Children's Hospital of Eastern Ontario Pain. Scale (CHEOPS) (12) (Table 2). The BOPS is constructed like the Princess Margaret Hospi- tal Pain Assessment ...
Validity and reliability of the Behavioural Observational Pain Scale for postoperative pain measurement in children 1–7 years of age* Karin Hesselgard, RN, PhD; Sylvia Larsson, RN, PhD; Bertil Romner, MD, PhD; Lars-Göran Strömblad, MD, PhD; Peter Reinstrup, MD, PhD
Objective: Pain measurement is a necessity in pain treatment but can be difficult in young children. The aim of this study was to evaluate the validity and reliability of the Behavioural Observational Pain Scale (BOPS) as a postoperative pain measurement scale for children aged 1–7 yrs. The scale assesses three elements of pain behaviors: facial expression, verbalization, and body position. Design: A prospective study. Setting: A day surgery care unit for children and a neurosurgical postoperative care unit. Patients: Seventy-six children aged 1–7 yrs (4.5 ⴞ 1.8) undergoing elective surgical procedures were observed. Interventions: None. Measurements and Main Results: The study was divided into interrater reliability, concurrent validity, and construct validity. The interrater reliabilities of the observers were very good with a high agreement between the different nurses’ BOPS scores. Each item of the BOPS scale ranged from w 0.86 to 0.95. In the
E
ffective pain management in infants and children starts with routine evaluation of pain and clear documentation. This requires assessment of pain intensity and pain relief with reliable, valid, and clinically sensitive assessment tools (1– 4). In a recent Swedish nationwide study, pain assessment was performed in only 43% of all postoperative units for children, and pain measurements with a validated pain scale were less frequent (5). Self-report scales for pain are the best way to assess pain, but they can only be used in children old enough or cognitively competent to express and quantify
*See also p. xx. From the Department of Neurosurgery (KH, BR, LGS) and Department of Anaesthesia & Intensive Care (SL), University Hospital, Lund, Sweden; and the Department of Nursing Science, Lund University, Lund, Sweden (PR). The authors have not disclosed any potential conflicts of interest. Copyright © 2007 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies DOI: 10.1097/01.PCC.0000257098.32268.AA
Pediatr Crit Care Med 2007 Vol. 8, No. 2
concurrent validity, BOPS and Children’s Hospital of Eastern Ontario Pain Scale scores had a positive correlation indicating that both tools described similar behaviors (rs ⴝ .871, p < .001). In construct validity, the effect of analgesic was tested before analgesic administration and at 15, 30, and 60 mins after analgesic administration. The differences in BOPS score between the time intervals were significant (p < .01) before administration of analgesia and at 15, 30, and 60 mins. There was also statistical significance in the BOPS score (p < .01) between 15 and 60 mins after administration of analgesia. Conclusions: With BOPS, the caretaker can evaluate and document pain with high reliability and validity and thereby improve postoperative pain treatment in preschool children. The simple scoring system makes BOPS easy to incorporate in a postoperative unit. (Pediatr Crit Care Med 2007; 8:●●●–●●●) KEY WORDS: children; pain measurement; postoperative pain; Behavioural Observational Pain Scale; reliability; validity
pain (1, 3). According to Anand and Craig (6), self-reports may be absent or a faulty source of inference; nonverbal behavioral information is often needed and used for pain assessment. It is important to ensure that children are able to provide information before their report is accepted, especially those between 3 and 7 yrs of age (3). When children are recovering from anesthesia and in the state of easy arousal, it is difficult for them to self-assess. Before they are fully awake they can be restless, and factors like excitement, agitation, or sedation may influence their outcome (7–9). Preschool children or children who have cognitive and verbal deficits may be unable to describe their feeling of pain or physical discomfort. Therefore, observation of behavior can be an acceptable alternative when valid self-report is not possible (3, 10 –12). Behavioral indicators such as facial expression, crying, and body movements are used to estimate the presence of pain and intensity in nonverbal or preverbal children (4, 10 –13). Some behavioral pain scales can be clinically difficult to use because of the
complexity of the instrument, being unwieldy or lengthy to score and difficult to interpreter to score (14, 15). In 1996 at the Neurointensive Care Unit in Lund, Sweden, the Behavioural Observational Pain Scale (BOPS) (Fig. 1) was developed for nurses and physicians to identify, evaluate, and document pain. It was important that the pain scale was simple, clear, and easy to use for the caregivers. The purpose was to reduce the amount of indicators for pain and simplify the rating system. Facial expression, vocalization, and body movements were used as indicators of pain, as experienced nurses in postoperative care of children regarded these as the most reliable indicators of pain. Former studies have shown a strong correlation between these signs and pain (12, 16 –18). This was further confirmed (11, 19) in 1998 and 2001 in other studies. Reliability and validity are two important criteria for evaluating a quantitative instrument. In pain assessment for children, interrater reliability (1) is important as it provides dependable and trustworthy pain ratings; this is true regardless of the time of testing, the age 1
or gender of the child, and the clinicians who perform the measurement (20). Validity is the degree to which an instrument measures what it supposed to measure (1). The instrument must measure the child’s pain so that a change in pain ratings reflects meaningful differences in pain experience (20). The aim of this study was to test the reliability and validity of the BOPS postoperatively for children aged 1–7 yrs.
PATIENTS AND METHODS Subjects and Setting After approval from the local ethical committee and the parent’s oral and written informed consent, a prospective study was performed between September 2003 and April 2004. Seventy-six children 1.1–7.7 yrs old (4.5 ⫾ 1.8) (Table 1), ASA I–II, were consecutively included in the study. The children were undergoing different elective surgery (Table 1) and were studied either in the day surgery care unit for children or the neurosurgical postoperative care unit. Children with known development delay and children who received pain relief with continuous infusion of analgesics were excluded. The last group was excluded because they most likely would not develop postoperative pain.
Instruments Behavioural Observational Pain Scale. The BOPS (Fig. 1) was developed in 1996 as a simplified hybrid between two well-known behavioral pain scales, the Princess Margaret Hospital Pain Assessment Tool (16) and the Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS) (12) (Table 2). The BOPS is constructed like the Princess Margaret Hospital Pain Assessment Tool, but this scale is only evaluated for children 7–14 yrs of age and includes five items. We choose the three items with a correlation to pain in this age group of 1–7 yrs of age: facial expression, vocalization, and body position. These items are to be found in both CHEOPS and the Princess Margaret Hospital Pain Assessment Tool. The score in BOPS is derived by assessing three variables indicative for children in pain (facial expression, vocalization, and body movements). Each of these variables was allocated in three grades, 0, 1, or 2, to keep the scale as simple as possible. The sum of these variables in BOPS will be between 0 and 6 points. Based on clinical experience and the way that the score was constructed, a decision was made that scores ⬎2 points should lead to pain relief treatment (i.e., if fear, discomfort, or parent separation could be excluded as obvious reasons). BOPS was used in Swedish during the study.
2
Figure 1. Behavioural Observational Pain Scale (BOPS), which includes the accompanying explanation text. The left column is the score. The next three columns—facial expression, verbalization, and body position—are the items used for the pain evaluation. For translation into Swedish, contact the authors. Table 1. Patients’ characteristics and type of surgery for the three different parts Interrater Reliability (n ⫽ 25)
Concurrent Validity (n ⫽ 26)
Construct Validity (n ⫽ 25)
15 (60) 10 (40) 4.5 ⫾ 2.0
18 (69) 8 (30) 4.5 ⫾ 1.7
17 (68) 8 (32) 4.0 ⫾ 1.6
3 (12) 10 (40) 1 (5) 11 (44)
1 (4) 24 (92) 0 (0) 1 (4)
4 (16) 11 (44) 5 (19) 5 (19)
Male Female Age, yrs Type of surgery Abdomen Ear, nose, or throat Groin, genitals Neurosurgery Ages are given as mean ⫾
SD;
all other values are n (%).
Children’s Hospital of Eastern Ontario Pain Scale. The CHEOPS was developed in 1985 by McGrath et al (12). It is an observation scale for measuring postoperative pain in children aged 1–7 yrs. The scale includes six categories of pain behavior: cry, facial, verbal, torso, touch, and legs. Each category has three or four grades. CHEOPS has a minimum possible score of 4 points (no pain) to a maximum of 13 points (the worst pain). The scale has been tested for both reliability and validity. To use the CHEOPS in Sweden, the scale was first translated to Swedish by a general practitioner and back again to English by an anesthesiologist, as the two were fluent in both languages.
Procedure For the evaluation to commence, several criteria were first met; children had to be easily arousable after anesthesia, they had to be admitted to the postoperative wards, and there had to be a clinical assumption that the child was in pain. The nurses were generally knowledgeable in the use of behavioral observation pain scales, but they received organized
education in the use of the two pain scales, BOPS and CHEOPS. Furthermore, the nurses involved were individually instructed in the use of the CHEOPS and the BOPS immediately preceding their first use of the scales. This training included discussion of the elements, the definition of behavior, and use of the scoring system. The study consisted of three parts to assess the interrater reliability, concurrent validity, and construct validity for the BOPS.
Interrater Reliability In this evaluation we want to show that different persons can make similar observations independently of each other, and in this type of evaluation it is vital to have as many different characters as possible to evaluate. In interrater reliability, two trained observers are watching the event at the same time and independently assessing data according to the instrument instructions. The data can then be used to measure the degree of association between the observers (1). Interrater reliability of BOPS was tested in 25 children. Three observations at 10-min intervals were com-
Pediatr Crit Care Med 2007 Vol. 8, No. 2
Table 2. Princess Margaret Hospital Pain Assessment Tool (PMHPAT) and Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS), the two scales from which the Behavioural Observational Pain Scale (BOPS) is constructed, as a simplification Score
BOPS
Score
PMHPAT
Score
0 1 2
Facial expression Neutral/positive, smiling, composed Negative facial expression and/or concerned Negative facial expression grimace, distorted
0 1 2
Facial expression Face composed/smiling Face distorted Facial grimace
1 2 2 3
0 1 2
0 1 2
Verbalization Normal conversation, laugh, crow Completely quiet or sobbing and/or complaining but not because of pain Crying, screaming, and/or complaining about pain Body position Inactive, lying relaxed with all extremities or sitting, walking Restless movements, shifting fashion, and/ or touching wound or wound area Lying rigid and/or drawn up with arms and legs to the body
0 1 2
Nurses’ assessment No pain/slight pain Moderate pain Severe pain
1 2 0
0 1 2
Position in bed Lying still/relaxed Restless/holding wound Lying rigid/thrashing
1 1 2 2
0
0 1 2
Sounds Normal conversation Whimpering/grizzling/ complaining (not of pain) no sounds Crying loudly/ screaming/complaining of pain
1 2 2 2 2 2
0 1 2
Self-assessment (Wong-Baker faces) Face 0 or 1 Face 2 or 3 Face 4 or 5
Cry No cry: child is not crying Moaning: child is moaning or quietly vocalizing, silent cry Crying: child is crying but the cry is gentle or whimpering Scream: child is in a full-lunged cry; sobbing; may be scored with complaint or without complaint Face Composed: neutral facial expression Grimace: score only if definite negative facial expression Smiling: score only if definite positive facial expression Child verbal None: child is not talking Other complaints: child complains but not about pain, e.g., “I want to see my mommy” or “I am thirsty” Pain complaints: child complains about pain Both complaints: child complains about pain and about other things, e.g., “it hurts” and “I want mommy” Positive: child makes any positive statement or talks about other things without complaints Torso Neutral: body (not limbs) is at rest; torso inactive Shifting: body is in motion in a shifting or serpentine fashion Tense: body is arched or rigid Shivering: body is shuddering or shaking involuntarily Upright: child is in vertical or upright position Restrained: body is restrained Touch
1 2 2 2 2 1
2
2 2
Pediatr Crit Care Med 2007 Vol. 8, No. 2
CHEOPS
Not touching: child is not touching or grabbing at wound Reach: child is reaching for but not touching wound Touch: child is gently touching wound or wound area Grab: child is grabbing vigorously at wound Restrained: child’s arms are restrained Legs Neutral: legs may be in any position but are relaxed; includes gentle swimming or serpentine-like movements Squirming/kicking: definitive uneasy or restless movements in the legs and/or striking out with foot or feet Drawn up/tensed: legs tensed and/or pulled up tightly to body and kept there Standing: standing, crouching, or kneeling Restrained: child’s legs are being held down
3
Construct Validity. Nonparametric tests were used to compare pain scores obtained before and after analgesia, representing construct validity. Friedman was used to distinguish a difference over time, and p ⬍ .05 was considered as significant. Wilcoxon’s signed ranks test with Bonferroni correction was used to compare the effect of analgesic between two intervals of time. We accepted p ⬍ .01 as significant. Values are given as median and IQR. To analyze validity, we used the software SPSS 11.5 for Windows.
RESULTS Interrater Reliability
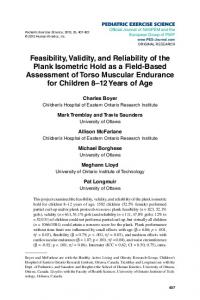
Figure 2. Scatter-plot where the horizontal axis represents Behavioural Observational Pain Scale (BOPS) scores 1– 6 points and the vertical axis represents Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS) scores 4 –13 points. The n represents the amount of observations in the different groups. Each single dot in the figure represents one observation. In the dots with irradiating arms, the sum of arms represents the amounts of observations at this point.
pleted, giving a total of 75 paired observations. At each observation two different nurses, independently of each other, observed the child at the same time and made a BOPS evaluation. To strengthen the interrater reliability test, it is important to have many different persons performing the evaluation. A total of 24 different nurses made the ratings in this part. The nurses did not share or discuss observations or ratings.
travenously, morphine 0.05– 0.1 mg/kg or ketobemidone 0.05 mg/kg (a synthetic morphine with nearly the same potency), was based on the department’s routine pain management. The nurses were instructed to make their own decision when to give pain treatment and to estimate BOPS score immediately before they administered analgesics and at 15, 30, and 60 mins after intravenous medication. The nurses were not blinded to the pain relief medication.
Concurrent Validity In concurrent validity, a new scale and a standard measure are used at the same time to see if they correlate on the present criterion (pain) (1). In the second part of the study, we used CHEOPS as the gold standard or standard measure for testing the concurrent validity to BOPS. Twenty-six children were observed for 30 mins postoperatively with both the BOPS and the CHEOPS, for three consecutive 10-min intervals. CHEOPS scores were done by the investigator, whereas BOPS scores were simultaneously performed independently by another nurse. Each observer was blinded to each other’s observation.
Construct Validity In construct validity, the instrument’s ability to measure the concept of interest (pain) is tested by comparison with external variables related to the construct (1). Twenty-five children were observed before and three times after analgesic administration. The decision to administer further postoperative analgesic in-
4
Statistical Analysis Interrater Reliability. Weighted kappa (w) evaluation was used to determine interrater reliability with the software program Analyze-it ⫹ Clinical Laboratory 1.71. The statistics measure agreement between categorical assessments. The value of w renders a grade as follows: ⬍0.2, poor agreement; 0.21– 0.40, fair agreement; 0.41– 0.60, moderate agreement; 0.61– 0.80, good agreement; and 0.81–1.00, very good agreement (21). Concurrent Validity. The correlation between BOPS and CHEOPS was analyzed with Spearman rank order correlation coefficient (rs). After BOPS was divided into three categories, a cross-tabulation between BOPS and CHEOPS was used to confirm agreement between the scales: no pain (scored 0 –2 points), moderate pain (3– 4 points), and severe pain (5– 6 points). Differences in CHEOPS scores between BOPS categories were analyzed using nonparametric Kruskal-Wallis test with p ⬍ .05 considered statistically significant. Values for CHEOPS are given as median and interquartile range (IQR).
The patient population is described in Table 1. In interrater reliability, 75 paired observations were made by 24 nurses. The interrater reliabilities of the observers were good. There was a high agreement between the different nurses’ BOPS scores. The w value for facial expression was 0.86 (90%), for verbalization 0.92 (93%), and for body position 0.95 (97%), and the total BOPS score was w 0.93 (89%). The figures in parentheses represent the percent agreement.
Concurrent Validity Of 78 possible evaluations, 77 were performed. One scoring was not possible as the child had left the ward earlier than expected. BOPS and CHEOPS scores had positive correlation indicating that both tools described similar behaviors. The correlation between BOPS and CHEOPS was statistically significant (rs ⫽ .871, p ⬍ .001). In the cross-tabulation, BOPS was divided into three categories. In the nopain group, the median score for CHEOPS was 6 (IQR ⫽ 6 – 6); in the moderate pain group 9 (8 –10); and in the severe pain group 11 (11–12) (p ⬍ .001, Kruskal-Wallis test). A high agreement (96.1%) was found when comparing BOPS categories with the CHEOPS 4- to 13-point score (Fig. 2).
Construct Validity Table 3 shows when the nurses decided to give pain relief. Eighty-nine percent of the nurses decided to give pain relief when BOPS was ⬎2 points. The BOPS score before analgesic administration was higher (with a median [IQR] score of 5 [4 – 6]) than BOPS scored 15 mins after analgesic administration (0 [0 –3.5]), 30 mins later (0 [0 –1]), and at 60 mins (0 [0 – 0], p ⬍ .001 by Friedman’s Pediatr Crit Care Med 2007 Vol. 8, No. 2
Table 3. Distribution of the nurses’ pain treatment (n ⫽ 100) listed in occasions
BOPS Score
Occasions, No.
No Pain Relief, No. (%)
Pain Relief, No. (%)
65
64 (98)
1 (2)
14
4 (29)
10 (71)
21
0 (0)
21 (100)
No pain (0–2 points) Moderate pain (3–4 points) Severe pain (5–6 points)
All children with moderate and severe pain received pain treatment except for the four with moderate pain, who received pain treatment 15 mins previously.
test). The differences between the time intervals (Wilcoxon’s signed-rank test) were significant (p ⬍ .01) between before analgesia and at 15 mins, 30 mins, and 60 mins after analgesic administration. There was also significance between 15min and 60-min time intervals (Fig. 3).
DISCUSSION Preschool children may be unable to describe physical discomfort and pain intensity because of a general lack of verbal and cognitive skills (11). Pain treatment must therefore rely on indirect measurements of pain, as there is no accepted determinant in this age group (15). When caregivers estimate pain as well as the effect of pain treatment, the use of any kind of scale is important (1, 15, 18). To this end, the American Academy of Pediatrics (3) recommends that effective pain management in infants and children be monitored routinely and documented clearly in a visible place. This requires assessment of pain intensity and pain relief with reliable, valid, and clinically sensitive assessment tools. Many hospitals use different behavioral scales that are modifications after translations from other languages, but none of them have been validated or tested for reliability (13). Some behavioral observation scales have been reported to be difficult to use. They are lengthy and lack the attributes necessary for easy implementation (14, 15, 22). CHEOPS is one of the first and most well-known scales, but it includes six items with a complicated scoring system from 4 to 13 points. Since then different and simpler pain scales have been developed. There is a growing need for approved and simple pain evaluation instruments that can be incorporated into daily care (2, Pediatr Crit Care Med 2007 Vol. 8, No. 2
Figure 3. Box-and-whisker plot showing change in Behavioural Observational Pain Scale (BOPS) score in response to analgesic administration. The vertical axis represents BOPS score and the horizontal represents time. The horizontal line seen in the box (Before) is the median value; the median value at 15, 30, and 60 mins is zero. Boxes correspond to interquartile ranges and error bars to ranges. Scores were estimated before the administration of analgesic (Before) and 15, 30, and 60 mins after analgesic administration. 䡬 Two outliers at 30 mins; # one outlier with one point and one with two points at 60 mins.
23). With regard to this, we have created BOPS (Fig. 1), which is simple and easy to use in a busy clinical care unit. The scale is in some way like FLACC but simpler, as it consists of three items compared with FLACC’s five items.
the facts that BOPS only evaluates three behaviors, that it had a smaller sum score, and that it was a simpler scale could account for better interrater reliability.
Interrater reliability
Because CHEOPS is so well reputed and has been used in many studies (7–9, 15, 24 –30), we chose it as our gold standard for testing the concurrent validity. CHEOPS was one of the first behavior observational pain scales and has been found to be very good for postoperative pain measurement (12, 19, 26). BOPS and CHEOPS had a high correlation, indicating that BOPS could discriminate pain of different intensity to the same extent. When we compared BOPS with CHEOPS, the agreement between the scales was 96% (Fig. 2). In planning this study, we assumed that children between 5 and 7 yrs old could self-report pain as an extra control to BOPS and CHEOPS using the Coloured Analogue Scale (20). However, most of the children were unable to do so as they were still affected by anesthesia when these tests were performed. Such findings have been published before, and the noted reasons were factors like excitement, agitation, pain, and sedation (6 – 8).
BOPS rating as a whole showed a superior interrater reliability with a value of 0.93. Noting the three items in the scale, one surprising fact was that the best reliability was found in body position. Other pain scales do not have the same high interrater reliability. For example, the values for the ToddlerPreschooler Postoperative Pain Scale with seven individual behavior items were 0.53– 0.78 (17), the five items in the FLACC pain assessment tool were 0.52– 0.82 (14), and the nine items in the COMFORT scale including the three physiologic variables were 0.54 – 0.93 (23). BOPS is a simple hybrid derived from two other behavioral pain scales. If simplification had made the BOPS a more inaccurate instrument, one would expect a lower value. Fewer investigators could be one reason for a better interrater reliability; for example, 39 persons are involved in the COMFORT scale (23). However, only two observers performed the Toddler-Preschooler Postoperative Pain Scale (17), whereas the numbers of investigators involved are not clearly mentioned in the FLACC study (14). Therefore,
Concurrent Validity
Construct Validity If the pain scale in fact measures pain, it should show a lower score after admin5
istration of analgesic. By selecting times when the clinical presumption was that the child was in pain, the nurses could evaluate the response to analgesics. Similar approaches have been used in other comparable studies validating pain measures (12, 15, 19). BOPS was sensitive and the score decreased after pain relief was given. A significant decrease in BOPS was found as early as 15 mins after analgesia administration. The children received their analgesic intravenously, which was the most probable reason for the fast BOPS response. An effect of the analgesic was found in all children with a BOPS score ⬎2, which strengthens our normal recommendation to treat pain when BOPS is ⬎2 points (Table 3). Unfortunately, an unequivocal cutoff point to give pain treatment is not described for our gold standard CHEOPS. A CHEOPS score around 7 points indicates the need for pain treatment in most studies (19, 26, 28 –30). Others wait until 9 points (9, 25, 27) or even ⱖ10 (8). Our study showed that a CHEOPS score between 4 and 7 points was equal to BOPS 0 –2 points, which the cross-tabulation and the agreements (Fig. 2) show. This suggested that a BOPS score ⬎2 should lead to pain treatment. Several factors can influence the nurses’ scoring in a postoperative or intensive care unit. Just before children recover from anesthesia, they can be restless for a limited period of time before they are fully awake (7, 9, 19, 25). Even hunger, fear, and anxiety as well as parental separation can enhance pain scoring in all observational pain scales (4, 8, 13, 25). In this study, nurses were instructed to exclude such reasons for high BOPS scores and try to correct the problem that influenced the measuring. However, the study was hampered by the fact that the nurses performing the BOPS assessment were the same nurses giving the analgesic.
CONCLUSION We found BOPS to be a simple, clear, and easy pain scale to use by caregivers. The simple scoring system could make BOPS easy to incorporate in a busy postoperative unit. With BOPS, the caretaker can evaluate and document pain with a reliable and valid assessment tool and thereby improve pain treatment in preschool children. 6
ACKNOWLEDGMENTS We thank the staff of the day surgery care unit for children and neurosurgical postoperative care unit at the University Hospital of Lund for their assistance. We are grateful to the university lecturer and statistician Per Nyberg for the statistical analysis.
REFERENCES 1. Johnston CC: Psychometric issues in the measurement of pain. In: Measurement of Pain in Infants and Children. Progress in Pain Research and Management. Vol. 10. Finley GA, McGrath J (Eds). Seattle, WA, IASP Press, 1998, pp 5–20 2. Larsson BA: The measurement of paediatric pain. Acta Paediatr 1999; 88:115–119 3. American Academy of Pediatrics & American Pain Society: The assessment and management of acute pain in infants, children and adolescents. Pediatrics 2001; 108:793–797 4. Merkel S, Malviya S: Pediatric pain, tools, and assessment. J Perianesth Nurs 2000; 15: 408 – 414 5. Karling M, Renström M, Ljungman G: Acute and postoperative pain in children: A Swedish nationwide survey. Acta Paediatr 2002; 91:660 – 666 6. Anand KJ, Craig KD: New perspectives on definition of pain. Pain 1996; 67:3– 6 7. Sutters KA, Levine JA, Dibble S, et al: Analgesic efficacy and safety of single-dose intramuscular ketorolac for postoperative pain management in children following tonsillectomy. Pain 1995; 61:145–153 8. Bennie RE, Boehringer LA, Dierdorf SF, et al: Transnasal Butorphanol is effective fore postoperative pain relief in children undergoing myringotomy. Anesthesiology 1998; 89: 385–390 9. Bolton P, Bridge HS, Montgomery CJ, et al: The analgesic efficacy of preoperative high dose (40 mg·kg⫺1) oral acetaminophen after bilateral myringtomy and tube insertion in children. Paediatr Anaesth 2002; 12:29 –35 10. McGrath PJ: Behavioral measures of pain. In: Measurement of Pain in Infants and Children. Progress in Pain Research and Management. Vol. 10. Finley GA, McGrath PJ (Eds). Seattle, WA, IASP Press, 1998, pp 83–102 11. Stevens B: Composite measures of pain. In: Measurement of Pain in Infants and Children. Progress in Pain Research and Management. Vol. 10. Finley GA, McGrath PJ (Eds). Seattle, WA, IASP Press, 1998, pp 161–178 12. McGrath PJ, Johnson G, Goodman JT, et al: CHEOPS: A behavioral scale for rating postoperative pain in children. In: Advances in Pain Research and Therapy. Vol. 9. Fields HL. Dubner R, Cervero F (Eds). New York, Raven Press, 1985, pp 395– 402
13. Jylli L: Smärta hos barn och ungdo mar. In: Smärtbedöming och smärtskattning. Olsson GL, Jylli L (Eds). Lund, Studentlitteratur, 2001, pp 119 –140 14. Merkel S, Voepel-Lewis T, Shayevitz JR, et al: The FLACC: A behavioural scale for scoring postoperative pain in young children. Pediatr Nurs 1997; 23:293–797 15. Tyler DC, Tu A, Douthit J, et al: Toward validation of pain measurement tools for children: A pilot study. Pain 1993; 5:301–309 16. Robertson J: Pediatric pain assessment: Validation of multidimensional tool. Pediatr Nurs 1993; 19:209 –213 17. Tarbell SE, Cohen IT, Marsh JL: The toddlerpreschooler postoperative pain scale: An observational scale for measuring postoperative pain in children aged 1–5. Preliminary report. Pain 1992; 50:273–280 18. Schade JG, Joyce BA, Gerkensmeyer J, et al: Comparison of three preverbal scales for postoperative pain assessment in a diverse pediatric sample. J Pain Symptom Manage 1996; 12: 348 –359 19. Suraseranivongse S, Santawat K, Kraip rasit S, et al: Cross-validation of composite pain scale for preschool children within 24 hours of surgery. Br J Anaesthesia 2001; 87: 400 – 405 20. McGrath PA, Seifert CE, Speechley KN, et al: A new analogue scale for assessing children’s pain: An initial validation study. Pain 1996; 64:435– 443 21. Altman DG: Some common problems in medical research. In: Practical Statistics for Medical Research. Altman DG (Ed). London, Chapman & Hall, 1991, pp 404 – 408 22. Voepel-Lewis T, Merkel S, Tait AR, et al: The reliability and validity of the face, legs, activity, cry, consolability observational tool as a measure of pain in children with cognitive impairment. Anesth Analg 2002; 95: 1224 –1229 23. van Dijk M, de Boer JB, Koot HM, et al: The reliability and validity of the COMFORT scale as a postoperative pain instrument in 0 to 3-years-old infants. Pain 2000; 84:367–377 24. Rose JB, Cuy R, Cohen DE, et al: Preoperative oral Dextromethorphan does not reduce pain or analgesic consumption in children after adenotonsillectomy. Anesth Analg 1999; 88:749 –753 25. Bridge H, Montgomery C, Kennedy R, et al: Analgesic efficacy of ketorolac 0.5% ophthalmic solution (Accular) in paediatric strabismus surgery. Paediatr Anaesth 2000; 10: 521–526 26. McCarty EC, Mencio GA, Anderson Walker L, et al: Ketamine sedation for the reduction of children’s fractures in emergency department. J Bone Joint Surg Am 2000; 82: 912–918 27. de Negri P, Ivani C, Visconti C, et al: How to prolong postoperative analgesia after caudal
Pediatr Crit Care Med 2007 Vol. 8, No. 2
anaesthesia with ropivacaine in children: Sketamin versus clonidine. Paediatr Anaesth 2001; 11:679 – 683 28. Özbek H, Bilen A, Özcengiz D, et al: The comparison of caudal ketamine, alfentanil and ketamine plus alfentanil administration
Pediatr Crit Care Med 2007 Vol. 8, No. 2
for postoperative analgesia in children. Paediatr Anaesth 2002; 12:610 – 616 29. Suraseranivongse S, Chowvanayotin S, Pirayavaraporn S, et al: Effect of bupivacaine with epinephrine wound instillation for pain relief after pediatric inguinal herniorrhaphy
and hydrocelectomy. Reg Anesth Pain Med 2003; 28:24 –28 30. Tay CLM, Tan S: Diclofenac or paracetamol for analgesia in paediatric myringotomy outpatients. Anesth Intensive Care 2002; 30: 55–59
7