NC 271 04. Address reprint requests to A. Dyer, Department of Radiology, Bowman Gray School of Medicine,. Winston-Salem,. NC 27103. 2 Lexington Memorial.
321
.:
.
The Segmental Ray
Dyer,1
Stephen
Prolongation
of
Miller1
the
.
#{149}1
Nephrogram ,
Bonnie
nephrogram
L. Anderson1
is a common
,
James
finding
E. Drake2,
and
John
S. Shaffer
in
excretory urography, most often due to acute extrarenal obstruction from calculous disease. The persistent nephrogram is usually unilateral and affects the entire kidney. The segmental nephrogram [1 ] represents an uncommon variation in which persistence of the nephrogram occurs in only one part of the kidney. A case is reported, and mechanisms of development and differential diagnostic concerns are discussed.
Case Report A previously pain, blood
healthy 23-year-old
man had acute onset of right flank
radiating into the right groin. Urinalysis cells per high power field. A preliminary
showed
a small calcific
injection increase
of contrast material for excretory in the density of the nephrogram
density
revealed abdominal
in the right anatomic
1 5-20 red radiograph
pelvis. After
urography, progressive in the upper part of the
right kidney was noted (fig. 1A). An 18-hr delayed film (fig. 1B) showed obstruction duplicated
in the ureter draining the upper moiety of a completely system. The stone was cystoscopically extracted via the lower of two ureteral orifices identified in the bladder.
Discussion
The nephrogram, the radiographic image of the renal parenchyma, is produced predominantly by contrast material within the renal tubules with a lesser contribution by contrast material present in renal vascular structures [2]. Urographic contrast material is freely filtered at the nephron and concentrated by water reabsorption in the tubules [2]. Under normal physiologic circumstances, there is no tubular secretion or reabsorption
of the
contrast
material,
and
tubular
concentra-
tion is proportional to plasma concentration [2]. After rapid intravenous injection of contrast material, the maximal nephrographic density normally is achieved within minutes. Persistence of the nephrogram has been described with hypotension [3], as well as in conditions that bring about obstruction either at the tubular level [4] or at a point within the collecting system or ureter. Nephrographic persistence in hypotension and intratubular obstruction due to crystal or protein
precipitation
is ascribed
to slowed
intratubular
transit
A
[4]. These conditions usually produce a bilateral, persistent nephrogram. In the face of acute urinary tract obstruction, increased pressure develops proximal to the site of the obstruction and
Received January 15, 1985; accepted after revision March 18, 198g. 1 Department of Radiology, Bowman Gray School of Medicine, North Carolina Baptist Hospital, Wake Forest University, reprint requests to A. Dyer, Department of Radiology, Bowman Gray School of Medicine, Winston-Salem, NC 27103. 2 Lexington Memorial Hospital, Lexington, NC 27292. AJR 145:321-322,
August
1985 0361-803X/85/1452-0321
C American
B
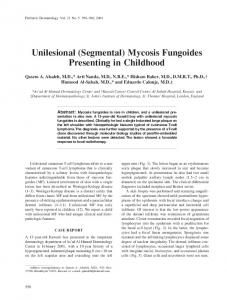
Fig. 1 -A, 2-hr radiograph. Persistent nephrogram in upper part of right kidney. B, 18-hr-delay film. Segmental nephrogram and opacification of right upper collecting system down to small calcified stone in distal ureter (arrow).
Roentgen Ray Society
Winston-Salem,
NC 271 04. Address
DYER
322
is propagated in a retrograde fashion to the renal pelvis and throughout the nephron. Although this is accompanied by reduction in glomerular filtration rate, filtration continues as a result of continued resorption of water from the tubule [5]. The slowed intratubular transit causes hyperconcentration with persistence and progressive increase in density of the nephrogram. This is usually a unilateral process affecting the whole of the kidney. The segmental nephrogram represents persistence of the nephrographic density in some part of the kidney [1 ]. This is most commonly seen when obstruction occurs in one limb of a bifid renal pelvis or in one ureter of a completely duplicated system. The elevated pressure is then transmitted to only those nephrons drained by the obstructed part of the collecting system. Because of the high prevalence of calculous disease and of urinary tract duplication anomalies, their coexistence in the patient should be anticipated. Obstruction in an isolated segment of a nonduplicated collecting system by causes other than calculi may produce a similar finding [6]. On the basis of the mechanisms previously described, causes of a segmental nephrogram apart from obstructive lesions
should
be considered.
A unilateral
hypotensive
neph-
rogram has been described following successful medical treatment of hypertension due to renal artery stenosis [2]. This appearance results from the relative hypotension that occurs in the kidney supplied by the stenotic renal artery. While no such reports exist in the literature to our knowledge, significant stenosis of an intralobar artery might produce a segmental nephrogram as a result of hypotension limited to that part of the kidney perfused by the stenotic vessel. Similarly,
occurs event
slowed
intratubular
transit,
diffusely within the kidney, in association with certain
a condition
that
usually
might occur as a localized pathologic entities. Focal
ET
AL.
AJR:145, August 198S
inflammation (lobar nephronia) [7], localized contusion [8], or segmental renal vein occlusion [9] might be expected to produce focal edema. The resultant increased parenchymal pressure would oppose tubular transit, prolonging transit time with production of a segmental nephrogram. Although uncommon, the segmental nephrogram may produce a striking urographic appearance. Recognition of the segmental nature of the nephrogram usually implies extrarenal obstruction in one limb of some form of duplication. However, on the basis of mechanisms for the production of the persistent dense nephrogram, consideration of other diagnostic concerns may be necessary. REFERENCES 1 Raghavaiah .
NV. Segmental
nephrogram.
J Urol 1978;1 19:278-
279
2. Newhouse JH, Pfister AC. The nephrogram. Radio! Clin North Am 1979;17:213-226 3. Korobkin MT, Kirkwood A, Minagi H. The nephrogram of hypotension.
Radiology
1971;98:
129-133
4. Fry 1K, Cattell WA. The nephrographic pattern during excretion urography. Br Med Bull 1972;28:227-232 5. Brenes LG, Forlano H, Koutouratsas N, Stauffer HM. Mechanism of the nephrographic effect during [Diagn] (Stockh) 1966;4: 14-20
6. Breatnach
ES, Stanley
lonephritis.
of a transitional 1019-1022
MA. The striated
Urol Radio!
stasis.
Acta
AJ, Lloyd K. Focal obstructive
gram: an unusual CT appearance J Comput Assist Tomogr 1984;8:
7. Berliner L, Bosniak
urinary
1981;4:41
nephrogram
Radio!
nephro-
cell carcinoma.
in acute pye-
-44
8. Rubin BE, Schliftman A. The striated nephrogram in renal contusion. Urol Radio! 1979;1 : 1 19-1 21 9. Cool MN, Talner LB. Obstructive nephrogram due to renal vein thrombosis.
Radiology
1971;101
:573-574