213
Journal of Alzheimer’s Disease 40 (2014) 213–220 DOI 10.3233/JAD-131766 IOS Press
Widespread Alterations in Functional Brain Network Architecture in Amnestic Mild Cognitive Impairment Ludovico Minatia,b,∗,1 , Dennis Chana,1 , Chiara Mastropasquac,d , Laura Serrac , Barbara Span`oc , Camillo Marrae , Carlo Caltagironef,g , Mara Cercignania,c and Marco Bozzalic a Clinical
Imaging Sciences Centre, Brighton and Sussex Medical School, Falmer, UK Department, Fondazione IRCCS Istituto Neurologico Carlo Besta, Milano, Italy c Neuroimaging Laboratory, Fondazione IRCCS Santa Lucia, Rome, Italy d Neuroscience Department, University of Trieste, Trieste, Italy e Institute of Neurology, Universit´ a Cattolica, Rome, Italy f Clinical and Behavioural Neurology, Fondazione IRCCS Santa Lucia, Rome, Italy g Department of Neuroscience, University of Rome “Tor Vergata”, Rome, Italy b Scientific
Accepted 12 November 2013
Abstract. We investigated changes in functional network architecture in amnestic mild cognitive impairment using graphbased analysis of task-free functional magnetic resonance imaging and fine cortical parcellation. Widespread disconnection was observed primarily in cortical hubs known to manifest early Alzheimer’s disease pathology, namely precuneus, parietal lobules, supramarginal and angular gyri, and cuneus, with additional involvement of subcortical regions, sensorimotor cortex and insula. The connectivity changes determined using graph-based analysis significantly exceed those detected using independent component analysis both in amplitude and topographical extent, and are largely decoupled from the presence of overt atrophy. This superior ability of graph-based analysis to detect disease-related disconnection highlights its potential use in the determination of biomarkers of early dementia. Graph-based analysis source code is provided as supplementary material. Keywords: Amnestic mild cognitive impairment (aMCI), functional connectivity, graph theory, prodromal Alzheimer’s disease, resting-state functional MRI
INTRODUCTION Impairment of brain function precedes the onset of atrophy in Alzheimer’s disease (AD). As such, there is increasing interest in the use of functional magnetic resonance imaging (fMRI) to detect alterations of brain function in prodromal AD. Studies of functional connectivity in mild cognitive impairment (MCI), investigated using independent-component analysis ∗ Correspondence
to: Ludovico Minati, Clinical Imaging Sciences Centre (CISC) Brighton & Sussex Medical School, Southern Ring Road, Falmer BN1 9RR, UK. Tel.: +39 335 486670; +44 784 960 3287; E-mails:
[email protected];
[email protected]. 1 These authors contributed equally to the study.
(ICA) or seed-based analysis (SBA) of task-free fMRI, have demonstrated disconnection across the default mode network (DMN), primarily in precuneus and posterior cingulate cortex. However, the low amplitude and limited topographical extent of these changes restricts the potential usage of these approaches in studies aimed at determining biomarkers of early AD [1, 2]. These issues arise as a consequence of theoretical limitations inherent in ICA and SBA which impact on their ability to detect disease effects. By segregating brain connectivity into separate “components” assumed to be independent of one another, ICA and SBA are unable to identify key architectural properties
ISSN 1387-2877/14/$27.50 © 2014 – IOS Press and the authors. All rights reserved
214
L. Minati et al. / Functional Networks in Amnestic Mild Cognitive Impairment
of functional brain networks, such as small-worldness (the optimal balance between local connection clustering and interregional information-transfer efficiency) and presence of “cortical hubs”, representing highlyinterconnected regions that are central to whole-brain connectivity and that in AD are associated with early accumulation of amyloid pathology [3–7]. Instead, network architecture can be evaluated using models based on graph theory, which represent connectivity as structured sets of functional associations between brain regions (nodes), thus generating maps of connection density (node degree). This approach also permits computation of parameters of global network integrity such as completeness (overall proportion of observed connections), average clustering coefficient (aggregation of connections in tightly-interconnected neighborhoods) and global efficiency (reciprocal of the number of nodes traversed in transferring information across the network) [5–8]. There is converging evidence that graph-based network analyses are highly relevant to the study of AD and may improve the differentiation between patients and controls with respect to ICA and SBA. Recent reports have suggested that measurement of network architecture parameters can substantially improve detection of disease-related changes, and progression of pathology may itself be determined by brain network architecture [3–6]. However, an explicit comparison between ICA and graph-base analysis remains to be conducted. This issue was addressed in the current study by undertaking a cross-sectional comparison of graph-based analysis and ICA of task-free fMRI in patients with amnestic MCI (aMCI) [9] at high risk of developing AD. METHODS Study population Forty-nine patients with a diagnosis of aMCI were recruited from the Specialist Dementia Clinic of Catholic University of Rome and investigated at the IRCCS Santa Lucia Foundation, Rome. Details are as follows: 25 female, aged 70.2 ± 8.7 years, mean MMSE score 26.4 ± 1.8, Clinical Dementia Rating 0.5, Rey auditory verbal learning test corrected scores 31 ± 6 immediate, 4.6 ± 2.4 delayed, 26 single-domain and 23 multiple-domain. At one year follow-up, 13/34 aMCI patients had converted to AD. The control group comprised 32 cognitively normal participants, 14 female, age 65.9 ± 8.0 years, mean MMSE score 30 ± 0. Approval from the ethics committee of the
Santa Lucia Foundation was obtained. All participants gave written informed consent and the study was conducted in accord with the ethical principles of the Helsinki Declaration. Data acquisition Task-free fMRI was performed on a 3.0 T Siemens Allegra scanner using a gradient-echo echo-planar sequence (TR = 2,080 ms, TE = 30 ms, matrix 64 × 64, voxel size 3 × 3 mm2 , 2.5 mm slice thickness, no gap, flip angle 70◦ , 32 axial slices, 216 volumes). The median volume-to-volume head displacement during this sequence was comparable between patients and controls (0.08 ± 0.05 mm versus 0.09 ± 0.07 mm, p = 0.6). The temporal signal-to-noise ratio (tSNR), measured on the raw time-series in the deep white matter as mean signal divided by standard deviation after linear detrending, was 53 ± 10 in patients and 52 ± 11 in controls (p = 0.9). Dual-echo turbo spin echo, fastFLAIR scans and volumetric T1 scans were acquired (TR = 1,338 ms, TE = 2.4 ms, matrix 256 × 224 × 176, voxel size 1 mm3 isotropic). Structural scans were assessed by a neuroradiologist to exclude additional pathology. Connectivity analysis fMRI data preprocessing was performed using SPM8 (Wellcome Trust Centre for NeuroImaging, London, UK), followed by graph analysis as previously described [10]. In brief, slice-timing correction, realignment/unwarping and normalization were performed, then segmented grey matter maps were averaged across all participants. The brain with smallest squared difference from average was chosen and iteratively parcellated at high resolution, yielding 742 regions with volume 1.55 ± 0.33 ml. These were overlaid to each participant’s anatomy assigning each grey matter voxel to the nearest region, intrinsically removing potential atrophy-related confounds. Resulting masks were used to extract the blood oxygen level-dependent (BOLD) signal, which was de-spiked, de-trended with a 4th degree polynomial, low-pass filtered at f-3dB = 0.12 Hz and filtered by regressing out movement vectors, average white matter and cerebrospinal fluid signal. All nuisance time-series were temporally filtered with the same settings as the BOLD data prior to regression. The processing workflow is shown in Supplementary Figure 1 and implemented in the attached MatLab script. Inter-regional connectivity was determined through pair-wise linear regressions;
L. Minati et al. / Functional Networks in Amnestic Mild Cognitive Impairment
resulting Pearson coefficients were thresholded for |r|>0.15, 0.2 . . . 0.75 and node degrees calculated. Network completeness, clustering coefficient, and global network efficiency were also computed [8]. Additional equi-completeness analyses were performed, thresholding Pearson coefficients with individuallydetermined values yielding fixed completeness across all participants; such analyses were conducted for 13 completeness levels, corresponding to the average completeness across all patients and controls observed at each r-level threshold in the fixed r-value analyses (Fig. 1a). For comparison, we also performed grouplevel spatial ICA, using the Group ICA Toolbox v. 2.0e (University of New Mexico, USA) assuming 12 components as given by the minimum description length criterion and using the same temporal filtering settings. Voxel-based morphometry was performed using the VBM8 toolkit of SPM8 [2]. Statistical analysis After co-varying for age and median volume-tovolume head displacement, global network parameters were compared between aMCI patients and controls using two-tailed t-tests, with false-discovery rate (FDR) correction over the 13 correlation thresholds. Individual node degree maps were smoothed, averaging between each region and its neighbors with a factor of 0.75; subsequently, the number of regions for which node degree was significantly reduced in patients was calculated for all thresholds using two-tailed ttests, with FDR correction over the 742 regions. The threshold yielding the largest difference, |r|>0.60 (see results), was selected for generation of the presented maps, shown at pFDR < 0.05. To facilitate comparison with previous studies using the more coarsely parcellated Automated Anatomical Labeling (AAL) atlas, node degrees were also averaged over the 90 AAL regions and compared using analyses of variance. Outlier rejection was performed for >3 SD. Statistical analysis of ICA and voxel-based morphometry (VBM) maps was performed using SPM8, co-varying for age and median volume-to-volume head displacement. For each ICA component, an inclusive mask was determined by thresholding the main effect over all participants at pFWE < 0.05; subsequently, patients and controls were compared applying a voxellevel threshold of p < 0.005, followed by a corrected cluster level inference threshold of pFWE < 0.05. The DMN component was identified by visual inspection of the main effect maps with reference to established topographical maps [1], upon agreement of three
215
observers. To exclude potential confounding effects related to smoothing scale, ICA was repeated after smoothing the functional images with a Gaussian kernel having FWHM 20 mm, which corresponded to the FWHM of the distribution of voxel counts for a ROI with its neighbors, 20.3 ± 5.3 mm. VBM results are presented for p < 0.05; this extremely permissive voxel-level threshold was deliberately chosen to determine whether VBM would reveal any atrophy in areas of significant disconnection. As for ICA, the presence of significant difference was inferred at the cluster level, applying a corrected cluster threshold of pFWE < 0.05. Receiver operating characteristic (ROC) curves for discrimination between aMCI patients and controls were calculated for regional and global parameters. Regional connectivity, intended as average node degree and ICA z-score, was measured over the precuneus and posterior cingulate region, which forms the core of the DMN [1]; to avoid circularity, this region was identified on the AAL atlas, without any reference to the topographic maps of connectivity differences between patients and controls. Global DMN connectivity was measured by averaging the ICA z-score over the precuneus/posterior cingulate cortex, lateral parietal, and medial prefrontal regions. For comparison, the Pearson correlation coefficient averaged over all combinations of the 742 regions used for network analysis was considered. The area under the resulting ROC curves was calculated alongside corresponding standard error and significance [11].
RESULTS For all thresholds |r|>0.45, aMCI patients were consistently characterized by decreased network completeness (k in Fig. 1a; for |r|>0.60:0.0147 ± 0.0100 versus 0.0096 ± 0.0046, t(78) = 3.1, pFDR = 0.009), decreased clustering coefficient (CP in Fig. 1a; for |r|>0.60:0.291 ± 0.089 versus 0.233 ± 0.085, t(78) = 2.9, pFDR = 0.01), and reduced global network efficiency (EGLOB in Fig. 1a; for |r|>0.60:0.1210 ± 0.0694 versus 0.0848 ± 0.0558, t(78) = 2.6, pFDR = 0.01). The number of regions for which node degree was lower in patients than controls gradually increased for |r|>0.20 and peaked at |r|>0.60. At this threshold, reduced node degree in aMCI was widespread and most pronounced in cuneus and pre-cuneus (extending to posterior cingulate cortex), supramarginal and angular gyri, inferior and superior parietal gyri, pre- and
216
L. Minati et al. / Functional Networks in Amnestic Mild Cognitive Impairment
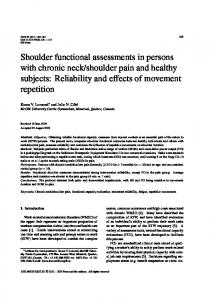
Fig. 1. a) Differences in global network parameters as a function of correlation threshold. Blue: controls, red: amnestic MCI patients. k: network completeness, CP : average clustering coefficient, EGLOB : global efficiency, %REGIONS : proportion of regions for which significant disconnection was observed. b) Bar plots of node degrees calculated for |r|>0.6 for regions of the AAL atlas. Error bars denote ± 1 standard deviation. *pFDR < 0.05, **pFDR < 0.01, ***pFDR < 0.001.
post-central gyri (Fig. 2). Reduced connectivity was also detected in insula and inferior frontal operculum, predominantly on the right, and in posterior inferior temporal gyrus, putamen, pallidus, and caudate. Average node degree was reduced in 32/45 bilateral AAL regions (Fig. 1b), with the most significant differences in the precuneus, inferior and superior parietal gyri, supramarginal gyrus, post- and pre-central gyri, paracentral lobule, superior occipital lobe, extending to the insula, cuneus, middle and inferior occipital, lin-
gual and fusiform gyri, middle and posterior cingulum; there were no lateralization effects. The corresponding equi-completeness analysis (for k = 0.01) revealed weaker effects, with decreased degree in the superior parietal gyrus, superior occipital lobe, paracentral lobule and post-central gyrus and increased degree in the medial frontal and temporal lobe; there were no lateralization effects (Supplementary Figure 2) and no differences in average clustering coefficient and global network efficiency.
L. Minati et al. / Functional Networks in Amnestic Mild Cognitive Impairment
217
Fig. 2. Topographical distribution of node degree reduction in amnestic MCI patients compared to controls.
ICA revealed decreased connectivity only for the DMN component in the medial parietal region, as well as in precuneus and posterior cingulate cortex, particularly on the right (Fig. 3, x = 10, y = −44, z = 26 mm, kE = 432 voxels, cluster-level pFWE = 0.02); increasing smoothing to 20 mm FWHM confirmed this effect (x = 10, y = −44, z = 26 mm, kE = 398 voxels, clusterlevel pFWE = 0.03). VBM analyses showed cerebral grey matter atrophy primarily confined to medial temporal structures, and precuneus to a lesser extent; these effects were weak, and did not survive correction for multiple comparisons (Fig. 3). The best discrimination accuracy was provided by node degree measured in the posterior cingulate and precuneus region, with an area-under-curve (AUC) of 0.70 ± 0.06, p = 0.001. The AUC for average ICA z-score in this region was lower and non-significant
(0.61 ± 0.07, p 0.05; Fig. 4a). The AUC for average ICA z-score calculated over the whole DMN was also non-significant (0.55 ± 0.07, p = 0.2), and similarly for the average Pearson correlation coefficient (0.59 ± 0.07, p = 0.1), however, the AUCs for network completeness (0.67 ± 0.06, p = 0.004), average clustering (0.68 ± 0.06, p = 0.002), and global efficiency (0.67 ± 0.06, p = 0.004) were all significant (Fig. 4b). DISCUSSION Graph-based analyses have shown that in aMCI there is marked disconnection of the precuneus, parietal and temporal areas, regions representing densely interconnected cortical hubs within which early deposition of extracellular amyloid is observed [3, 12, 13]. However, these analyses also demonstrate disruption
218
L. Minati et al. / Functional Networks in Amnestic Mild Cognitive Impairment
Fig. 3. Comparison of node degree changes, reduced connectivity in the default-mode network as determined by ICA, and reduced grey matter volume as revealed by VBM.
Fig. 4. ROC curves for discrimination of aMCI patients and controls. a) Node degree and ICA z-score averaged over the precuneus and posterior cingulate cortex. b) In order: average ICA z-score averaged over precuneus/posterior cingulate cortex, lateral parietal and medial frontal regions, Pearson correlation coefficient averaged over all combinations of 742 regions, network completeness (k), mean clustering (CP ) and global efficiency (EGLOB ) at |r|>0.6.
of network connectivity in brain regions where AD pathology is not manifest until late disease stages, such as sensorimotor cortex and insula, thalamus and basal ganglia. These changes may represent the downstream consequences of disconnection of the hub regions which are also involved in the DMN. The importance of modeling network architecture in full was underlined by the observation that computation of global network parameters, which are agnostic to topographical localization of changes, demonstrate disruption of small-world architecture. The extent and magnitude of these changes contrasts with the
results obtained using ICA, which revealed weaker and much more restricted connectivity changes in the precuneus-posterior cingulate region, consistent with several previous studies using ICA and SBA in aMCI [1, 2, 5, 6]. These results are in line with those of a recent study [12] on a similarly-sized cohort of aMCI patients, in which task-free fMRI was also analyzed with network graphs determined through a 1,024 region high-resolution parcellation. But there are important methodological differences between the two studies. Specifically, these relate to global signal regressions
L. Minati et al. / Functional Networks in Amnestic Mild Cognitive Impairment
(performed here but not in [12]), determination of the connectivity matrices (performed here by thresholding Pearson correlation coefficients at multiple levels and by regression significance testing after wavelet decomposition in [12]), and cortical parcellation technique (here the atlas was ‘projected’ over individual grey matter, in [12] the average grey matter probability was considered). Nevertheless, the results of the group comparisons are similar, in respect to decreased network completeness and efficiency in aMCI, with decreased nodal strength particularly in the precuneus, lateral parietal and prefrontal cortex; the more diffuse effect observed here is likely due to the different connectivity thresholding criterion. Our results additionally provide an explicit comparison with ICA and VBM. The widespread changes in functional network architecture contrasted markedly with the relatively restricted topographical distribution of atrophy. Even at an extremely permissive uncorrected threshold, volume loss as determined by VBM was primarily limited to medial temporal lobe regions with relative sparing of parietal regions. This decoupling of changes in network connectivity and brain volume supports the notion that altered brain function precedes atrophy in aMCI, and at the same time the areas where the earliest atrophy is observed are not those where disconnection is most pronounced. As such, these data may support models of AD pathophysiology which propose that in early AD the accumulation of extracellular amyloid pathology in cortical hubs proceeds separately from tau pathology, which is more closely associated to medial temporal atrophy [3, 4, 6]. While follow-up structural imaging on the AD converters still needs to be completed, the distribution of functional disconnection in our aMCI cohort has a clear correspondence to the localization of gray matter atrophy in AD patients as reported in a previous study [2], involving the precuneus, inferior temporal gyrus, fusiform gyrus, orbitofrontal and medial frontal cortex, angular gyrus, and insula. Receiver operating characteristic curves confirmed that node degree was superior to ICA DMN z-score in discriminating aMCI patients and controls, at the level of global as well as regional connectivity in the posterior cingulate cortex and precuneus region. While ICA revealed significant DMN connectivity differences in a localized cluster in the posterior cingulate cortex, the effect vanished when averaging over the whole anatomical region, and discrimination accuracy was at chance level; by contrast, discrimination based on node degree was clearly above chance level, though the accuracy was relatively modest. Of note, the best
219
AUC obtained in this study, 0.70, was considerably lower than that obtained in [12] for average correlation strength, 0.90. There are three main differences between the studies that this difference can be ascribed to: i) in our study, aMCI patients were less severely impaired, as indicated by Mini-Mental State Examination (MMSE) scores greater by about 2 points and better recall performance, ii) in our study, SNR was limited by the single-channel setup of the Siemens Allegra scanner, whereas in [12], the dense multichannel sampling implemented in the Siemens Trio likely provided much higher SNR, though this was not reported, and iii) in [12] connectivity was established on the basis of wavelet decomposition in specific frequency ranges, whereas here linear correlation was utilized. In spite of these differences, our study retains internal validity in demonstrating that graph analysis is superior to ICA on data acquired in a given setting. Decreased network completeness in patients and the fact that node degree differences were much weaker in the equi-completeness analysis indicate that the observed effects are primarily driven by diffuse reduction in connectivity strength, rather than by focal topological changes. While marked alterations in network topology and connectivity of hub regions have been previously demonstrated in equi-completeness analyses, these are primarily found in moderate to severe AD; it appears plausible that in MCI, such architecture changes are not strong enough to survive normalization of the number of connections [13]. Indeed, a recent study on aMCI found that the best discriminant between patients and controls was the mean functional connectivity strength [12]. Even though compensatory changes cannot be ruled out, we ascribe the apparent increase in connectivity observed mainly in frontal regions to the effect of completeness normalization; in these areas, functional connectivity is better preserved in comparison to others, hence their degree increases when overall connectivity is normalized. In summary, aMCI is associated with disrupted functional connectivity not only involving the cortical hub regions constituting the DMN and known to be associated with early amyloid deposition but also extending to regions where AD pathology is not observed until late stages of disease. The amplitude and topographical extent of these changes significantly exceed both the connectivity changes identified using ICA and the atrophy as determined using VBM. These data highlight the potential value of graph-based analyses of functional networks in network connectivity in the determination of biomarkers of early AD.
220
L. Minati et al. / Functional Networks in Amnestic Mild Cognitive Impairment
ACKNOWLEDGMENTS This study was partly funded by Italian Ministry of Health grants numbers GR08.22, RF09.150, and RF10.047 to MB. During the study period, DC and LM, employed by their respective institutions, were partly funded by UK Medical Research Council and Technology Strategy Board. The authors are grateful to several anonymous reviewers for insightful feedback on earlier drafts of the manuscript. Preliminary results from this study were presented at AAIC2013 Boston. Authors’ disclosures available online (http://www.jalz.com/disclosures/view.php?id=2022).
[4]
[5]
[6]
[7] [8]
[9]
SUPPLEMENTARY MATERIAL Supplementary figures and source code are available in the electronic version of this article: http:// dx.doi.org/10.3233/JAD-131766. REFERENCES [1]
[2]
[3]
Rosazza C, Minati L (2011) Resting-state brain networks: Literature review and clinical applications. Neurol Sci 32, 773-785. Gili T, Cercignani M, Serra L, Perri R, Giove F, Maraviglia B, Caltagirone C, Bozzali M (2011) Regional brain atrophy and functional disconnection across Alzheimer’s disease evolution. J Neurol Neurosurg Psychiatry 82, 58-66. Buckner RL, Sepulcre J, Talukdar T, Krienen FM, Liu H, Hedden T, Andrews-Hanna JR, Sperling RA, Johnson KA (2009) Cortical hubs revealed by intrinsic functional connectivity: Mapping, assessment of stability, and relation to Alzheimer’s disease. J Neurosci 29, 1860-1873.
[10]
[11]
[12]
[13]
deHaan W, Mott K, van Straaten ECW, Scheltens P, CJ, Stam (2012) Activity dependent degeneration explains hub vulnerability in Alzheimer’s disease. PLoS Comp Biol 8, e1002582. Petrella JR, Doraiswamy PM (2013) From the bridges of Konigsberg to the fields of Alzheimer: Connecting the dots. Neurology 80, 1360-1362. Tijms BM, Wink AM, de Haan W, van der Flier WM, Stam CJ, Scheltens P, Barkhof F (2013) Alzheimer’s disease: Connecting findings from graph theoretical studies of brain networks. Neurobiol Aging 34, 2023-2036. Sporns O, Honey CJ, K¨otter R (2007) Identification and classification of hubs in brain networks. PLoS One 2, e1049. Rubinov M, Sporns O (2010) Complex network measures of brain connectivity: Uses and interpretations. NeuroImage 52, 1059-1069. Jack CR, Jr., Albert MS, Knopman DS, McKhann GM, Sperling RA, Carrillo MC, Thies B, Phelps CH (2011) Introduction to the recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7, 257-262. Minati L, Nigri A, Cercignani M, Chan D (2013) Detection of scale-freeness in brain connectivity by functional MRI: Signal processing aspects and implementation of an open hardware co-processor. Med Eng Phys 35, 1525-1531. Hanley JA, McNeil BJ (1982) The meaning and use of the area under a Receiver Operating Characteristic (ROC) curve. Radiology 143, 29-36. Wang J, Zuo X, Dai Z, Xia M, Zhao Z, Zhao X, Jia J, Han Y, He Y (2013) Disrupted functional brain connectome in individuals at risk for Alzheimer’s disease. Biol Psychiatry 73, 472-481. Liu Y, Yu C, Zhang X, Liu J, Duan Y, Alexander-Bloch AF, Liu B, Jiang T, Bullmore E (2013) Impaired long distance functional connectivity and weighted network architecture in Alzheimer’s disease. Cereb Cortex, doi: 10.1093/cercor/bhs410.