Intensive Care Med DOI 10.1007/s00134-007-0859-9
CORRESPONDENCE
adjusts to changes in vascular resistance [4]. The response time to changes in vascular tone has been improved in a subsequent version of software (version 1.10) and the 10-min moving window for assessing vascular tone set to 1 min. The present investigator-blinded study was performed to evaluate the accuracy of Evaluation of an improved the latest version of COAP software algorithm for arterial in a setting of postoperative cardiac pressure-based cardiac output surgery using COPAC as the method assessment without external of reference. With approval of the institucalibration tional ethics committee and written informed consent by participants, Received: 18 April 2007 we studied 20 postoperative cardiac Accepted: 30 August 2007 surgical patients who underwent elec© Springer-Verlag 2007 tive coronary artery bypass grafting (Table 1). Prior to surgery all patients Sir: A recently introduced device for received a radial arterial line and measuring arterial pressure based car- a 7.5-F PAC. Following admission to diac output (COAP ; FloTrac, Vigileo; the intensive care unit the sensor was Edwards Lifesciences, Irvine, Calif., attached to the existing arterial line USA) has been discussed as a less and connected to a Vigileo monitor invasive alternative to the pulmonary for COAP assessment. COPAC measartery catheter (PAC) for cardiac urements were performed every 2 h output (COPAC ) assessment. To faduring mechanical ventilation and cilitate COAP assessment by arterial weaning from ventilation and after pulse waveform analysis without an extubation COPAC to obtain at least external calibration mode, the system seven values per patient. The average estimates individual arterial compliof three measurements randomly disance according to the five-component tributed over the respiratory cycle was model of Langewouters et al. [1] and calculated. COAP values were taken compensates for changes in vascusimultaneously at the end of bolus lar tone by detecting characteristic determinations and correspondingly alterations in the arterial pressure averaged. Volume administration waveform. However, recent studies and inotropic support remained conhave demonstrated limited agreement stant during measuring periods. Data between the intermittent bolus theracquisition was completed when modilution COPAC measurement and the PAC or the arterial catheter was COAP [2–4], probably caused by the removed. calculation mode with which the used A total of 158 coupled measureCOAP algorithm (version 1.03) ments were obtained. Bland–Altman
Christopher Prasser Benedikt Trabold Alexander Schwab Cornelius Keyl Susanne Ziegler Christoph Wiesenack
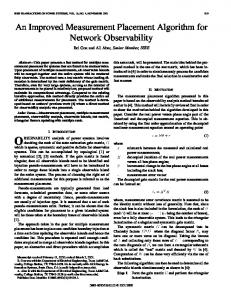
analysis between COPAC and COAP for all values showed a mean bias and limits of agreement (LOA) of 0.01 ± 1.63 l/min, as displayed in Fig. 1a. The percentage error (± 1.96 SD of the bias/mean CO) between COPAC and COAP was 26.9%. Trend analysis between percentage changes in COPAC (∆ COPAC ) and COAP (∆ COAP ) for 138 consecutive measurements revealed a bias of 0.93% with LOA of ± 28.27%, as shown in Fig. 1b. Separate analysis for mean CO values of 6 l/min or less and of more than 6 l/min showed
Table 1 Patients’ characteristics and preoperative risk scoring. (BMI, body mass index; COPD, chronic obstructive pulmonary disease; CPB, cardiopulmonary bypass; EF, left ventricular ejection fraction; EuroSCORE, European System for Cardiac Operative Risk Evaluation; PVD, peripheral vascular disease) Demographic data Age (years) 64.4 ± 9.0 Sex: M/F 15/5 (75%/25%) Weight (kg) 82.7 ± 17.3 Height (cm) 172 ± 7.8 BMI 27.8 ± 5.3 EF (%) 59.6 ± 7.7 Preoperative risk factors EuroSCORE 2.9 ± 1.5 Diabetes 6 (30%) Hypertension 16 (80%) Smoking 9 (45%) Hyperlipidemia 11 (55%) Obesity 6 (30%) History of stroke 3 (15%) PVD 2 (10%) COPD 2 (10%) Renal disease 3 (15%) Intraoperative data Grafts (n) 2.6 ± 0.8 CPB-time (min) 82 ± 25 Cross-clamp 52 ± 16 time (min)
Fig. 1 Bland–Altman plots for comparison between the intermittent thermodilution-derived cardiac output (CO PAC ) and the arterial pressure-based cardiac output (CO AP ) for all values (a), between the percentage changes in COPAC (∆CO PAC ) and COAP (∆CO AP )
a bias and LOA of –0.16 ± 1.31 and 0.21 ± 1.88, respectively. The results of the present study revealed a minimal bias and LOA below 30% between the two methods, which is within the recommended value proposed by Critchley and Critchley [5] to accept a new technique that has been compared to the reference method. Furthermore, the ability of the improved FloTrac software to reasonably detect the direction of changes in CO under different hemodynamic conditions
for consecutive measurements (b), and between mean CO values of 6 l/min or less (c) and of more than 6 l/min (d). Solid line, mean difference (bias); dashed lines, limits of agreement (bias ± 1.96 SD)
was confirmed by the trend analysis of percentage changes in CO between consecutive measurements. The tendency of the system to slightly overestimate COPAC at lower CO values and underestimate it at higher CO values should be clinically negligible as the proportional error was 25.7% and 26.0%, respectively (Fig. 1c, d). Despite the fact that the latest version of software was not directly compared to the older one, the new FloTrac algorithm appears to provide an enhanced accuracy of
COAP assessment in this setting of postoperative cardiac surgery, suggesting that the system can present a valuable alternative in the field of hemodynamic monitoring. Nevertheless, further studies are required to confirm these findings in different clinical settings. Acknowledgements. The study was supported by departmental funding from the Department of Anesthesiology, University Hospital, Regensburg, Germany. C.W. received speaking fees from Edwards Lifesciences.
References 1. Langewouters GJ, Wesseling KH, Goedhard WJ (1985) The pressure dependent dynamic elasticity of 35 thoracic and 16 abdominal human aortas in vitro described by a five component model. J Biomech 18:613–620 2. Mayer J, Boldt J, Schöllhorn T, Röhm KD, Mengistu AM, Suttner S (2007) Semi-invasive monitoring of cardiac output by a new device using arterial pressure waveform analysis: a comparison with intermittent pulmonary artery thermodilution in patients undergoing cardiac surgery. Br J Anaesth 98:176–182
3. Opdam HI, Wan L, Bellomo R (2007) A pilot assessment of the FloTrac™ cardiac output monitoring system. Intensive Care Med 33:344–349 4. Sander M, Spies CD, Grubitzsch H, Foer A, Müller M, von Heymann C (2006) Comparison of uncalibrated arterial waveform analysis in cardiac surgery patients with thermodilution cardiac output measurements. Crit Care 10:R164 5. Critchley LA, Critchley JA (1999) A meta-analysis of studies using bias and precision statistics to compare cardiac output measurement techniques. J Clin Monit Comput 15:85–91
C. Prasser · B. Trabold · A. Schwab · C. Wiesenack (u) University Hospital of Regensburg, Department of Anesthesiology, Franz-Josef-Strauss-Allee 11, 93052 Regensburg, Germany e-mail:
[email protected] Fax: +49-941-9447802 C. Keyl Heart Center Bad Krozingen, Department of Anesthesiology, Südring 15, 79188 Bad Krozingen, Germany S. Ziegler University Hospital of Regensburg, Department of Cardiothoracic and Vascular Surgery, Franz-Josef-Strauss-Allee 11, 93052 Regensburg, Germany