Randomized controlled trial of the effect of daily supplementation with zinc or multiple micronutrients on the morbidity, growth, and micronutrient status of young Peruvian children1–3 Mary E Penny, R Margot Marin, Augusto Duran, Janet M Peerson, Claudio F Lanata, Bo Lönnerdal, Robert E Black, and Kenneth H Brown ABSTRACT Background: Zinc supplements reduce childhood morbidity in populations in whom zinc deficiency is common. In such populations, deficiencies in other micronutrients may also occur. Objective: The objective was to determine whether the administration of other micronutrients with zinc modifies the effect of zinc supplementation on children’s morbidity and physical growth. Design: Two hundred forty-six children aged 6 –35 mo with persistent diarrhea were randomly assigned to 1 of 3 groups to receive a daily supplement of 10 mg Zn alone (Zn; n ҃ 81), zinc plus vitamins and other minerals at 1–2 times recommended daily intakes (ZnѿVM; n ҃ 82), or placebo (n ҃ 83) for 앒6 mo after the diarrhea episode ended. Morbidity information was collected on weekdays. Weight, length, and other anthropometric indicators were measured monthly, and plasma zinc and other indicators of micronutrient status were measured at baseline and 6 mo. Results: Supplement consumption was high (앒90%) in all groups, although slightly more vomiting was reported in the ZnѿVM group (P 쏝 0.0001, analysis of variance). The change in plasma zinc from baseline to 6 mo was greater in the 2 zinc groups (6.1, 27.3, and 16.2 g/dL in the placebo, Zn, and ZnѿVM groups, respectively; P 쏝 0.0001, analysis of variance). The Zn group had fewer episodes of diarrhea, dysentery, and respiratory illness and a lower prevalence of fever and cough than did the ZnѿVM group and a lower prevalence of cough than did the placebo group (P ҃ 0.05). No significant effects of supplementation on growth were observed. Conclusion: Morbidity was greater after supplementation with zinc plus multivitamins and minerals than it was after supplementation with zinc alone. Am J Clin Nutr 2004;79:457– 65. KEY WORDS Zinc supplementation, zinc deficiency, diarrhea, respiratory infection, growth
INTRODUCTION
Zinc is an essential nutrient that, because of its fundamental role in many aspects of cellular metabolism (1), is critical for normal immune function (2) and physical growth (3). Zinc deficiency appears to be widespread in low-income countries because of a low dietary intake of zinc-rich animal-source foods and a high consumption of cereal grains and legumes, which contain inhibitors of zinc absorption (4, 5). Children in poor countries are also frequently affected by diarrhea, which causes
excess fecal losses of zinc (6). In such settings, zinc supplementation has been shown to reduce the rates of diarrhea and pneumonia (7) and to enhance the physical growth of young children at risk of stunting (3). Inadequate zinc nutriture may be associated with deficiencies of other micronutrients, and these coexisting nutritional problems could reduce the potential benefit of zinc supplementation on morbidity or growth (8, 9). On the other hand, it is possible that simultaneous administration of multiple other micronutrients could interfere with zinc absorption or utilization. For example, adverse interactions between iron and zinc supplements have been described (10 –12). Thus, it is important to determine whether supplementation with multiple micronutrients would be as effective as with zinc alone. There are several reasons to suspect that poor children in periurban Lima may be zinc deficient, including their frequent consumption of diets that have inadequate zinc contents (13), a high prevalence of diarrhea (14), and low plasma zinc concentrations (13, 15). The current study was therefore designed to evaluate whether daily zinc supplementation for 6 mo in children who had recovered from a recent episode of persistent diarrhea would reduce the incidence and prevalence of subsequent episodes of diarrhea and respiratory illness. Children with a prior episode of persistent diarrhea were selected for study because we anticipated that they would have an elevated risk of zinc deficiency and therefore would likely respond to zinc supplementation. To determine whether additional micronutrients would enhance or diminish the effects of zinc alone, we studied a third group of children who received zinc in combination with multiple other micronutrients. 1 From the Instituto de Investigacio´n Nutricional, Lima, Peru´ (MEP, RMM, AD, and CFL); the Program in International Nutrition and Department of Nutrition, University of California, Davis (JMP, BL, and KHB); and the Department of International Health, The Johns Hopkins Bloomberg School of Public Health, Baltimore (REB). 2 Supported primarily by the Thrasher Research Fund and the World Health Organization; additional funds were provided by the University of California Pacific Rim Program. 3 Address reprint requests to ME Penny, Instituto de Investigacio´n Nutricional, Avenue La Universidad 685–La Molina, Apartado 18-0191, Lima 18, Peru´. E-mail:
[email protected]. Received March 3, 2003. Accepted for publication August 25, 2003.
Am J Clin Nutr 2004;79:457– 65. Printed in USA. © 2004 American Society for Clinical Nutrition
457
458
PENNY ET AL
SUBJECTS AND METHODS
TABLE 1 Composition of the supplement during phase 2 of the study1
Study design, site, and population This randomized, double-masked, placebo-controlled, community-based trial was carried out in Canto Grande, a shanty town on the outskirts of Lima, Peru. Characteristics of the study community were described previously (13, 16). The study was carried out in 2 phases. During the first phase we evaluated the effect of zinc or multiple micronutrient supplementation on the recovery from persistent diarrhea. During the second phase we assessed the effect of continued supplementation on morbidity from new infections during the following 6 mo. The results of the first phase of the study were published previously (16). Briefly, 412 children aged 6 –36 mo with diarrhea for 욷 14 d were randomly assigned, after being stratified for breastfeeding status, to receive 2 wk of daily supplementation with 1 of 3 indistinguishable supplements: placebo, 20 mg Zn/d as zinc gluconate (Zn group), or 20 mg Zn/d as zinc gluconate plus a mixture of other micronutrients, ie, vitamins and minerals (ZnѿVM group). A subset of children consisting of the first 246 children enrolled who intended to remain in the study area subsequently received the same assigned supplement at one-half the initial daily dose (10 mg Zn/d) and continued under observation for a total of 6 mo. The study protocol was approved by the institutional review boards of the Instituto de Investigacio´ n Nutricional and the University of California, Davis. Children were enrolled in the study only after a parent provided written informed consent. Micronutrient supplements The supplements were supplied as individual doses of a dry micronutrient mixture with added sugar, coloring, and flavoring agents, which were dissolved in clean water in the subjects’ homes and provided as a liquid beverage under the supervision of study personnel on Monday through Friday and by parents or other caregivers during the weekends. The composition of the supplements is shown in Table 1. Fieldworkers recorded the amount of supplement consumed in their presence each day and any amount reportedly given by caregivers at other times. Eighty-three children (29 in the placebo group, 28 in the Zn group, and 26 in the ZnѿVM group; P ҃ 0.82) consumed additional iron, either as prescribed by the study team because of anemia at baseline (hemoglobin 쏝 9.0 g/dL) or for familydetermined reasons. Of these 83 children, 56 (22 in the placebo group, 18 in the Zn group, and 16 in the ZnѿVM group; P ҃ 0.47) received additional iron for 욷 7 d. Household surveillance for morbidity During the weekday home visits, the fieldworkers asked about the children’s health, including the number and characteristics of all stools passed each day since the last visit. In cases in which the caregiver was absent from the home, retrospective data were collected subsequently for a maximum of 7 d. When the caregiver reported any new sign of illness (eg, lethargy, cough, fever, diarrhea, or skin lesions) or a worsening of an existing illness, the child was examined by the fieldworker. In addition, all children were examined at the end of the month if they had not been examined previously that month. Examination always included assessment of hydration status, measurement of rectal tempera-
Supplement
Ingredient para-Aminobenzoic acid (mg) Zinc, as gluconate (mg)2 Magnesium, as carbonate (mg)2 Iron, as ferrous sulfate (mg)2 Copper, as sulfate (mg)2 Selenium, as sodium selenate (g)2 Vitamin A, as palmitate (g) Vitamin D3 (g) Vitamin E, acetate (IU) Vitamin C (mg) Niacin (mg) Thiamine (mg) Riboflavin (mg) Pyridoxine (mg) Vitamin B-12 (g) Folic acid (g) Strawberry flavor, SD GL 13892 (mg)3 Red color, Rojo rubi 7017/NEC (mg)3 Yellow color, Tartrazine 1000/NEC (mg)3 Vitamin C (mg)
Placebo
Zinc only
10
10 10
80 35 5 50
80 35 5 50
ZincѿVM 10 10 50 10 0.65 23 450 6.4 8.5 50 11.5 1.75 1.45 1.55 6.5 283 80 40 2.5 50
1
The filler used was Maltrin M100 (Ross Laboratories, Columbus, OH). All 3 original supplements also contained sugar, red punch flavor, silicon dioxide, and powdered citric acid, as prepared by the manufacturer. VM, vitamins and minerals at 1–2 times recommended daily intakes. 2 Values for elemental mineral. 3 Manufactured by Globe Sabores y Fragrancias, Lima, Peru; added to mask the color and metallic taste of the supplements.
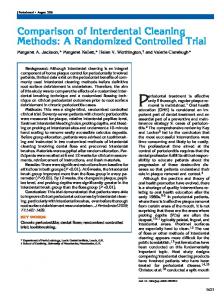
ture, and monitoring of respiratory rate, which was counted for 1 min and repeated if the rate was greater than age-specific upper limits (50/min for children aged 6 –11 mo and 40/min for children aged 쏜 11 mo). Children were referred to the study physician for diagnosis and treatment when the fieldworker or caregiver was concerned about the child’s health status or if the child had any one of several predefined signs of illness, including fever, presentation or worsening of cough with elevated respiratory rate (ie, fieldworker-defined acute lower respiratory infection), persistent diarrhea, diarrhea with signs of dehydration, or vomiting or skin conditions requiring diagnosis. Additional information on characteristics of the home, occupation and education of the parents, and hygiene practices and feeding pattern of the children at the beginning of and during the study was obtained by questionnaire or by direct observation. Children were followed until they completed 6 mo in the study, had no symptoms of illness, and their final blood test was completed. Criteria for terminating the study early in individual children included death of the child, permanent departure from the area, parental decision to withdraw, and, in one case, inability of the study personnel to obtain reliable information (Figure 1). Anthropometry Anthropometric assessments were completed at the time of the enrollment episode, on day 15, and then monthly for 6 mo. Weight was determined with a mechanical beam balance with a precision of 1 g (model 1119-DO; O’Haus, Florham Park, NJ); supine length was measured to 1 mm with a locally constructed
ZINC SUPPLEMENTATION AND CHILD MORTALITY
459
insufficient to allow a second measurement. Plasma ferritin concentrations were measured by (IRI kit; Diagnostics Products Corporation, Los Angeles). Sample size A sample size of 70 per group for the principal morbidity outcomes was calculated to be sufficient to detect a 25% difference between the placebo and each of the supplemented groups in subsequent prevalence and incidence of diarrhea and a 50% reduction in new episodes of persistent diarrhea, considering a probability of type I and type II errors of 0.05 and 0.2, respectively, and based on information from previous studies in the same communities (14, 17). The number of children who completed the study exceeded the calculated sample size requirements for all principal outcomes. Data analysis
FIGURE 1. Flow diagram of study participants. VM, vitamins and minerals at 1–2 times recommended daily intakes.
rigid measuring board; midupper arm circumference was measured to within 1 mm with a flexible, nonstretch tape; and biceps, triceps, suprailiac, and subscapular skinfold thicknesses were measured to within 0.1 mm with a Lange caliper (Beta Technology Inc, Santa Cruz, CA). Ninety-seven percent of the measurements were taken by 1 of 2 persons, and 70% were taken by a single person. The anthropometrists were standardized at the beginning of the study, and training exercises were repeated at intervals during the study. Blood samples and laboratory analyses Nonfasting venous blood was drawn between 0900 and 1200 with the use of mineral-free, lithium-heparin syringes (Sarstedt Inc, Newton, NC). Samples were obtained at enrollment, on day 15, and after 6 mo for measurement of hemoglobin, hematocrit, and plasma zinc. Hemoglobin was measured in the field with a portable Hemocue device (AB Leo Diagnostics, Helsingborg, Sweden). Plasma was separated in acid-washed glassware, and aliquots were stored in mineral-free, colorless plastic vials at Ҁ20 °C until processed. The materials and procedures were checked to rule out possible zinc contamination before sampling started. For the measurement of plasma zinc concentration, 2.2 mL of 1 N Ultrex II ultrapure HNO3 (J T Baker Inc, Phillipsburg, NJ) was added to 200 L plasma (12:1 dilution) in polypropylene tubes and allowed to stand overnight at 4 °C. The samples were then centrifuged (8 min, 앒24 °C), and the supernatant fluid was analyzed for trace element concentrations with a Tracescan inductively coupled plasma atomic emission spectrometer (Thermo Jarrell Ash; Spectrocell Inc, Oreland, PA). All samples from the same child were measured in a single analytic run and were compared with appropriate ultrapure acid blanks, pooled plasma samples, and inductively coupled plasma standards (QC-21 Spex; Fisher Scientific, Pittsburgh). Specimens were run in duplicate unless the quantity of available sample was
Data were recorded in the field on pretested forms, which were checked by the field supervisor before the data were entered in computers with the use of programs that had range and logical checks incorporated. About 10% of the data were double-entered to check keypuncher accuracy; such errors were 쏝 0.5%. Univariate analysis was used to identify outliers and extreme values, which were then double-checked against the original field forms. The plan of analysis, including cutoff values for categorical analyses, was determined before the final analysis and before the codes were broken. Analyses were done by using SPSS-PC (version 9; SPSS Inc, Chicago) and SAS (SAS for WINDOWS version 6.12; SAS Institute Inc, Cary, NC). Groups were compared with analysis of covariance by using treatment group as the main effect and sex, age category, stunting, wasting, initial zinc category, initial ferritin category, breastfeeding status, hygiene score, socioeconomic status variables, and number of liquid stools on the day before enrollment as covariates. Nonsignificant covariates were removed in stepwise fashion; a P value 쏜 0.05 was the criterion for exclusion from the model. Adjusted means were compared among groups with Tukey’s test. Collapsed socioeconomic variables were created by using variable clustering techniques and factor analysis (PROC VARCLUS and PROC FACTOR) to aggregate individual items into logical categories. Scale variables were then created from the 4 categories that were derived representing house quality, household size, possessions, and parental characteristics. Several aspects of home hygiene were observed monthly and used to compute a hygiene score for each household. During each monthly assessment, the fieldworkers rated each of the following items as adequate or inadequate using predefined categories: general tidiness of the house, cleanliness of the floor, appearance of the child, stool disposal methods, handling of diapers, and condition of the child’s play area. The hygiene score for each subject was calculated as the mean of the hygiene scores for all visits. Information was also collected weekly on the children’s breastfeeding status. Definitions Diarrhea was defined as 욷 3 liquid or loose stools in 24 h. An episode was considered to have ended on the last day of diarrhea followed by 2 diarrhea-free days. If visible blood was reported or observed in any stool during a diarrheal episode, the illness was considered an episode of dysentery. Persistent diarrhea was defined as diarrhea lasting 욷 14 d. Severe diarrhea was defined as
460
PENNY ET AL
TABLE 2 Characteristics of the children at enrollment by treatment group1 Treatment group
Variable Male:female Age at enrollment (mo) Received breast milk (%) Anthropometrics at enrollment Initial body weight (kg) Weight-for-age z score Length (cm) Length-for-age z score Stunted, length-for-age z score 쏝 Ҁ2 SD (%) Weight-for-length z score Midupper arm circumference (cm) Sum of 4 skinfold thicknesses (mm)5 Midupper arm muscle area (mm2) Socioeconomic variables Maternal education (y) Paternal education (y) Number of children in household aged 쏝18 y Plasma zinc concentration (g/dL) Children with a low plasma zinc concentration, 쏝65 g/dL (%) Hemoglobin (g/dL) Hematocrit (%) Plasma ferritin concentration (g/L) Children with a low plasma ferritin concentration, 쏝12 g/L (%) Plasma retinol concentration (g/dL) Children with a low plasma retinol concentration, 쏝20 g/dL (%)
Placebo (n ҃ 79)
Zinc only (n ҃ 80)
ZincѿVM (n ҃ 79)
P2
42:37 18.5 앐 7.44 44.3
38:42 19.3 앐 8.1 46.2
54:27 19.1 앐 8.2 46.9
0.043 0.77 0.943
9.8 앐 1.9 Ҁ1.07 앐 0.86 76.3 앐 7.3 Ҁ1.52 앐 1.05 29.5 Ҁ0.10 앐 0.73 14.7 앐 1.2 26.9 앐 5.4 1217 앐 188
9.8 앐 1.9 Ҁ1.19 앐 1.00 76.5 앐 7.0 Ҁ1.60 앐 0.98 35.0 Ҁ0.22 앐 0.85 14.8 앐 1.3 27.0 앐 6.4 1193 앐 184
10.3 앐 2.1 Ҁ0.87 앐 0.97 77.8 앐 7.8 Ҁ1.22 앐 1.02 18.5 Ҁ0.11 앐 0.81 14.9 앐 1.3 26.9 앐 6.5 1214 앐 204
0.29 0.096 0.38 0.044 0.0593 0.59 0.85 0.99 0.70
4.2 앐 2.5 5.3 앐 2.4 3.2 앐 1.7 70.2 앐 15.0
3.9 앐 2.6 5.5 앐 2.4 3.2 앐 1.9 70.4 앐 12.1
4.2 앐 2.5 5.2 앐 2.3 3.8 앐 1.8 70.8 앐 15.7
0.74 0.75 0.07 0.97
35.1 10.2 앐 1.4 32.2 앐 3.3 17 앐 15
35.5 10.5 앐 1.3 33.0 앐 3.6 18 앐 19
43.6 10.1 앐 1.3 32.2 앐 3.0 15 앐 12
0.473 0.18 0.19 0.746
48.5 26.4 앐 7.7
46.8 27.0 앐 8.3
53.2 25.9 앐 8.0
0.763 0.73
22.5
15.7
24.6
0.413
1
VM, vitamins and minerals at 1–2 times recommended daily intakes. ANOVA unless otherwise stated. 3 Chi-square test. 4 x 앐 SD. 5 Triceps, biceps, subscapular, and suprailiac skinfold thicknesses. 6 Kruskal-Wallis test. 2
an episode lasting 욷 1 d with any 1 of the following signs or symptoms: 욷 6 liquid stools, reported or documented fever, documented dehydration, use of any health service for treatment of diarrhea, or the presence of visible blood in any stool. The definition of vomiting excluded regurgitation, which was defined as intentional spitting out or return of recently consumed food or supplement within 15 min after it was ingested. Acute lower respiratory infection was defined according to the “fieldworker definition” as cough plus 2 consecutive age-specific elevated respiratory rates (쏜 50/min for children aged 6 –11 mo and 쏜 40/ min for children aged 쏜 11 mo) or according to the “physician definition” as an episode of bronchitis, pneumonia, asthma, or bronchiolitis diagnosed by the physician’s clinical examination. The physician’s diagnosis of pneumonia was based on the presence of cough and crepitations on chest auscultation. Fever was defined as either reported fever or a rectal temperature 쏜 38 °C, and children were considered to have a poor appetite when the caregiver stated that the child’s dietary intake was reduced from normal. Incidence rates are given as the number of new episodes of illness per 100 d of observation, and prevalence rates are
expressed as the percentage of days of observation when the relevant symptoms or signs were present.
RESULTS
Initial characteristics of the study subjects The initial characteristics of the 246 children admitted to the second phase of the study are shown in Table 2. The children showed a pattern of stunting without wasting, which is typical of urban preschool children in Peru (18). There was a significantly greater proportion of boys in the ZnѿVM than in the Zn group (P ҃ 0.04, chi-square test), and children in the Zn group had a marginally lower mean length-for-age z score, but there were no other group-related differences in initial anthropometric variables or characteristics of the initial episode of persistent diarrhea. Likewise, there were no differences between the study groups with regard to any of the specific socioeconomic characteristics, including housing and possessions, parental education, presence of parents at home, number of people in the household,
461
ZINC SUPPLEMENTATION AND CHILD MORTALITY TABLE 3 Biochemistry outcomes by treatment group1 Treatment group
Outcome Change in plasma zinc concentration (g/dL) Change in hematocrit (%) Change in hemoglobin (g/dL) Change in plasma ferritin concentration (g/L)
P
Placebo (n ҃ 69)
Zinc only (n ҃ 65)
ZincѿVM (n ҃ 70)
Unadjusted2
Adjusted3
6.1 앐 23.0a 1.52 앐 3.44a 0.83 앐 1.32a
27.3 앐 33.7c 0.00 앐 3.88a 0.33 앐 1.41a
16.2 앐 29.8b 2.47 앐 3.38b 1.53 앐 1.34b
쏝0.0001 0.0003 쏝0.0001
쏝0.0001 0.002 쏝0.0001
16.4 앐 24.2b
0.0005
0.0004
Ҁ0.5 앐 15.3a
8.1 앐 47.0a,b
x 앐 SD. VM, vitamins and minerals at 1–2 times recommended daily intakes. 2 Groups compared with ANOVA, with outcome variables suitably transformed. 3 Groups compared with analysis of covariance, potentially controlled for initial age, sex, initial length-for-age, initial weight-for-length, breastfeeding status, initial plasma zinc, initial plasma ferritin, iron supplementation, mean hygiene score, family size, possessions score, housing quality, parental characteristics, severity of diarrhea on enrollment, and initial value of the outcome variable. Adjusted means were compared with Tukey’s test; values in the same row with different superscript letters are significantly different, P 쏝 0.05. 1
or the composite indexes of socioeconomic status or hygienic conditions of the household. However, socioeconomic and hygiene scores did predict morbidity, so they were included as covariables in the subsequent analyses. Biochemical indicators of nutritional status, including plasma zinc concentration, were not different at enrollment (Table 2). Six children (4 in the placebo group, 1 in the Zn group, and 1 in the ZnѿVM group) were withdrawn from the study by their parents after randomization, but before any morbidity data were collected. For the remaining 240 children, information on morbidity was available for 쏜 90% of days during the period of supplementation (95% for the placebo group, 92% for the Zn group, and 97% for the ZnѿVM group). Consumption of supplement There was a high level of adherence to the supplementation protocol, with mean reported daily intake volumes of 94.1%, 92.3%, and 89.5% in the placebo, Zn, and ZnѿVM groups, respectively. Consumption of the supplement was slightly lower in the ZnѿVM group than in the placebo group (P ҃ 0.019, Tukey’s test for means weighted by days of observation), but there were no significant differences between Zn and placebo groups or between the Zn and ZnѿVM groups. Similar results were found when the analysis was restricted to days when consumption of the supplements was observed by the fieldworkers. Vomiting, excluding regurgitation, occurring within 15 min of taking the supplement was more common in the ZnѿVM group (4.8% of doses) than in the placebo group (0.6% of doses) or the Zn group (0.6% of doses) (P 쏝 0.0001, log transformation). Biochemical measures Both baseline and final plasma zinc concentrations were measured in 204 children (n ҃ 69, 65, and 70 in the placebo, Zn, and ZnѿVM groups). Mean plasma zinc concentrations increased by 6.1 g/dL in the placebo group, 27.3 g/dL in the Zn group, and 16.2 g/dL in the ZnѿVM group. Differences between the groups are significant (P 쏝 0.0001, ANOVA). With control for initial plasma zinc concentration, the rise in plasma zinc was greater in the Zn group than in both the placebo (P 쏝 0.0001) and the ZnѿVM (P ҃ 0.053) groups and greater in the ZnѿVM group than in the placebo group (P ҃ 0. 049) (Table 3). All
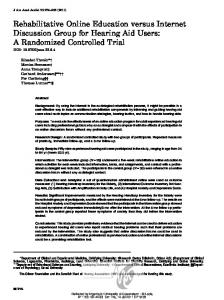
groups showed a significant increase in hemoglobin from the initial values, and these changes from baseline to 6 mo were significantly different between groups (P 쏝 0.001; Table 3). The ZnѿVM group, who received iron in the micronutrient supplement, had an increase in mean hemoglobin of 1.53 g/dL, which was significantly greater than the increase of 0.83 g/dL in the placebo group and the increase of 0.33 g/dL in the Zn group (P 쏝 0.0001). Hematocrit increased in the ZnѿVM group by 2.47%, which was significantly greater (P 쏝 0.001) than the increase of 1.52% in the placebo group and the 0% increase in the Zn group. The plasma ferritin concentration increased by 16.4 g/L in the ZnѿVM group and by 8.1 g/L in the Zn group and decreased by 0.5 g/L in the placebo group. The differences between the groups were significant (P 쏝 0.001). Morbidity outcomes Children in this community had high incidences of infectious illness. There was a pattern of very frequent, but generally mild, diarrheal episodes of short duration. The mean incidence of diarrheal episodes was 4.7 episodes/100 days of observation, and the prevalence of diarrhea was 13.9%. The mean duration of the episodes was 2.9 d, and less than one-half of the episodes were considered severe. Only 28 episodes of persistent diarrhea (욷 14 d) were recorded in 19 children. Respiratory symptoms were common, with cough reported on 49.4% of days. A total of 537 episodes of acute lower respiratory infections were identified, of which 68 were based only on the fieldworker report, 283 were diagnosed by the doctor in children who had not been referred by the fieldworker, and 186 were diagnosed by the fieldworker and confirmed by the doctor. Fifty episodes of pneumonia, as diagnosed by the physician, occurred in 43 children. Reduced appetite was reported on 9.2% of days, and fever was reported on 6.5% of days. For every illness variable analyzed, the direction of the differences between the Zn group and the placebo group tended toward less illness in the Zn group, whereas the direction of the differences between the ZnѿVM group and the placebo group tended toward more illness in the ZnѿVM group. The particular differences that were statistically significant are indicated in Figure 2. The results of the analysis of covariance models in which the adjusted means of morbidity outcomes were compared
462
PENNY ET AL
FIGURE 2. Percentage change (adjusted x 앐 SE) in morbidity outcomes in the group who received 10 mg Zn alone (■, Zn group; n ҃ 80) and in the group who received 10 mg Zn plus vitamins and other minerals at 1–2 times recommended daily intakes (䊐; n ҃ 81) relative to the placebo group (n ҃ 79). *Significantly different from the Zn group, P 쏝 0.05 (Tukey’s test). ALRI, acute lower respiratory infection. ‡Significantly different from the placebo group, P 쏝 0.05 (Tukey’s test).
by treatment group are shown in Table 4. Variables included in the models were age, sex, initial length-for-age, initial weightfor-length, severity of the diarrhea at entry, baseline plasma zinc concentration, baseline plasma ferritin concentration, consumption of additional therapeutic iron supplements, and hygiene score. Age, length-for-age, number of liquid stools at entry, and hygiene score predicted diarrhea morbidity. The significance values given in Table 4 refer to the results of the general linear models procedure. There was a consistent trend for reduced morbidity in the children who received zinc alone compared with
those who received placebo, and this difference was statistically significant for the prevalence of days with cough (P 쏝 0.05, Tukey’s test). In contrast, children in the ZnѿVM group had significantly greater rates of morbidity than did the Zn group for the incidence of severe diarrhea, prevalence of cough, prevalence of fever (all P 쏝 0.05, Tukey’s test) and the proportion of children with at least one episode of dysentery (P ҃ 0.05, chi-square test). Adding initial iron status (plasma ferritin 쏝 12 g/L) to the model, as an interaction term with treatment group, did not account for the differences in morbidity between the groups; however, therapy with additional ferrous sulfate to treat anemia was a significant predictor of fieldworker-defined acute lower respiratory infection, independent of treatment group. Children receiving iron therapy also had a higher rate of cough (P 쏝 0.01) than did those not receiving iron therapy. Anthropometry The results of the analysis of covariance models in which the adjusted means of anthropometry outcomes were compared by treatment group are shown in Table 5. There was no significant difference between groups in length gain during the 6-mo period of supplementation (P ҃ 0.61). In the full model that controlled for initial length, hygiene score, breastfeeding status, and time elapsed between measurements, there tended to be a difference between treatment groups (P ҃ 0.062) that favored both zinc groups relative to the placebo group, but there were no significant differences in changes in length-for-age z score (P ҃ 0.65) or weight gain (P ҃ 0.40) by treatment group. The 3 groups tended to be different with regard to unadjusted change in weight-forage z score (P ҃ 0.068), but this difference became nonsignificant in the full model (P ҃ 0.16). No differences between groups
TABLE 4 Morbidity outcomes by treatment group1 Treatment group
Outcome Incidence of diarrhea (episodes/100 d observed) Incidence of severe diarrhea (episodes/100 d observed) Prevalence of diarrhea (% of days observed) Duration of diarrheal episodes (d) Children with any episode of dysentery (%) Children with any episode of persistent diarrhea (%) Prevalence of cough (% of observed days) Incidence of ALRI, diagnosed by a physician or fieldworker (episodes/100 d observed) Incidence of ALRI, diagnosed by a fieldworker (episodes/ 100 d observed) Children with any episode of pneumonia (%) Prevalence of fever (% of observed days) Prevalence of anorexia (% of observed days) 1
P
Placebo (n ҃ 79)
Zinc only (n ҃ 80)
ZincѿVM (n ҃ 81)
Unadjusted2
Adjusted3
4.86 앐 2.464 1.97 앐 1.51a,b 13.2 앐 9.9 2.7 앐 1.1 42 (31, 53)a,b,5 3.8 (0, 8) 51.0 앐 23.1a
4.32 앐 2.27 1.63 앐 1.19b 11.5 앐 9.1 2.7 앐 1.1 39 (28, 50)a 7.5 (1.6, 13.4) 42.0 앐 22.9b
4.96 앐 2.68 2.34 앐 1.69a 16.3 앐 14.9 3.3 앐 2.3 58 (47, 69)b 12.4 (5.0, 19.7) 54.7 앐 25.5a
0.30 0.07 0.08 0.05 0.036 0.136 0.004
0.25 0.04 0.10 0.20 — — 0.005
1.26 앐 1.19
1.11 앐 0.96
1.41 앐 1.05
0.31
0.46
0.61 앐 1.36a,b 15 (7, 23) 6.6 앐 4.6a,b 8.5 앐 7.4
0.53 앐 0.91a 15 (7, 23) 5.6 앐 5.0a 8.0 앐 7.9
0.72 앐 0.91b 22 (12, 30) 7.3 앐 5.5b 10.0 앐 9.3
0.18 0.536 0.03 0.30
0.06 — 0.06 0.46
VM, vitamins and minerals at 1–2 times recommended daily intakes; ALRI, acute lower respiratory infection. Groups compared with ANOVA, with outcome variables suitably transformed, except where noted. 3 Groups compared with analysis of covariance, potentially controlled for initial age, sex, initial length-for-age, initial weight-for-length, breastfeeding status, initial plasma zinc, initial plasma ferritin, iron supplementation, mean hygiene score, family size, possessions score, housing quality, parental characteristics, and severity of diarrhea on enrollment. Adjusted means were compared with Tukey’s test; values in the same row with different superscript letters are significantly different, P 쏝 0.05. 4 x 앐 SD. 5 x ; 95% CI in parentheses. 6 Groups compared with Pearson’s chi-square test of homogeneity; Bonferroni adjustment was used for individual comparisons. 2
463
ZINC SUPPLEMENTATION AND CHILD MORTALITY TABLE 5 Anthropometric outcomes by treatment group1 Treatment group
Change in outcome Length (cm/6 mo) Length-for-age z score Weight (kg/6 mo) Weight-for-age z score Sum of 4 skinfold thicknesses (mm/6 mo) Midupper arm circumference (mm/6 mo)
P
Placebo (n ҃ 75)
Zinc only (n ҃ 71)
ZincѿVM (n ҃ 78)
Unadjusted2
Adjusted3
5.0 앐 1.4 0.10 앐 0.43 1.42 앐 0.54 0.24 앐 0.39 2.7 앐 4.6 7.4 앐 8.1
5.3 앐 1.4 0.16 앐 0.44 1.48 앐 0.67 0.34 앐 0.59 3.3 앐 5.2 7.3 앐 9.2
5.2 앐 1.4 0.09 앐 0.39 1.32 앐 0.69 0.13 앐 0.60 2.0 앐 5.2 5.3 앐 9.4
0.61 0.51 0.29 0.068 0.29 0.25
0.062 0.65 0.40 0.16 0.31 0.39
x 앐 SD. VM, vitamins and minerals at 1–2 times recommended daily intakes. Groups compared with ANOVA. 3 Groups compared with analysis of covariance, potentially controlled for initial age, sex, initial length-for-age, initial weight-for-length, breastfeeding status, initial plasma zinc, initial plasma ferritin, iron supplementation, mean hygiene score, family size, possessions score, housing quality, parental characteristics, severity of diarrhea on enrollment, and initial value of the outcome variable. Adjusted means were compared with Tukey’s test; values in the same row with different superscript letters are significantly different, P 쏝 0.05. 1 2
in the change in the sum of the 4 skinfold thicknesses (P ҃ 0.31) or change in midupper arm muscle area (P ҃ 0.39) were observed. DISCUSSION
This study was designed to test whether 6 mo of daily zinc supplementation with or without other micronutrients would reduce morbidity and enhance growth in children with persistent diarrhea at baseline. Children presenting with persistent diarrhea were selected for the study because they were felt to be at especially high risk of zinc deficiency and subsequent high morbidity. Our finding of a consistent tendency for reduced morbidity in children receiving zinc supplements is in keeping with other studies (7), although in our study only the reduction in cough was statistically significant. In contrast, we observed higher rates of these illnesses when other micronutrients were provided together with zinc. The strengths of this study included its randomized, doubleblind design and the supervised administration of the supplements. Except for differences in the relative proportions of boys and girls and the minor differences in initial anthropometric status, the groups were similar at baseline, and child sex and anthropometric variables were controlled during the statistical analyses. Thus, any differences in study outcomes were likely due to the treatments that were provided. Surveillance was conducted daily, so reporting error was unlikely; 쏝 8% of the children dropped out of the study, and no significant differential loss to follow-up between the groups was observed. Although treatment compliance was slightly lower and the number of vomiting episodes was greater after supplementation in the ZnѿVM group than in the ZN and placebo groups, compliance was still high in all 3 groups, and it is unlikely that the minor differences that occurred in consumption of the supplements explained the observed differences in morbidity outcomes. When the compliance variable and a group-by-compliance interaction were included in the model, the results were unchanged. Overall, the study group was likely to have been zinc deficient, as indicated by the high percentage of children with low plasma zinc concentrations, and the prevalence of diarrhea was high, as predicted. The micronutrients contained in the supplements were reasonably well absorbed, as indicated by the increase in plasma zinc
concentrations in both zinc-supplemented groups and the increase in hemoglobin concentration in the ZnѿVM group. However, it is apparent that some nutrient-nutrient interactions did occur, in that plasma zinc concentrations increased less in the ZnѿVM group than in the Zn group. Although we cannot be certain, it is highly likely that the lower plasma zinc concentration in the ZnѿVM group than in the Zn group was due to the iron included in the vitamin-mineral mix. It was clearly shown that iron inhibits zinc absorption in humans when these minerals are given together in aqueous solution (12), and infants in a recent study in Java who received supplements containing both iron and zinc had significantly lower plasma zinc concentrations than did those who received zinc only (19). It is also conceivable that zinc inhibited iron absorption from the ZnѿVM supplement, as was observed in previous studies (19, 20), but the design of the current study did not permit detection of that possibility. The sample size was calculated to allow us to distinguish differences of 25% in changes in morbidity. Combined analysis of similar studies showed 앒20% reductions in diarrhea morbidity (7), so our sample may have been too small to detect this effect size with statistical confidence. Nevertheless, our results are consistent with the hypothesis that zinc supplements taken alone reduce diarrheal and respiratory illness, which agrees with the results of other studies (7, 9). Contrary to our original hypothesis, we found a consistent increase in rates of diarrhea and respiratory illnesses when a full set of micronutrients was provided along with zinc. The design of the study did not permit us to attribute the adverse effect on morbidity to individual micronutrients included in the ZnѿVM supplement. Some other studies with single micronutrients also reported adverse outcomes, especially when the supplements were provided to children who were replete with respect to the micronutrient. For example, Sempertegui et al (21) reported that Ecuadorian children with a normal weight-for-age had an increase in acute lower respiratory infections after receiving supplemental vitamin A. Increased cough was also reported after vitamin A supplementation in India (22), Indonesia (23), and Haiti (24). Because of reports of an increased incidence of malaria, diarrhea, and tuberculosis after parenteral iron supplementation (25–27), and because of the known enhancement of bacterial virulence provided by iron (28), iron
464
PENNY ET AL
supplements have also come under suspicion. However, some studies have not found increased malarial morbidity with oral iron supplementation (29). Although few studies have provided definitive evidence that oral iron supplementation causes increased infectious morbidity in nonmalarial areas (30), some studies have documented increased rates of diarrhea, particularly in infants aged 쏝 12 mo. In one study, for example, Bangladeshi infants aged 2–11 mo who received 15 mg elemental Fe/d had a higher incidence of diarrhea and an increase in the total number of days of diarrhea during the year (31). In Chile, Brunser et al (32) reported increased diarrhea from shigellae in infants who received iron-enriched milk. In a study of infants in Honduras and Sweden (33), lower growth and increased morbidity were reported in the subgroup of iron-replete children who received iron supplements. Children in the current study were older than those enrolled in these aforementioned trials, and the children in the current study seemed to have an increase in symptoms of respiratory disease as well as diarrhea. One factorial trial of iron, zinc, or iron plus zinc supplements in Mexico (34) reported 7–23% more respiratory illness in the iron-supplemented group than in the placebo group, whereas those who received zinc alone and zinc plus iron had less morbidity than did those who received placebo. Given these sets of results and the absence of reports of adverse events associated with the other micronutrients in our mixture, iron may be the most likely component of the mixture responsible for the increased rates of morbidity that were observed. The dose of iron in the supplement provided in the current study was 10 mg elemental Fe, 앒1 mg · kg body wtҀ1 · dҀ1, which is the standard recommended prophylactic dose for infants (35). The iron was given between meals in an aqueous solution along with vitamin C, which may have enhanced absorption of iron from the supplement. It is also possible that the children in the ZnѿVM group were subjected to a higher concentration of unabsorbed iron in the small intestine, which could create a local iron-rich environment that would enhance bacterial proliferation, because it is known that many pathogens require iron (28), or impair mucosal immune function, possibly in response to iron-induced cytokine secretion (36). Although speculative, these 2 mechanisms could possibly explain the adverse gastrointestinal outcomes observed in the ZnѿVM group. On the other hand, the fact that respiratory outcomes were also affected by the ZnѿVM supplement suggests that a systemic effect may have been operative. We found no effects of the supplements on physical growth. This is in contrast with other studies and with the findings of a recent meta-analysis of zinc supplementation and child growth (3), in which stunted children who received zinc supplements had increased linear growth and weight gain. Control for initial length-for-age in the analysis of the current study did not alter this conclusion, but only 28% of the study subjects were stunted (쏝 Ҁ2 SD), and our study was not powered to show differences in this fairly small number of children. The results of the current study provide additional support for the efficacy of zinc supplements in reducing childhood morbidity in zinc-deficient populations but also suggest a need for caution regarding possible adverse events when other micronutrients are provided with zinc supplements. More studies are needed to determine which nutrients are responsible for the adverse effects that were observed and to confirm the safety of multiple micronutrient supplementation. Unfortunately, confirmation of the current findings would complicate public health programs be-
cause such results would imply a need for prior screening of micronutrient status, differential dosing of micronutrients, or both. Given the large number of children who are possible targets of micronutrient supplementation programs, screening could considerably increase program costs. Thus, more studies are needed in a range of different populations to establish appropriate policy recommendations concerning the optimal use of multiple micronutrient supplements. We are very grateful to all the parents who cooperated in allowing us to undertake this study and to the Instituto de Investigacio´ n Nutricional team for their dedication and professionalism in the execution of this study. The zinc analyses were conducted at the Department of Nutrition, University of California, Davis, by Natalia Leon and Joel Commisso. The study was designed by KHB, MEP, REB, and CFL with advice from BL. KHB wrote the grant application. MEP directed the field study. AD was the field coordinator. RMM was responsible for the study design and the supervision of the entry and preliminary analysis of the data. BL was responsible for the biochemical analyses. JP was responsible for the data analysis. MEP and KHB wrote the first draft of the manuscript with help from REB and BL. All of the authors reviewed the final manuscript. None of the authors had any conflicts of interest.
REFERENCES 1. Hambidge M. Human zinc deficiency. J Nutr 2000;130:1344S–9S. 2. Shankar AH, Prasad AS. Zinc and immune function: the biological basis of altered resistance to infection. Am J Clin Nutr 1998;68(suppl):447S– 63S. 3. Brown KH, Peerson JM, Rivera J, Allen LH. Effect of supplemental zinc on the growth and serum zinc concentrations of prepubertal children: a meta-analysis of randomised trials. Am J Clin Nutr 2002;75:1062–71. 4. Gibson RS. Zinc nutrition in developing countries. Nutr Res Rev 1994; 7:151–73. 5. Gibson RS, Hotz C. Dietary diversification/modification strategies to enhance micronutrient content and bioavailability of diets in developing countries. Br J Nutr 2001;85(suppl):S159 – 66. 6. Castillo-Duran C, Vial P, Uauy R. Trace mineral balance during acute diarrhea in infants. J Pediatr 1988;113:452–7. 7. Zinc Investigators’ Collaborative Group. Prevention of diarrhea and pneumonia by zinc supplementation in children in developing countries: pooled analysis of randomised controlled trials. J Pediatr 1999; 135:689 –97. 8. Gibson RS, Ferguson EL. Assessment of dietary zinc in a population. Am J Clin Nutr 1998;68 (suppl):430S– 4S. 9. Bhan MK, Sommerfelt H, Strand T. Micronutrient deficiency in children. Br J Nutr 2001;85(suppl):S199 –203. 10. Solomons NW. Competitive interaction of iron and zinc in the diet: consequences for human nutrition. J Nutr 1986;116:927–35. 11. Whittaker P. Iron and zinc interactions in humans. Am J Clin Nutr 1998;68:(suppl)442S– 6S. 12. Sandström B, Davidsson L, Cederblad A, Lönnerdal B. Oral iron, dietary ligands and zinc absorption. J Nutr 1985;115:411– 4. 13. Duggan C, Penny ME, Hibberd P, et al. Oligofructose-supplemented infant cereal: two randomised, blinded, community-based trials in Peruvian infants. Am J Clin Nutr 2003;77:937– 42. 14. Black RE, Lopez de Roman˜ a G, Brown KH, Bravo N, Grados Bazalar O, Kanashiro HC. Incidence and etiology of infantile diarrhea and major routes of transmission in Huascar, Peru. Am J Epidemiol 1989;129: 785–99. 15. Brown KH, Lanata CL, Yuen ML, Peerson JM, Butron B, Lönnerdal B. Potential magnitude of the misclassification of a population’s trace element status due to infection: example from a survey of young, Peruvian children. Am J Clin Nutr 1993;58:549 –54. 16. Penny ME, Peerson JM, Marin RM, et al. Randomised community based trial of the effect of zinc supplementation, with and without other micronutrients, on the duration of persistent childhood diarrhea in Lima, Peru. J Pediatr 1999;135:208 –17. 17. Lanata CF, Black RE, Gilman RH, Lazo F, Del Aguila R. Epidemiologic, clinical and laboratory characteristics of acute vs persistent diarrhea in periurban Lima, Peru. J Pediatr Gastroenterol Nutr 1991;12:82– 8.
ZINC SUPPLEMENTATION AND CHILD MORTALITY 18. Instituto Nacional de Estadistica y Informatica. Encuesta Nacional Demografíca y Salud. (National demographic and health survey.) Lima, Peru: Instituto Nacional de Estadistica y Informatica, 2001. 19. Lind T, Lönnerdal B, Stenlund H, et al. A community-based, randomized, controlled trial of iron and/or zinc supplementation of Indonesian infants—interactions between iron and zinc. Am J Clin Nutr 2003;77: 883–90. 20. Rossander-Hulthén L, Brune M, Sandström B, Lönnerdal B, Hallberg L. Competitive inhibition of iron absorption by manganese and zinc in humans. Am J Clin Nutr 1991;54:152– 6. 21. Sempertegui F, Estrella B, Camaniero V, et al. The beneficial effect of low-dose vitamin A supplementation on acute lower respiratory infections and diarrhea in Ecuadorian children. Pediatrics [serial online] 1999;104:e1. Internet: http://www.pediatrics.org/cgi/content/full/104/1/e1 (accessed 5 December 2003). 22. Ramakrishnan U, Latham MC, Frongillo EA. Vitamin A supplementation and morbidity among pre-school children in South India. Am J Clin Nutr 1995;61:1295–303. 23. Dibley MJ, Sadjimin T, Kjolhede CL, Moulton LH. Vitamin A supplementation fails to reduce the incidence of acute respiratory illness in pre school-age Indonesian children. J Nutr 1996;126:434 – 42. 24. Stansfield SK, Pierre-Louise M, Lerebours G, Augustin A. Vitamin A supplementation and increased prevalence of childhood diarrhoea and acute respiratory infections. Lancet 1993;342:578 – 82. 25. Murray MJ, Murray NJ, Murray AB, Murray MB. Refeeding-malaria and hyperferraemia. Lancet 1975;1:653– 4. 26. Oppenheimer SJ, Macfarlane SB, Moody JB, Bunari O, Hendrickse RG. Effect of iron prophylaxis on morbidity due to infectious diseases: report on clinical studies in Papua New Guinea. Trans R Soc Trop Med Hyg 1986;80:596 – 602.
465
27. Bates CJ, Powers HJ, Lamb WH, Gelman W, Webb E. Effects of supplementary vitamins and iron on malaria indices in rural Gambian children. Trans R Soc Trop Med Hyg 1987;81:286 –91. 28. Keusch GT. Micronutrients and susceptibility to infection. Ann N Y Acad Sci 1990;587:181– 8. 29. Menendez C, Kahigwa E, Hirt R, et al. Randomized placebo controlled trial of iron supplementation and malaria chemoprophylaxis for prevention of severe anaemia and malaria in Tanzanian infants. Lancet 1997; 350:844 –50. 30. Oppenheimer SJ. Iron and its relation to immunity and infectious disease. J Nutr 2001;131:616S–33S. 31. Mitra AK, Akramuzzaman SM, Fuchs GJ, Rahman MM, Mahalanabis D. Long-term oral supplementation with iron is not harmful for young children in a poor community of Bangladesh. J Nutr 1997;127:1451–5. 32. Brunser O, Espinoza J, Araya M, Pacheco I, Cruchet S. Chronic iron intake and diarrhoeal disease in infants. A field study in a less-developed country. Eur J Clin Nutr 1993;47:317–26. 33. Dewey KG, Domellöf M, Cohen RJ, Landa Rivera L, Hernell O, Lönnerdal B. Iron supplementation affects growth and morbidity of breastfed infants: results of a randomized trial in Sweden and Honduras. J Nutr 2002;132:3249 –55. 34. Rosado JL, Lopez P, Mun˜ oz E, Martinez H, Allen LH. Zinc supplementation reduced morbidity, but neither zinc nor iron supplementation affected growth or body composition of Mexican preschoolers. Am J Clin Nutr 1997;65:13–9. 35. National Research Council. Recommended dietary allowances. 10th ed. Washington, DC: National Academy Press, 1989. 36. Srigiridhar K, Nair KM. Iron deficient intestine is more susceptible to peroxidative damage during iron supplementation in rats. Free Radic Biol Med 1998;25:660 –5.