ORIGINAL ARTICLE
Verification of the Reliability of the Three-dimensional Virtual Presurgical Orthodontic Diagnostic Protocol Giampietro Farronato, MD, DDS, Lucia Giannini, DDS, Guido Galbiati, DDS, Lucia Pisani, DDS, Carmen Mortellaro, MD, and Cinzia Maspero, MD, DDS Abstract: The precision of presurgical orthodontic diagnostic protocol plays a key role for the success of orthognathic surgery. Recently, the introduction of cone beam computed tomography and the development of digital technologies led to the possibility to create new virtual protocols of diagnostic protocol. The purposes of this study were to describe the virtual presurgical orthodontic diagnostic protocol experimented by the Orthodontics Department of the University of Milan and to assess its reliability by comparing it with the nonvirtual protocol. The study sample was a group of 18 adult patients who required surgical correction of skeletal asymmetric class II or III malocclusion: 9 of them were subjected to the virtual diagnostic protocol, whereas the other 9 were subjected to the traditional one. A comparison between the 2 methods was carried out by evaluating the degree of the discrepancy between setup and presurgical models in both groups. The values of maximum positive deviation, maximum negative deviation, mean deviation, and standard deviation that characterize the points of the superimpositions were considered. An optimal superimposition (>75%) between the scanning of the setup and presurgical models was obtained for all subjects except for 2 patients with asymmetry. The analysis of the punctual deviation variables did not show statistically significant differences between the techniques. The study suggested a high precision for both diagnostic protocols, and the reliability of the 2 methods is comparable. However, the virtual protocol has several advantages such as quantity of information obtainable, repeatability, and speed of execution. Key Words: Orthodontics, orthognathic surgery, orthodontic diagnostic protocol, CBCT, three-dimensional (J Craniofac Surg 2014;25: 2013–2016)
O
rthodontic-surgical treatment is indicated in patients who are at the end of growth and present with a three-dimensional position of the bone bases incompatible with the oral functions or severe malocclusions, which are uncorrectable with mere orthodontic compensation.1 From the Department of Orthodontics, Fondazione IRCCS Cà GrandaOspedale Maggiore Policlinico, University of Milan, Milan, Italy. Received December 20, 2013. Accepted for publication April 20, 2014. Address correspondence and reprint requests to Giampietro Farronato, MD, DDS, Università di Milano, Via Commenda 10, 20100 Milano; E-mail:
[email protected] The authors report no conflicts of interest. Copyright © 2014 by Mutaz B. Habal, MD ISSN: 1049-2275 DOI: 10.1097/SCS.0000000000001046
A careful diagnostic protocol is required to simulate surgical displacements and to predict orthodontic movements necessary before the surgery verifying their feasibility.2,3 This will allow the obtainment of the best aesthetic and functional results after the intervention with a minimum discomfort for the patient and a shorter postsurgical orthodontic phase. The Orthodontics Department of the University of Milan developed a diagnostic protocol that implied the simulation of surgical displacements on radiographs using templates on acetate papers, model surgery on a semiadjustable articulator, and orthodontic setup. An occlusal splint was used as a guide for the presurgical preparation to avoid detecting other diagnostic records.4,5 In the last decade, the development of digital technologies revolutionized both the clinical approach and the diagnostic approach in dentistry. The introduction of cone beam computed tomography (CBCT) provides real three-dimensional cranial reconstructions free from overlap and projection errors.6–8 Thanks to the Computer-Aided Design/Computer-Aided Manufacturing (CAD-CAM) technology, it is now possible to design and implement orthodontic and prosthetic devices in a totally computerized way.9–11 The integration of these 2 methods leads to the possibility of digitalizing the diagnostic protocol for surgical-orthodontic treatment.12 The purpose of this study was to confirm the validity of the virtual presurgical orthodontic diagnostic protocol used at the Orthodontics Department of the University of Milan by comparing its reliability with the nonvirtual protocol. The comparison was made by evaluating the degree of discrepancy between the situation envisaged by the presurgical orthodontic diagnostic protocol and the cast model obtained immediately before surgery in both groups. In addition, we have assessed the advantages derived from the use of digital technology in the diagnostic protocol phase of the treatment.
MATERIALS AND METHODS The study involved 18 patients referred for orthognathic surgery treatment at the Orthodontics Department of the University of Milan. These were placed in 2 groups: group A and group B. Group A involved 9 patients on which the orthodontic presurgical diagnostic protocol was performed in accordance with a virtual protocol. Group B involved 9 patients subjected to a nonvirtual diagnostic protocol (Table 1).
Three-dimensional Virtual Orthodontic-Surgical Diagnostic Protocol The three-dimensional virtual orthodontic-surgical diagnostic protocol developed and tested by the School of Milan involves the following steps: -Precision impression with polyvinyl siloxane. -Recording of the reference aligner: it is a particular wax with spherical radiopaque landmarks (Fig. 1) that will subsequently be worn by the patient during the execution of CBCT and interposed between
The Journal of Craniofacial Surgery • Volume 25, Number 6, November 2014
Copyright © 2014 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
2013
The Journal of Craniofacial Surgery • Volume 25, Number 6, November 2014
Farronato et al
TABLE 1. Illustrative Table of the Sample Considered by the Study Virtual Planning
Nonvirtual Planning
5 4 9
5 4 9
Males (10) Females (8) Total (18)
the arches of the plaster model during its digitization. The landmarks will allow a precise overlapping of the 2 diagnostic records. -Cone beam computed tomography with landmarks and threedimensional cephalometric analysis: the patient is subjected to CBCT wearing the reference aligner. Special software is used to evaluate the craniofacial structures according to the three-dimensional cephalometric examination proposed by the School of Milan.13–15 -Digitization of plaster casts: via the use of a specific scanner, it is possible to obtain three-dimensional digital images of plaster casts in .stl format.11 The arches are digitized in the proper relationship by placing the reference aligner between them. Subsequently, individual dental elements are scanned separately. Because wax reflects light, unlike plaster that absorbs it, it will not be captured by the camera; hence, it will not be visible in the digital model. -Virtual orthodontic-surgical visual treatment objective: the stl files of digital models and CBCT are imported into CAD software CATIA. The software recognizes the radiopaque landmarks allowing the superimposition of three-dimensional images of the arches with digital imaging and communications in medicine files of CBCT. It is now possible to merge the skeletal and dental structures into a single volumetric rendering for the diagnostic protocol of surgical displacements (Fig. 2). Powerful segmentation tools of the software separate the maxillofacial complex from the jaw, creating 2 distinct images that can be moved. In this way, it is possible to determine and measure the displacements of the bone bases necessary for the correction of the malocclusion. -Virtual orthodontic setup: diagnostic protocol of orthodontic movements allows the achievement of an optimal occlusion at the end of treatment. The software performs the segmentation of the teeth and replaces them in the correct relation. This procedure can be automatic or controlled by the operator who can simulate the orthodontic treatment varying torque and tip as well as rotations and dental movements with a three-dimensioal vision of the dentoalveolar relationships. A patented system based on the Ricketts arches allows the software to align teeth according to the more appropriate dental arch for the patient's biotype. This makes the procedure standardized and reproducible.16 -Realization of presurgical templates: the CAD-CAM techniques allow the realization of presurgical occlusal templates to check the quality and the progression of presurgical orthodontic treatment. They have to be worn by the patient at each session. Once they perfectly fit, the objectives set in the diagnostic protocol can be considered achieved. At the end of the presurgical orthodontic preparation, impressions had to be taken for each patient. Presurgical plaster casts and models relating to the group B’s diagnostic protocols were digitized using a structured light threedimensional scanner (Maestro 3D Dental Scanner by Age Solutions).
FIGURE 1. The reference aligner.
2014
FIGURE 2. The reference aligner allows to match digitized models with CBCT.
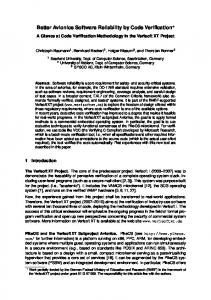
The scanner captures the positions of the different points of the models, providing highly accurate three-dimensional digital images. Group A’s diagnostic protocols were already filed in the computer in digital format. Digital images were acquired in the software CATIA and cropped selecting only occlusal, lingual, and palatal surfaces because the brackets in presurgical records would have resulted in a big difference on the vestibular surface of the models. It was therefore possible to perform the superimposition between models and respective presurgical setup for each group. A best-fit algorithm was used to find the position of the arches in space for which the sum of the discrepancies was the shortest. A punctual variation colorimetric map indicating percentages of areas subjected to different discrepancies was used to evaluate the degree of congruence between the 2 models (Fig. 3). Furthermore, for each arch, the software provided metric values of maximum positive deviation, maximum negative deviation, mean deviation, and standard deviation that characterize the points compared in the superimposition.
RESULTS For all patients, an overlap of greater than 75% (range, ±1 mm) between the diagnostic protocol and the presurgical model was obtained, except for 2 patients with asymmetry. Data provided by the software related to the patients of the 2 groups were placed in 2 separate tables and subdivided according to the considered arch (Tables 2 and 3). Because the distribution of the data did not present normal type, a nonparametric test with a degree of reliability of 95% (Wilcoxon-Mann–Whitney rank sum test) was performed for each variable to determine whether the difference between the values observed for the 2 protocols was statistically significant. For each variable, the P value for the hypothesis test was calculated (Table 4). The same test was applied, taking account also of the considered arch (Table 5).
DISCUSSION Both diagnostic protocols showed high reliability. Presurgical templates allow the orthodontist to more easily achieve the objectives set in the diagnostic phase.
FIGURE 3. The color scale represents the degree of discrepancy between presurgical situation and setup.
© 2014 Mutaz B. Habal, MD
Copyright © 2014 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
The Journal of Craniofacial Surgery • Volume 25, Number 6, November 2014
TABLE 2. Values for Each Arch of the Group Subjected to the Virtual Presurgical Planning ID
PosMaxDev, mm
NegMaxDev, mm
Mean Dev, mm
TABLE 4. P Values Derived From the Comparison of the Punctual Deviation Values of the 2 Groups (Student t test) SD, mm
Pz Pz Pz Pz Pz Pz Pz Pz
2 3 4 5 6 7 8 9
0.9999 4.9999 0.8645 3.8706 6.4189 6.1597 3.5404 5.1743 5.6770
−0.9997 −4.9999 −1.9857 −4.3066 −6.9841 −6.1289 −5.6395 −5.3023 −6.9597
0.1506 0.0158 0.043 −0.0506 0.2558 −0.48 −0.0152 −0.3172 −0.69441
0.4967 1.778 0.0349 0.9081 0.8922 1.0365 0.8450 12120 1.2386
0.9987 4.8815 4.9965 4.7712 7.1743 2.2765 4.6162 3.4200 4.0198
−0.9985 −3.4768 −4.9998 −4.7726 −9.27539 −4.5369 −6.5734 −3.4927 −5.0228
0.05 0.4953 0.0612 −0.1552 0.1703 −0.1506 0.4586 −0.1127 −0.1265
0.4309 1.2801 1.6641 1.1057 1.0984 0.6659 0.8767 0.7475 0.7986
Lower arch Pz Pz Pz Pz Pz Pz Pz Pz Pz
1 2 3 4 5 6 7 8 9
POSMAXDEV, positive maximum deviation; NEGMAXDEV, negative maximum deviation; MEANDEV, mean deviation; ID, identification; Pz, patient.
The unprecise overlap that occurred for the 2 patients is attributable to an important asymmetry that resulted in neuromuscular influence on orthodontic movements.17–21 The analysis of results, independently from the considered arch, shows that the discrepancies reported for the virtual diagnostic protocol are, on average, lower than those obtained in the group receiving the nonvirtual diagnostic protocol.
TABLE 3. Values for Each Arch of the Group Subjected to the Traditional Presurgical Planning ID
PosMaxDev, mm
NegMaxDev, mm
Mean Dev, mm
SD, mm
4.991 3.5799 4.9958 4.5182 4.1146 3.0915 3.5303 3.4919 4.0612
−4.999 −3.5795 −4.9999 −2.5513 −3.1088 −2.4294 −1.8071 −3.5315 −4.4305
0.2139 −0.138 −0.1084 0.5746 −0.2101 0.0493 1.0164 2.548 0.0953
1.3411 0.9713 1.6733 1.1333 0.458 0.7505 0.7432 0.9028 0.8842
4.9945 4.9907 2.4112 3.4453 3.65186 4.2897 2.7392 6.0683 5.5906
−4.9956 −4.9956 −2.5755 −3.3041 −2.59007 −2.7601 −3.0097 −5.8490 −4.0417
0.3224 −0.2268 −0.0707 0.2668 0.1430 0.1215 0.1352 −0.0700 0.7043
1.0735 1.1477 0.6659 1.0825 0.59583 0.8862 0.6972 1.3853 1.1508
Upper arch Pz 10 Pz Pz Pz Pz Pz Pz Pz Pz
11 12 13 14 15 16 17 18
Lower arch Pz Pz Pz Pz Pz Pz Pz Pz Pz
10 11 12 13 14 15 16 17 18
P
Variable PosMaxDev
Upper arch Pz 1
Orthodontic Diagnostic Protocol
0.51 0.08 0.10 0.97
NegMaxDev MeanDev SD
However, the differences between the values of the variables related to the 2 study groups are not statistically significant (P > 0.05). It can be observed that, although the average values of the discrepancies for the 2 protocols are in the range of 1 mm, maximum positive deviation and maximum negative deviation of up to 7 mm were detected. This result is explained by the fact that, regardless of the protocol used, not all tooth surfaces can be accurately reproduced from dental impression. In fact, the points or areas of contact may be inaccessible to the impression material. These critical areas are reconstructed arbitrarily manually or through dedicated software during the orthodontic setup. Moreover, orthodontic movements are complex and absolutely different for each case in terms of quality and with regard to the dental elements to which they were applied. It is evident that the orthodontic movement on the incisors is easier compared with the molars because of their greater resistance. For this reason, regardless of the protocol, an optimistic diagnostic protocol of posterior expansion that is not reflected at the end of presurgical phase is shown (Fig. 4). It should also be considered that, in all the examined patients, orthodontic movements were performed through the application of standardized attacks and progressive arches. This, however, does not allow the transfer of the information of movements established in the virtual simulation, which would be permitted by the implementation of individualized appliances realized on the diagnostic protocol models. The reliability of the 2 methods can therefore be considered comparable. However, thanks to the digital method, the following actions are possible: • to eliminate some laboratory steps and reduce the operating time and errors associated to manual procedures because the detection of the face bow and the mounting on the articulator are not necessary. All data can be derived from the integration of the CBCT and the scanning of the models, • to have a vision of the patient’s entire skull, • to transmit information to the patient in a simple and immediate way with a strong communicative effect, • to perform a faster and more repeatable setup because the procedure is standardized and the teeth are moved with completely measurable parameters and values, • to design, on the basis of the digital setup, a completely preprogrammed and individualized appliance able to fulfill a specific TABLE 5. P Values Derived from the Comparison of the Punctual Deviation Values of the 2 Groups Regarding the Considered Arch (Student t test) Variable PosMaxDev NegMaxDev MeanDev SD
P (Upper Arch)
P (Lower Arch)
0.33 0.2 0.13 0.79
0.79 0.21 0.47 0.96
© 2014 Mutaz B. Habal, MD
Copyright © 2014 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
2015
The Journal of Craniofacial Surgery • Volume 25, Number 6, November 2014
Farronato et al
FIGURE 4. In this case, the amount of expansion planned was possible to obtain.
movement from a position A to a position B; the CAD-CAM technology allows to design brackets with specific shapes as well as positions information according to the needs of the clinician and the characteristics of the individual dental element. These appliances allow to reach the predetermined position in the shortest time and with minimum discomfort to the patient, making the presurgical orthodontic phase shorter as well as more effective and efficient.22,23
Scientific research is focused on the implementation of the system through the development of intraoral scanners able to detect three-dimensional dental impressions. This will be able to replace conventional impression-detecting procedure and plaster casts realization, which can be subject to several operator-dependent errors.1,23 The reliability and validity of the measurements made on the virtual models obtained from intraoral scans have been demonstrated by several studies.24–27 The introduction of digital study models in daily practice allows the transmission of traditional plaster-cast archives in virtual models archives where the documentation of every single patient is more easily found and cataloged. This results in a significant reduction in the storage space, which becomes a virtual one on a hard disk. Because of the possibility of sending data through the Web, the dentist and the dental technician are able to exchange information in a more simple, inexpensive, and immediate way, with an important benefit in the management of a modern dental practice.28 It is therefore evident how these new technologies represent a revolution in terms of method, materials, costs, efficiency, and execution time, which can bring numerous advantages to both the clinician and the patient.
CONCLUSIONS Traditional orthodontic-surgical diagnostic protocol requires several laboratory steps that inevitably introduce uncorrectable errors and lead to an imprecise final result. The virtual diagnostic protocol experienced by the Orthodontics Department of the University of Milan implies the creation of digital three-dimensional models and their integration with the CBCT to perform a totally computerized simulation of surgery and definition of presurgical orthodontic objectives. The study suggests that the reliability of the 2 protocols is comparable, but digital procedures and CAD-CAM technologies imply important advantages regarding the amount of information obtainable, the reduction of the times and errors related to the laboratory phases, as well as the reproducibility of the diagnostic protocol.
REFERENCES 1. Pasciuti E, Franchi L, Baccetti T, et al. Comparison of three methods to assess individual skeletal maturity. J Orofac Orthop 2013;74:397–408
2016
2. Farronato G, Giannini L, Galbiati G, et al. Long term results of open reduction management of condylar fracture: a 20 years follow-up. Case report. Minerva Stomatol 2012;61:457–465 3. Farronato G, Maspero C, Paini L, et al. Sistematica di programmazione ortodontica-pre chirurgica. Mondo Ortodontico 2004;3:197–202 4. Farronato G, Maspero C, Giannini L, et al. Occlusal splint guides for presurgical orthodontic treatment. J Clin Orthod 2008;42:508–512 5. Farronato G, Giannini L, Galbiati G, et al. Presurgical orthodontic diagnostic protocol: predictability. J Craniofac Surg 2013;24:1–3 6. Van Vlijmen OJ, Bergè SJ, Swennen GR, et al. Comparison of cephalometric radiographs obtained from cone beam computer tomography scans and conventional radiographs. J Oral Maxillofac Surg 2009;67:92–97 7. Cattaneo PM, Melsen B. The use of cone-beam computed tomography in an orthodontic department in between research and daily clinic. World J Orthod 2008;9:269–282 8. Dominici AD, De Nardi S, Luini G, et al. Analisi cefalometrica 3D dei “10 punti” con T.C. Cone Beam a basso dosaggio. Dent Mod 2008;12:42–50 9. Duret F, Blouin JL, Duret B. CAD-CAM in dentistry. J Am Dent Assoc 1998;117:715–720 10. Liu PR, Essig ME. Panorama of dental CAD/CAM restorative systems. Compend Contin Educ Dent 2008;29:486–488 11. Mehl A, Hickel R. A new optical 3D-scanning system for CAD/CAM technology. Int J Comput Dent 1999;2:129–136 12. Farronato G. Ortognatodonzia. Vol. 1. Milan: Edi.Ermes, 2013. 13. Farronato G, Farronato D, Toma L, et al. A synthetic three-dimensional craniofacial analysis. J Clin Orthod 2010;44:673–679 14. Farronato G, Garagiola U, Dominici A, et al. “Ten-point” 3D cephalometric analysis using low-dosage cone beam computed tomography. Prog Orthod 2010;11:2–12 15. Matarese G, Portelli M, Mazza M, et al. Evaluation of skin dose in a low dose spiral CT protocol. Eur J Paediatr Dent 2006;7:77–80 16. Maver G, Magni A. La moderna progettazione. Dent Dialogue 2013;2:88–104 17. Giannini L, Maspero C, Batia C, et al. Valutazione elettromiografica ed elettrognatografica del trattamento ortodontico-chirurgico. Mondo Ortod 2011;36:12–28 18. Farronato G, Giannini L, Galbiati G, et al. Orthodontic-surgical treatment: neuromuscular evaluation in skeletal class II and class III patients. Prog Orthod 2012;13:226–236 19. Farronato G, Giannini L, Galbiati G, et al. Orthodontic-surgical treatment: neuromuscular evaluation in open and deep skeletal bite patients. Prog Orthod 2013;14:41 20. Nucci P, Farronato G, Serafino M, et al. Restrictive strabismus after blow-out orbital fracture in children: is the muscle involved? J Trauma 2004;56:209–210 21. Farronato G, Giannini L, Grillo E, et al. Occlus-O-Guide vs Andresen activator appliances: neuromuscular evaluation. Prog Orthod 2013;14:4 22. Mandolesi F, Duranti G, Raffaelli R. Modelli 3D digitali e ortodonzia assistita da computer. Ortodonzia tecnica 2005;1:13–18 23. Weber DJ 2nd, Koroluk LD, Phillips C, et al. Clinical effectiveness and efficiency of customized vs conventional preadjusted bracket systems. J Clin Orthod 2013;47:261–266 24. Pieper R. Digital impressions—easier than ever. Int J Comput Dent 2009;12:47–52 25. Ender A, Mehl A. Full arch scans: conventional versus digital impressions—an in-vitro study. Int J Comput Dent 2011;14:11–21 26. Kim SY, Kim MJ, Han JS, et al. Accuracy of dies captured by an intraoral digital impression system using parallel confocal imaging. Int J Prosthodont 2013;26:161–163 27. Wiranto MG, Engelbrecht WP, Tutein Nolthenius HE, et al. Validity, reliability, and reproducibility of linear measurements on digital models obtained from intraoral and cone-beam computed tomography scans of alginate impressions. Am J Orthod Dentofacial Orthop 2013;143:140–147 28. Garino F, Garino GB. Digital treatment objectives: procedure and clinical application. Prog Orthod 2004;5:248–256
© 2014 Mutaz B. Habal, MD
Copyright © 2014 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.