Adaptive differential pulse code modulation (ADPCM) is a popular ... code modulation (PCM) signal, a 3 kHz sampling rate is often ... 2 Experimental techniques.
f
Errors associated with the use of adaptive differential pulse code modulation in the compression of isometric and dynamic myo-electric signals A. D. C. Chan
D.F.
Lovely
B. Hudgins
Institute of Biomedical Engineering, University of New Brunswick, PO Box 4400, Fredericton, New Brunswick, Canada E3B 5A3
Abstract--Muscle activity produces an electrical signal termed the myo-electric signal (MES). The MES is a useful clinical tool, used in diagnostics and rehabilitation. This signal is typically stored in 2 bytes as 12-bit data, sampled at 3 kHz, resulting in a 6 kbyte s storage requirement. Processing MES data requires large bit manipulations and heavy memory storage requirements. Adaptive differential pulse code modulation (ADPCM) is a popular and successful compression technique for speech. Its application to MES would reduce 12-bit data to a 4-bit representation, providing a 3:1 compression. As, in most practical applications, memory is organised in bytes, the realisable compression is 4 : 1, as pairs of data can be stored in a single byte. The performance of the ADPCM compression technique, using a real-time system at 1 kHz, 2 kHz and 4 kHz sampling rates, is evaluated. The data used include MES from both isometric and dynamic contractions. The percent residual difference (PFtD) between an unprocessed and processed MES is used as a performance measure. Errors in computed parameters, such as median frequency and variance, which are used in clinical diagnostics, and waveform features employed in prosthetic control are also used to evaluate the system. The results of the study demonstrate that the ADPCM compression technique is an excellent solution for relieving the data storage requirements of MES both in isometric and dynamic situations. Keywords--Real-time signal processing, Data compression, Myo-electric signal, Biological signals, Intelligent instrumentation Med. Biol. Eng. Comput., 1998, 36, 215-219
1 Introduction
DURING THE contraction of skeletal muscle, there is an associated movement of sodium and potassium ions in the individual muscle fibres. This electrical activity can be detected on the skin surface directly overlying the muscle using electrodes. The resultant signal is the sum of the muscle fibre action potentials in the vicinity of the electrodes, termed the myoelectric signal (MES). The MES can be used in a variety of ways, for example as a diagnostic tool or rehabilitation aid. The amplitude of the surface-recorded MES is in the order of tens of millivolts, with a bandwidth of "10 Hz-1 kHz although most of the signal energy is concentrated below 250 Hz. In converting the MES into a binary stream or pulse code modulation (PCM) signal, a 3 kHz sampling rate is often used. In addition, because of the wide dynamic range of the MES, a 12-bit resolution has become the de facto standard. Assuming the 12-bit samples are stored in byte pairs, then the storage requirement for a single channel is 6 kbytes s -l.
Correspondence should be addressed to Prof. Lovely First received 17 February 1997 and in final form 6 August 1997 9 tFMBE:1998 Medical & Biological Engineering & Computing
March 1998
It is highly desirable to reduce this large data storage requirement to lower the demands placed on memory resources. Adaptive differential pulse code modulation (ADPCM) is a compression scheme that is widely used in telephony applications to compress speech. This compression applied to MES would be able to reduce the data into a 4-bit representation. Pairs of 4-bit ADPCM data can be conveniently stored in bytes, providing an overall 4 : 1 compression ratio, i.e. the storage requirement for a signal channel is reduced to 1.5 kbytes s -1. Earlier work carried out by NORRIS and LOVELY (1995) has proven the feasibility of using ADPCM compression on MES. In this earlier study, harmonic distortion and percent residual difference (PRD) for the compression of sinusoidal signal were used as performance measures. The system was implemented in real time using dedicated hardware. A brief discussion of the errors associated with the compression of MES data for an isometric contraction of arbitrary intensity was included. The purpose of this research is to address the following questions: 9 How does the level of myo-electric activity affect performance? 9 What effect does the sampling rate have on performance? 215
9 Can the predictive nature of the compression algorithm cope with dynamic contractions?
ADC
To answer these questions, a series of experiments were performed using the same basic hardware as developed in the earlier study. The only change made to the hardware was the capability of lowering the frequency of the ADPCM clock to a 1 kHz sampling rate.
f ......... t
:
~-
I
,
......
"1:
J___M__S_M_S_2!8___:
.... ~ . ~ - - f ~ o ~ ADPCM compression system
1.1 Myo-electric signal in clinical applications In clinical diagnostics, the median frequency (MF) of the MES has been shown to reflect the action potential conduction velocity (STULEN and DELUCA, 1981). This is related to the accumulation of metabolic byproducts from cellular respiration, which can be attributed to fatigue. Research in this area has resulted in the development of several 'fatigue monitors' based on conduction velocity measurements (FIORITO et al., 1994). The MES is often modelled as a bandlimited white-noise process, whose variance increases with contraction strength. This model fits quite well for a steady-state isometric contraction, with research continuing to link the myo-electric activity to mechanical output (LEEDHAMand DOWLING, 1995). In the area of clinical rehabilitation, the MES from remnant musculature in an amputated limb can be used to control a prosthetic replacement. In commercial prosthesis, the mean absolute value (MAV) of the MES is extracted and coded into an appropriate prosthetic function, using an amplitude or slope scheme (PARKERand SCOTT, 1986). Recently, research has shown that, during the onset of a dynamic contraction, there exists a deterministic structure within the MES. This observation has been exploited in the area of multifunction prosthetic control, in which an artificial neural network (ANN) has been used to implement a classification scheme based on the first 200 ms of a dynamic contraction (HUDGINSe t aL, 1993). However, this control system is computationally intensive, requiring the use of a dedicated digital signal processor (DSP). Part of this computational burden is due to the manipulation of 12-bit samples and the extraction of a discriminant feature set. Many of the clinical applications of MES use off-line processing of the data, which requires the information to be stored in digital format. For example, in a recent study, carried out at the University of New Brunswick Institute of Biomedical Engineering, use was made of the MES to indicate the activity level of musculature of nurses. This was part of a project to investigate the effects of injury-prevention programmes introduced in the hospital workplace. To allow the unobtrusive collection of data from nurses during a standard shift, a dedicated portable monitor was designed (LOVELYe t al., 1995). The storage limitations made it impractical to store raw MES, and only peak MAVs of the MES could be collected. A data-compression system may allow the collection of raw MES, from which more clinical information could be derived.
T12-bit] "- j ~senal
~PAR/SER'i. ~. . . . . .~ 4-b~-d~Ta-~. . . . . . . . .
ADPCM ~ "~ ]pr~ cock ~ ~.~ penpheraJ I interface ISA businterface T
ii r,. LPF surface P " ~ ~ electr~ ~ - L , / isolated differential 500 Hz amplifier signal generator electronic 4,metronome
I( ~
!
i
. . . . .
,,
,, I I
[
[
I
L
~I 12-bit ADC system LPF ADC
I
oscilloscope feedbackl~~
~ I
LPF
ADC
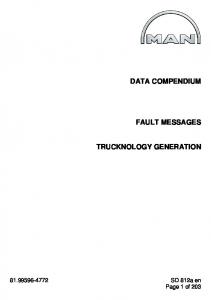
Fig. 1 Experimental setup that was used in the experiments performed by NORRIS and LOVELY (1995), except that the board was modified to operate at ADPCM sampling rates of 1, 2 and 4 kHz. Inputs to the system are provided by Ag-AgCI Red Dot* surface electrodes, via an isolated differential amplifier followed by a first-order Butterworth lowpass filter (LPF) for anti-aliasing purposes (fc = 500 Hz). The signal is split into two paths: one path undergoes ADPCM processing, and the other path passes the signal through unchanged. The ADPCM compression board is used exclusively in a 'transparent' mode, which converts the analogue input into a 4-bit ADPCM digital format and immediately decompresses it back into a reconstituted analogue signal. The raw and processed signals are passed through eighth-order Butterworth anti-aliasing filters and are sampled at 10 kHz with 12-bit resolution. This high sampling rate was used to allow accurate determination of the processing delay inherent in the ADPCM system. The two digitised signals were stored for off-line performance evaluation of the ADPCM compression scheme using MATLAB. A metronome and oscilloscope were used to provide auditory and visual feedback to the subjects. The overall experimental setup is shown in Fig. 1.
2.2 Experimental procedure for isometric contractions
The ADPCM compression was performed using a dedicated hardware system, designed around the MSM5218 speech analysis/synthesis integrated circuit*. This is the same setup
Six right-handed males were recruited for the study who had no previous history of neuromuscular disease. The MES data were taken from static isometric contractions of the right-arm bicep. The subject was placed in a chair, with the bicep resting parallel to his body, and the forearm, strapped to the chair, perpendicular to his body. Two electrodes were placed on the bicep 5 cm apart, centred on the upper arm. The reference electrode was placed at a convenient location on the forearm of the subject. The maximum voluntary contraction (MVC) for each subject was determined by monitoring the RMS DC (z = 500 ms) MES during a maximum static contraction. Target levels for isometric contractions of 10, 20, 30, 40 and 50% MVC could
* Oki Semiconductor, Sunnyvale, CA 94086, USA
* 3M Corporation, Type 2259
2 Experimental techniques 2.1 System overview
216
Medical & Biological Engineering & Computing
March 1998
then be calculated. The target level and the RMS DC MES of the subject were presented on a digital oscilloscope to aid in achieving the desired contraction level. Recordings of 10 s duration isometric contractions were made in sets of ten measurements, at ADPCM sampling frequencies of 1, 2 and 4 kHz. The target levels were presented in a random order determined using a random-number generator, using a known seed to permit repetition of the experiment. The order of the sampling frequencies was changed for each subject. With three sampling rates, there were six permutations, allowing a unique order for each of the six subjects. Before and after each set of measurements, 40 s static contractions of 10% MVC were used to monitor fatigue during the experiment. As a muscle fatigues, the median frequency of the MES power spectrum shifts to a lower frequency. The spectral compression is related to the accumulation of metabolic byproducts, giving a clear and reliable indicator of muscle fatigue. To limit fatigue effects, the subjects rested between contractions for approximately 1 min.
2.3 Experimental procedure f o r dynamic contractions The same subject pool was used for the dynamic-contraction experiments as was employed for the isometric case. The dynamic contractions were a right-arm bleep contraction, with a bungee cord used to provide an opposing force. The bleep was kept parallel to the body during the contraction, while the forearm and hand were lifted, using the elbow as the pivot point. Just as in the isometric experiment, bipolar recordings were obtained with electrodes placed on the biceps 5 cm apart, centred on the upper arm. The reference electrode was placed near the right shoulder blade of the subject, to minimise movement during the dynamic contraction. The frequency of contraction was kept constant at 0.8 Hz (period = 1.25 s) using an electronic metronome, created from a 0.8 Hz square wave fed into an audio speaker. The square wave produced two pulse sounds per cycle, or a pulse every 625 ms. On the first pulse, the bleep was contracted, and it was relaxed on the second pulse. The subject underwent a training process of 3-5 contractions using the metronome prior to sampling. Sampling was performed at a rate of 10 kHz, for a duration of 15 s, giving approximately 5-7 contractions per record. Records were made at each of the three ADPCM sampling frequencies. As with the isometric contractions, the six permutations of the sampling frequency orders were uniquely assigned to the six subjects.
The main performance measurement used in the experiment is the PRD. The PRD between the raw MES data time sequence x l , x 2 . . . . . x N and the processed MES data time sequence Yl, Y2 . . . . . YN is calculated using the formula
[ Ni~=l--(;Yi)2-
S
3 Results Typical time-domain results of the compression/expansion scheme are shown in Fig. 2. Here, a typical data segment before and after compression/expansion is shown for a dynamic contraction. From this Figure, it is clear that the ADPCM scheme reproduces the original signal with a very high degree of fidelity. This level of detail would not be possible if the sampling resolution was simply reduced to 4 bits. However, 2600 original data 2400 "~ 2200 Q < 2000
2.4 Evaluation protocol
PRD =
Various clinical parameters can be extracted from the MES to be utilised as a clinical or diagnostic tool. These include the variance and mean absolute value (MAV) of the MES, which reflects muscle activity level, and the median frequency, which can be used as a fatigue measure. These features are usually derived from isometric contractions. In addition, HUDGINS et al. (1993) have used the dynamic MES patterns associated with the onset of a contraction as a control input for a myo-electric control system. In this system the dimensionality is reduced by segmenting the MES patterns and extracting a set of time-based features. This feature set included MAV, zero crossings (ZCs), slope changes (SCs) and running length of the waveform (WL) calculated from each of the time segments. The success of the classification scheme, which relies on how well this feature set represents the waveform, can be affected by ADPCM processing. To evaluate the ADPCM compression scheme for both isometric and dynamic MES, a combination of these performance measures were employed. For the isometric case, the PRD, signal variance and MF were used. For the dynamic situation, again the PRD measure was used, in addition to the segment features used in the Hudgins classification scheme. In this way, the significance of errors introduced by the ADPCM could be evaluated in a clinical sense. To eliminate the effects of mismatched gain and time lag from ADPCM processing, the raw and processed data were normalised and temporally aligned using an unbiased bow-tie cross-correlation technique. The alignment accuracy of the cross-correlation is 4-1 sample (0.1 ms), and so the errors in the experiment will be on the high side.
2400
(1)
"~ 2200 a < 2000 1800
This performance measure is identical to the mean square error (MSE) used in optimum signal-processing algorithms. As the MES is a complex signal, typically modelled as bandlimited white noise, this is a practical and appropriate performance measure. Medical & Biological Engineering & Computing
2600 compressed/expanded data
I/2 x 100%
1800
March 1998
0
1000
2000
3000
40 4000
6000
sample number
Fig. 2
Time domain comparison of ADPCM applied to dynamic MES
217
Table 1 Percent con tractions
residual
difference
analysis
of
isometric
ADPCM
MVC
20% MVC
30% MVC
40% MVC
50% MVC
Mean
1 kHz 2 kHz 4 kHz
20.4 17.7 14.8
16.1 11.5 9.7
14.2 9.1 7.5
12.5 6.8 5.7
13.1 9.2 8.1
15.3 10.9 9.1
10%
ADPCM
25 od 20
~
--O-- Norris data ""="- 10% MVC
~=
~
20% MVC
"o "~
~
30% MVC
10
---x