considered the endpoint of multiple biological processes in male and female partners, and it represents a useful tool to investigate the effects of occupational and environmental exposures on human fertility (Bonde et al., 2006). In our study, we did not find evidence of a reduction in fecundability, corresponding to a prolonged TTP, in relation to paternal occupational exposure to DDT. The modest inverse FR observed in the decade immediately following the end of the antimalarial campaign among the spouses of DDT applicators, and of subjects in the middle and upper tertile of cumulative DDT exposure, with reference to the unexposed, was due to a significant increase in fecundability among the latter in the post-war years. However, such reduction was not observed among the less exposed bystanders and inspectors sub-cohort. It is not possible to infer from our data whether DDT exposure was responsible for the lack of a parallel increase in fecundability among the spouses of DDT applicators beyond the levels achieved prior to the onset of the anti-malarial operations. To retrieve previous publications on the same subject, we conducted a systematic search on PubMed and Scopus® using the keywords “dichlorodiphenyltrichloroethane”, “time to pregnancy”, “fecundability” and “fertility”. We identified five papers published in 2003–14 addressing the specific hypothesis of an association between DDT body burden, or documented occupational or environmental DDT exposure, and a prolonged TTP. Only one, our previous report, was based on occupational data for the male partner (Cocco et al., 2005b); in that study, the FR among the spouses of DDT applicators was 0.72 (95% CI, 0.41 to 1.21) with reference to the unexposed. Another study tested fecundability odds ratios (FOR) in relation to lipid-adjusted p,p′-DDE serum level in the male partners in three areas, Greenland, Poland, and Ukraine; results from pre-delivery maternal samples were also reported for Sweden (Axmon et al., 2006). We used a meta-analysis approach to combine the results from these areas; among men, the fixed summary estimate of the unadjusted FOR was 0.99 (95% CI 0.78 to 1.26) for p,p′DDE level ranging 740–1200 ng/g and 0.96 (95% CI 0.74 to 1.24) for p, p′-DDE level above 1200 ng/g, with reference to men with p,p′-DDE level below 740 ng/g. Among pregnant women, the fixed summary estimate was 1.02 (95% CI 0.87 to 1.20) for p,p′-DDE level ranging 370– 750 ng/g and 0.89 (95% CI 0.74 to 1.07) for p,p′-DDE level above 750 ng/g, with reference to women with p,p′-DDE level below 370 ng/g. Random estimates were always identical to the corresponding fixed summary estimates. The individual studies presented in the Axmon et al. paper used different adjusting covariates, including paternal and maternal age, frequency of sexual intercourses and others, which made the adjusted FORs not immediately comparable. However, the adjustments did not substantially change the risk estimates, and the overall interpretation of lack of an association. Two other studies investigated TTP in relation to prior lipid-adjusted p,p′-DDE serum levels in pregnant women (Gesink Law et al., 2005; Harley et al., 2008), using Cox proportional hazard modeling. In the Gesink Law et al. study population, the median lipidadjusted p,p′-DDE serum level was about 2.0 μg/g, and the FR for levels
M. Campagna et al. / Environment International 77 (2015) 42–47
Unexposed
45
Bystanders and inspectors
DDT applicators
Fig. 1. Fecundability curves in the unexposed, bystanders and inspectors, and DDT applicators by time windows in relation to the anti-malarial campaign.
above the median was 1.03 (95% CI 0.91 to 1.16) with reference to below the median (Gesink Law et al., 2005). In the Harley et al. study population, the geometric mean of lipid-adjusted p,p′-DDE serum level was 1.5 μg/g, and the FR (FR = 0.91, 95% CI 0.68 to 1.22) was expressed in relation to log10 of lipid adjusted p,p′-DDE serum level as a continuous variable (Harley et al., 2008), which would not permit combination of their results with the aggregated results obtained using categorical exposure variables by Gesink Law et al. One additional study explored fecundability in the eldest daughter in relation to maternal DDE serum level at delivery between the late fifties and early sixties (Cohn et al., 2003): the FR was significantly, although modestly, elevated (FR = 1.16, 95% CI, 1.06 to 1.26) with reference to levels below 10 μg/L. Therefore, the few epidemiological reports published to date, consistent with our findings, do not support the hypothesis of a detrimental effect on human fertility, male or female, following occupational and environmental exposure to DDT. P,p′-DDE showed in-vitro anti-androgen properties by competing with natural androgens at the receptorial level and/or binding the serum hormone binding globulin (SHBG) (Kelce et al., 1995). Also, studies on infertile men in malaria endemic regions have reported lower sperm concentrations, chromatin defects, impaired motility and morphology alterations as a result of total DDT-DDE exposure (Ayotte et al., 2001; Dalvie et al., 2004a; De Jager et al., 2006; Weiss et al., 2006; Aneck-Hahn et al., 2007; Pant et al., 2007; Messaros et al., 2009). On the other hand, in vivo human studies of hormone levels in relation to environmental exposure to DDT or DDE body burden have yielded unconvincing findings (Ayotte et al., 2001; Martin et al., 2002;
Cocco et al., 2004; Dalvie et al., 2004b), further weakened by lack of consideration of plausible confounders, such as nutritional shortage, or malaria itself (Singer et al., 1987), and/or by being typically based on small size population samples. The apparent contradiction between epidemiological studies on human fertility and specific reproductive outcomes, such as semen quality, associated with occupational and environmental exposure to DDT, might reflect the limited value of morphological sperm characteristics and number as indicators of reproductive potential or outcome (Shamsi et al., 2011). Besides, due to the much lower receptor affinity in respect to the natural hormone, such effects in vivo might plausibly show up only at extremely high DDT serum levels, capable of resulting in a significant interference with a normal human androgenic or estrogenic function (Cocco, 2002). If such circumstances would occur, endocrine disruption might result. However, apart from receptor mediated mechanisms, like other endocrine disruptors, DDT can act through other mechanisms, such as activation of enzymatic pathways involved in biosynthesis and/or metabolism of steroid hormones. Also, the period of exposure to endocrine disruptors has been suggested as relevant, the most critical for possible health outcomes being the period of development (Bergman et al., 2013). The effects of simultaneous exposure to multiple endocrine disruptors are also poorly known. Further studies are warranted addressing these specific hypotheses as possible mechanisms for an impaired male fertility. Interpreting our findings requires caution and careful consideration of its limitations. The use of official marriage and birth records as surrogates for calculating TTP has been previously discussed (Cocco et al.,
Table 3 Fecundability ratio by job title and by cumulative exposure to DDT within four time windows among the participants in the 1946–1950 anti-malarial campaign in Sardinia, Italy. Time period
Unexposed
Bystanders
DDT applicators
Cumulative exposure to DDT (milligrams) 0.4–33.1
≤1946 1947–1950 1951–1960 1961–1979
≥2101.4
33.11–2101
N
FR
95% CI
N
FR
95% CI
N
FR
95% CI
N
FR
95% CI
N
FR
95% CI
N
FR
95% CI
52 71 173 61
1.0 1.0 1.0 1.0
– – – –
96 82 172 48
1.64 0.93 1.00 0.98
1.00–2.69 0.62–1.41 0.77–1.30 0.58–1.65
83 124 183 74
1.49 1.07 0.82 0.93
0.89–2.48 0.74–1.56 0.63–1.07 0.59–1.47
73 71 114 46
1.98 0.91 1.05 1.05
1.20–3.28 0.60–1.40 0.78–1.41 0.63–1.77
42 69 121 36
1.32 0.93 0.81 0.81
0.73–2.39 0.60–1.44 0.61–1.10 0.46–1.43
64 66 120 40
1.32 1.23 0.87 0.97
0.76–2.28 0.81–1.87 0.65–1.17 0.57–1.65
46
M. Campagna et al. / Environment International 77 (2015) 42–47
b. 1947 – 1950
c. 1951 – 1960
d. 1961 – 1979
e. 1947 – 1950
f. 1951 – 1960
g. 1961 – 1979
Fecundability rate
a. ≤ 1946
Time to pregnancy (months)
Fig. 2. Fecundability curves by time periods in relation to the 1946–1950 anti-malarial campaign, by job (a, b, c, d), and by tertiles of cumulative DDT exposure (e, f, g).
2005b). The decision of relying on official records to calculate TTP was due to the more than 60 year time lag between entering the cohort and conducting the present study, with most cohort members expected to have died or to be too old to afford a personal interview. In a traditionally observant Catholic setting, having excluded couples who had their first child less than nine months after the date of marriage, we considered date of marriage to be a reasonable approximation for the beginning of the couple's attempt to conceive. Information on maternal age at marriage was not available, which might have introduced bias in our analysis if differentially distributed across the sub-cohorts. We have no information about whether this was the case. We are aware that an unknown proportion of spontaneous abortions might have occurred, and that couples might have continued protected intercourses even after marriage, thus leading to a wrong calculation of TTP in these couples. Risk of spontaneous abortion was not elevated in relation to paternal occupational exposure to DDT (Salazar-García et al., 2004), while an association was reported with maternal DDE body burden (Longnecker et al., 2005). However, if DDT would have induced a higher frequency of spontaneous abortion in the exposed sub-cohort, we would have overestimated TTP in this cohort, which would reinforce our result of no impairment in male fertility following occupational exposure to DDT. As it concerns continuation of protected intercourses after marriage, this could have affected our findings if more frequently discontinued in the unexposed sub-cohort and in the bystander and inspector subcohort, during the anti-malarial operations and afterwards, in respect to the DDT applicator sub-cohort. However, we do not have information about continuation of protected intercourses after marriage differential by study sub-cohorts. We suspect that the substantial improvement in income and nutrition in the post-war reconstruction, unequally spread by socio-economic categories, might have contributed, coincidentally
accompanying the exposure to DDT during the anti-malarial campaign. On the other hand, an advantage of relying on official records is to avoid recall bias and selection bias from differential participation rate among study sub-cohorts, which typically affect retrospective studies based on questionnaire interviews. 5. Conclusion Nowadays, several cost-effective degradation strategies in contaminated soils could minimize DDT exposure and drift (Sudharshan et al., 2012). In the areas where DDT is used, personal and collective protective equipment and preventive procedures can be applied to reduce exposure for the workers and the population, with special precaution for children and adolescents. These and other preventive actions would reduce any hypothetical impact of DDT on the environment and human health. Still, DDT is a persistent organic pollutant and a reproductive threat for wild life and for humans at toxicologically adequate doses, and for this reason precautionary measures are justified. However, based on the current scientific evidence, the search of safe, effective and affordable alternatives to DDT shall consider the availability of information on the long term health effects as extensive and detailed as for DDT. Competing interests None of the co-authors declare support from any organization for the submitted work, nor financial relationships with any organization that might have an interest in the submitted work, nor other relationships or activities that could appear to have influenced the submitted work.
M. Campagna et al. / Environment International 77 (2015) 42–47
Acknowledgments This study was funded with a grant from the Italian National Institute for Prevention and Safety at Work (ISPESL), research projects 1998. The funding agency did not intervene at any step in the study design; in the collection, analysis and interpretation of data; in the writing of the manuscript; and in the decision to submit the article for publication. References Aneck-Hahn, N.H., Schulenburg, G.W., Bornman, M.S., Farias, P., de Jager, C., 2007. Impaired semen quality associated with environmental DDT exposure in young men living in a malaria area in the Limpopo Province, South Africa. J. Androl. 28, 423–434. http://dx.doi.org/10.2164/jandrol.106.001701. Axmon, A., Thulstrup, A.M., Rignell-Hydbom, A., Pedersen, H.S., Zvyezday, V., Ludwicki, J.K., et al., 2006. Time to pregnancy as a function of male and female serum concentrations of 2,2′4,4′5,5′-hexachlorobiphenyl (CB-153) and 1,1-dichloro-2,2-bis(pchlorophenyl)-ethylene (p,p′-DDE). Hum. Reprod. 21, 657–665. http://dx.doi.org/ 10.1093/humrep/dei397. Ayotte, P., Giroux, S., Dewailly, E., Hernández, Avila M., Farias, P., Danis, R., et al., 2001. DDT spraying for malaria control and reproductive function in Mexican men. Epidemiology 12, 366–367. Baird, C., Cann, M., 2008. Environmental Chemistry. 4th ed. W.H. Freeman and Company, New York, NY. Bergman, Å., Heindel, J.J., Kasten, T., Kidd, K.A., Jobling, S., Neira, M., et al., 2013. The impact of endocrine disruption: a consensus statement on the state of the science. Environ. Health Perspect. 121, a104–a106. http://dx.doi.org/10.1289/ehp.1205448. Bonde, J.P., Joffe, M., Sallmén, M., Kristensen, P., Olsen, J., Roeleveld, N., et al., 2006. Validity issues relating to time-to-pregnancy studies of fertility. Epidemiology 17, 347–349. http://dx.doi.org/10.1097/01.ede.0000210239.80406.46. Bouwman, H., Bornman, R., van den Berg, H., Kylin, H., 2013. DDT: fifty years since Silent Spring. Late Lessons From Early Warnings: Science, Precaution, Innovation. EEA Report 1/2013. European Environment Agency, Copenhagen, Denmark. Breslow, N.E., Day, N.E., 1980. Statistical methods in cancer research. The Design and Analysis of Case–Control Studies vol. I. International Agency for Research of Cancer, Lyon, France. Cocco, P., 2002. On the rumors about the silent spring. Review of the scientific evidence linking occupational and environmental pesticide exposure to endocrine disruption health effects. Cad. Saude Publica 18, 379–402. http://dx.doi.org/10.1590/S0102311X2002000200003. Cocco, P., Loviselli, A., Fadda, D., Ibba, A., Melis, M., Oppo, A., et al., 2004. Serum sex hormones in men occupationally exposed to dichloro-diphenyl-trichloro ethane (DDT) as young adults. J. Endocrinol. 182, 391–397. Cocco, P., Fadda, D., Billai, B., D'Atri, M., Melis, M., Blair, A., 2005a. Cancer mortality among men occupationally exposed to dichlorodiphenyltrichloroethane. Cancer Res. 65, 9588–9594. http://dx.doi.org/10.1158/0008-5472.CAN-05-1487. Cocco, P., Fadda, D., Ibba, A., Melis, M., Tocco, M.G., Atzeri, S., et al., 2005b. Reproductive outcomes in DDT applicators. Environ. Res. 98, 120–126. http://dx.doi.org/10.1016/ j.envres.2004.09.007. Cohn, B.A., Cirillo, P.M., Wolff, M.S., Schwingl, P.J., Cohen, R.D., Sholtz, R.I., et al., 2003. DDT and DDE exposure in mothers and time to pregnancy in daughters. Lancet 361, 2205–2206. http://dx.doi.org/10.1016/S0140-6736(03)13776-2. Cupul-Uicab, L.A., Gladen, B.C., Hernández-Avila, M., Weber, J.P., Longnecker, M.P., 2008. DDE, a degradation product of DDT, and duration of lactation in a highly exposed area of Mexico. Environ. Health Perspect. 116, 179–183. http://dx.doi.org/10.1289/ ehp.10550. Dalvie, M.A., Myers, J.E., Thompson, M.L., Robins, T.G., Dyer, S., Riebow, J., et al., 2004a. The long-term effects of DDT exposure on semen, fertility, and sexual function of malaria vector-control workers in Limpopo Province, South Africa. Environ. Res. 96, 1–8. Dalvie, M.A., Myers, J.E., Lou Thompson, M., Dyer, S., Robins, T.G., Omar, S., et al., 2004b. The hormonal effects of long-term DDT exposure on malaria vector-control workers in Limpopo Province, South Africa. Environ. Res. 96, 9–19. De Jager, C., Farias, P., Barraza-Villarreal, A., Avila, M.H., Ayotte, P., Dewailly, E., et al., 2006. Reduced seminal parameters associated with environmental DDT exposure and p,p′DDE concentrations in men in Chiapas, Mexico: a cross-sectional study. J. Androl. 27, 16–27. http://dx.doi.org/10.2164/jandrol.05121.
47
Eskenazi, B., Chevrier, J., Goldman Rosas, L., Anderson, H.A., Bornman, M.S., Bouwman, H., et al., 2009. The pine river statement: human health consequences of DDT use. Environ. Health Perspect. 117, 1359–1367. http://dx.doi.org/10.1289/ehp.11748. Gesink Law, D.C., Klebanoff, M.A., Brock, J.W., Dunson, D.B., Longnecker, M.P., 2005. Maternal serum levels of polychlorinated biphenyls and 1,1-dichloro-2,2-bis(pchlorophenyl) ethylene (DDE) and time to pregnancy. Am. J. Epidemiol. 162, 523–532. http://dx.doi.org/10.1093/aje/kwi240. Harley, K.G., Marks, A.R., Bradman, A., Barr, D.B., Eskenazi, B., 2008. DDT exposure, work in agriculture, and time to pregnancy among farm workers in California. J. Occup. Environ. Med. 50, 1335–1342. http://dx.doi.org/10.1097/JOM.0b013e31818f684d. Kelce, W.R., Stone, C.R., Laws, S.C., Gray, L.E., Kemppainen, J.A., Wilson, E.M., 1995. Persistent DDT metabolite p,p′-DDE is a potent androgen receptor antagonist. Nature 375, 581–585. http://dx.doi.org/10.1038/375581a0. Logan, J.A., 1953. The Sardinian Project: An Experiment in the Eradication of an Indigenous Malarious Vector. Johns Hopkins Press, Baltimore, Maryland. Longnecker, M.P., Klebanoff, M.A., Dunson, D.B., Guo, X., Chen, Z., Zhou, H., et al., 2005. Maternal serum level of the DDT metabolite DDE in relation to fetal loss in previous pregnancies. Environ. Res. 97, 127–133. http://dx.doi.org/10.1016/S00139351(03)00108-7. Longnecker, M.P., Gladen, B.C., Cupul-Uicab, L.A., Romano-Riquer, S.P., Weber, J.P., Chapin, R.E., et al., 2007. In utero exposure to the antiandrogen 1,1-dichloro-2,2-bis(pchlorophenyl)ethylene (DDE) in relation to anogenital distance in male newborns from Chiapas, México. Am. J. Epidemiol. 165, 1015–1022. http://dx.doi.org/10.1093/ aje/kwk109. Martenies, S.E., Perry, M.J., 2013. Environmental and occupational pesticide exposure and human sperm parameters: a systematic review. Toxicology 307, 66–73. http://dx.doi. org/10.1016/j.tox.2013.02.005. Martin Jr., S.A., Harlow, S.D., Sowers, M.F., Longnecker, M.P., Garabrant, D., Shore, D.L., et al., 2002. DDT metabolite and androgens in African-American farmers. Epidemiology 13, 454–458. Messaros, B.M., Rossano, M.G., Liu, G., Diamond, M.P., Friderici, K., Nummy-Jernigan, K., et al., 2009. Negative effects of serum p,p′-DDE on sperm parameters and modification by genetic polymorphisms. Environ. Res. 109, 457–464. http://dx.doi.org/10.1016/j. envres.2009.02.009. Pant, N., Kumar, R., Mathur, N., Srivastava, S.P., Saxena, D.K., Gujrati, V.R., 2007. Chlorinated pesticide concentration in semen of fertile and infertile men and correlation with sperm quality. Environ. Toxicol. Pharmacol. 23, 135–139. http://dx.doi.org/10.1016/j. etap.2006.07.012. Parham, P.E., Michael, E., 2010. Modeling the effects of weather and climate change on malaria transmission. Environ. Health Perspect. 118, 620–626. http://dx.doi.org/10. 1289/ehp.0901256. Salazar-García, F., Gallardo-Díaz, E., Cerón-Mireles, P., Loomis, D., Borja-Aburto, V.H., 2004. Reproductive effects of occupational DDT exposure among male malaria control workers. Environ. Health Perspect. 112, 542–547. http://dx.doi.org/10.1289/ehp. 6759. Shamsi, M.B., Imam, S.N., Dada, R., 2011. Sperm integrity DNA assays: diagnostic and prognostic challenges and implications in management of fertility. J. Assist. Reprod. Genet. 28, 1073–1085. http://dx.doi.org/10.1007/s10815-011-9631-8. Singer, R., Segenreich, E., Sagiv, M., Shohat, B., Livni, E., Bartoov, B., et al., 1987. Decreased semen quality in a male infected with malaria. Int. J. Androl. 10, 685–689. Sudharshan, S., Naidu, R., Mallavarapu, M., Bolan, N., 2012. DDT remediation in contaminated soils: a review of recent studies. Biodegradation 23, 851–863. http://dx.doi.org/ 10.1007/s10532-012-9575-4. United Nations Environment Programme, 2002. Stockholm convention on persistent pollutants (POPs). UNEP/Chemicals/2002/9. United Nations Environment Programme, Geneva, Switzerland. van den Berg, H., 2009. Global status of DDT and its alternatives for use in vector control to prevent disease. Environ. Health Perspect. 117, 1656–1663. http://dx.doi.org/10. 1289/ehp.0900785. Vos, J.G., Dybing, E., Greim, H.A., Ladefoged, O., Lambré, C., Tarazona, J.V., et al., 2000. Health effects of endocrine-disrupting chemicals on wildlife, with special reference to the European situation. Crit. Rev. Toxicol. 30, 71–133. Weiss, J.M., Bauer, O., Bluthgen, A., Ludwig, A.K., Vollersen, E., Kaisi, M., et al., 2006. Distribution of persistent organochlorine contaminants in infertile patients from Tanzania and Germany. J. Assist. Reprod. Genet. 23, 393–399. http://dx.doi.org/10.1007/ s10815-006-9069-6. World Health Organization, 2011. The Use of DDT in Malaria Vector Control. WHO Position Statement. World Health Organization, Geneva, Switzerland.